


Abstract
White blood cell (WBC) scintigraphy is considered the nuclear medicine imaging gold standard for diagnosing osteomyelitis in the diabetic foot. Recent papers have suggested that the use of 18F-FDG PET/CT produces similar diagnostic accuracy, but clear interpretation criteria have not yet been established. Our aim was to evaluate the role of sequential 18F-FDG PET/CT in patients with a high suspicion of osteomyelitis to define objective interpretation criteria to be compared with WBC scintigraphy. Methods: Thirteen patients whom clinicians considered positive for osteomyelitis (7 with ulcers, 6 with exposed bone) were enrolled. The patients underwent 99mTc-exametazime WBC scintigraphy with acquisition times of 30 min, 3 h, and 20 h and sequential 18F-FDG PET/CT with acquisition times of 10 min, 1 h, and 2 h. A biopsy or tissue culture was performed for final diagnosis. Several interpretation criteria (qualitative and quantitative) were tested. Results: At final biopsy, 7 patients had osteomyelitis, 2 had soft-tissue infection without osteomyelitis, and 4 had no infection. The best interpretation criterion for osteomyelitis with WBC scintigraphy was a target-to-background (T/B) ratio greater than 2.0 at 20 h and increasing with time. A T/B ratio greater than 2.0 at 20 h but stable or decreasing with time was suggestive of soft-tissue infection. A T/B ratio of no more than 2.0 at 20 h excluded an infection. Thus, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for osteomyelitis were 86%, 100%, 100%, 86%, and 92%, respectively. For 18F-FDG PET/CT, the best interpretation criterion for osteomyelitis was a maximal standardized uptake value (SUVmax) greater than 2.0 at 1 and 2 h and increasing with time. A SUVmax greater than 2.0 after 1 and 2 h but stable or decreasing with time was suggestive of a soft-tissue infection. An SUVmax less than 2.0 excluded an infection. 18F-FDG PET at 10 min was not useful. Using these criteria, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for osteomyelitis were 43%, 67%, 60%, 50%, and 54%, respectively. Combining visual assessment of PET at 1 h and CT was best for differentiating between osteomyelitis and soft-tissue infection, with a diagnostic accuracy of 62%. Conclusion: 18F-FDG PET/CT, even with sequential imaging, has a low diagnostic accuracy for osteomyelitis and cannot replace WBC scintigraphy in patients with diabetic foot.
According to data from the World Health Organization, about 180 million people in the world have diabetes mellitus, with foot infection being one of the most common and severe complications (1). Up to 15% of diabetic patients will develop foot ulcers, and about 15%–25% of these patients require amputation (2–4). About 2.5% of diabetic patients have a Charcot joint, a progressive degenerative disease of the musculoskeletal system usually involving the tarsal and tarsometatarsal joints (5). The disorder results in destruction of bone and soft tissue, causing significant damage to the bony architecture. Clinically, patients present with swelling, crepitus, palpable loose bodies, and osteophytes. The etiology may be caused by peripheral neuropathy complicated by motor, sensory, and autonomic disorders, and to vascular insufficiency, both secondary to diabetes. In addition, local trauma or pressure may result in diabetic foot. Antibiotic therapy, in conjunction with conservative surgery (debriding), may be curative and avoid amputation, but an early and prompt diagnosis is necessary. The detection of diabetic foot infection can be difficult. With clinical examination, it is difficult to differentiate between soft-tissue infection and osteomyelitis. The erythrocyte sedimentation rate is not specific (6). Bone biopsy is not always performed because it is an invasive procedure that loses its reliability when the biopsy fragment is contaminated by cutaneous bacteria (7). Therefore, imaging is crucial in the evaluation. Plain radiography and CT are used routinely but are not accurate enough. MRI is able to differentiate between osteomyelitis and soft-tissue infection (1,8), but the specificity is reduced if bony destruction, dislocation, marrow edema, synovial effusion, and loss of discernible bone and joint margins are present—conditions that characterize neuropathic joints as well as osteomyelitis. Nuclear medicine techniques play an important role in the diagnosis of infections. The sensitivity of 3-phase bone scintigraphy has been quite variable (≤75%) (9,10), but specificity for osteomyelitis in diabetic foot infection is low. White blood cell (WBC) scintigraphy with either 99mTc-exametazime– or 111In-oxine–labeled cells is currently the radionuclide gold standard for the diagnosis of osteomyelitis. The labeling method is well described in several guidelines, including those from the European Association of Nuclear Medicine, Society of Nuclear Medicine, and International Society of Radiolabeled Blood Elements (11–15).
Another possibility is the use 18F-FDG PET/CT, which has some theoretic advantages: no blood manipulation is necessary, acquisition time is shorter, and image resolution is higher. 18F-FDG accumulates in inflammatory cells because these, like malignant cells, metabolize glucose as a source of energy (16). With the routine 18F-FDG PET protocols, it is not possible to reliably distinguish infection from inflammation. No acquisition protocols for 18F-FDG PET in the diabetic foot have yet been validated, and only a few comparison studies between 18F-FDG PET and WBC scintigraphy are available.
One aim of this study was to define whether a new acquisition protocol with sequential 18F-FDG PET/CT may help in differentiating between infection and inflammation and may contribute to the diagnosis of osteomyelitis in the diabetic foot. To meet this aim, we compared this protocol with WBC scintigraphy for diagnostic accuracy. Another aim was to investigate possible interpretation criteria—both qualitative and quantitative—for WBC scintigraphy and for 18F-FDG PET/CT to see which criteria are best able to differentiate between osteomyelitis, soft-tissue infection, and no infection at all.
MATERIALS AND METHODS
Patients
Thirteen diabetic patients with a high clinical suspicion of foot osteomyelitis, as evaluated by the diabetologist and surgeon, were included in this study (12 men and 1 woman) and evaluated using WBC scintigraphy and sequential 18F-FDG PET/CT. Seven patients had ulcers of the forefoot or mid- to hindfoot with exposed bone, and 6 patients had a high clinical suspicion of osteomyelitis without exposed bone. The high clinical suspicion was based on the presence of signs and symptoms of infection. Wound infection was defined according to the criteria of the International Working Group on the Diabetic Foot as the presence of 2 or more signs and symptoms of local inflammation or systemic signs of infection with no other apparent cause, along with purulent exudates (17). In addition, other specific signs such as necrosis, delayed wound healing, and foul odor were used.
Five patients had an increased level of hemoglobin A1c, but all had a blood glucose level below 160 mg/dL at time of the 18F-FDG PET/CT scan. Four patients had an increased erythrocyte sedimentation rate and C-reactive protein, and 5 patients had leukocytosis. All patients were treated with antibiotic therapy, but this therapy was suspended 1 wk before the imaging studies, thereby not reducing the sensitivity of the imaging. The patients’ characteristics are listed in Tables 1 and 2.
Patients’ Characteristics
Characteristics of Involved Regions, Type and Size of Lesions, and Results of Bone Biopsies and Microbiology
WBC scintigraphy was performed on day 1 and, for the delayed acquisition, at 20 h (day 2), and 18F-FDG PET/CT was performed on day 2. One patient also underwent bone marrow scintigraphy with 99mTc-nanocolloids for differential diagnosis of Charcot foot. All patients underwent biopsy or surgery for definitive diagnosis within a week of the scans.
Informed consent was obtained from all patients as requested by the local Medical Ethical Committee.
99mTc-Exametazime WBC Scintigraphy
WBC scintigraphy was performed according to previously published methods, with slight modifications (12,14), using Leukokit (Gipharma). Images of the foot (anteroposterior and mediolateral views) were acquired 30 min (100 s/image), 3 h (140 s/image), and 20 h (1,040 s/image) after intravenous injection of 555–740 MBq of 99mTc-exametazime. Because calculation of acquisition time was based on the decay of technetium, the resulting images were decay-corrected and their interpretation did not require an operator postacquisition modification.
In 1 equivocal case, a bone marrow scan was performed using 185 MBq of 99mTc-Nanocoll (GE Healthcare) with images acquired 20 min after injection (600 s/image). This bone marrow scan was performed after WBC scintigraphy and before 18F-FDG PET/CT.
18F-FDG PET/CT
Patients had to fast for at least 6 h before receiving a 185-MBq intravenous injection of 18F-FDG. They followed their regular drug schedule. The blood glucose level was measured before injection and was less than 160 mg/dL in all patients. 18F-FDG PET and unenhanced CT images of the lower limbs were acquired at 10 min (3 min per bed position), 1 h (4.5 min per bed position), and 2 h (6 min per bed position) after the injection, considering 18F decay time. A Gemini PET/CT system (Philips) was used, combining a third-generation multislice spiral CT scanner (low-dose, 16-slice, 100-mAs) with a dedicated full-ring PET scanner (bismuth germinate crystals). The PET and CT devices were mechanically aligned back to back and shared a table. Proper registration of images was ensured by shared positional information on the table and patient for both the CT and the PET acquisitions. Data obtained from the CT scan were used for attenuation correction of the PET data and for fusion with attenuation-corrected PET images to integrate physiologic and anatomic images.
Imaging Analysis
For WBC scintigraphy, the determination of abnormal increased uptake was based qualitatively on visual assessment of asymmetry versus symmetry in comparisons with the other foot and with other parts of the same foot. The area of suspected infection was identified, and a region of interest was drawn around this lesion (target). The WBC scintigraphy findings were assessed quantitatively by drawing a second region of interest on the same area on the other foot (background) and calculating the target-to-background ratio (T/B) at each time point.
For 18F-FDG PET/CT, the same procedure was followed. For quantification, the maximal standardized uptake value (SUVmax) in the target lesion was calculated at each time point.
All images were analyzed by 3 independent nuclear medicine physicians, who reached agreement in every case.
Bone Biopsy, Cultures, and Surgery
Bone biopsy was performed for a definitive diagnosis. The sample of bone (a small cylinder a few millimeters in length and 1.5–2 cm in diameter) was taken from the site of suspected osteomyelitis. The procedure was performed in outpatient settings and with local anesthesia. Biopsies were analyzed histologically for neutrophilic infiltration (considered a sign of osteomyelitis). When surgery was necessary, the bone biopsy was performed, or samples for culturing obtained, in a surgical setting.
Statistical Analysis
To determine the highest diagnostic accuracy, several cutoff values of T/B and SUVmax were considered. Data were compared, and t tests were used when appropriate.
RESULTS
Results of Biopsy and Microbiology
After biopsy or culture, osteomyelitis was proven in 7 patients and soft-tissue infection without bone involvement in 2. Four patients had no infection (Table 2). These final diagnoses were considered the gold standard.
99mTc-Exametazime WBC Scintigraphy
Table 3 lists the results of WBC scintigraphy and the T/B ratios after 30 min, 3 h, and 20 h. The visual (qualitative) assessment of the WBC scintigraphy showed a high diagnostic accuracy for the final diagnosis (92%). The best quantitative results occurred when the following interpretation criteria were used (Table 4): WBC scintigraphy was considered negative for an infection when the T/B ratio was no more than 2.0 after 20 h and the ratios were stable or decreasing over time; WBC scintigraphy was considered positive for osteomyelitis when the T/B ratio after 20 h was more than 2.0 and the ratios were increasing over time; and WBC scintigraphy was considered positive for a soft-tissue infection when the T/B ratio after 20 h was more than 2.0 but the ratios were stable or decreasing over time.
Quantitative and Qualitative Results of WBC Scintigraphy and 18F-FDG PET/CT Compared with Final Diagnosis by Biopsy
Interpretation Criteria for WBC Scintigraphy and 18F-FDG PET/CT
Using these criteria, WBC scintigraphy was able to identify correctly all 4 patients who were without infection and 6 of the 7 patients with proven osteomyelitis. Only 1 patient was considered to have a soft-tissue infection on WBC scintigraphy but had a final diagnosis of osteomyelitis. This patient was also considered to have a soft-tissue infection on visual assessment. In the 2 patients who had a final diagnosis of soft-tissue infection, these quantitative criteria gave the correct diagnosis. Overall, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy for osteomyelitis with these quantitative interpretation criteria were 86%, 100%, 100%, 86%, and 92%, respectively.
18F-FDG PET/CT
The results of 18F-FDG PET/CT, including SUVmax calculated at 10 min, 1 h, and 2 h after injection, are also listed in Table 2. The best quantitative results were obtained using interpretation criteria that were comparable with the criteria of the WBC scintigraphy. However, the calculated T/B ratios 10 min after injection were not useful. The following interpretation criteria were used (Table 4): 18F-FDG PET was considered negative for infection when the SUVmax was less 2.0 after 1 and 2 h; 18F-FDG PET was considered positive for osteomyelitis when the SUVmax was no more than 2.0 after 1 and 2 h and was increasing over time; 18F-FDG PET was considered positive for a soft-tissue infection when the SUVmax was more than 2.0 after 1 and 2 h, but was stable or decreasing over time.
Using these criteria, 18F-FDG PET was able to correctly identify 3 of the 4 patients who were without infection. One infection-free patient was considered to have osteomyelitis using these criteria. Only 3 of the 7 patients with proven osteomyelitis were correctly identified by 18F-FDG PET. Of the remaining 4, 3 were considered to have a soft-tissue infection and 1 was considered to have no infection. Of the 2 patients with a soft-tissue infection, 1 was correctly identified by 18F-FDG PET and the other was considered to have osteomyelitis. The overall sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of 18F-FDG PET for osteomyelitis with these quantitative interpretation criteria, was 43%, 67%, 60%, 50%, and 54%, respectively.
Combining the visual (qualitative) assessment of the 18F-FDG PET and CT images changed the results for 2 patients. In 1 patient, considered to have osteomyelitis when the interpretation criteria were used, CT allowed exclusion of osteomyelitis and showed a soft-tissue infection. This patient had a negative final diagnosis. In the other patient, with a soft-tissue infection when the interpretation criteria were used, CT was able to detect osteomyelitis. The overall diagnostic accuracy for the qualitative assessment was 62%.
Examples of use of the interpretation criteria for WBC scintigraphy and 18F-FDG PET/CT are shown in Figures 1–3.
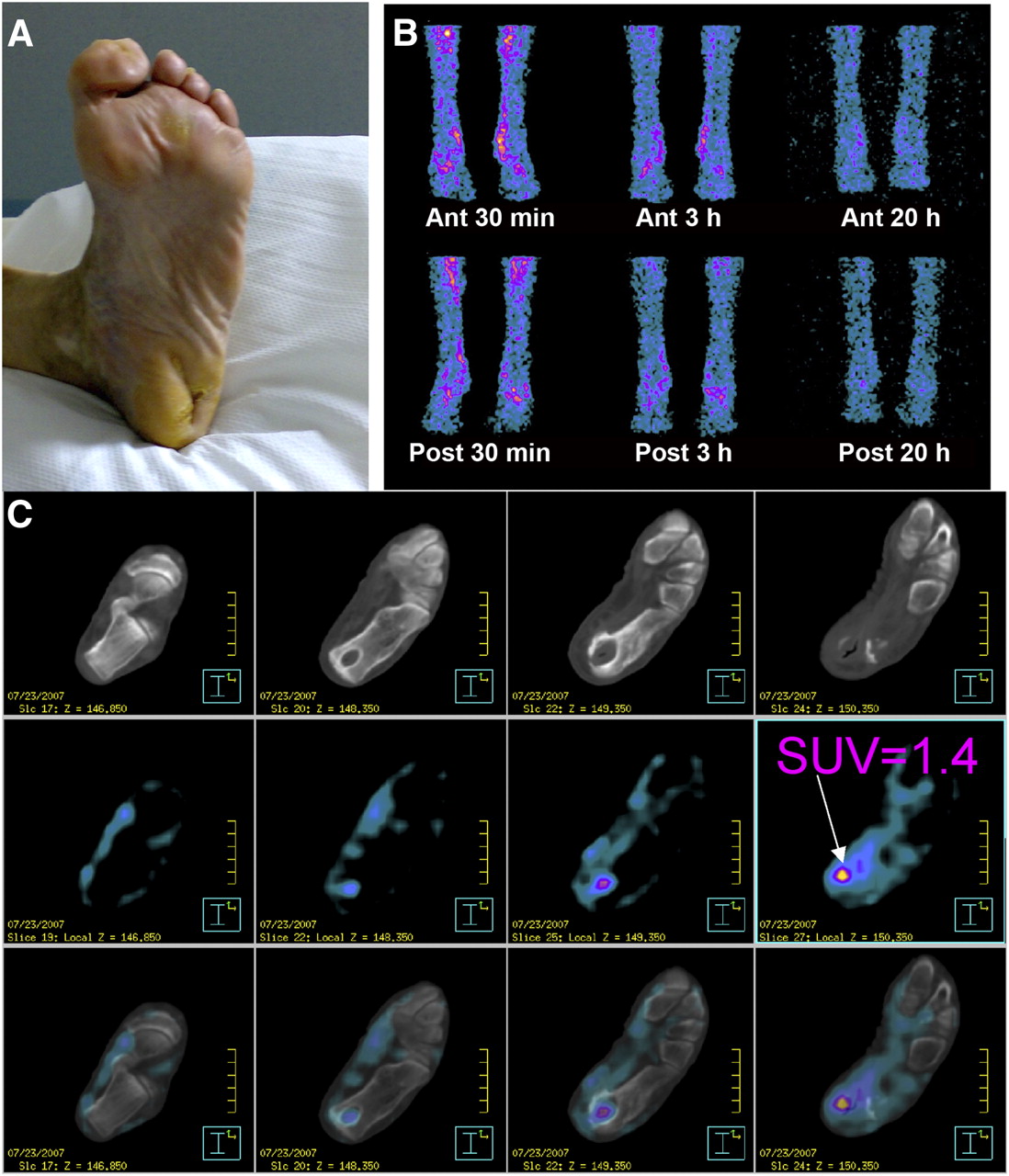
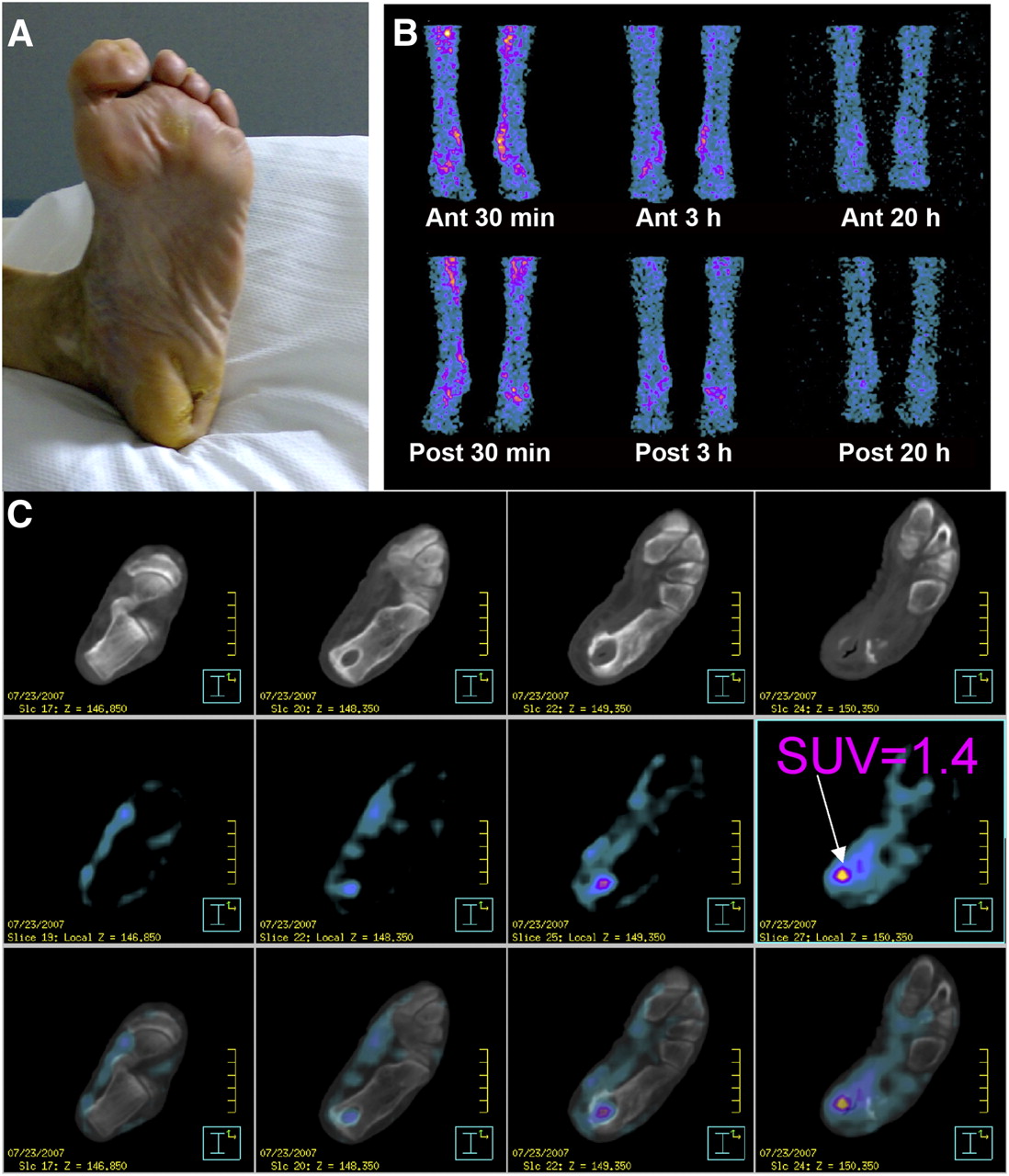
In patient 3, negative results concordant between WBC scintigraphy (T/B ratio < 2.0 and decreasing over time) and 18F-FDG PET/CT (SUVmax < 2.0): clinical image of diabetic foot (A); anterior and posterior WBC scintigraphy images after 30 min, 3 h, and 20 h (B); transaxial 18F-FDG PET/CT images after 1 h (C). Ant = anterior; Post = posterior.
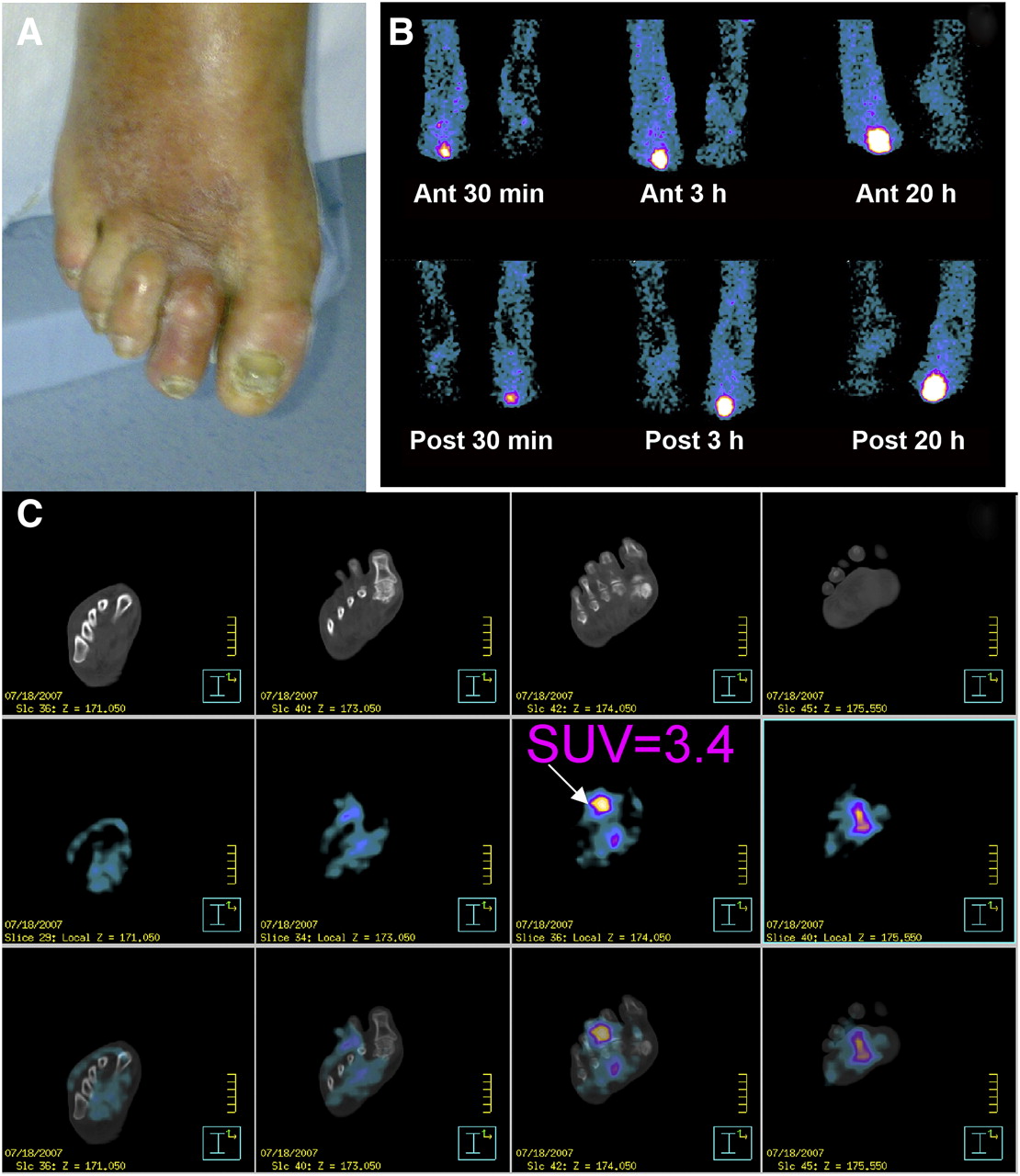
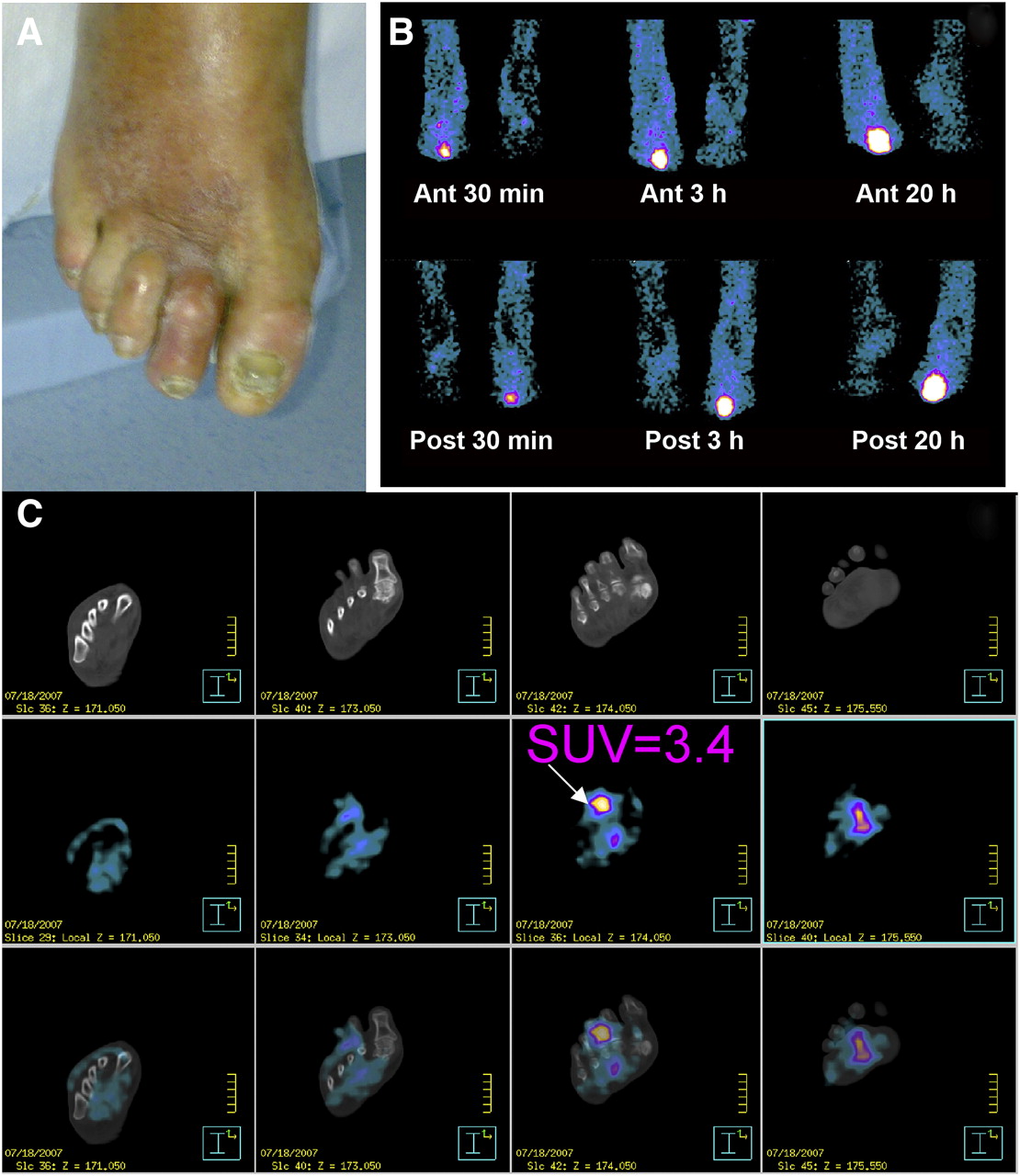
In patient 13, positive osteomyelitis results concordant between WBC scintigraphy (T/B ratio > 2.0 and increasing over time) and 18F-FDG PET/CT (SUVmax > 2.0 and CT-confirmed localization in bone): clinical image of diabetic foot (A); anterior and posterior WBC scintigraphy images after 30 min, 3 h, and 20 h (B); transaxial 18F-FDG PET/CT images after 1 h (C). Ant = anterior; Post = posterior.

In patient 12, discordant results between WBC scintigraphy, which was positive for osteomyelitis (T/B ratio > 2.0 and increasing over time), and 18F-FDG PET/CT, which was negative for osteomyelitis (SUVmax < 2.0): clinical image of diabetic foot (A); anterior and posterior WBC scintigraphy images after 30 min, 3 h, and 20 h (B); transaxial 18F-FDG PET/CT images after 1 h (C). Ant = anterior; Post = posterior.
DISCUSSION
Infection of the diabetic foot is a common complication in diabetic patients and often requires hospitalization. Early diagnosis is invaluable but is difficult using noninvasive imaging techniques. Different radiologic and nuclear medicine imaging techniques are available, but most lack accuracy. WBC scintigraphy is considered the nuclear medicine gold standard and has high accuracy. To preserve cell viability, it is important that WBCs be labeled using a validated method performed by trained personnel. It is an ex vivo procedure for which there are several available guidelines. The image acquisition method and interpretation criteria may vary among centers and countries but are also important because they may affect the diagnostic accuracy of the technique (procedural guidelines are also available from most scientific societies). The use of 18F-FDG PET/CT should have the advantages of easier preparation, shorter acquisition times, and better image resolution, besides the fact that no blood manipulation is necessary. However, when one is following normal 18F-FDG PET protocols that call for imaging 60–90 min after injection, differentiation between infection and inflammation is usually not possible. Therefore, the aim of this study was to determine whether sequential 18F-FDG PET/CT could help with this differentiation. The results were discouraging. Several interpretation criteria were tried, but even the best criterion had only a low diagnostic accuracy. For example, when we used a criterion of SUVmax (after 2 h) > SUVmax (after 1 h) or SUVmax (after 1 h) > SUVmax (after 10 min), all patients were positive for osteomyelitis, including 3 of 4 patients that were finally found to be negative for infection. The highest accuracy for osteomyelitis was obtained using a positivity criterion of an SUVmax (after 2 h) of at least 2.0 and increasing over time. However, the diagnostic accuracy remained low: 54%. A typical pattern for 18F-FDG uptake over time in patients with a diabetic foot could not be defined.
The acquisition 10 min after injection was found not to be useful. A dual-acquisition protocol could be helpful for differentiating between osteomyelitis and soft-tissue infection, but of primary relevance for this differentiation is the CT component. The contribution of CT is more important than the interpretation criteria, because the CT images contribute to the conclusion about whether the 18F-FDG uptake is primarily in the bone or in the surrounding soft tissue.
The literature includes only a few studies of the role of 18F-FDG PET (or PET/CT) in diabetic-foot patients, and most of these studies had high accuracy results. Basu et al. evaluated a total of 63 patients and found a high SUVmax of 2.9–6.2 for osteomyelitis, compared with 0.7–2.4 for Charcot joints and 0.2–0.7 for uncomplicated diabetic foot. The authors stated that 18F-FDG PET can differentiate between Charcot neuroarthropathy, osteomyelitis, and soft-tissue infection (16). The same group also compared the utility of 18F-FDG PET with that of MRI and radiography in 101 subjects. 18F-FDG PET correctly diagnosed osteomyelitis in 21 of 26 patients and correctly excluded it in 74 of 80, with sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 81%, 93%, 78%, 94%, and 90%, respectively (18). Keidar et al. used PET/CT to evaluate 14 diabetic patients with 18 clinically suspected sites of infection for suspected osteomyelitis complicating diabetic foot disease. PET detected 14 foci of increased 18F-FDG uptake suspected of being infection in 10 patients. PET/CT correctly localized 8 foci in 4 patients to bone, indicating osteomyelitis, and correctly excluded osteomyelitis in 5 foci in 5 patients, with the 18F-FDG uptake limited to infected soft tissues. Four patients showed no increased uptake and no further evidence of an infectious process on follow-up. The authors concluded that 18F-FDG PET can be used for diagnosis of diabetes-related infection and that PET/CT enables accurate differentiation between osteomyelitis and soft-tissue infection (2). Only 1 study, published by Schwegler et al., found disappointing results for 18F-FDG PET, with MRI being superior to 18F-FDG PET and to 99mTc-labeled monoclonal antigranulocyte antibody scintigraphy (19).
The low diagnostic accuracy we found for 18F-FDG PET, even with sequential scanning, is discordant with most results known from the literature. The reason for our low accuracy is not understood. A possible reason could be that the long duration of infection and lengthy use of antibiotics (mean, 45 d) led to a low uptake of 18F-FDG. However, our study also found a role for PET/CT in differentiation between osteomyelitis and soft-tissue infection, but the CT component was most important in that differentiation.
In agreement with the literature, our study found WBC scintigraphy to have high diagnostic accuracy for infectious disorders. The diagnostic accuracy we found—92%—was even higher than found in the literature but could be the result of the high prevalence of infection in our selected population.
Agreement was excellent between the 3 independent nuclear medicine physicians who analyzed the WBC scintigraphy results; no discordance was found. Interpretation criteria showing high diagnostic accuracy were determined for WBC scintigraphy. Good differentiation between osteomyelitis, soft-tissue infection, and no infection at all is possible using the correct cell-labeling methods, acquisition protocols, and interpretation criteria. A T/B ratio greater than 2.0 after 20 h is suggestive of infection: osteomyelitis if the ratio is increasing over time; soft-tissue infection if the ratio is decreasing over time. A ratio of 2.0 or less can be considered negative for infection.
Despite some limitation (such as a high pretest probability of disease in our population and a small sample size), this study leads to 2 important conclusions: osteomyelitis, when highly suspected clinically in the diabetic foot, is not necessarily present, and further examinations are required; sequential 18F-FDG PET is not useful for the diagnosis of diabetic foot osteomyelitis; WBC scintigraphy is more accurate. Trials on larger populations of patients may help elucidate the clinical role of 18F-FDG PET/CT in the diabetic foot.
CONCLUSION
The results of this pilot study confirmed the high diagnostic accuracy of WBC scintigraphy in the diabetic foot. Interpretation criteria that are helpful in differentiating between osteomyelitis, soft-tissue infection, and no infection were determined. When the correct labeling procedures and acquisition protocols are followed, WBC scintigraphy remains the gold standard noninvasive imaging technique.
18F-FDG PET/CT was found to have a low diagnostic accuracy in the diabetic foot. No useful SUVmax criteria for differentiating between soft-tissue infection and osteomyelitis could be found. Combining visual assessment of the PET and CT images was more useful. Sequential 18F-FDG PET/CT was not found to be helpful for diagnosis of the diabetic foot. On the basis of the obtained results, we believe that WBC scintigraphy currently remains the gold standard imaging technique.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication August 12, 2010.
- Accepted for publication February 16, 2011.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Detection of Osteomyelitis in the Diabetic Foot by Imaging Techniques: A Systematic Review and Meta-analysis Comparing MRI, White Blood Cell Scintigraphy, and FDG-PET
- Radionuclide Imaging of Musculoskeletal Infection: A Review
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- 18F-FDG and Diabetic Foot Infections: The Verdict Is...