


Abstract
The study aims to investigate the presence of physiologic prostate-specific membrane antigen (68Ga-PSMA)-ligand uptake on PET in cervical, celiac, and sacral ganglia of the sympathetic trunk as a pitfall for lymph node metastases in prostate cancer imaging. Methods: Four hundred seven patients who underwent Glu-NH-CO-NH-Lys radiolabeled with 68Ga-gallium N,N-bis[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N-diacetic acid (68Ga-PSMA-HBED-CC) PET (combined with a diagnostic CT) were retrospectively analyzed. The number of 68Ga-PSMA PET–positive cervical, celiac, and sacral ganglia was determined, and the configuration and SUVmax of each ganglion were measured. In addition, the configuration and SUVmax of adjacent lymph node metastases in the respective region (cervical, celiac, or sacral) were determined. Results: 68Ga-PSMA-ligand uptake above background was detected in 401 (98.5%) patients in any peripheral ganglia, in 369 (92%) patients in cervical ganglia, in 363 (89%) patients in celiac ganglia, and in 183 (46%) patients in sacral ganglia. The 68Ga-PSMA-ligand uptake was highest in celiac (mean SUVmax, 2.9 ± 0.8 vs. cervical mean SUVmax, 2.4 ± 0.6) and sacral (mean SUVmax 1.7 ± 0.5; both P < 0.0001) ganglia. Intraindividually there was a statistically significant but weak to moderate correlation between the 68Ga-PSMA-ligand uptake in cervical versus celiac ganglia (R = 0.34, P < 0.0001), cervical versus sacral (R = 0.52, P < 0.0001), and celiac versus sacral (R = 0.16, P < 0.05). The 68Ga-PSMA-ligand uptake was significantly more intense in adjacent lymph node metastases than the respective ganglia (cervical: 18.0 ± 16.2 vs. 2.4 ± 0.6, P < 0.0001; celiac: 13.5 ± 12.3 vs. 2.9 ± 0.8, P < 0.0001; sacral: 13.4 ± 11.6 vs. 1.7 ± 0.5, P < 0.0001). Furthermore, ganglia predominantly exhibit a band-shaped configuration (71.2%), followed by a teardrop (26.8%) and only rarely a nodular configuration (2.0%). Conversely, lymph node metastases are only rarely band-shaped (1.1%), but more often show teardrop (40.3%) or nodular appearance (58.6%) (P < 0.00001). Conclusion: 68Ga-PSMA-ligand uptake in ganglia along the sympathetic trunk as assessed by 68Ga-PSMA-HBED-CC PET represents an important pitfall in prostate cancer PET imaging. The 68Ga-PSMA-ligand uptake is higher in celiac ganglia than cervical or sacral ganglia, and the level of 68Ga-PSMA-ligand uptake seems to be patient-related. For the differentiation between lymph node metastases and sympathetic ganglia, both intensity of 68Ga-PSMA-ligand uptake and exact localization and configuration of the respective lesion should be examined carefully.
The prostate-specific membrane antigen (68Ga-PSMA) is a membrane-bound enzyme, which is highly expressed on prostate cancer cells and its metastases (1). It is also named glutamate carboxypeptidase II based on its enzymatic function. 68Ga-PSMA-targeted imaging using PET radiotracers, such as Glu-NH-CO-NH-Lys radiolabeled with 68Ga-gallium N,N-bis[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N-diacetic acid (68Ga-PSMA-HBED-CC), has therefore experienced an increasing demand during the last few years (2). In some centers, 68Ga-PSMA PET imaging is now regarded as the method of reference for staging and restaging of patients with confirmed (high-risk) prostate cancer or in the case of biochemical recurrence; furthermore, even at low prostate-specific antigen levels and for small lymph node metastases, 68Ga-PSMA PET imaging offers a high sensitivity (2–5).
However, high 68Ga-PSMA expression has also been described in malignant lesions not related to the prostate (e.g., renal cell carcinoma, bronchial carcinoma, glioblastoma), in benign tissues (e.g., renal tubules, duodenum, colon), and in benign lesions such as schwannomas, osteophytes, thyroid adenomas or vertebral and subcutaneous hemangiomas (1,6–14). The ganglia of the sympathetic trunk are another tissue in which an increased 68Ga-PSMA expression has been reported (15,16). Histologic studies have found that the glutamate carboxypeptidase II is highly expressed on nonmyelinating Schwann cells in ganglia of the sympathetic nervous system. This potentially explains 68Ga-PSMA-ligand uptake in various parts of the sympathetic nervous system (17). As the sympathetic trunk runs along the vertebra, sympathetic ganglia can easily be confused with lymph node metastases that are often found near particularly to cervical, celiac, or sacral ganglia. Consequently, 68Ga-PSMA-ligand uptake in such ganglia is a potential source of misdiagnosis, which may even result directly in change of therapy regimen and therefore represents an important pitfall. The aim of this retrospective analysis was to give a detailed description of the incidence and imaging pattern in 68Ga-PSMA-HBED-CC PET/CT of cervical, celiac, and sacral ganglia to facilitate the discrimination from prostate cancer–related lymph node metastases.
MATERIALS AND METHODS
Patient Population, Radiotracer Synthesis, and Imaging Protocol
Four hundred seven patients from 2 centers (Technical University Munich and University of Freiburg) who underwent 68Ga-PSMA-HBED-CC PET/CT between October 2012 and August 2015 were randomly selected and analyzed. Only studies with a diagnostic CT were chosen to allow for detailed anatomic description of the configuration of ganglia and lymph node metastases.
The retrospective study was approved by the Ethics Committee of the Technical University Munich (permit 5665/13), and written informed consent was obtained from all patients for the purpose of anonymized evaluation and publication of their data. All reported investigations were conducted in accordance with the Helsinki Declaration and with national regulations.
PET/CT scans were obtained on a Siemens Biograph mCT (Siemens Healthcare) or a 64-slice GEMINI TF PET/CT (Philips Healthcare). Radiotracer synthesis was performed as previously described (3) and injected via an intravenous bolus (167 ± 28 MBq; range, 120–240 MBq). PET/CT acquisition was started 56 ± 8 min (range, 32–85 min) after tracer injection. The diagnostic CT scan was acquired after patients received oral contrast and in portal venous phase. Subsequently, the PET scan was acquired in 3-dimensional mode with an acquisition time of 3–4 min per bed position (Munich) or with 2 min per bed position, whole-body protocol with 50% overlap (Freiburg). Correction of emission data for randoms, dead time, scatter, and attenuation was performed. Iterative reconstruction of PET data by an ordered-subsets expectation maximization algorithm (4 iterations, 8 subsets) followed by a postreconstruction smoothing gaussian filter (5 mm in full width at one-half maximum) was performed (Munich), or PET list-mode data were reconstructed using a lines-of-response–based ordered-subsets algorithm with time-of-flight information in a 2 × 2 × 2 mm voxel matrix (BLOB-OS-TF, 3 iterations, 33 subsets, relaxation parameter l = 0.35, no additional smoothing) (Freiburg).
Image Analysis
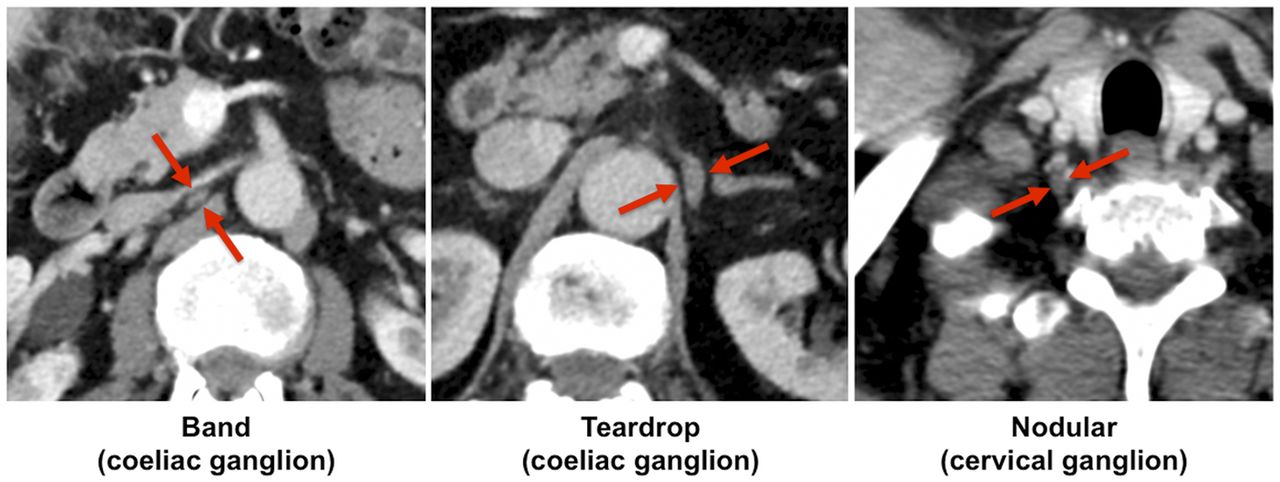
Images were analyzed by 2 experienced nuclear medicine physicians (4 and 12 y of training). PET and CT images were analyzed side by side and the number, location (left/right, cervical/celiac/sacral), 68Ga-PSMA-ligand uptake intensity (SUVmax normalized to body weight and visual intensity ranging from 0 to 3 [faint/mild/moderate/intense uptake]; Fig. 1), and configuration (band, teardrop, or nodular shape; Fig. 2) of 68Ga-PSMA-positive sympathetic ganglia were assessed. Main criteria for ganglia were focal 68Ga-PSMA-ligand uptake that projected onto a structure with typical location for sympathetic ganglia. In a second step, the same parameters for definite lymph node metastases near the respective ganglia were determined, to investigate potential criteria for differentiation.

68Ga-PSMA-HBED-CC uptake of cervical, celiac, and sacral ganglia. (Left) Diagnostic, contrast-enhanced CT. (Middle) 68Ga-PSMA-HBED-CC PET. (Right) Overlay of 68Ga-PSMA-HBED-CC PET and CT. Red arrows indicate ganglia at respective location.

Overview of different anatomic configurations of ganglia. Red arrows indicate ganglia at respective location.
Histology
From patients who had an extensive surgery of the pelvis, sacral ganglia were obtained and stained for 68Ga-PSMA expression as previously described (18).
Statistics
Results are either demonstrated as frequencies (%) or as mean ± SD. P values less than 0.05 were considered statistically significant. For comparison of unmatched, continuous variables, the 2-tailed unpaired Student t test was used. The χ2 test was applied to compare nominal variables. Matched continuous variables were compared using the 2-tailed paired Student t test. The association between continuous variables was investigated using the Pearson correlation coefficient. For statistical analyses MedCalc (version 17.4; MedCalc Software) for Windows (Microsoft) and SPSS Statistics for Windows (version 22.0; IBM Corp Released 2013; IBM Corp.) were used.
RESULTS
Prevalence and Semiquantitative 68Ga-PSMA-Ligand Uptake of Sympathetic Ganglia
On a per-patient basis, 68Ga-PSMA-ligand uptake in any peripheral sympathetic ganglia was detected in 98.5% (401/407 patients). Grouped by anatomy, local positive 68Ga-PSMA-ligand uptake was found at a frequency of 91.8% (369/402 patients), 89.4% (363/406 patients), and 45.5% (183/402 patients) in cervical, celiac, and sacral ganglia, respectively (Fig. 3A). The lower rate of 68Ga-PSMA-positive sacral than cervical and celiac ganglia was highly statistically significant. Notably, because of adjacent bone or lymph node metastases 68Ga-PSMA-ligand uptake in cervical, celiac, and sacral ganglia could not be evaluated in 5, 1, and 5 patients, respectively.

Number and uptake intensity of 68Ga-PSMA-HBED-CC–positive ganglia. (A) Frequencies (on per-patient-basis) of 68Ga-PSMA-HBED-CC uptake in any, celiac, cervical, and sacral ganglia. (B) Distribution of visual uptake intensities of sympathetic ganglia. (C) Quantitative comparison of 68Ga-PSMA-HBED-CC uptake (SUVmax) in sympathetic ganglia. *Significant differences.
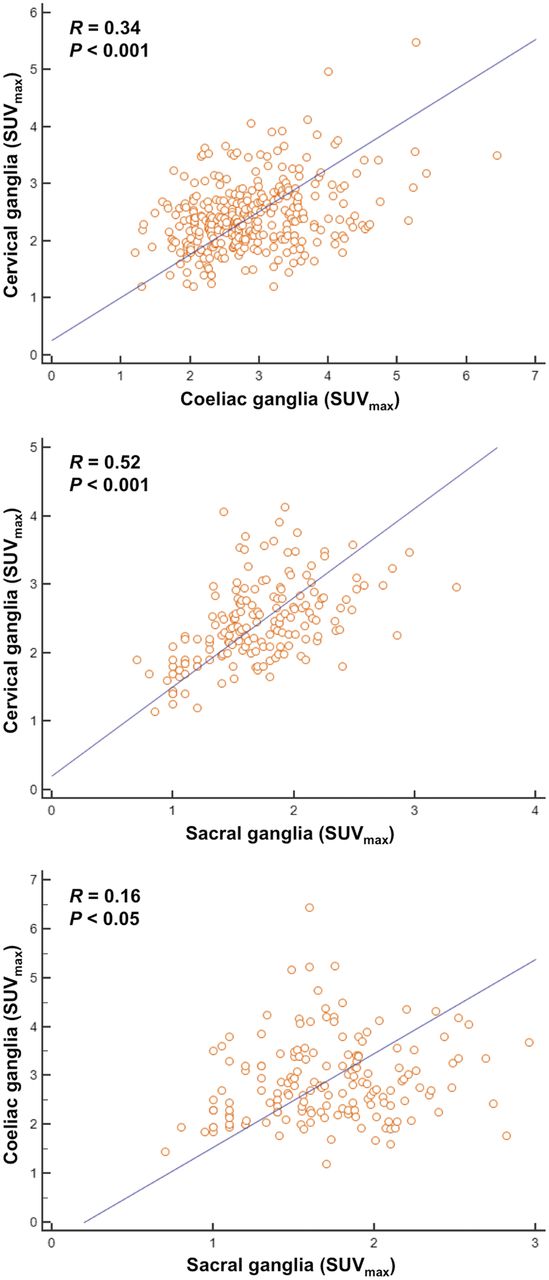
68Ga-PSMA-ligand uptake in ganglia was mostly rated as “mild” or “moderate” and less often as “faint” or “intense” (Fig. 3B). Absolute 68Ga-PSMA-ligand uptake was highest in celiac ganglia followed by cervical and sacral ganglia (celiac mean SUVmax, 2.9 ± 0.8; cervical mean SUVmax, 2.4 ± 0.6; sacral mean SUVmax, 1.7 ± 0.5; P < 0.0001 for all pairs) (Fig. 3C). There was a weak to moderate but significant correlation of 68Ga-PSMA-ligand uptake between different ganglia within a patient (cervical vs. celiac [n = 327]: r = 0.34, P < 0.0001; cervical vs. sacral [n = 169]: r = 0.52, P < 0.0001; and celiac vs. sacral [n = 163]: r = 0.16, P < 0.05) (Fig. 4).
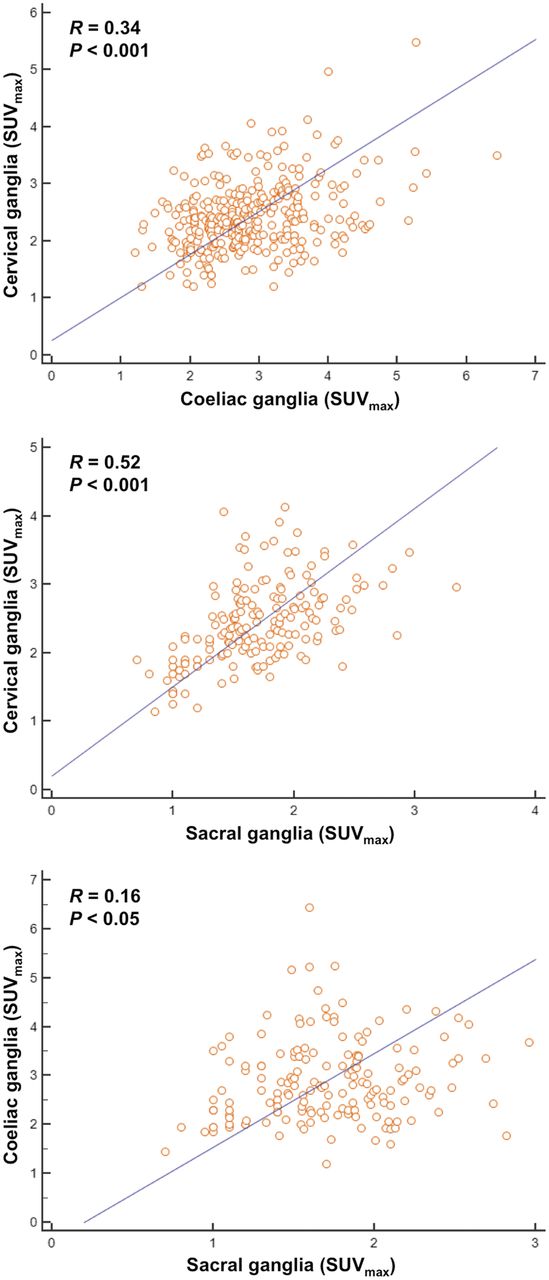
Intrapatient correlation of 68Ga-PSMA-HBED-CC uptake in cervical (top), celiac (middle), and sacral (bottom) ganglia, respectively.
Comparison of Anatomic Configuration and Quantitative Uptake Pattern of Ganglia and Adjacent Lymph Node Metastases
On a per-patient basis, 68Ga-PSMA-ligand–positive lymph node metastases in any location (i.e., cervical, celiac, or sacral) were detected in 34.1% (139/407 patients). Grouped by anatomy, local 68Ga-PSMA-ligand–positive lymph nodes metastases were found at a frequency of 7.4% (30/407 patients), 12.5% (51/407 patients), and 27.5% (112/407 patients) near the typical location of cervical, celiac, and sacral ganglia, respectively. Frequencies between the occurrence of 68Ga-PSMA-positive ganglia and lymph node metastases were different for any and each separate location (P < 0.0001). 68Ga-PSMA-ligand uptake in lymph node metastases was significantly higher than in ganglia for cervical, celiac, and sacral locations (cervical [n = 28]: 18.3 ± 16.8 vs. 2.6 ± 0.7, P < 0.0001; celiac [n = 44]: 12.0 ± 10.6 vs. 2.9 ± 0.8, P < 0.0001; sacral [n = 54]: 14.6 ± 12.8 vs. 1.8 ± 0.4, P < 0.0001) (Fig. 5B).

68Ga-PSMA expression and 68Ga-PSMA-HBED-CC uptake in sympathetic ganglia and lymph node metastases. (A) Examples of immunhistochemical staining for 68Ga-PSMA in ganglia. (B) Comparison of 68Ga-PSMA-HBED-CC uptake in ganglia and adjacent lymph node metastases. Red arrows indicate 68Ga-PSMA expression in ganglia. *P < 0.0001. Mets = metastases.
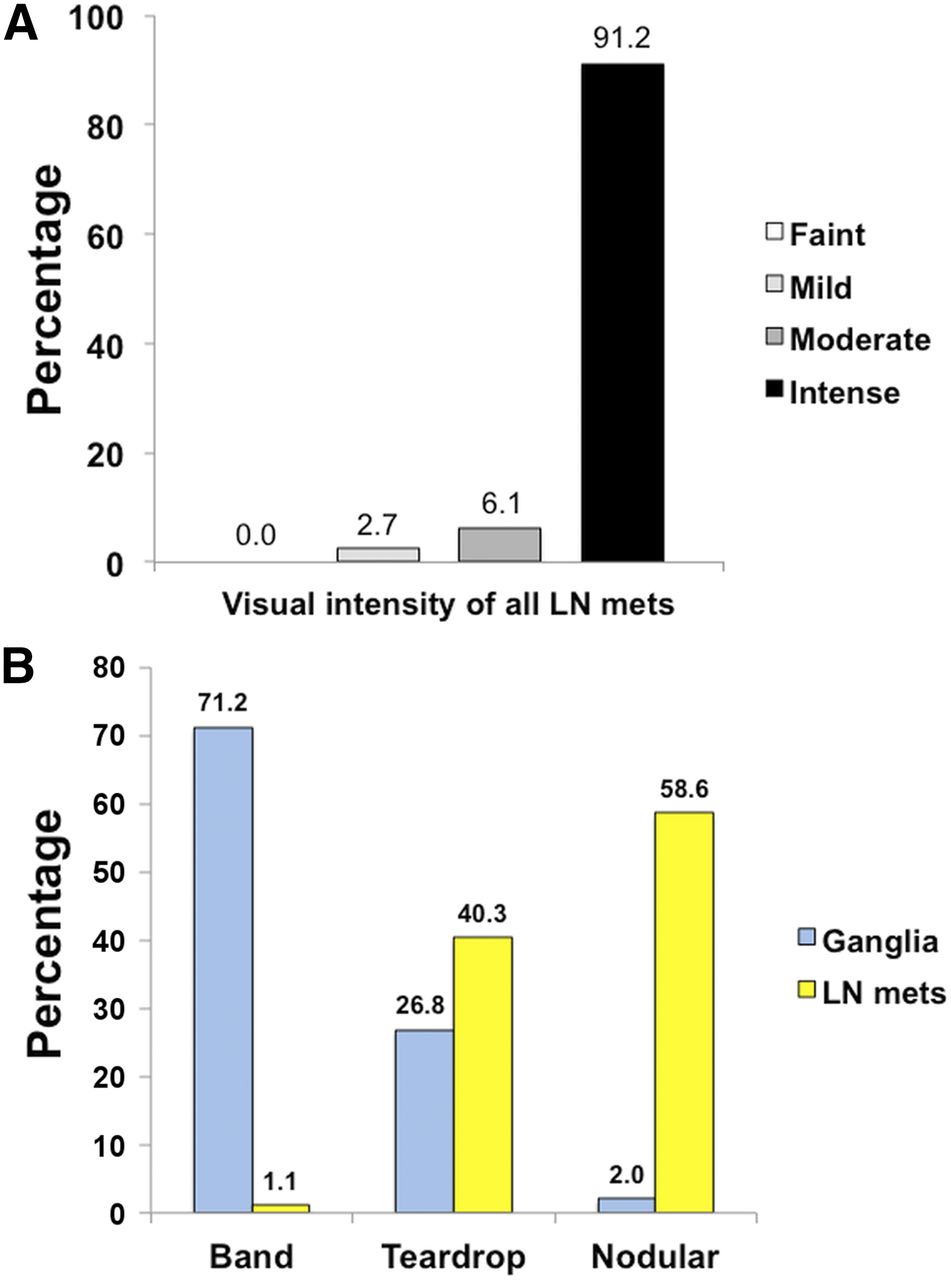
Furthermore, substantial differences in the anatomic configuration of ganglia compared with (adjacent) lymph node metastases were found. Ganglia predominantly exhibited a band-shaped configuration (all ganglia: 71.2%; cervical: 57.5%; celiac: 81.3%; sacral: 81.1%), followed by a teardrop (all ganglia: 26.8%; cervical: 38.5%; celiac: 18.1%; sacral: 18.5%) and only rarely a nodular configuration (all ganglia: 2.0%; cervical: 4.0%; celiac: 0.6%; sacral: 0.4%). Conversely, lymph node metastases were only rarely band-shaped (all lymph node metastases: 1.1%; cervical: 1.7%; celiac: 1.7%; sacral: 0.5%) but more often showed teardrop (all lymph node metastases: 40.3%; cervical: 39.7%; celiac: 47.9%; sacral: 35.9%) or nodular appearance (all lymph node metastases: 58.6%; cervical: 58.6%; celiac: 50.4%; sacral: 63.6%) (P < 0.00001; Fig. 6).

68Ga-PSMA-HBED-CC uptake of lymph node metastases and configuration of sympathetic ganglia and adjacent lymph node metastases. (A) Distribution of visual uptake intensities of lymph node metastases adjacent to sympathetic ganglia. (B) Configuration of sympathetic ganglia and adjacent lymph node metastases. LN = lymph node; mets = metastases.
In a small number of patients with extensive surgery, immunhistochemical staining for 68Ga-PSMA expression in sympathetic ganglia was performed (Fig. 5A). 68Ga-PSMA expression was visually clearly more intense in lymph node metastases in comparison to sympathetic ganglia.
DISCUSSION
Recently, 68Ga-PSMA PET has grown rapidly, and more and more centers worldwide offer this promising imaging modality for staging and restaging of prostate cancer (2). With the increasing number of scanned patients and the growing distribution of 68Ga-PSMA PET, nuclear medicine physicians and radiologists need to become familiar with pearls and pitfalls of this imaging modality (19). Several malignancies and also benign structures that exhibit an elevated 68Ga-PSMA expression have already been described (1,6–14).
In this retrospective analysis, we investigated in detail the 68Ga-PSMA-ligand uptake in ganglia of the sympathetic trunk using 68Ga-PSMA-HBED-CC PET/CT and compared these findings and parameters with the most often confounding structure, namely adjacent lymph node metastases. To the best of our knowledge, our study represents the largest cohort analyzing 68Ga-PSMA-ligand uptake using 68Ga-PSMA-HBED-CC in ganglia so far. Furthermore, we investigated the 68Ga-PSMA-ligand uptake patterns at different locations (cervical, celiac, and sacral) and found that the intensity of 68Ga-PSMA-ligand uptake is a patient-related phenomenon. Last, as a novelty we performed a systematic comparison of the different sympathetic ganglia and adjacent lymph node metastases and demonstrated that 68Ga-PSMA-ligand uptake is higher in lymph node metastases and that lymph node metastases show a clearly different configuration in comparison to sympathetic ganglia.
For an inexperienced reader, 68Ga-PSMA-ligand uptake in cervical, celiac, or sacral ganglia may be misinterpreted as pathologic 68Ga-PSMA expression in soft-tissue structures, particularly lymph node metastases, which in turn may result in debilitating, therapeutic consequences for the patient. For instance, misinterpretation of ganglia as distant lymph node metastases in the case of primary staging may result in systemic medical (antihormonal therapy combined with chemotherapy) versus curative surgical treatment.
In general, the number, location, and appearance of ganglia described in the present study is in line with previously published reports, in which 68Ga-PSMA-ligand PET/CT or CT was used (15,20,21). More specifically, we were able to demonstrate that 68Ga-PSMA-ligand uptake assessed by 68Ga-PSMA-HBED-CC PET is highest in celiac ganglia, followed by cervical and sacral ganglia. Despite this fact, 68Ga-PSMA PET–positive cervical and celiac ganglia were found at a similar frequency, most likely because background surrounding cervical ganglia is lower than in the celiac region. Notably, however, lymph node metastases in the cervical region are rather untypical; challenges to discriminate ganglia from lymph node metastases occur only very rarely. Furthermore, we showed that the 68Ga-PSMA expression in ganglia of the sympathetic trunk is a patient-related phenomenon—that is, if a patient exhibits a high 68Ga-PSMA-ligand uptake in one ganglia it is likely that the other ganglia also show an increased 68Ga-PSMA expression—a finding that may help in the differentiation of 68Ga-PSMA-ligand uptake in ganglia versus 68Ga-PSMA-ligand uptake in adjacent lymph node metastases. The frequency reported in our analysis is slightly different than that in a recent publication reporting on peripheral ganglia seen on 18F-DCFPyL PET/CT imaging (22). One might expect higher numbers for 68Ga-PSMA-ligand PET–positive ganglia when using 18F-labeled compounds (the lower positron range of 18F may lead to a higher local circumscribed uptake). Comparison with current data in the literature does not back this hypothesis so far. However, differences between 18F- and 68Ga-labeled 68Ga-PSMA agents regarding affinity, internalization, and retention as well as local imaging techniques (e.g., injected dose, time between injection and imaging, emission time) might explain these variations. In addition, different scanner types, especially the emergence of digital PET techniques, might have substantial impact. So far, however, no studies directly comparing different PET scanners regarding 68Ga-PSMA-ligand PET positivity of ganglia are available. Nevertheless, in principle, our results confirm that 68Ga-PSMA-ligand uptake in sympathetic ganglia is a frequent observation also when using 68Ga-PSMA-HBED-CC PET imaging.
In addition to the aforementioned recent publication, we also investigated and compared quantitative uptake as well as anatomic configuration of these ganglia compared with adjacent lymph node metastases. We demonstrated that the intensity of 68Ga-PSMA-ligand uptake in lymph node metastases is significantly higher than in sympathetic ganglia. This is not unexpected given the usual high 68Ga-PSMA expression of prostate cancer and its metastases compared with neurogenic tissue. In addition, the anatomic configuration assessed by CT is an important parameter, which may help in the differentiation of these 2 structures, because ganglia are more often band- and teardrop-shaped as opposed to lymph node metastases presenting with a nodular configuration. However, in the case of a 68Ga-PSMA-ligand–positive teardrop-shaped structure the reader should not only rely on configuration but also consider additional features such as exact localization and intensity of radiotracer uptake. Nevertheless, we are convinced that both factors—configuration and intensity of 68Ga-PSMA-ligand uptake—might aid the clinician in discriminating ganglia from adjacent lymph node metastases with relative high certainty. Notably, because size is not a reliable criterion to identify lymph node metastases (demonstrated by various studies using 68Ga-PSMA-ligand PET (4)), the size of lymph nodes and ganglia were not assessed in our study.
This study has some limitations. The definition of ganglia and lymph node metastasis was based on characteristic imaging features only, such as typical anatomic location. However, because for ethical and practical reasons biopsies are only rarely obtained in metastatic prostate cancer, no histologic validation was possible. Nevertheless, we present immunohistochemical slices demonstrating 68Ga-PSMA positivity of sympathetic ganglia, and there is accumulating evidence that false-positive findings in 68Ga-PSMA PET is very low (23,24). In addition, on the basis of thorough review and experience of our readers, this approach seems reasonable. Finally, our study is of retrospective nature and only included patients who underwent a diagnostic CT within the hybrid PET/CT examination.
CONCLUSION
68Ga-PSMA-ligand uptake in sympathetic ganglia is a very common and important pitfall using 68Ga-PSMA-HBED-CC. However, on the basis of different anatomic configuration and uptake characteristics (intensity and intraindividual correlation of uptake), differentiation from possible adjacent lymph node metastases should be easily accomplishable.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Jan. 25, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 6, 2017.
- Accepted for publication January 4, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 68Ga-FAPI PET/CT Interobserver Agreement on Tumor Assessment: An International Multicenter Prospective Study
- Pitfalls and Common Findings in 68Ga-FAPI PET: A Pictorial Analysis
- Radionuclide Therapy in Prostate Cancer: From Standalone to Combination PSMA Theranostics
- Comparison of 3 Interpretation Criteria for 68Ga-PSMA11 PET Based on Inter- and Intrareader Agreement
- Total-Body 68Ga-PSMA-11 PET/CT for Bone Metastasis Detection in Prostate Cancer Patients: Potential Impact on Bone Scan Guidelines
- Matched-Pair Comparison of 68Ga-PSMA-11 PET/CT and 18F-PSMA-1007 PET/CT: Frequency of Pitfalls and Detection Efficacy in Biochemical Recurrence After Radical Prostatectomy
- Novel Structured Reporting Systems for Theranostic Radiotracers
- Synthesis and Preclinical Characterization of the PSMA-Targeted Hybrid Tracer PSMA-I&F for Nuclear and Fluorescence Imaging of Prostate Cancer
- Interobserver Agreement for the Standardized Reporting System PSMA-RADS 1.0 on 18F-DCFPyL PET/CT Imaging