


Abstract
Meningiomas express members of the somatostatin receptor family. The present study assessed the long-term benefits and harm of somatostatin-based radiopeptide therapy in meningioma patients. Methods: Patients with progressive unresectable meningioma were treated with 90Y-DOTATOC and 177Lu-DOTATOC until tumor progression or permanent toxicity occurred. Multivariable Cox regression analyses were used to study predictors of survival. Results: Overall, 74 treatment cycles were performed on 34 patients. Stable disease was achieved in 23 patients. Severe hematotoxicity occurred in 3 patients, and severe renal toxicity in 1 patient. Mean survival was 8.6 y from the time of recruitment. Stable disease after treatment (hazard ratio, 0.017 vs. progressive disease; 95% confidence interval, 0.001–0.35; n = 34; P = 0.01) and high tumor uptake (hazard ratio, 0.046 vs. intermediate or low tumor uptake; 95% confidence interval, 0.004–0.63; n = 34; P = 0.019) were associated with longer survival. Conclusion: 90Y-DOTATOC and 177Lu-DOTATOC are promising tools for treating progressive unresectable meningioma, especially in cases of high tracer uptake in the tumor.
Meningiomas are the most common intracranial extraaxial neoplasms, accounting for approximately 30% of central nervous system tumors in adults. Although usually asymptomatic, meningiomas can be associated with seizures, headaches, vision loss, or focal neurologic deficits depending on their intracranial location (1). About 80% of meningiomas are benign (World Health Organization [WHO] grade I) and are considered curable with gross total resection. The remaining 20% of meningiomas are atypical (WHO grade II) or anaplastic (WHO grade III) and demonstrate malignant potential, significantly higher recurrence rates, and shorter median survival.
The treatment strategy is based on tumor grade, size, and location. Locations near vital structures, especially in the skull base, represent a major therapeutic challenge. Overall, less than 50% of newly diagnosed meningiomas are fully resectable. The therapeutic options in these cases are currently limited.
Importantly, meningioma cells express members of the somatostatin receptor family (2), which provided rationale for somatostatin receptor–targeted radiopeptide therapy with radiolabeled DOTATOC in patients with progressive meningiomas. Radiolabeled DOTATOC is injected intravenously, binds to the somatostatin receptor on the target cell, and irradiates the tumor via β− emission.
The present study evaluated the long-term outcome after treatment with the somatostatin-based radiopeptides 90Y-DOTATOC and 177Lu-DOTATOC in patients with unresectable progressive meningioma.
MATERIALS AND METHODS
Patients
Eligibility was screened at the University Hospital Basel, Switzerland. Patients were eligible if they met the following criteria: histologically confirmed meningioma, disease progression within 12 mo before study entry, and visible tumor uptake on pretherapeutic octreotide scintigraphy. Patients were excluded if they met one of the following criteria: concurrent antitumor treatment other than somatostatin analogs, pregnancy, breastfeeding, urinary incontinence, preexisting grade 3 or 4 hematologic toxicity, or severe concomitant illness, including severe psychiatric disorders. Initial staging and eligibility were based on CT and MR imaging and clinical results from the referring centers.
All patients were prospectively recruited into this study, which was designed and performed in accordance with good clinical practice guidelines, Swiss drug laws, and the Declaration of Helsinki. The study was approved by the local ethics committee for human studies (EKBB reference number M120/97; www.ekbb.ch). Written informed consent was obtained from all participants or their legal representatives. The current results represent a post hoc analysis of the long-term data on safety and efficacy.
Test Drug
90Y-DOTATOC was the standard treatment from 1997 to 2001 (3). Combined treatment with 90Y-DOTATOC plus 177Lu-DOTATOC became standard treatment after 2001; after 2001, patients with reduced baseline kidney function preferably received 177Lu-DOTATOC alone (4,5).
DOTATOC was synthesized as previously described (6) or was purchased from Bachem AG. Radiolabeling was performed using lyophilized kits containing, for example, 220 μg of DOTATOC, 8 mg of gentisic acid, and sodium acetate buffer (0.4 M, pH 5.5 after reconstitution). A total of 7.4 GBq (200 mCi) of 90Y (Perkin Elmer) and 111 MBq (3 mCi) of 111In (Mallinckrodt) solution (both in 0.1 M HCl) were added to the lyophilized kit followed by heating to 95°C for 30 min. Alternatively, 7.4 GBq of 177Lu (0.1 M HCl; IDB Holland bv) were added to the lyophilized kit followed by heating as described above.
Quality control was performed using reverse-phase high-performance liquid chromatography on a Phenomenex Jupiter C18 5 μm, 250 × 4.6 mm column (eluents, A = 0.1% trifluoroacetic acid and B = acetonitrile; flow, 0.75 mL/min; gradient, 0–25 min; 95%–50% A). Labeling yields were greater than 99.5%. Amino acid solutions containing lysine and arginine were administered before and after radiopeptide injection to inhibit tubular reabsorption (7–9).
Intervention
Patients were hospitalized 3 d for each cycle, in accordance with the Swiss requirements for legal radiation protection. Long-acting somatostatin analogs were withheld for at least 6 wk and short-acting somatostatin analogs for at least 3 d before radiopeptide therapy. On the basis of the results of our pilot study (10), repeated treatment cycles were performed with a minimum interval of 6 wk in cases of stabilization or decrease in the longest diameter of all pretherapeutically detected tumor lesions or any clinical improvement, such as pain relief or improvement of visual symptoms.
There was no a priori defined upper limit to the number of treatment cycles. Further cycles were withheld if there was progression, permanent toxicity, loss of the ability to travel to the treatment center, or refusal of further treatment.
Somatostatin Receptor Imaging
Tumor uptake and intratherapeutic biodistribution of the radiopeptide were assessed using planar whole-body imaging 24 h after injection of radiolabeled DOTATOC. The maximum tracer accumulation in the tumor was scored by a panel of 3 board-certified nuclear medicine physicians using a 4-point scale: no uptake (score 0), uptake lower than liver uptake (score 1), uptake similar to liver uptake (score 2), and uptake higher than liver uptake (score 3). The interpreters were masked to patient baseline data (including sex, age, histology, duration of disease, and pretreatment) and all follow-up results (including response, toxicity, and survival).
Follow-up
During hospitalization, clinical status and vital signs were monitored before and for 72 h after each therapeutic cycle. All toxicity was continuously recorded. After discharge, blood chemistry and hematologic parameters were measured at biweekly intervals for 10 wk after each cycle or until normalization of marker levels. Follow-up was performed to obtain information on survival and long-term toxicity until the patient’s death. Follow-up data were obtained from the referring centers, with a minimum frequency of 2 follow-up visits per year, adapted to the patient’s individual requirements.
All follow-up data were centrally collected, and each case was reviewed and approved for completeness at the study center. Family physicians and the patients were directly contacted if additional follow-up results were needed.
Acute and long-term adverse events were graded according to the Common Terminology Criteria for Adverse Events, version 3.0 (11), of the National Cancer Institute. Kidney function was assessed using the Modification of Diet in Renal Disease formula (12). Renal toxicity was classified according to the guidelines of the National Kidney Foundation (www.kidney.org), where grade 4 and 5 renal toxicity is defined as a glomerular filtration rate of less than 30 and less than 15 mL/min/1.73 m2, respectively.
Outcomes and Statistical Analyses
The main outcomes of interest were survival, response, and toxicity. Survival was assessed from the time of diagnosis and the time of first radiopeptide treatment to death from any cause. Predictors of survival were studied by multivariable Cox regression with the following candidate variables: high tumor uptake (uptake score 3 vs. score 1 or 2), sex (male vs. female), age, and response (stable disease vs. disease progression). Disease progression was defined as an at least 20% increase in the sum of the longest diameters of target lesions or the appearance of one or more new lesions or unequivocal progression of existing nontarget lesions, according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1. Effect estimates were expressed as hazard ratios with 95% confidence intervals. The overall response rate was defined following intention-to-treat principles, and loss of follow-up after treatment was regarded as treatment failure.
Sensitivity analyses were performed to compare overall survival, survival predictors, and toxicity in all patients and patients treated with 90Y-DOTATOC alone. Further sensitivity analyses assessed the influence of WHO grade on survival after enrollment. Two-sided P values of less than 0.05 were considered to indicate statistical significance.
RESULTS
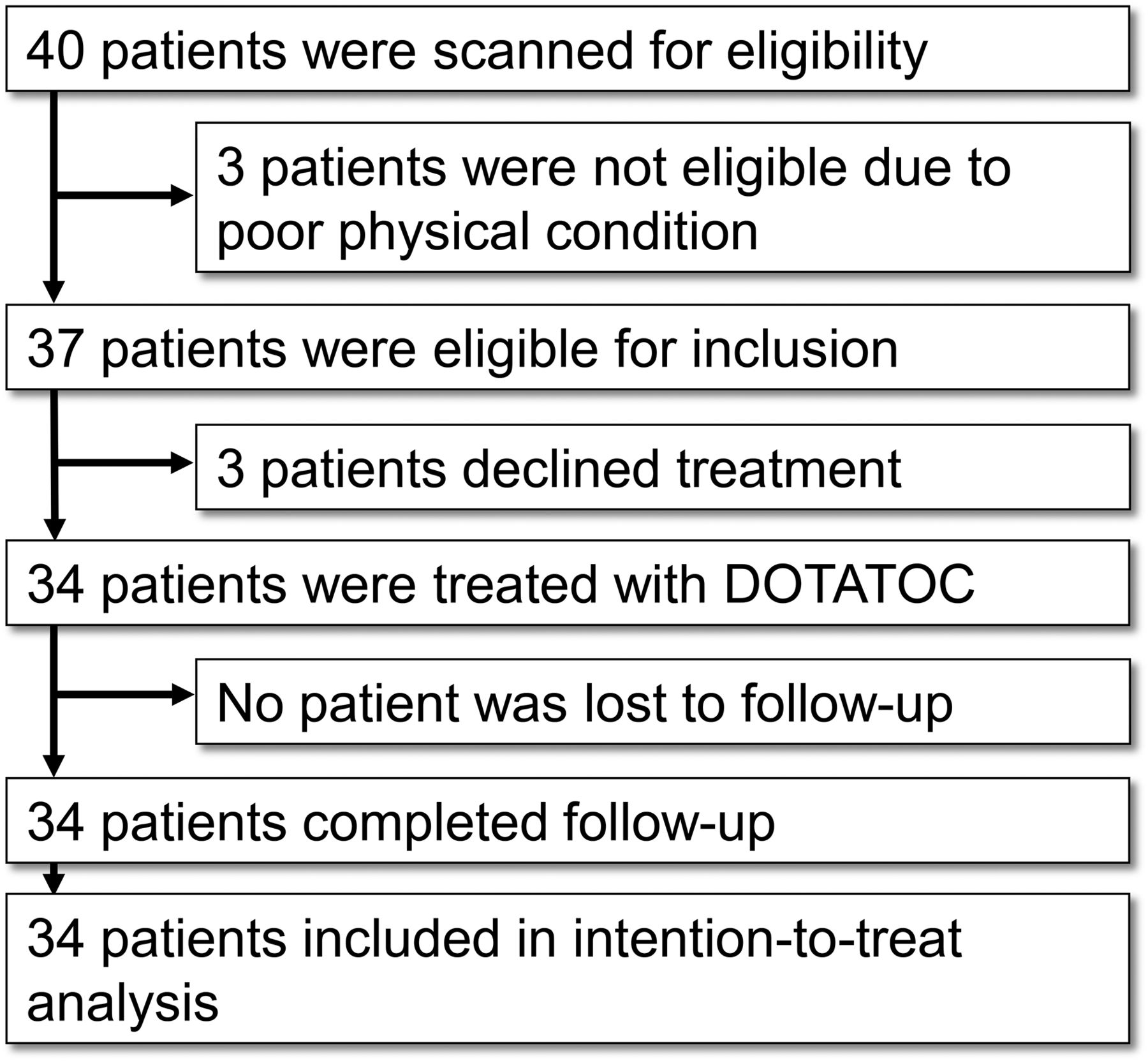
Between October 1998 and September 2010, 40 patients with progressive meningioma were screened for eligibility. Of these, 3 patients (7.5%) were not eligible because of poor physical condition and 3 patients (7.5%) chose other treatment options (Fig. 1). The remaining 34 patients (85%) were recruited. Patients were enrolled from Europe and North America; their baseline characteristics are presented in Table 1.

Trial profile.
Patients’ Baseline Characteristics
Intervention
In total, 74 treatment cycles (1–4 cycles per patient) were performed, including 66 cycles of 90Y-DOTATOC (range, 1.5–18.3 GBq) and 8 cycles of 177Lu-DOTATOC (range, 7.4–22.2 GBq). Intratherapeutic scintigraphy revealed grade 3 visual tumor uptake in 14 patients, grade 2 in 12 patients, and grade 1 in 8 patients. Stable disease was achieved in 23 patients (65.6%), whereas progressive disease was found in 11 patients (34.4%).
Toxicity
During follow-up, 23 patients (67.6%) developed hematotoxicity, grade 1 (16 patients, 47.1%), grade 2 (4 patients, 11.8%), or grade 3 (3 patients, 8.8%). Grade 4 hematotoxicity did not occur. The detailed list of all detected hematotoxicity is presented in Table 2. Sensitivity analyses revealed similar hematotoxicity in patients treated with 90Y-DOTATOC alone. One patient (2.9%) developed renal toxicity (grade 4).
Hematologic Toxicity (n = 34)
Survival
After a median follow-up period of 21.8 mo (range, 1.0–137.4 mo), 8 patients (23.5%) had died and 26 patients (76.5%) had survived. No patient was lost to follow-up. The mean survival was 27.0 y from the time of diagnosis (Fig. 2A) and 8.6 y from the time of recruitment (Fig. 2B).

Survival after DOTATOC in progressive meningioma (n = 34). (A) Kaplan–Meier plot demonstrating probability of survival from time of diagnosis. Mean survival is indicated by vertical bar. (B) Kaplan–Meier plot demonstrating probability of survival from time of treatment. Mean survival is indicated by vertical bar. (C) Cox regression plot demonstrating posttreatment probability of survival in patients with stable versus progressive disease (n = 34, P = 0.01, Cox regression analysis). (D) Kaplan–Meier plot of sensitivity analysis demonstrating probability of survival in patients with meningioma grade 1 (n = 5), grade 2 (n = 6), and grade 3 (n = 3, P = 0.34, Mantel–Cox log rank test).
Longer survival was found in patients with stable disease than in patients with progressive disease after treatment (mean survival, 9.6 y vs. 4.7 y; hazard ratio, 0.017; 95% confidence interval, 0.001–0.35; n = 34; P = 0.01; Cox regression analysis; Fig. 2C).
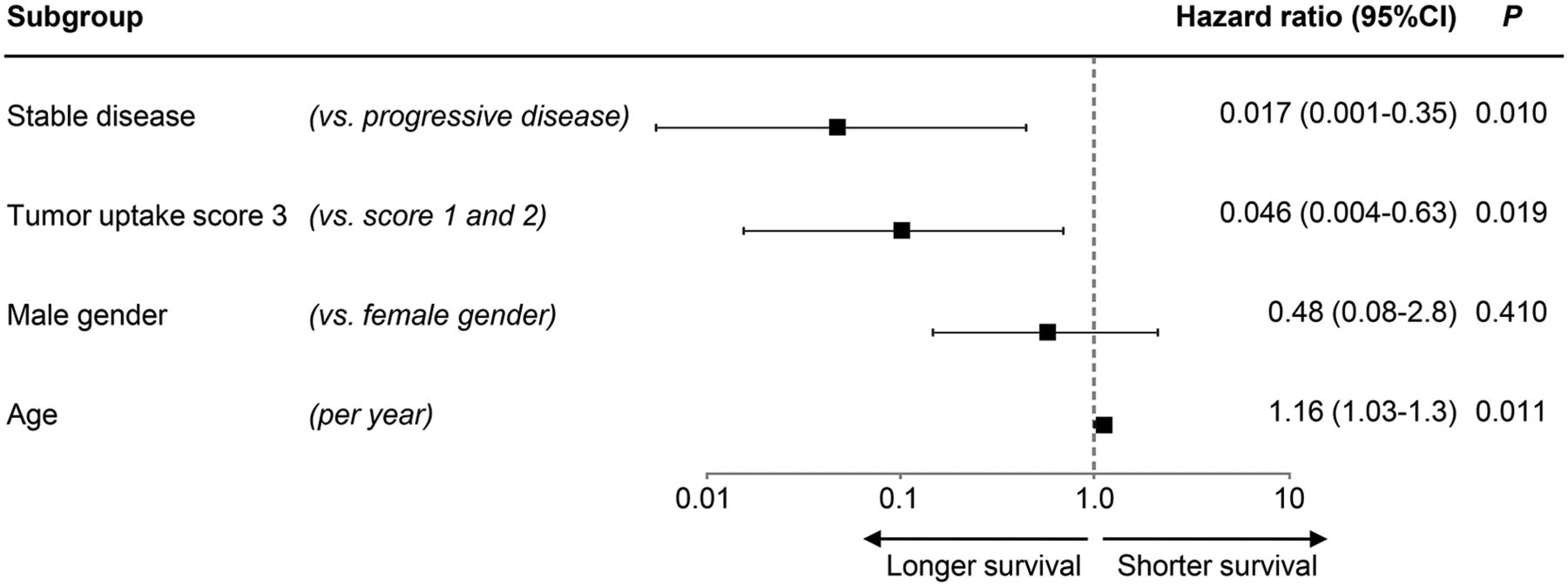
The effects of all relevant predictors on survival after treatment are listed in Figure 3. Sensitivity analyses revealed similar results for survival predictors in patients treated with 90Y-DOTATOC alone compared with all patients. Sensitivity analyses in all cases with a known WHO grade revealed a trend toward longer survival in patients with low-grade meningioma (n = 14, P = 0.34, Mantel-Cox log rank test, Fig. 2D).

Predictors of survival (n = 34). Forest plot demonstrates results of multivariable Cox regression with covariable response, tumor uptake, sex, and age. Effect estimates are expressed as hazard ratio with 95% confidence interval (CI).
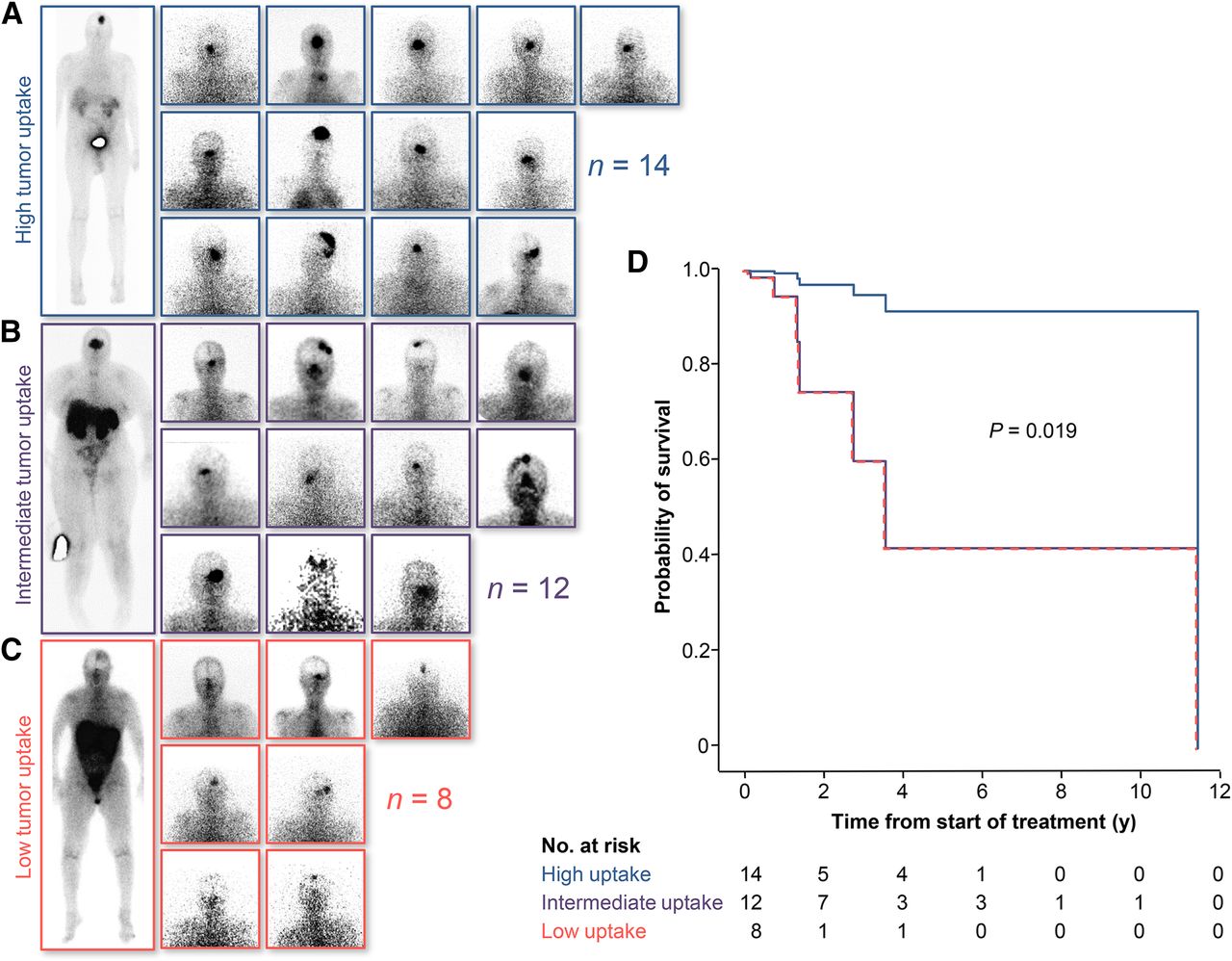
Finally, longer survival was found in patients with high tumor uptake of the radiopeptide than in patients with intermediate or low tumor uptake (hazard ratio, 0.046; 95% confidence interval, 0.004–0.63; n = 34; P = 0.019; Cox regression analysis; Fig. 4).

Influence of DOTATOC uptake on survival after treatment (n = 34). (A–C) Intratherapeutic scanning reveals meningioma DOTATOC uptake higher than liver uptake (n = 14, A), equal to liver uptake (n = 12, B) and lower than liver uptake (n = 8, C). (D) Cox regression plot demonstrates survival of patients with meningioma showing high uptake (n = 14) vs. low uptake (n = 20, P = 0.019, Cox regression analysis).
DISCUSSION
The present study suggests that somatostatin receptor–targeted radiopeptide therapy can achieve disease stabilization in most patients with progressive unresectable meningioma. Moreover, uptake of the radiopeptide during treatment and disease stabilization after treatment were significant predictors for overall survival after somatostatin receptor–targeted radiopeptide therapy.
To our knowledge, this is the largest study available to date on somatostatin receptor–targeted radiopeptide therapy in patients with progressive unresectable meningioma. Importantly, this study collected the longest follow-up data, which were sufficient to report significant results on predictors of survival in meningioma patients after somatostatin receptor–targeted radiopeptide therapy.
The study has several strengths and limitations. The single-center design provided a standardized protocol for 90Y-DOTATOC and 177Lu-DOTATOC therapy in all patients. The dosing protocols for 90Y and 177Lu were chosen according to established standards from the largest trials on somatostatin receptor–targeted radiopeptide therapy with 90Y and 177Lu (3–5,13). However, these standard doses are known to have different therapeutic efficacies (14,15).
Patients were referred for treatment from North America and all over Europe. They were accepted for treatment if disease progression was documented and all other treatment options had been exhausted. To provide the treatment as quickly as possible for these patients, biopsy was not required for enrollment if the WHO grade was still undetermined. Thus, analyses were underpowered to demonstrate that WHO grade is a significant predictor for survival after somatostatin receptor–targeted radiopeptide therapy. After failing DOTATOC, several patients received further experimental therapies. However, because of the global recruitment, the complete dataset on these experimental therapies was not available.
Baseline and follow-up imaging was performed in each patient’s home country at the respective referral center, either with CT or MR imaging. This practice was feasible with respect to all referrals from abroad and was sufficient to discriminate stable from progressive disease. However, it did not allow gathering of a complete set of RECIST data, which would be useful to define different grades of treatment response. Yet, morphologic imaging could not detect even a single case of tumor shrinkage in our patients with unresectable progressive meningioma, indicating little potential gain from implementing RECIST. Nevertheless, studies with complete sets of biopsies and RECIST data would be of considerable interest.
So far, several reports have indicated a potential value for somatostatin receptor–targeted radiopeptide imaging in meningioma. However, to our knowledge, only one study has reported somatostatin receptor–targeted radiopeptide therapy in meningioma, and that study showed that 90Y-DOTATOC achieved disease stabilization in 66%; progressive disease was observed in the remaining 34% (16).
The present study confirms the efficacy and safety results of this previous report and provides analyses on predictors of survival. In addition, the present study found results on hematotoxicity and renal adverse events in line with previous reports on somatostatin-based radiopeptide therapy with 90Y-DOTATOC and 177Lu-DOTATOC in progressive neuroendocrine tumors (3,4,17).
Comparisons of the outcome of DOTATOC treatment and other treatment modalities would be highly warranted. These are limited mainly by the fact that only few studies report long-term survival data comparable to the present report. A recent study investigated survival in 12,284 meningioma patients under various treatment regimes (18). Similar to our study, biopsy results were available for about 50% of patients. This study found survival rates 3 y after diagnosis comparable to those in our cohort; however, a reliable comparison to demonstrate a potential superiority of DOTATOC therapy was not feasible.
Somatostatin-based radiopeptide therapy with 90Y-DOTATOC and 177Lu-DOTATOC has an established value for treating patients with neuroendocrine tumors (17,19–21). On the basis of the current results, DOTATOC is a relatively safe treatment option that should be considered for patients with progressive nonoperable meningiomas who have failed all other treatment options. Further research, however, is warranted to compare the harm and benefits of other treatment modalities in progressive nonoperable meningiomas.
CONCLUSION
The present study documents the long-term outcome of 90Y-DOTATOC and 177Lu-DOTATOC treatment in a large cohort of patients with progressive nonoperable meningioma. Treatment was well tolerated, disease stabilization was observed in most patients, and intratherapeutic imaging was predictive of survival after treatment. These results suggest that in meningioma patients with a poor prognosis and limited treatment options, DOTATOC is an alternative treatment that has reasonable potential for improving the quality and longevity of life.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We are grateful to our nursing, laboratory, and technical staff for support with patient care, preparation of radiopharmaceuticals, and acquisition of scans.
Footnotes
↵* Contributed equally to this work.
Published online Jan. 15, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 13, 2014.
- Accepted for publication December 8, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Meningioma: Molecular Updates from the 2021 World Health Organization Classification of CNS Tumors and Imaging Correlates
- Intraarterial Administration of Peptide Receptor Radionuclide Therapy in Patients with Advanced Meningioma: Initial Safety and Efficacy
- Radiolabeled Somatostatin Receptor Antagonist Versus Agonist for Peptide Receptor Radionuclide Therapy in Patients with Therapy-Resistant Meningioma: PROMENADE Phase 0 Study
- Somatostatin Receptor-Targeted Radiopeptide Therapy in Treatment-Refractory Meningioma: Individual Patient Data Meta-analysis
- Upregulation of Key Molecules for Targeted Imaging and Therapy
- Somatostatin Receptor-Targeted Radiopeptide Therapy in Patients with Progressive Unresectable Meningioma
- Reply: Somatostatin Receptor-Targeted Radiopeptide Therapy in Patients with Progressive Unresectable Meningioma