


Abstract
81mKr is widely used as a ventilation agent to diagnose pulmonary embolism (PE). However, 81mKr is expensive, which limits its continuous availability. Technegas can be an alternative ventilation agent with the advantage of being less expensive and available daily. The aim of this study was to compare the value of technegas with that of 81mKr in the detection of PE. Methods: Ninety-two consecutive patients (29 men; mean ± SD, 53 ± 17 y old) with at least one segmental perfusion defect (Hull criteria) were studied prospectively. Perfusion and ventilation (V/Q) lung scintigraphy with both technegas and 81mKr were performed within 24 h on all patients. V/Q lung scan results were classified as high probability for PE (normal ventilation study) or nondiagnostic (abnormal ventilation study). All V/Q lung scans were read by two experienced nuclear physicians in consensus. For the intra- and interobserver variabilities, two experienced observers independently read the V/Q lung scans. Results: 81mKr and technegas showed a good agreement (κ, 0.68; 95% confidence interval [CI], 0.53–0.82). However, technegas significantly increased the number of nondiagnostic V/Q lung scans (P = 0.035). In 15 patients, a discrepancy was found between 81mKr and technegas. False-positive V/Q lung scan results occurred in 4 of 12 patients (33%) with 81mKr and in 2 of 3 patients (66%) with technegas. The intra- and interobserver variabilities were 0.71–0.88 (95% CI, 0.56–1.0) for perfusion/81mKr and 0.74–0.96 (95% CI, 0.58–1.0) for perfusion/technegas. Conclusion: In comparison with 81mKr, technegas does not result in more false-positive V/Q lung scan results. The use of technegas, however, increases the number of nondiagnostic V/Q lung scan results, which would increase the demand for further additional testing to confirm or refute PE.
Pulmonary embolism (PE) is a frequently occurring disease that, in addition to its treatment with anticoagulants, has both a high morbidity and mortality (1,2). Because the clinical presentation of PE is nonspecific, objective diagnostic testing is necessary to establish a definite diagnosis (3,4). Pulmonary angiography is generally regarded as the gold standard in diagnosing PE, but its invasiveness and limited availability hamper its use as the initial test of choice. Instead, perfusion scintigraphy is usually considered the optimal first diagnostic test in patients with clinically suspected PE because this technique is safe, noninvasive, and highly sensitive (5,6). However, the specificity of the perfusion scan alone is low because various diseases that clinically mimic PE may also have perfusion defects. The addition of ventilation scintigraphy enables the further identification of patients with a high probability (>85%) of PE (5,7).
In general, perfusion scans are obtained with 99mTc-labeled macroaggregates of albumin (MAA). For ventilation scintigraphy, various radiopharmaceuticals are currently available, of which 133Xe, 99mTc-labeled aerosols, and 81mKr are most frequently used (in contrast to 99mTc-labeled aerosols, 133Xe and 81mKr are true gases). Because of the low γ energy of 133Xe, ventilation scintigraphy must be performed before perfusion scintigraphy to avoid misinterpretation. Moreover, its significant solubility and relatively long half-life (5.3 d) leads to high and often unnecessary radiation doses for the patient. Finally, the use of 133Xe may introduce errors because of the uptake of tracer in the blood and chest wall.
81mKr, by virtue of its radiophysical characteristics, is often considered to be the reference gas for ventilation scintigraphy (8–10). Its very short half-life (13 s) enables multiple views. The high photon energy (190 keV) allows simultaneous or immediate acquisition of perfusion and ventilation (V/Q) data in multiple and strictly comparable views. Consequently, a relatively short time is required for the procedure and, because 81mKr is not readily soluble, the absorbed radiation dose is low. Unfortunately, the 81Rb generator, from which 81mKr is eluted, has a very short half-life (4.7 h) and is expensive, which limits the continuous availability of 81mKr.
Technegas is a relatively new aerosol that can be used for ventilation scintigraphy. In contrast to the earlier aerosols (e.g., 99mTc–diethylenetriaminepentaacetic acid), technegas is considered to behave truly like a gas, because of the ultrafine dispersion of the 99mTc-labeled carbon particles (<0.2 μm) (11–13). Several investigators have studied the image quality and quantity of deposition of technegas compared with that of various gases such as 133Xe and 81mKr. The results of these studies are contradicting: Some investigators found no differences and others found technegas images to be superior (10,14–16). Most of these studies, however, involved a limited number of patients and lacked a systematic verification of the diagnosis of PE in all patients.
The purpose of this study was to assess the incidence and significance of discrepancies between technegas and 81mKr ventilation images in patients with clinically suspected PE. In addition, the reproducibility of the scintigraphic evaluation of both technegas and 81mKr ventilation images was evaluated.
MATERIALS AND METHODS
The data reported here are from the Advances in New Technologies Evaluating the Localization of Pulmonary Embolism (ANTELOPE) study, performed from May 1997 through March 1998 in six teaching hospitals. For the purpose of this study, we used only the data of the three centers that performed both 81mKr and technegas ventilation scintigraphy.
All patients with a clinical suspicion of PE and for whom a request for V/Q lung scintigraphy was made were considered for study entry. The eligible study population consisted of both in- and outpatients, ≥18 y old who were not pregnant, did not have an indication for thrombolytic therapy, and in whom objective examinations for diagnosing venothrombotic disease according to patient’s current symptoms had not been made previously. The study was designed as an “intention to diagnose” study, which means that patients with contraindications for spiral CT angiography or conventional pulmonary angiography (or both) were not excluded from participation in the study. The institutional review boards of all participating centers approved the study, and informed consent was obtained from all patients enrolled in the study.
Study Protocol
The attending physicians were asked to give a probability estimate for PE on the basis of evaluation of the clinical history, physical examination, chest radiography, electrocardiography, and arterial blood gas before further objective testing was done. Within 24 h of referral, the patients gave a detailed clinical history and had a physical examination, chest radiography, electrocardiography, venous duplex sonography of the lower extremities, D-dimer testing, and perfusion scanning. Patients were stratified according to the V/Q lung scan result. If the perfusion scan was normal, no further tests were performed. Ventilation scintigraphy with both 81mKr and technegas was indicated in all patients with at least one segmental perfusion defect. Both studies were performed on the same day or at least within 24 h after the perfusion scan. When >24 h elapsed between the first perfusion scan and one of the ventilation scans, a second perfusion scan was obtained.
Spiral CT angiography was performed on all patients with perfusion defects, irrespective of the size of these defects. All CT scanners used in this study were capable of scanning at least 16 cm (Somatom 6 [Siemens Medical Systems, Erlangen, Germany], Elscint [Elscint, Haifa, Israel], and SR7000 and SR8000 [Philips Medical Systems, Best, The Netherlands]). Scanning was performed during a 32-s single breath hold or during shallow breathing if patients were very dyspneic. The chest was scanned in the caudocranial direction over a 16-cm distance, from the upper level of the diaphragm to a level slightly above the aortic arch (5-mm collimation, pitch of 1, 120 kV, 200–250 mAs). Image acquisition was started 20 s after intravenous injection of iodine (900 mg/s) for 40 s, either by injection of 100 mL nonionic contrast agent with 35% iodine content (Iomeron 350; Bracco Byk Gulden, Konstanz, Germany) at an injection rate of 2.5 mL/s or by injection of 120 mL nonionic contrast agent with 30% iodine content (Ultravist 300; Schering, Berlin, Germany) at an injection rate of 3.0 mL/s. Images were reconstructed every 2 mm. All scans were assessed in cine mode using window width and level in both mediastinal and lung settings.
The criteria of Remy-Jardin et al. (17) were used to establish the presence of PE. The sensitivity and specificity of spiral CT angiography for diagnosing central PE are considered to be high, but the sensitivity is low for diagnosing subsegmental PE (18). Pulmonary angiography was performed in patients with a nondiagnostic 81mKr V/Q lung scan result and in patients with discordance between V/Q lung scintigraphy and spiral CT angiography (high-probability 81mKr V/Q lung scan and a normal spiral CT scan). Complete pulmonary angiography runs and CT image acquisitions were digitally and independently reviewed by two experienced radiologists. If the second radiologist’s reading was in conflict with that of the first, a third radiologist was consulted whose judgement was decisive. In patients with a contraindication for spiral CT angiography or pulmonary angiography (or both), the study protocol was violated. We aimed at performing the complete study protocol within 48 h after the first V/Q lung scan, with a maximum of 24 h between the examinations under study. According to the study protocol, diagnosis of PE was made on the basis of pulmonary angiography, as the strongest source of evidence, or a high-probability 81mKr V/Q lung scan result. A normal perfusion scan or pulmonary angiogram ruled out PE. In all cases, the final diagnosis was established by independent reading of the diagnostic imaging techniques without knowledge of the patient’s history and final diagnosis.
Perfusion Scintigraphy
Perfusion scintigraphy was performed within 24 h after referral using 50 MBq 99mTc-MAA. The tracer was injected intravenously with the patient in the supine position, whereas imaging was performed with the patient in a sitting position. Acquisition was performed in at least four standard projections (anterior, posterior, and right and left posterior oblique) with at least 150 kcts per view (low-energy, high-resolution [LEHR] collimator, 128 × 128 matrix).
81mKr Ventilation Scintigraphy
Ventilation scintigraphy with 81mKr gas was performed either immediately after perfusion scintigraphy (medium-energy, high-resolution collimator, 128 × 128 matrix) or using dual-isotope scanning (LEHR collimator, 128 × 128 matrix). If 81mKr was not available, ventilation scintigraphy was executed the following day or at least within 24 h. Ventilation scanning was performed using the same projections as for perfusion scanning with at least 200 kcts per view.
Technegas Ventilation Scintigraphy
Inhalation and imaging occurred preferably in the sitting position. Technegas ventilation scintigraphy was performed only in combination with 99mTc-MAA perfusion scanning. A counting rate of at least two times the counting rate of the perfusion scan was considered to be technically adequate (400 kcts per view; LEHR collimator, 128 × 128 matrix). Acquisition was performed using the same projections as for 81mKr ventilation scintigraphy.
Ventilation–Perfusion Scintigraphy Assessment
The V/Q lung scans were interpreted three times. The first interpretation was made immediately by the attending nuclear physician with all clinical information available at that time. For the purpose of the ANTELOPE study, a second reading was performed in consensus by two of a panel of experienced nuclear physicians who were unaware of the patient’s history and final diagnosis. The chest radiograph was available on request. Eighteen months later, two experienced observers from that group read all scans again individually. In this study the Hull criteria were used for the assessment of the V/Q lung scan result because these criteria are advised in the Dutch consensus for the diagnosis of PE. The lung scans were interpreted by using a lung segment reference chart (19). According to the Hull criteria, the V/Q lung scan result was categorized into three major groups for the presence of PE: high probability (evidenced by at least one segmental perfusion defect with preserved ventilation), nondiagnostic (all other ventilation–perfusion defects not fulfilling the criteria for high probability), or normal (no perfusion defects) (20). Before the study was begun, a training session was held for all readers who would perform an independent reading to eliminate variations in the assessment.
Comparison of 81mKr and Technegas Ventilation
The consensus reading was used to determine the agreement between technegas and 81mKr ventilation lung scintigraphy. The accuracy of ventilation studies could not be determined in this study because pulmonary angiography was not performed on all patients. Instead, the results of spiral CT angiography and pulmonary angiography are given when available. In addition, the diagnostic performance of 81mKr and technegas V/Q lung scintigraphy was compared. On one occasion, the two observers classified all 81mKr V/Q lung scans of one center into high probability, nondiagnostic, and normal. After at least a 2-wk interval, all V/Q lung scans of these patients were classified again using technegas as the ventilation agent.
Interobserver and Intraobserver Variabilities
The V/Q lung scans with at least one segmental perfusion defect at the consensus reading and ventilation performed with both 81mKr and technegas were used to determine the interobserver variability. The V/Q lung scans of two centers were assessed again for comparison of the intraobserver variability. In addition, a third reading was used to determine the intra- and interobserver variabilities for the indication to perform ventilation scintigraphy (i.e., the presence of at least one segmental perfusion defect). All perfusion scans of one hospital were reread by the two observers. At least a 2-wk interval occurred between the readings and the V/Q lung scans were presented in random order.
Statistics
The agreement between 81mKr and technegas V/Q lung scintigraphy and the inter- and intraobserver variabilities corrected for chance were evaluated with use of the κ statistic. A κ value of 1 corresponds to perfect agreement, 0 to agreement as expected by chance, and −1 to complete disagreement (21). In addition, the McNemar χ2 test was performed. This test indicates whether a systematic difference in interpretation of the lung scan by either physician accounts for possible disagreements. A two-tailed P < 0.05 was considered statistically significant. Statistical analyses were performed with SPSS statistical software (SPSS, Inc, Chicago, IL).
RESULTS
Patient Population
During the course of the study, 693 consecutive patients were referred for clinically suspected PE. Of these, 107 were excluded on the basis of the predefined exclusion criteria (8 were pregnant, 10 were <18 y old, 3 had an indication for thrombolytic therapy, diagnostic tests were already performed in 28, and it was expected that the protocol could not be completed within 48 h in 58 patients or patients were unable to give informed consent). Of the remaining 586 eligible patients, 328 (56%) agreed to participate. The demographic and clinical characteristics of these patients are given in Table 1.
Demographic and Clinical Characteristics of 328 Study Patients with Clinically Suspected PE
Availability of Ventilation Scintigraphy
In 316 of the 328 patients, a final consensus reading was available. On the basis of this reading, 117 patients had a normal perfusion scan, 54 had subsegmental perfusion defects, and 145 had at least one segmental perfusion defect and therefore an indication for ventilation scintigraphy. In 53 of the 145 patients with at least one segmental perfusion defect (on the basis of the consensus reading), technegas ventilation was not performed or was incomplete because of a local interpretation of the perfusion scan defect as subsegmental (n = 27), technical failure of the equipment including an insufficient amount of radiopharmaceutical (n = 8), severe illness (n = 8), withdrawal of informed consent (n = 4), logistic reasons (n = 3), and unknown causes (n = 3). 81mKr ventilation also could not be performed in only one of the eight severely ill patients. As a result, 92 patients were available for comparison of technegas with 81mKr ventilation studies.
Agreement Between 81mKr and Technegas
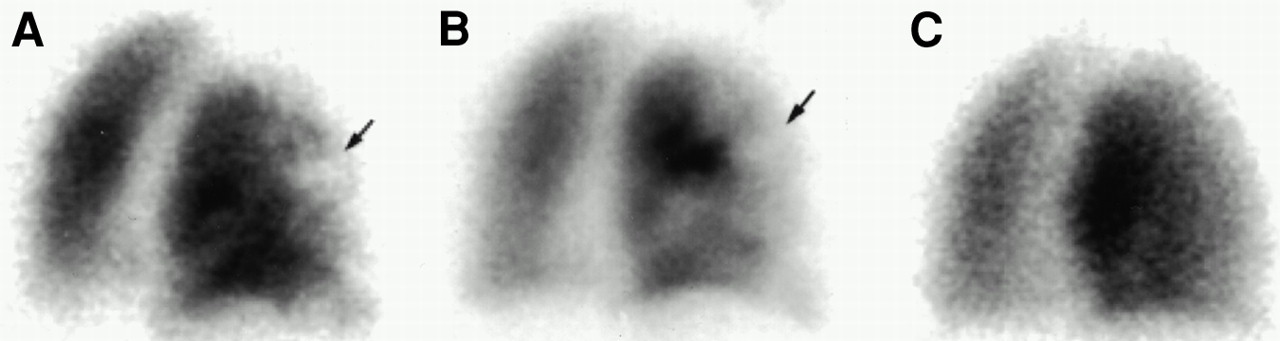
In 84% of the cases assessed by consensus reading, the technegas V/Q lung scan studies were in agreement with the 81mKr V/Q lung scan results (κ, 0.68; 95% confidence interval [CI], 0.53–0.82) (Table 2). The positive McNemar χ2 test indicates a statistically significantly trend toward more nondiagnostic V/Q lung scan results with technegas ventilation. Table 2 also gives the results of pulmonary angiography, if available, and spiral CT angiography, if no pulmonary angiography was available, in relation to the technegas and 81mKr V/Q lung scan results. A discrepancy was evident between the 81mKr and technegas V/Q lung scan results in 15 patients. A definite false-positive V/Q lung scan result (i.e., V/Q lung scan result indicating a high probability for PE and a normal pulmonary angiogram) occurred in 4 of the 12 patients (33%) with 81mKr and in 2 of the 3 patients (66%) with technegas. Pulmonary angiography was negative in 3 of the 40 patients (8%) who had a high-probability 81mKr and technegas V/Q lung scan result. The consensus spiral CT angiography reading was considered negative for PE in 7 additional patients. However, confirmatory angiography had not been performed in these patients, primarily because at local reading the spiral CT scans had been considered positive for PE. An example of a patient who had a nondiagnostic technegas V/Q lung scan result and a 81mKr V/Q lung scan result indicating a high probability for PE is given in Figure 1. The spiral CT angiography result was inconclusive, and the pulmonary angiography result was negative for PE.
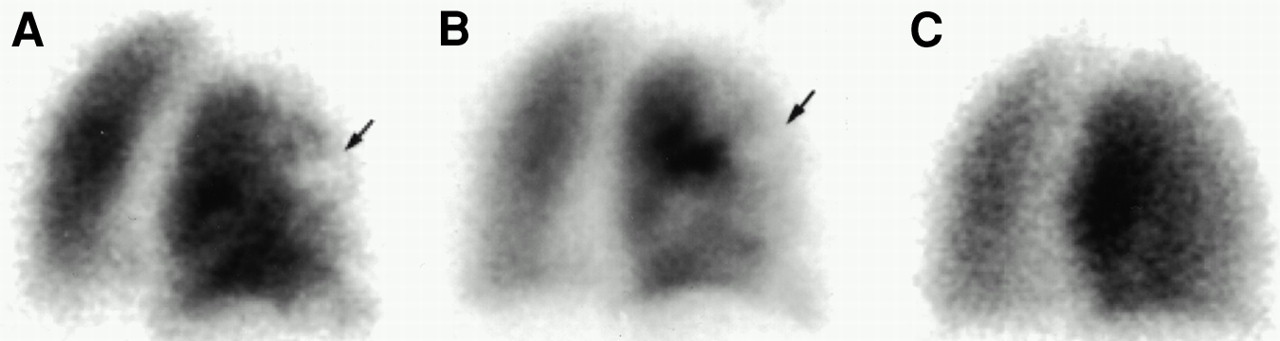
A 50-y-old man with acute dyspnea and pleuritic chest pain. (A) Perfusion scan in right posterior oblique projection shows segmental defect in anterior segment of right upper lobe (arrow). (B and C) Technegas ventilation scan (B) reveals match with perfusion defect (arrow), whereas 81mKr ventilation scan (C) shows complete mismatch. Pulmonary angiography result was negative for PE.
Technegas and 81mKr Ventilation–Perfusion Status in Relation to Spiral CT Angiography (SCTA) and Pulmonary Angiography (PA) Results
The 81mKr and technegas V/Q lung scans of 101 patients were classified into high probability, nondiagnostic, and normal by two observers (Table 3). Although the κs were acceptable, a similar trend toward nondiagnostic technegas V/Q lung scintigraphy was observed (McNemar χ2 test, 0.039 and 0.035).
Comparison of V/Q Scintigraphy with 81mKr vs. Technegas Assessed by Individual Observers
Intraobserver and Interobserver Variabilities
Good κs were observed for the ventilation with either 81mKr or technegas (Tables 4 and 5). The inter- and intraobserver agreement among the readers for the V/Q lung scans using 81mKr was good to very good with κs of 0.71–0.88 (95% CI, 0.56–1.0). This finding was comparable with the agreement for the technegas V/Q lung scan interpretations (κ, 0.74–0.96; 95% CI, 0.58–1.0). The McNemar χ2 test was negative in all of these cases, indicating no systematic bias in interpretation.
Interobserver and Intraobserver Variability for V/Q Scintigraphy with 81mKr
Interobserver and Intraobserver Variability for V/Q Scintigraphy with Technegas
Lower but acceptable κs were observed for the indication for ventilation (Table 6). The κs were 0.63–0.72 (95% CI, 0.54–0.80) for interobserver agreement and 0.85 (95% CI, 0.75–0.96) and 0.94 (95% CI, 0.87–1.0) for intraobserver agreement. However, the McNemar χ2 test was positive in many cases, indicating differences in the use of criteria for interpretation.
Interobserver and Intraobserver Variability for Assessment of Presence of Segmental Perfusion Defect
DISCUSSION
This study compared the performance of ventilation scintigraphy using technegas with that using 81mKr in consecutive patients with clinically suspected PE and in whom a systematic verification of the diagnosis was pursued. Using the Hull criteria for V/Q lung scan result assessment, the agreement between 81mKr and technegas ventilation studies was 84%. The reproducibility of the scintigraphic evaluation of both technegas and 81mKr and of the assessment of indication for ventilation scintigraphy was good to very good. In comparison with 81mKr, technegas had statistically significantly more nondiagnostic V/Q lung scan results, both at consensus and individual readings. In 15 of the 92 patients (16%), a discrepancy was found between technegas and 81mKr ventilation studies. A definite false-positive result was found in 4 of 12 patients with 81mKr (33%) compared with 2 of 3 patients (66%) with technegas.
Technegas was compared with 81mKr for ventilation in several studies performed on small patient groups; these studies showed contradicting results. In one study that compared these agents in 25 patients with suspected PE, no significant differences in V/Q lung scan result were observed (15). In another study, a tendency was found for technegas to ventilate areas that were not ventilated appreciably by 81mKr in 11 of 25 patients (44%); this resulted in 3 patients with a higher probability rating with technegas (22). A discrepancy between the two agents was found in 5 of 40 patients (12%) in another comparative study involving patients with known various respiratory diseases, and the authors reported an overestimation of ventilation with 81mKr and a relative decreased ventilation of the upper regions with technegas (23).
Several causes for the discrepancies between 81mKr and technegas ventilation have been suggested: absence of lung clearance of technegas (22); the recommended inhalation technique of technegas using a deep breath and breath hold instead of tidal breathing as for 81mKr (22); differences in the penetration index of technegas and 81mKr and, likewise, in the heterogeneity of distribution (15); and variation in the concentration of activity in the inspired air (most activity present at the end of expiration) and the uneven radiolabeling of 81mKr (23).
Technegas inhalation was well tolerated by the patients in these small studies, and no significant differences in diagnostic image quality between technegas and 81mKr were described (10,15,22,23). In our study, however, technegas ventilation failed because of severe illness in 8 of 53 patients (15%) who had an indication for ventilation scintigraphy. 81mKr ventilation could not be performed in only one of these 8 patients. Patients who were severely ill frequently could not be instructed for inhalation or had very shallow and rapid breathing (or both), which resulted in insufficient amounts of inhaled aerosol. Indeed, according to Alderson (24), the administration of insufficient amounts of aerosols is the most common error in ventilation studies performed after perfusion scintigraphy. When agents with the same photon energy are used for both perfusion and ventilation, the perfusion distribution will continue to dominate the final images when the amount of inhaled activity is insufficient. Technically poor images were described (occurring in 2% of the ventilation studies) in only one retrospective study in which technegas was used clinically for ventilation (25). Paradoxically, however, in severely ill patients, who are mechanically ventilated, technegas may more often give images of diagnostic quality because of the pressure by which the aerosol is driven into the lungs by the inspiratory pulse of the ventilator (26).
Although all perfusion scans were assessed using a lung reference chart, we found that most inter- and intraobserver variations occurred in the assessment of the size (i.e., segmental or not segmental) of the perfusion defects. Our results could not confirm the high intra- and interobserver agreements (90%–100% and 93%, respectively) in the assessment of V/Q lung scan results using a reference chart (19). Instead, the κs of 0.63–0.72 (95% CI, 0.54–0.80) for interobserver agreement and 0.85 (95% CI, 0.75–0.96) and 0.94 (95% CI, 0.87–1.0) for intraobserver agreement for the assessment of perfusion defect size confirm the results found using healthy volunteers (27) or virtual lung scintigraphy (28). A structural underestimation of the perfusion defect size was observed in these latter studies. The positive McNemar χ2 test indicates that differences in use of criteria for interpretation could contribute to the variation in estimation of segmental size as observed in our study.
Several methodologic aspects of this study deserve comment. Our investigation was aimed at completing the standardized protocol on every patient included in the study, especially on those patients with a nondiagnostic V/Q lung scan result. Unfortunately, pulmonary angiography could not always be performed because of severe illness, contraindications, refusal, or logistic reasons. The protocol did not require pulmonary angiography in patients with a high-probability V/Q lung scan result confirmed by spiral CT angiography. Pulmonary angiography is an invasive technique and is associated with a low, but not negligible, risk of complications. Moreover, it is generally accepted that anticoagulant treatment is indicated in patients with a high-probability V/Q lung scan result without further investigations. Thus, for ethical reasons, angiography was omitted in the case of a positive spiral CT scan.
Experienced nuclear physicians, who had had several consensus training sessions, performed the reading. The readers were unaware of each other’s results, the clinical information, and the results of other tests. They used well-defined and generally accepted criteria for the categorization of the V/Q lung scan results (20). In addition, to avoid recall bias, the scans were assessed in a random order with a time interval of at least 2 wk and, in most instances, 6 wk to 3 mo. As a result, our data show the variation based on true differences between and within observers.
Dual-isotope imaging with 81mKr was performed in some patients, which may have caused possible radionuclide downscatter of 81mKr into the 99mTc window. Furthermore, for technical reasons, we used for technegas ventilation imaging a counting rate difference of twice the counting rate of the 99mTc perfusion images. However, because the main question concerned (segmental or larger) perfusion defects, it is unlikely that contamination has had a significant influence on these perfusion defects, which themselves have a very low counting rate. Small defects were always considered nondiagnostic and did not require ventilation imaging for the V/Q scan result categorization. In addition, because some downscatter usually occurs, possible contamination is always taken into consideration when the images are assessed. In case of doubt, a count profile was performed to evaluate the possible occurrence of contamination.
Lastly, although there was an indication for ventilation in 145 patients, both 81mKr and technegas were available only in 92 cases. This was mostly related to discrepancies in estimation of the size of the perfusion defects. Nevertheless, the 95% CIs around the κs are reasonably small, indicating an acceptable precision.
CONCLUSION
This study shows a good agreement (κ, 0.68) between 81mKr and technegas lung ventilation in patients with suspected PE as well as comparable inter- and intraobserver variation. The benefits of technegas are the lower costs and the longer half-life and thus better availability compared with 81mKr. In comparison with 81mKr, technegas does not result in more false-positive V/Q lung scan results. However, the use of technegas increases the number of nondiagnostic and technically inadequate V/Q lung scan results, which would increase the demand for further additional testing to confirm or refute PE. Consequently, the desirability of replacement of 81mKr by technegas will depend not only on the costs of the isotopes but also on the acceptability, clinical consequences, and costs of further diagnostic testing. Clinical follow-up studies supplemented by cost-effectiveness analyses are warranted to fully evaluate the use of technegas.
Acknowledgments
The results of this study are reported on behalf of the study group of the Dutch Prospective Multicenter Trial on the Diagnosis of Pulmonary Embolism, ANTELOPE. The number of patients contributed by each center is given in parentheses. University Medical Center, Utrecht (n = 113): Jan Dirk Banga, MD; Paul F. G. M. van Waes, MD; Peter P. van Rijk, MD. Academic Medical Center, Amsterdam (n = 114): Bernd Jan Sanson, MD; Jeroen G. Lijmer, MD; Harry R. Büller, MD. University Hospital Vrije Universiteit, Amsterdam (n = 101): Pieter E. Postmus, MD; Otto S. Hoekstra, MD; Radu A. Manoliu, MD. This work was supported by a research grant from the Dutch Health Insurance Council.
Footnotes
Received Jun. 12, 2000; revision accepted Nov. 15, 2000.
For correspondence or reprints contact: Ieneke J.C. Hartmann, MD, Department of Radiology, University Medical Center, Rm. E 01.132, Heidelberglaan 100, Utrecht NL-3508 GA, The Netherlands.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Ventilation-Perfusion SPECT with 99mTc-DTPA Versus Technegas: A Head-to-Head Study in Obstructive and Nonobstructive Disease
- SPECT in Acute Pulmonary Embolism
- SPECT Imaging in the Diagnosis of Pulmonary Embolism: Automated Detection of Match and Mismatch Defects by Means of Image-Processing Techniques
- Tomographic Imaging in the Diagnosis of Pulmonary Embolism: A Comparison Between V/Q Lung Scintigraphy in SPECT Technique and Multislice Spiral CT