


Abstract
The somatostatin receptor subtype 2 is expressed on macrophages, an abundant cell type in the atherosclerotic plaque. Visualization of somatostatin receptor subtype 2, for oncologic purposes, is frequently made using the DOTA-derived somatostatin analogs DOTATOC or DOTATATE for PET. We aimed to compare the uptake of the PET tracers 68Ga-DOTATOC and 64Cu-DOTATATE in large arteries, in the assessment of atherosclerosis by noninvasive imaging technique, combining PET and CT. Further, the correlation of uptake and cardiovascular risk factors was investigated. Methods: Sixty consecutive patients with neuroendocrine tumors underwent both 68Ga-DOTATOC and 64Cu-DOTATATE PET/CT scans, in random order. For each scan, the maximum and mean standardized uptake values (SUVs) were calculated in 5 arterial segments. In addition, the blood-pool–corrected target-to-background ratio was calculated. Uptake of the tracers was correlated with cardiovascular risk factors collected from medical records. Results: We found detectable uptake of both tracers in all arterial segments studied. Uptake of 64Cu-DOTATATE was significantly higher than 68Ga-DOTATOC in the vascular regions both when calculated as maximum and mean uptake. There was a significant association between Framingham risk score and the overall maximum uptake of 64Cu-DOTATATE using SUV (r = 0.4; P = 0.004) as well as target-to-background ratio (r = 0.3; P = 0.04), whereas no association was found with 68Ga-DOTATOC. The association of risk factors and maximum SUV of 64Cu-DOTATATE was found driven by body mass index, smoking, diabetes, and coronary calcium score (P < 0.001, P = 0.01, P = 0.005, and P = 0.03, respectively). Conclusion: In a series of oncologic patients, vascular uptake of 68Ga-DOTATOC and 64Cu-DOTATATE was found, with highest uptake of the latter. Uptake of 64Cu-DOTATATE, but not of 68Ga-DOTATOC, was correlated with cardiovascular risk factors, suggesting a potential role for 64Cu-DOTATATE in the assessment of atherosclerosis.
Atherosclerosis is a systemic condition that can evolve to manifest cardiovascular disease, with potential fatal stroke or myocardial infarction as a result. Even though atherosclerosis is defined as a systemic condition, it consists of localized progressive plaques that can give rise to symptoms or proceed in a silent asymptomatic stage (1). The standard diagnosis of atherosclerosis includes physical examination; diagnostic tests such as blood tests, electrocardiogram, ankle/brachial index, and ultrasound; and invasive tests such as angiography, intravascular coronary ultrasound, and angioscopy (2,3). The examinations all vary in sensitivity, specificity, reproducibility, and availability. With emerging research identifying and unraveling cellular and molecular mechanisms of the changes in the progressive atherosclerotic plaque, new doors in diagnosing both clinical and subclinical stages of the disease have opened. Further, findings of molecular targets and cellular markers that are involved in the disease have led to development of new and noninvasive diagnostic techniques.
One particular target is the macrophage, which is an abundant cell type in the plaque and highly active in inflammation, a key process in progressive atherosclerosis. The macrophage migrates into the arterial intima as a monocyte where it matures to become a phagocytic macrophage. Various processes and cellular targets involved with the presence of this cell type have been investigated and identified as targets for PET, with expression of the somatostatin receptor, a G-protein–coupled 7-transmembrane protein, being one of them. Five human somatostatin receptors have been identified, and in atherosclerotic plaques the somatostatin receptor 2 is the most frequent (4–6). The somatostatin analogs DOTATOC and DOTATATE bind to somatostatin receptors, with highest affinity for the somatostatin receptor 2. Hence, they might be potential tracers for molecular imaging of atherosclerosis (7,8). A recent prospective study in patients with symptomatic carotid stenosis has indicated that uptake of 64Cu-DOTATATE is a marker of activated macrophages within the plaque (9).
In our study, DOTATOC was labeled with the radionuclide 68Ga and DOTATATE with 64Cu. 68Ga is produced by a 68Ge/68Ga generator that can last up to 9–12 mo because of the 68Ge half-life of approximately 270 d. 68Ga has a physical half-life of 68 min, which is compatible with the kinetics of most peptides. This makes 68Ga a favorable positron emitter, independent of an on-site cyclotron and with fast target localization and blood clearance, with mainly excretion through the kidneys. 64Cu, on the other hand, is generated on a cyclotron and has a half-life of 12.7 h. The long half-life of 64Cu allows for early as well as late PET scanning, even the day after injection. 64Cu has a substantially shorter positron range than 68Ga, 1 versus 4 mm, rendering it a much better spatial resolution, but a lower positron abundance (10–14).
The objective of this study was to evaluate the use of 2 somatostatin receptor–binding PET tracers in the assessment of the large arteries. The uptake of the tracers was compared in various vascular regions and the correlation with known cardiovascular risk factors was investigated, to support the hypothesis that vascular lesions containing macrophages are present in individuals with a recognized risk for atherosclerosis.
MATERIALS AND METHODS
Study Design and Patient Selection
We performed the analysis on scans from an ongoing clinical trial comparing 68Ga-DOTATOC and 64Cu-DOTATATE PET/CT in patients with neuroendocrine tumors. All patients (n = 60) included in the original trial were included in the present substudy. The original inclusion criterion was verified neuroendocrine tumor with clinical indication for 111In-octreotide SPECT/CT. Exclusion criteria were age below 18 y, pregnancy/lactation, performance status 0–2, and chemotherapy or radiation therapy in the previous 5 wk.
The study protocol complied with the Declaration of Helsinki (version 2013) and was approved by the Regional Scientific Ethical Committee. Written informed consent was obtained from all participants (protocol number H-D-2008-045).
For this substudy, the patients were reviewed regarding the 2 PET/CT scans, and known cardiovascular risk factors were collected retrospectively from their medical records. The investigated cardiovascular risk factors included age, sex, body mass index (BMI), smoking habits, diabetes, arterial hypertension defined by ongoing treatment, and hypercholesterolemia defined as ongoing treatment hereof. Because of few available cholesterol levels, the Framingham risk score was calculated by use of BMI, according to the Framingham Heart Study (15).
Imaging Procedures and Analysis
All patients underwent hybrid PET/CT scanning with 68Ga-DOTATOC and 64Cu-DOTATATE, in random order as soon as possible but with a maximum of 60 d in between. Each patient underwent the 2 examinations on the same hybrid PET/CT scanner (Biograph mCT64; Siemens). For the 68Ga-DOTATOC scan, 150 MBq were injected intravenously and, after 45 min, whole-body PET was performed in direct connection with a whole-body CT scan (120 kV; effective mAs, 40) for attenuation correction of the PET and anatomic localization of the vessels. Likewise, the PET/CT scan after intravenous injection of 200 MBq of 64Cu-DOTATATE was obtained 60 min after the injection. The PET scans were acquired in 3-dimensional (3D) list-mode for 3 min per bed position. The PET reconstruction settings were CT-based attenuation correction, resolution recovery (point-spread function, TrueX [Siemens]), and time of flight (3 iterations, 21 subsets; zoom, 1.0). A gaussian filter of 2 mm in full width at half maximum was then applied to all images after reconstruction.
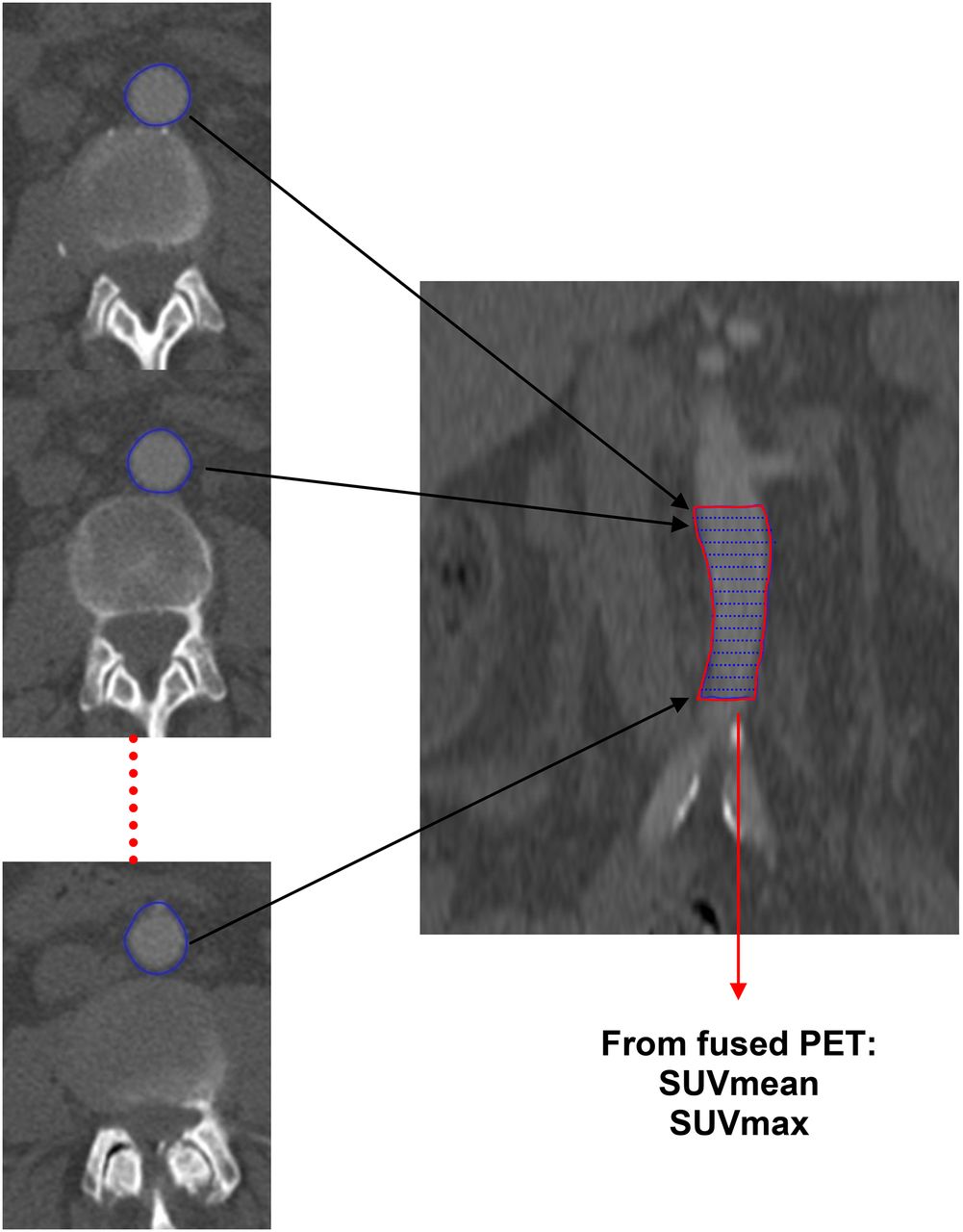
Anatomic coregistration of CT and PET was carefully checked before the assessment of vascular tracer uptake. Uptake was determined in 5 distinct vascular segments (the aortic arch, the descending thoracic aorta, the proximal and distal abdominal aorta, and the common iliac arteries). For analysis, 3D regions of interest (ROIs) were drawn manually slice by slice on both scans in these particular regions using Inveon Research Workplace (version 4.1; Siemens), avoiding adjacent hot spots arisen from, for example, lymph nodal metastases. The mean and maximal standardized uptake value (SUVmean and SUVmax, respectively) that correct for injected dose, patient weight, and time to acquisition were calculated for each 3D ROI (Fig. 1). In addition, each patient had whole-artery SUVmean and whole-artery SUVmax calculated as the average of the 5 SUVs in each patient. The target-to-background ratio (TBR) was determined by dividing SUV of the vascular segment with SUVmean from at least four 3D ROIs placed in the superior vena cava (representing the mean blood uptake).

Method for vascular tracer uptake quantification. Example from distal abdominal aorta: 1. outer vessel wall is manually delineated on all consecutive axial slices; 2. imaging software fuses these consecutive ROIs into single 3D volume of interest covering distal abdominal aorta; 3. single SUVmean and SUVmax are recorded for each volume of interest.
The coronary artery calcium score was assessed using Syngo.via version VB 10A (Siemens Healthcare) and the Agatston equivalent method with an attenuation threshold of 130 Hounsfield units.
Statistical Analysis
Statistical analyses were made using SPSS statistics (version 22; IBM). The analysis and comparison of the uptake of the 2 tracers were made using the Bland–Altman method. According to this method, the mean difference between measurements is defined as bias and represents the systemic error in measurements. The statistical significance of the bias was assessed using the t test. The 95% limits of agreement were defined as mean difference ± 1.96 times the SD. All limits of agreement were calculated assuming normal distribution of the differences. The associations between tracer uptake and cardiovascular risk factors were investigated using Spearman correlation and subsequent multiple regression with stepwise backward elimination to find potential predictors.
RESULTS
Patient Population
All 60 patients participating in the original study were also included in the present substudy. The baseline characteristics including cardiovascular risk factors are shown in Table 1. Framingham risk score describing the 10-y risk for cardiovascular disease, as calculated from BMI, showed 22% of patients with less than 10% risk (n = 13), 17% with 10%–20% risk (n = 10), 20% with 20%–30% risk (n = 12), and 27% with greater than 30% risk (n = 16). For 15% of the patients (n = 9), it was not possible to calculate the risk, because of missing data. Forty-five percent (n = 27) had a coronary calcium score of zero, whereas 15% (n = 9) had a score above 400.
Baseline Characteristics
PET/CT with 64Cu-DOTATATE and 68Ga-DOTATOC
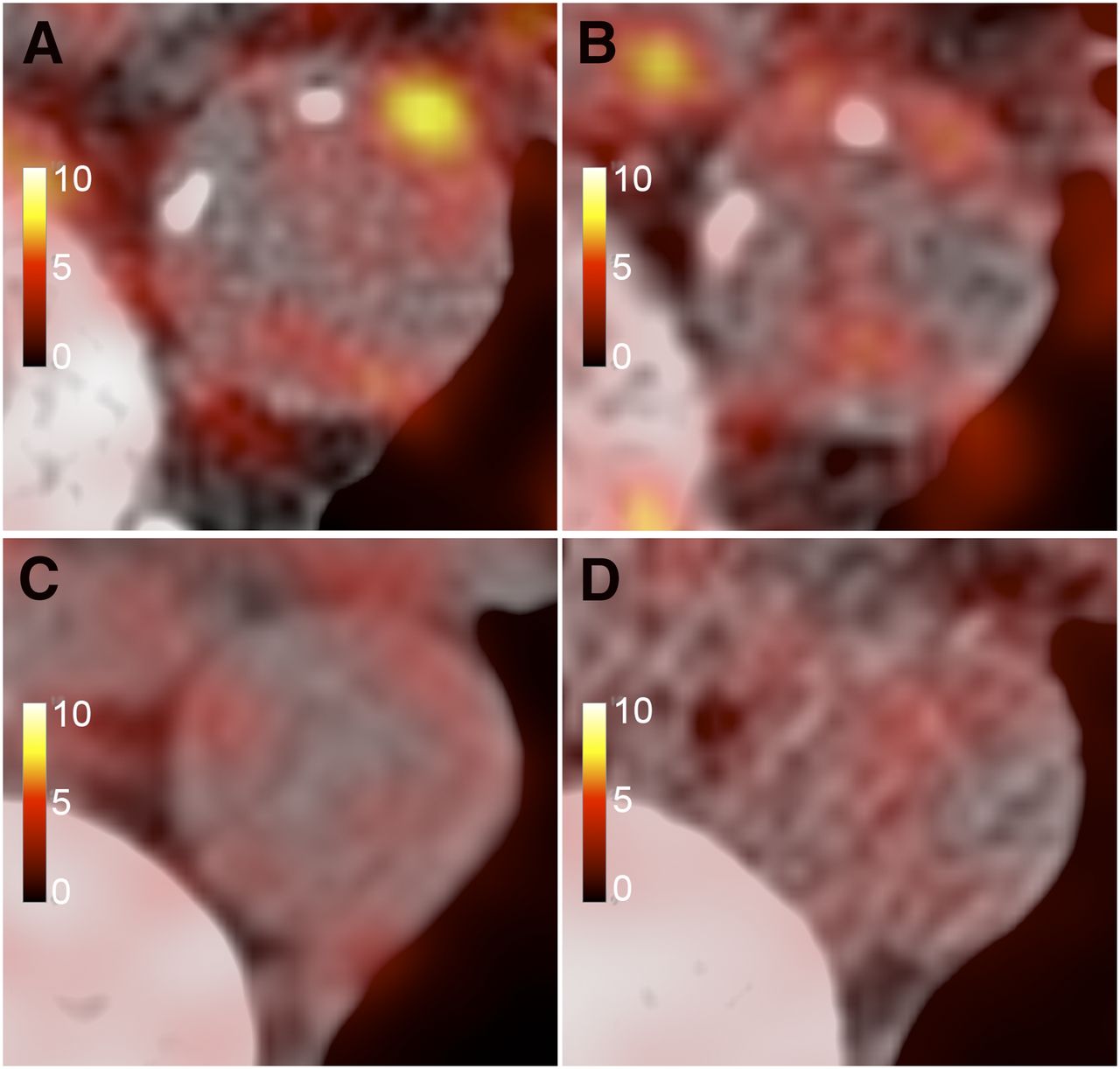
On the Bland–Altman plot, the comparison of the uptake of the 2 tracers (Fig. 2A) showed that 64Cu-DOTATATE had a significantly higher uptake value than 68Ga-DOTATOC when calculated as whole-artery SUVmax (P < 0.001). The 95% limits of agreement were from −2.3 to 5.7. The uptake of 64Cu-DOTATATE was also significantly higher measured as whole-artery SUVmean (P < 0.001), with 95% limits of agreement from −0.5 to 1.1 (Fig. 2B). Representative images of high focal and low diffuse uptake of the 2 tracers are shown in Figure 3. Also, venous SUV was higher with 64Cu-DOTATATE than with 68Ga-DOTATOC, and the numeric difference between arterial and venous uptake was highest with 64Cu-DOTATATE (Fig. 4).

Comparison of 68Ga-DOTATOC and 64Cu-DOTATATE uptake in large arteries. Bland–Altman plots of difference, with dashed lines indicating identity line and horizontal colored lines indicating mean difference with 95% limits of agreement, are shown. Top line shows comparison of SUVmax (A) and SUVmean (B). Likewise, bottom line shows comparison of maximum TBR (C) and mean TBR (D).
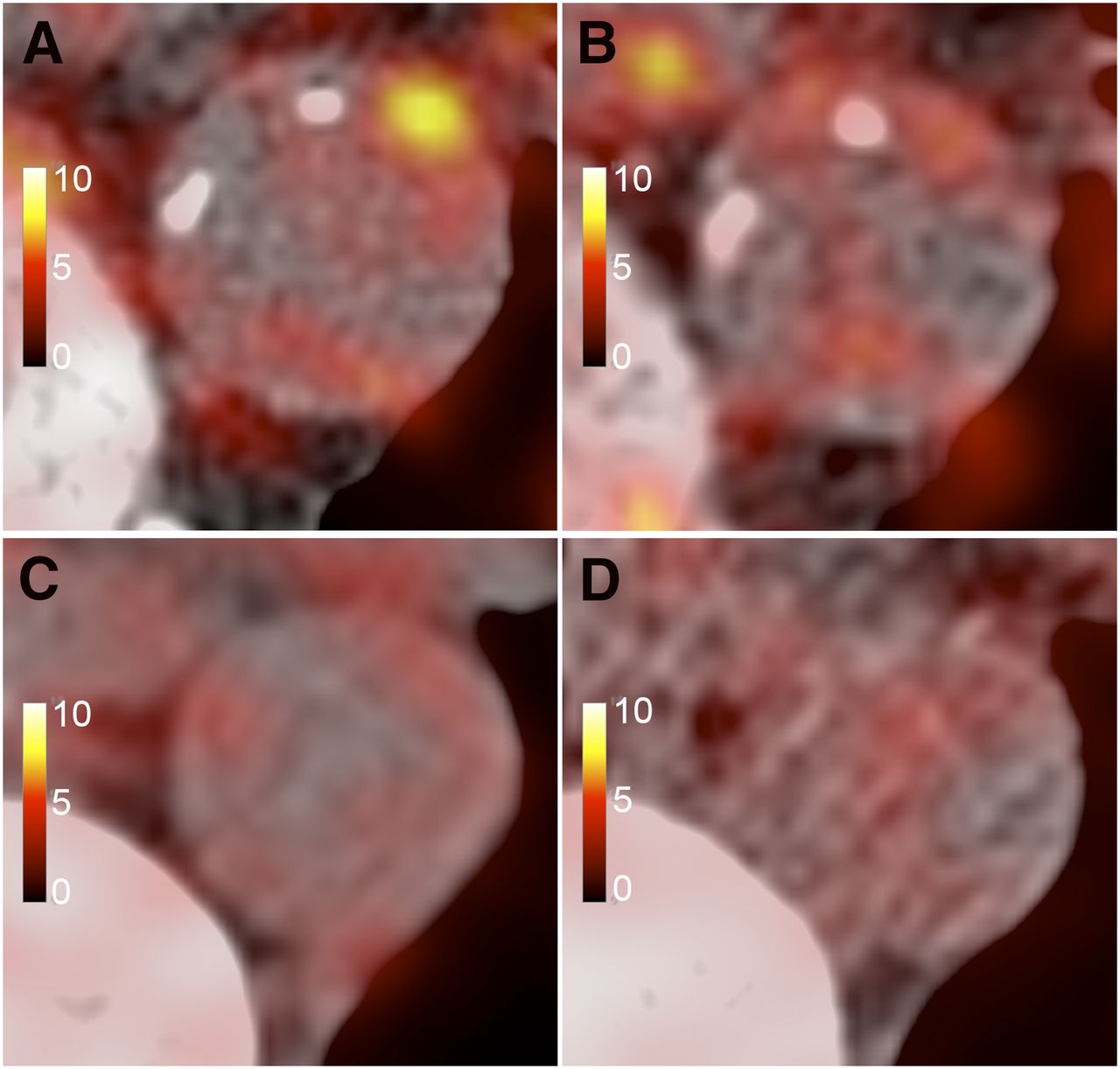
Examples of PET/CT fusion showing uptake of 64Cu-DOTATATE (A and C) and 68Ga-DOTATOC (B and D). Patient in A and B is 67-y-old man with Framingham risk score of 30. Images show high focal uptake in thoracic aorta on 64Cu-DOTATATE PET (A), whereas same location on 68Ga-DOTATOC PET is more blurred (B). Patient in C and D is 31-y-old woman with Framingham risk score of 2. Images show lower and more diffuse uptake with both tracers.
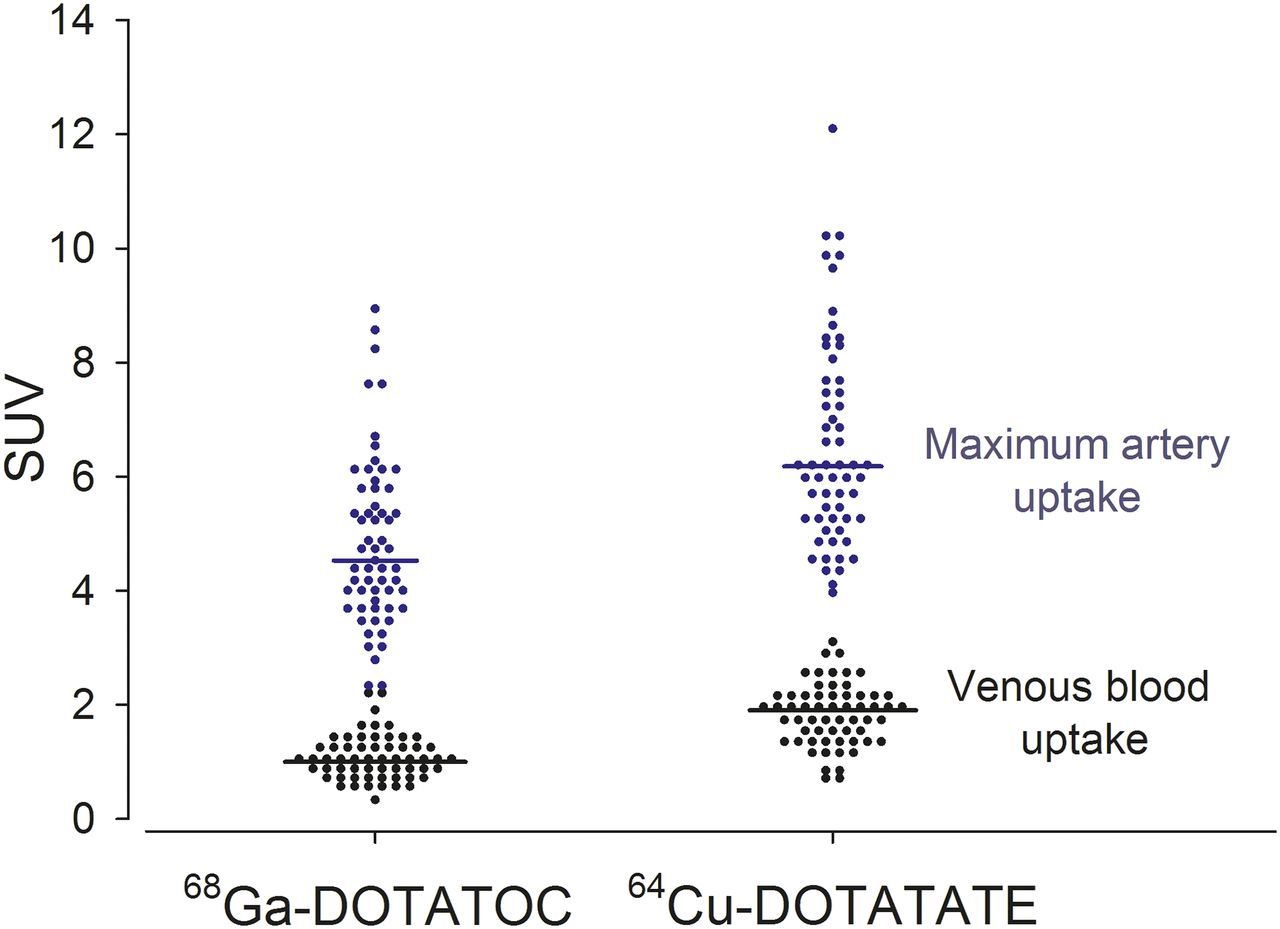
SUVs of 68Ga-DOTATOC and 64Cu-DOTATATE in arteries (blue) and superior cava vein (black). Data are paired, and each patient is represented with dot in each of the 4 categories. Median uptake is shown in bold lines.
The mean difference between uptake of the tracers (SUV) was also calculated in the 5 regions, respectively, with significant results in all 5 artery segments, showing higher uptake of 64Cu-DOTATATE, as seen in Table 2.
Mean Difference Between 64Cu-DOTATATE and 68Ga-DOTATOC Uptake in Each Region
Correlation with Risk Factors
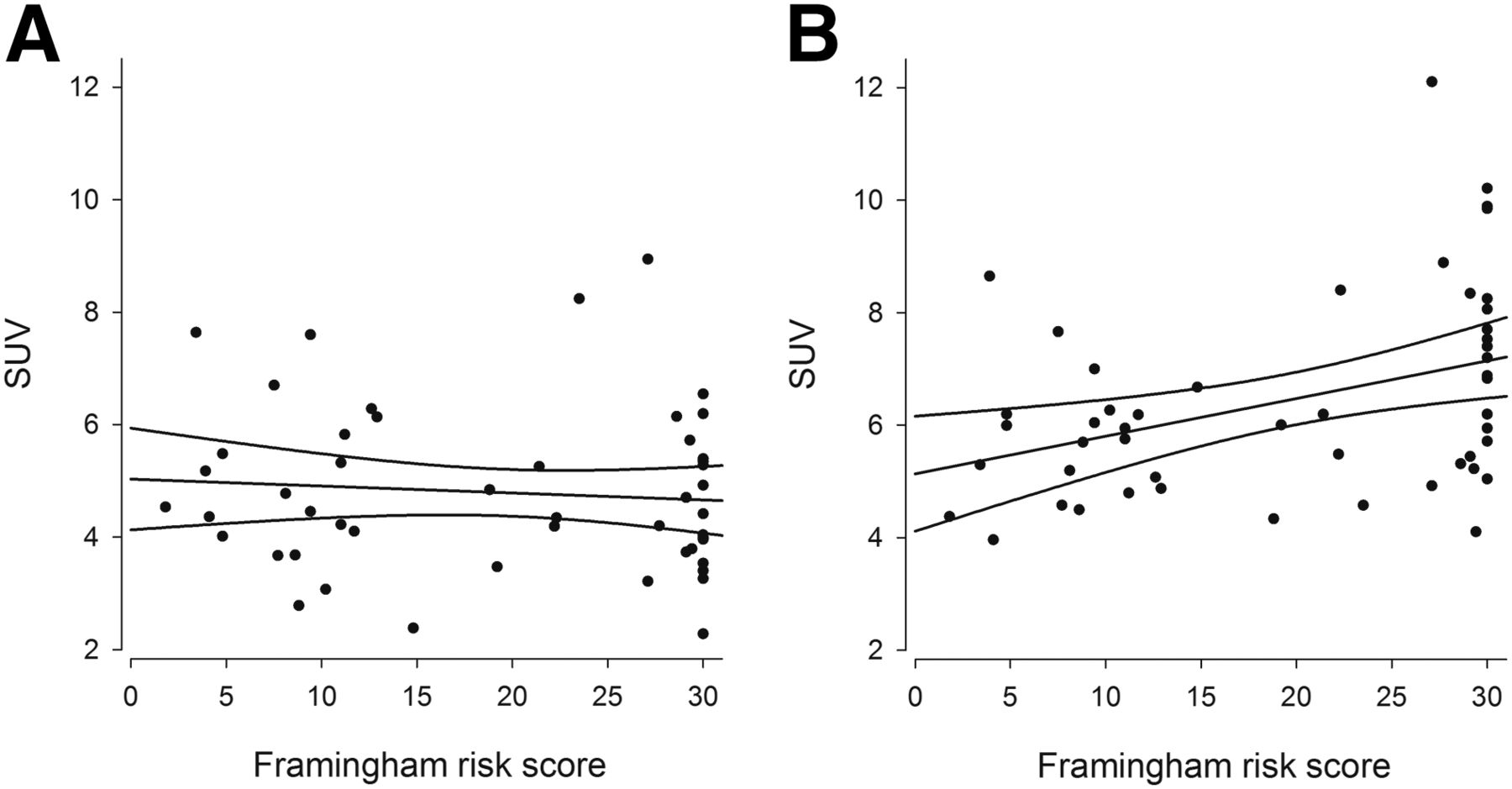
The association between tracer uptake and risk factors was investigated using both SUVmean and SUVmax in the 5 artery segments, for both tracers. We found an overall significant association between maximum 64Cu-DOTATATE uptake (whole-artery SUVmax) and Framingham risk score (r = 0.4; P = 0.004, Fig. 5B), whereas maximum 68Ga-DOTATOC (whole-artery SUVmax) did not correlate with Framingham risk score (P = 0.3, Fig. 5A). Whole-artery SUVmean did not correlate with Framingham risk score, neither with 64Cu-DOTATATE (r = 0.1; P = 0.4) nor with 68Ga-DOTATOC (r = −0.3; P = 0.1). Similar results were found when TBR was used rather than SUV, but with a lower correlation between maximum 64Cu-DOTATATE uptake (whole-artery maximum TBR) and Framingham risk score (r = 0.3; P = 0.04), and no correlation between Framingham risk score and 68Ga-DOTATOC uptake.

Correlation between Framingham risk score and 68Ga-DOTATOC uptake (A) and whole-artery 64Cu-DOTATATE uptake (B).
The association between maximum 64Cu-DOTATATE uptake and Framingham risk score was consistently found in 3 of the 5 vascular regions (descending thoracic aorta, proximal part of the abdominal aorta, and iliac arteries), whereas 68Ga-DOTATOC was only inversely correlated with Framingham risk score in 1 region (distal part of the abdominal aorta) (Table 3).
Correlations Between Framingham Risk Score and Maximum Tracer Uptake in 5 Regions
Multiple regression including sex, age, BMI, diabetes, smoking, systolic blood pressure, coronary calcium score, and treatment for hypertension and treatment for hypercholesterolemia showed that BMI, smoking, diabetes, and coronary calcium score were independent predictors of SUVmax with 64Cu-DOTATATE (P < 0.001, P = 0.01, P = 0.005, and P = 0.03, respectively).
DISCUSSION
We present here the first comparison of arterial uptake of 64Cu-DOTATATE with 68Ga-DOTATOC in a population unselected for cardiovascular risk profile using hybrid PET/CT. We found a higher uptake of 64Cu-DOTATATE and wide limits of agreement for maximum uptake (SUVmax) of the 2 tracers. In addition, we found results in support of an association between 64Cu-DOTATATE and cardiovascular risk factors suggesting this radiotracer as a potential noninvasive biomarker of cardiovascular risk. This result supports our recent finding in patients with severe carotid stenosis in whom 64Cu-DOTATATE uptake in excised carotid plaques was associated with the gene expression of a marker of alternatively activated macrophages (9). Together, it therefore may seem that 64Cu-DOTATATE may be valuable in imaging of atherosclerosis both in patients with and in patients without known atherosclerotic cardiovascular disease.
The use of the PET technique to visualize atherosclerosis was initiated by the finding that patients scanned after injection of FDG, labeled with the radionuclide 18F, for tumor visualization also showed arterial uptake of the tracer (16). The first clinical study with PET imaging of atherosclerosis, published in 2002 (17), was consequently performed using 18F-FDG, which is a marker for uptake of glucose and hereby metabolism in tissue. The uptake of 18F-FDG was later shown to correlate significantly with plaque macrophage content, with other circulating inflammatory biomarkers (18–21) and known cardiovascular risk factors (6,22). Therefore, hope has risen that 18F-FDG might be used to evaluate therapeutic intervention (23). After the optimistic results that PET scans with 18F-FDG have given, additional and more specific tracers have been developed, for example, tracers targeting macrophages. Although 18F-FDG visualizes the metabolism of the cell and therefore the physiologic state of inflammation that a given cell in an atherosclerotic plaque is in, targeting a macrophage-expressed receptor could be a more specific tracer.
The aim of this study was to compare the uptake of 2 somatostatin receptor–binding PET tracers in large arteries and evaluate their use in PET/CT in the assessment of atherosclerosis. These tracers have earlier been used and compared in connection with cancer diagnostics, primarily neuroendocrine tumors (24–26). Furthermore, 68Ga-DOTATATE has previously been assessed in relation to inflammation in the aorta and compared with 18F-FDG (27). There are to our knowledge no studies that have compared the uptake of DOTATOC and DOTATATE in the aorta in addition to their possible role for risk evaluation.
Both DOTATOC and DOTATATE are somatostatin analogs conjugated with the chelator abbreviated DOTA, which hereafter are labeled with radiopharmaceuticals to be visualized on PET scans. The difference between the peptides is a replacement of octreotide C-terminal threoninol (DOTATOC) to the natural amino acid threonine, which produces octreotate (DOTATATE). When the peptides are labeled with 67Ga, they both bind to the somatostatin receptor 2 with exceptional affinity; however, binding is highest for DOTATATE (7). On the basis of this and previous studies (7,14,28,29), we would expect an uptake of both tracers in regions with plaque formations and furthermore that, in our case, the 64Cu-labeled DOTATATE would show higher focal uptake in the aorta than 68Ga-DOTATOC.
We found a consistent difference between uptake of the tracers calculated as SUVmax, SUVmean, maximum TBR, and mean TBR in all tested vascular regions. All SUV results show highest uptake of 64Cu-DOTATATE. This was not unexpected, because 64Cu has a shorter positron range (∼1 mm) than 68Ga (∼4 mm). 64Cu is thus less sensitive to both spillover and partial-volume loss. In concordance with this, we found especially SUVmax to have wide limits of agreement when 64Cu-DOTATATE was compared with 68Ga-DOTATOC. The difference in affinity between the tracers is also consistent with the higher SUV of DOTATATE than DOTATOC in the vascular regions. It should be acknowledged that a higher PET signal is preferable when assessing plaques, because of their small dimensions.
We also investigated association between the uptake of tracer and classic cardiovascular risk factors. A positive correlation reinforces the theory that individuals with a certain behavior and phenotype, known to have higher risk of developing atherosclerosis, also would have high tracer uptake (30).
The results showed an association between Framingham risk score and overall maximum 64Cu-DOTATATE uptake whereas overall 68Ga-DOTATOC uptake was not associated with the risk score. This is important methodologic information because studies of atherosclerosis using 68Ga-labeled somatostatin receptor tracers may overlook true differences. Previous studies have shown a high congruence between 68Ga-DOTATATE and 68Ga-DOTATOC binding (24,31). Therefore, it is our hypothesis that the difference in both measured vessel wall uptake (Fig. 2) and Framingham risk correlation (Fig. 5) is primarily caused by the difference in radiotracer emission energy between 64Cu and 68Ga and thus related to the spatial resolution of the examination rather than a physiologic difference in tracer binding. Still, other studies have shown a correlation between DOTATATE labeled with 68Ga and risk factors (6,8,27). However, more atherosclerotic vessels in these studies may be the cause hereof.
As expected, we found only an association between Framingham risk score and SUVmax, whereas SUVmean did not correlate. This is in concordance with previous studies (6,8,27) and further supports the hypothesis that vascular 64Cu-DOTATATE uptake is heterogeneous and could serve as a marker of more advanced and potentially more vulnerable lesions. Similarly, we have previously found heterogeneous uptake of 18F-FDG in atherosclerotic carotid plaques (18).
A limitation of the study is the lack of histologic samples to validate that the uptake of tracer is actually from vascular lesions and to what cell type the tracer is binding. Therefore, prospective studies are warranted with other (nononcologic) and larger patient groups to further validate the clinical use of PET/CT with somatostatin receptor–binding tracers in the assessment of atherosclerosis (8).
CONCLUSION
In this study of 2 somatostatin receptor–binding tracers for PET/CT, we found a higher vascular uptake of the 64Cu-labeled DOTATATE than 68Ga-DOTATOC. Furthermore, results showed a significant correlation of Framingham risk score with uptake of 64Cu-DOTATATE, which was driven by smoking, BMI, and diabetes. No such correlation was found with 68Ga-DOTATOC. We suggest that 64Cu-DOTATATE seems suitable for the assessment of atherosclerosis even in the subclinical stages, but prospective studies to further validate this are required.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by unrestricted grants from the John & Birthe Meyer Foundation, the National Advanced Technology Foundation, Danish Medical Research Council, Rigshospitalets Research Foundation, Svend Andersen Foundation, AP Møller Foundation, Novo Nordisk Foundation, and Lundbeck Foundation. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the staff in the PET center for their skillful assistance.
Footnotes
↵* Contributed equally to this work.
Published online Oct. 1, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 20, 2015.
- Accepted for publication September 22, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Vascular Calcification: The Evolving Relationship of Vascular Calcification to Major Acute Coronary Events
- MR/PET Imaging of the Cardiovascular System
- PET/CT Imaging of Unstable Carotid Plaque with 68Ga-Labeled Somatostatin Receptor Ligand
- Imaging Vulnerable Plaque: A Medical Necessity or a Scientific Curiosity?
- Detection of Atherosclerotic Inflammation by 68Ga-DOTATATE PET Compared to [18F]FDG PET Imaging
- Linking Hemorrhage, Angiogenesis, Macrophages, and Iron Metabolism in Atherosclerotic Vascular Diseases
- Molecular Imaging of Inflammation: Current Status