


Abstract
For the noninvasive evaluation of coronary artery disease (CAD), both multislice CT and gated SPECT are available. How these 2 modalities relate, however, is yet unclear. The purpose of this study was to perform a head-to-head comparison of the results of multislice CT and gated SPECT on a regional basis (per vessel distribution territory) in patients with known or suspected CAD. Methods: One hundred forty patients underwent both multislice CT for coronary calcium scoring and coronary angiography and gated SPECT for myocardial perfusion imaging. The coronary calcium score was determined for each coronary artery. Coronary arteries on multislice CT angiography were classified as having no CAD, insignificant stenosis (<50% luminal narrowing), significant stenosis, or total or subtotal occlusion (≥90% luminal narrowing). Gated SPECT findings were classified as normal or abnormal (reversible or fixed defects) and were allocated to the territory of one of the various coronary arteries. Results: In coronary arteries with a calcium score of 10 or less, the corresponding myocardial perfusion was normal in 87% (n = 194/224). In coronary arteries with extensive calcifications (score > 400), the percentage of vascular territories with normal myocardial perfusion was lower, 54% (n = 13/24). Similarly, in most of the normal coronary arteries on multislice CT angiography, the corresponding myocardial perfusion was normal on SPECT (156/175, or 89%). In contrast, the percentage of normal SPECT findings was significantly lower in coronary arteries with obstructive lesions (59%) or with total or subtotal occlusions (8%) (P < 0.01). Nonetheless, only 48% of vascular territories with normal perfusion corresponded to normal coronary arteries on multislice CT angiography, whereas insignificant and significant stenoses were present in, respectively, 40% and 12% of corresponding coronary arteries. Conclusion: Although a relationship exists between the severity of CAD on multislice CT and myocardial perfusion abnormalities on SPECT, analysis on a regional basis showed only moderate agreement between observed atherosclerosis and abnormal perfusion. Accordingly, multislice CT and gated SPECT provide complementary rather than overlapping information, and further studies should address how these 2 modalities can be integrated to optimize patient management.
The choice of treatment strategy in patients with suspected or known coronary artery disease (CAD) stems from integration of both the extent and the severity of anatomic disease and the functional significance of the coronary lesions, that is, signs of ischemia. Coronary anatomy used to be accessible only through invasive coronary angiography, whereas inducible ischemia can be detected by several imaging techniques, among which was myocardial perfusion SPECT. Because of its invasive nature, coronary angiography came second to myocardial perfusion SPECT, and the presence or absence of ischemia on SPECT was the gatekeeper that determined access to the anatomic information provided by angiography.
This paradigm has been challenged with the emergence of noninvasive coronary angiography using multislice CT. Because information on coronary anatomy can now be obtained noninvasively, multislice CT coronary angiography is being performed increasingly often at earlier stages of the disease, in the absence of a functional evaluation (1). Preliminary data comparing multislice CT with SPECT show that, in fact, a large discrepancy exists between the anatomic extent of CAD and ischemia and that many stenoses do not result in abnormal perfusion (1,2). Thus, it remains undetermined in which sequence the tests should be performed and, ultimately, who will benefit from the performance of noninvasive coronary angiography. To design proper evaluation strategies, one must understand how anatomic and functional findings relate to each other on a regional basis, per vessel distribution territory.
Therefore, we have further explored, in an unselected patient population, the relationship between the severity of anatomic CAD based on coronary calcium and multislice CT angiography and the severity of perfusion abnormalities based on SPECT.
MATERIALS AND METHODS
Patients and Study Protocol
The study group consisted of 140 consecutive patients (84 men and 56 women; average age ± SD, 59 ± 11 y) who were referred for both gated SPECT and multislice CT because of clinically suspected CAD and who underwent these investigations within 1 mo of each other. CAD was known to be present in 32 patients (23%) and was suspected in the remaining 108 patients. The characteristics of the study population are summarized in Table 1. The average left ventricular ejection fraction during resting gated SPECT was 60% ± 13%.
Clinical Characteristics of Study Population (n = 140)
Exclusion criteria included contraindications to multislice CT (3) and the occurrence of unstable angina, myocardial infarction, or revascularization between the 2 procedures. The local ethics committee approved the study protocol, and all patients gave informed consent.
Multislice CT Coronary Angiography
First, a prospective coronary calcium scan was obtained before multislice CT angiography. The collimation was 4 × 3.0 mm; gantry rotation time, 500 ms; tube voltage, 120 kV; and tube current, 200 mA. The temporal window was set at 75% after the R wave for electrocardiographically triggered prospective reconstruction. The coronary calcium score was derived using dedicated software (Vitrea2; Vital Images). Coronary calcium was identified as a dense area in the coronary artery exceeding the threshold of 130 HU. The Agatston score, both global and per coronary artery, was recorded for each patient. Coronary calcium scores were classified into 4 categories (≤10, 11−100, 101−400, and >400).
For the contrast-enhanced helical scan, data were acquired with a collimation of either 16 × 0.5 or 64 × 0.5 mm and a tube rotation time of 400, 450, or 500 ms (depending on the heart rate). The tube current was 300 mA, at a voltage of 120 kV. In 31 patients, 16-slice CT (Aquilion 16; Toshiba Medical Systems) was used (3), and in 109 patients, 64-slice CT (Aquilion 64; Toshiba Medical Systems) was used. Nonionic contrast material (iomeprol [Iomeron 400]; Bracco) was administered in the antecubital vein at a volume of 120–140 mL for 16-slice CT and of 80–110 mL for 64-slice CT, depending on the total scanning time, and at a rate of 5 mL/s, followed by a saline flush. Subsequently, datasets were reconstructed and transferred to a remote workstation as previously described (3).
An interventional cardiologist who was unaware of the SPECT data evaluated the multislice CT angiograms to determine whether atherosclerosis was absent, present but not significantly stenotic (≥50% luminal narrowing), present and significantly stenotic (≥50% luminal narrowing), or present and totally or subtotally occlusive (≥90% luminal narrowing). In the analysis, the left main coronary artery was considered part of the left anterior descending coronary artery. In patients who had undergone previous coronary bypass grafting, the graft and its distal runoff were evaluated. In the case of an occluded or stenosed graft, the native coronary artery proximal to the anastomosis also was included in the analysis.
Stress–Rest Gated SPECT
In all patients, stress–rest gated SPECT (2 × 500 MBq of 99mTc-tetrofosmin) was performed using symptom-limited exercise or pharmacologic (adenosine or dobutamine) stress as previously described (4). After acquisition with a triple-head SPECT camera (GCA 9300/HG; Toshiba Corp.), data were reconstructed in long- and short-axis projections perpendicular to the heart axis. The short-axis data were displayed in polar map format, with the maps divided into 17 segments (5) and normalized to peak myocardial activity (100%). The 17 segments were allocated to the territories of the different coronary arteries as previously described (5). Perfusion defects were identified on the stress images (tracer activity < 75% of maximum) and classified as ischemia (reversible defects, with a ≥10% increase in tracer uptake on the resting images) or scar tissue (fixed defects, without a ≥10% increase in tracer uptake on the resting images). Accordingly, the findings were classified as either normal or abnormal, with the latter being further classified as either reversible or irreversible defects. The gated images were used to assess regional wall motion to improve differentiation between perfusion abnormalities and attenuation artifacts. For irreversible defects, whether the defects were located in a region with a documented previous myocardial infarction was recorded. Left ventricular ejection fraction was derived from the gated SPECT data using previously validated automated software (quantitative gated SPECT [QGS]; Cedars-Sinai Medical Center); gating was performed only at rest.
Statistical Analysis
Continuous variables were expressed as mean ± SD. Patient groups were compared using 1-way ANOVA for continuous variables and the χ2 test with Yates correction for categoric variables. A P value of less than 0.05 was considered statistically significant.
RESULTS
Analysis on a Vessel Basis
Multislice CT and SPECT Findings.
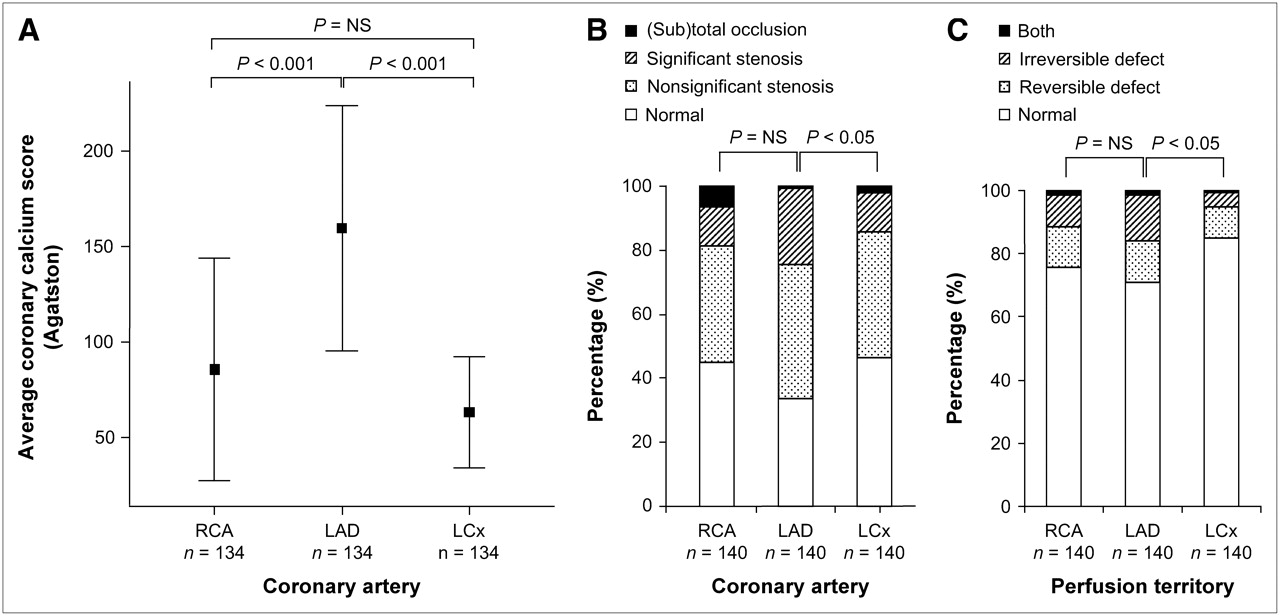
The coronary calcium score was available for 134 patients (96%) and, accordingly, for 402 coronary arteries. The average score per coronary artery was 102.6 ± 311.2 (range, 0−3,739). The distribution of scores per coronary artery is provided in Figure 1. In Figure 2A, average scores for the 3 coronary arteries are depicted, demonstrating more calcium in the left anterior descending coronary artery than in the right coronary artery and the left circumflex coronary artery (P < 0.001, Kruskal–Wallis).
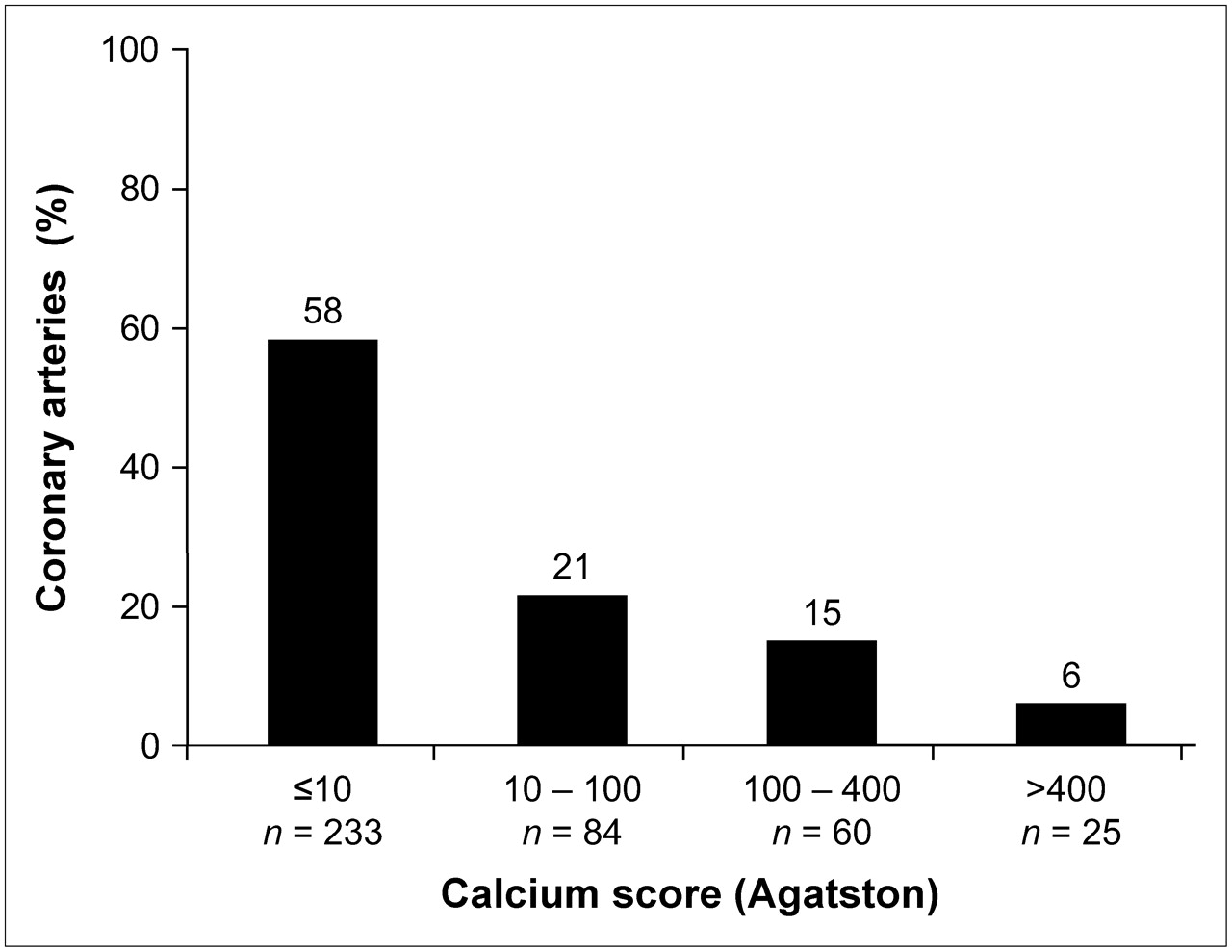
Distribution of coronary calcium score categories (per coronary artery).

Results per coronary artery and perfusion territory: average coronary calcium scores (+95% CI) per coronary artery (A), multislice CT results per coronary artery (B), and SPECT results per coronary perfusion territory (C). LAD = left anterior descending coronary artery; LCx = left circumflex coronary artery; RCA = right coronary artery.
With multislice CT angiography, a total of 420 vessels were evaluated. All coronary arteries were included. No abnormalities were observed on multislice CT angiography in 175 vessels (42%), whereas 245 vessels revealed either atherosclerosis without significant stenosis (n = 165, or 39%) or atherosclerosis with at least 1 significant stenosis (n = 80, or 19%). In the latter, total or subtotal occlusions were present in 13 vessels. Results per coronary artery are displayed in Figure 2B.
On SPECT, 420 vascular territories were available, of which 327 (78%) showed normal myocardial perfusion. Abnormal perfusion was observed in the remaining 93 territories (22%). In 20 territories, fixed defects corresponding to territories with a known previous myocardial infarction were observed. Of the remaining 73 vascular territories, 41 showed ischemia and 27 showed fixed defects, whereas 5 territories showed both. Figure 2C displays the distribution of perfusion findings among the territories of the different coronary arteries.
Stenoses on Multislice CT Angiography Versus Coronary Artery Calcium Score.
The average coronary artery calcium score was 1.4 ± 6.0 for normal coronary arteries and increased to 111.6 ± 212.9 and 313.3 ± 600.4 for coronary arteries with insignificant and significant stenoses, respectively (P < 0.001, Kruskal–Wallis). When only total or subtotal occlusion was considered, the extent of coronary calcifications was even higher, 656.5 ± 280.9 (P < 0.001). In most coronary arteries with a coronary calcium score below 100 (n = 284, or 90%), no significant stenoses were demonstrated. Of the 33 of 60 coronary arteries with a calcium score between 100 and 400, significant stenoses were present in 45%. This percentage further increased to 60% in the 25 coronary arteries with a calcium score above 400.
Perfusion on SPECT Versus Coronary Artery Calcium Score.
The average calcium score in coronary arteries with normal myocardial perfusion on SPECT was 69 ± 167, whereas a significantly higher calcium score of 272 ± 646 was noted for coronary arteries with abnormal myocardial perfusion on SPECT (P < 0.001, Mann–Whitney).
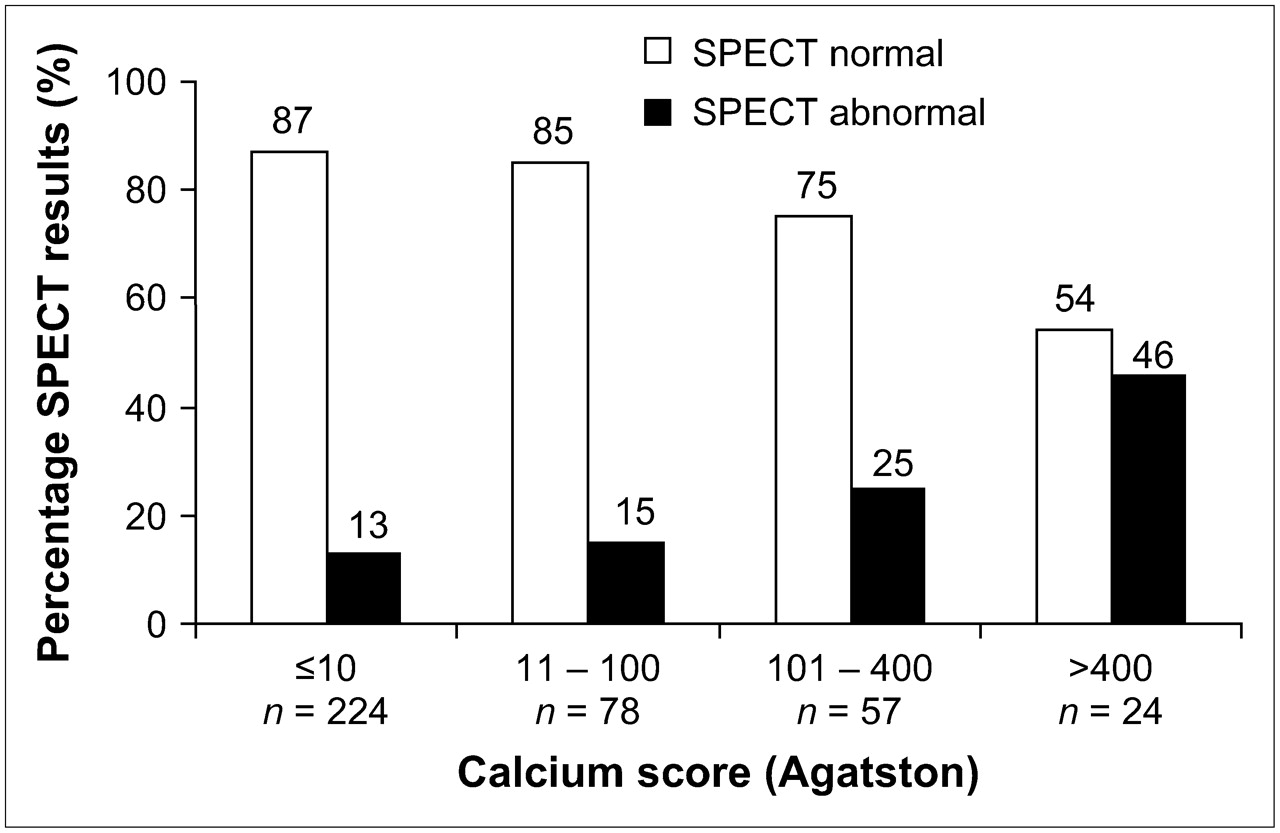
Figure 3 shows the distribution of normal and abnormal myocardial perfusion (with exclusion of 19 vascular territories with previous myocardial infarction) according to the different calcium scores. In most of the coronary arteries with no or minimal calcium (score ≤ 10) (n = 194, or 87%), the SPECT findings were normal. The percentage showing normal perfusion was only slightly lower (85%) in coronary arteries with a calcium score between 11 and 100 (P = not statistically significant [NS]). In coronary arteries with more extensive calcifications, the percentage showing normal myocardial perfusion on SPECT was significantly lower: 75% for coronary arteries with calcium scores between 100 and 400 and 54% for coronary arteries with calcium scores above 400 (P = 0.008).
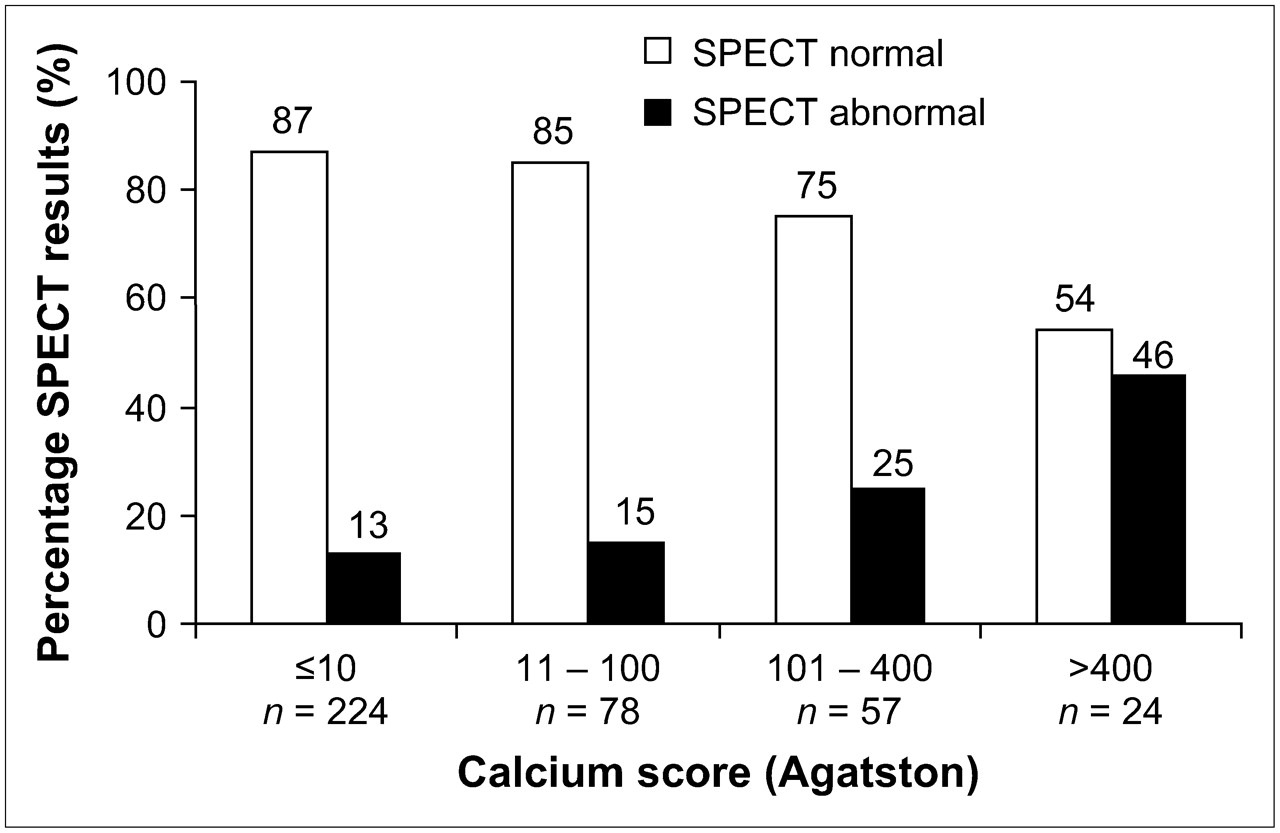
Distribution of normal (n = 316) and abnormal (n = 67) vessel-based myocardial perfusion on SPECT among coronary calcium score categories.
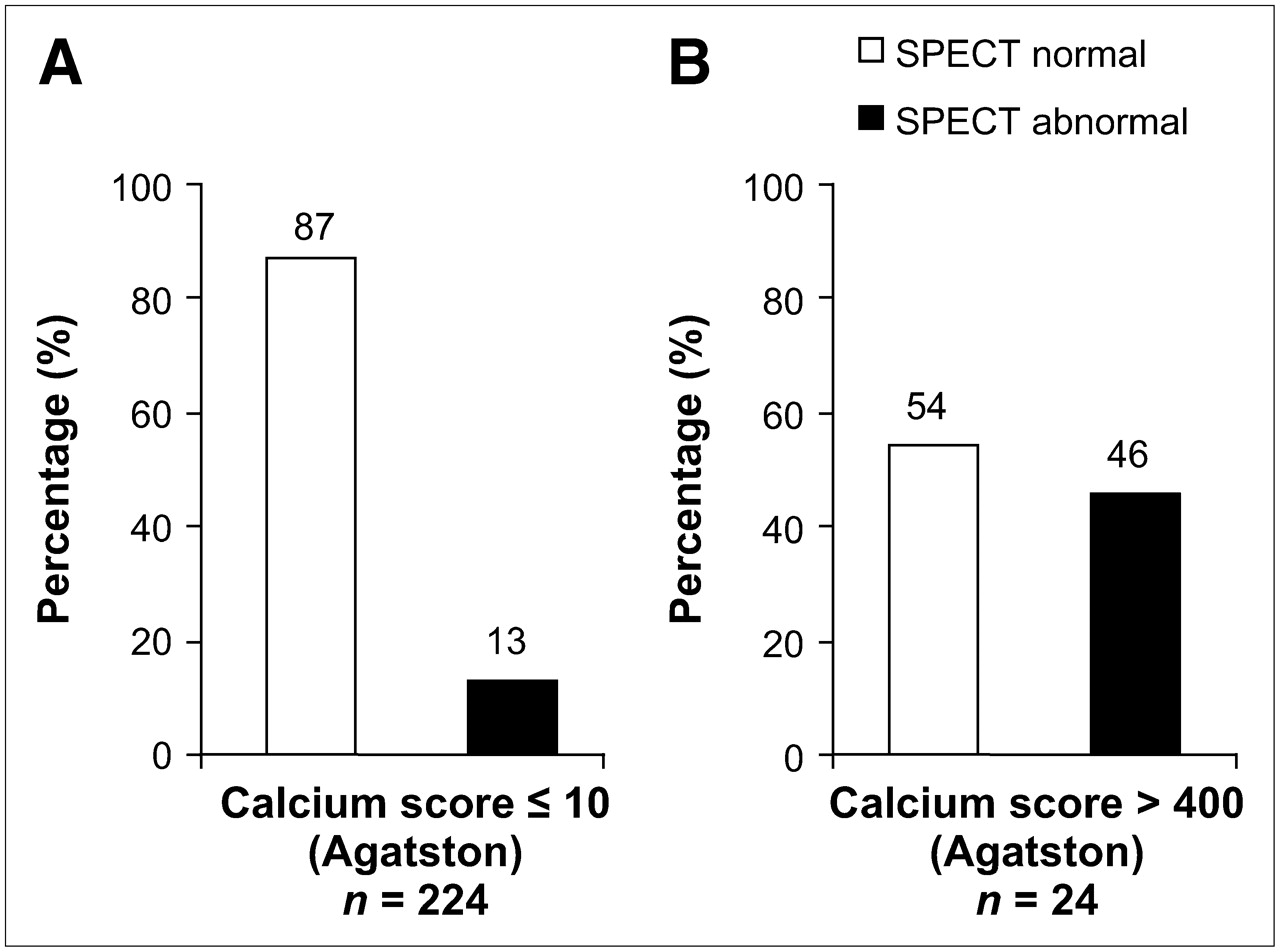
Thus, the likelihood of normal perfusion on SPECT decreased in parallel to an increasing calcium score on multislice CT. The predictive value of absence of calcium (score ≤ 10) for normal perfusion was 87% (Fig. 4A), but the value of significant calcium (score > 400) for prediction of abnormal perfusion was only 46% (Fig. 4B).

Relationship between calcium and perfusion: prediction of normal perfusion (A) and prediction of abnormal perfusion (B).
Perfusion Versus Stenoses on Multislice CT Angiography.
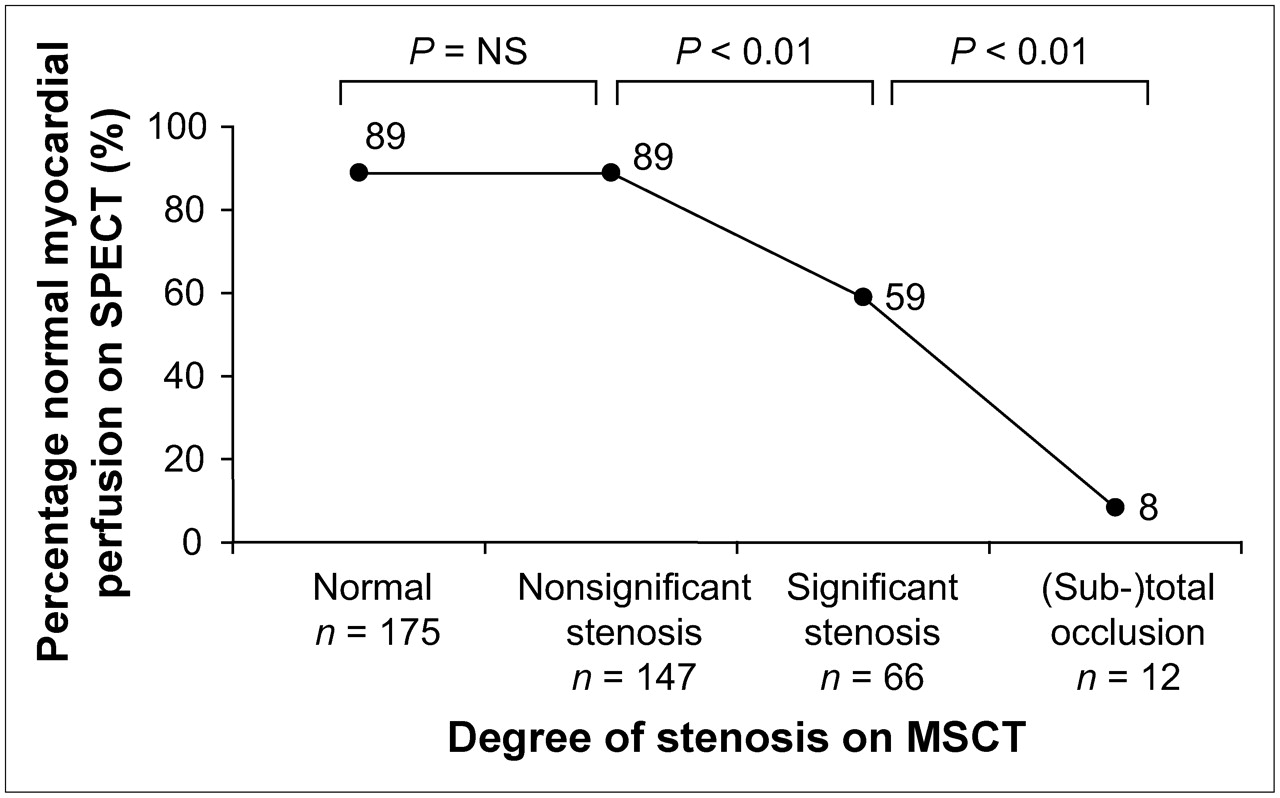
In most coronary arteries that were normal on multislice CT angiography, myocardial perfusion on SPECT in the corresponding territories was normal (156/175, or 89%). In coronary arteries with stenoses (regardless of severity, n = 225) on multislice CT (with exclusion of 20 vascular territories with previous myocardial infarction), myocardial perfusion on SPECT was still normal in 171 corresponding territories (76%). However, the likelihood of normal perfusion in coronary arteries with a significant stenosis or a total or subtotal occlusion decreased significantly (Fig. 5). Of the 78 coronary arteries with significant stenoses on multislice CT, abnormal perfusion on SPECT was present in 38 (49%) of the corresponding territories, and perfusion on SPECT was abnormal in almost all coronary arteries with a total or subtotal occlusion (11/12, or 92%).
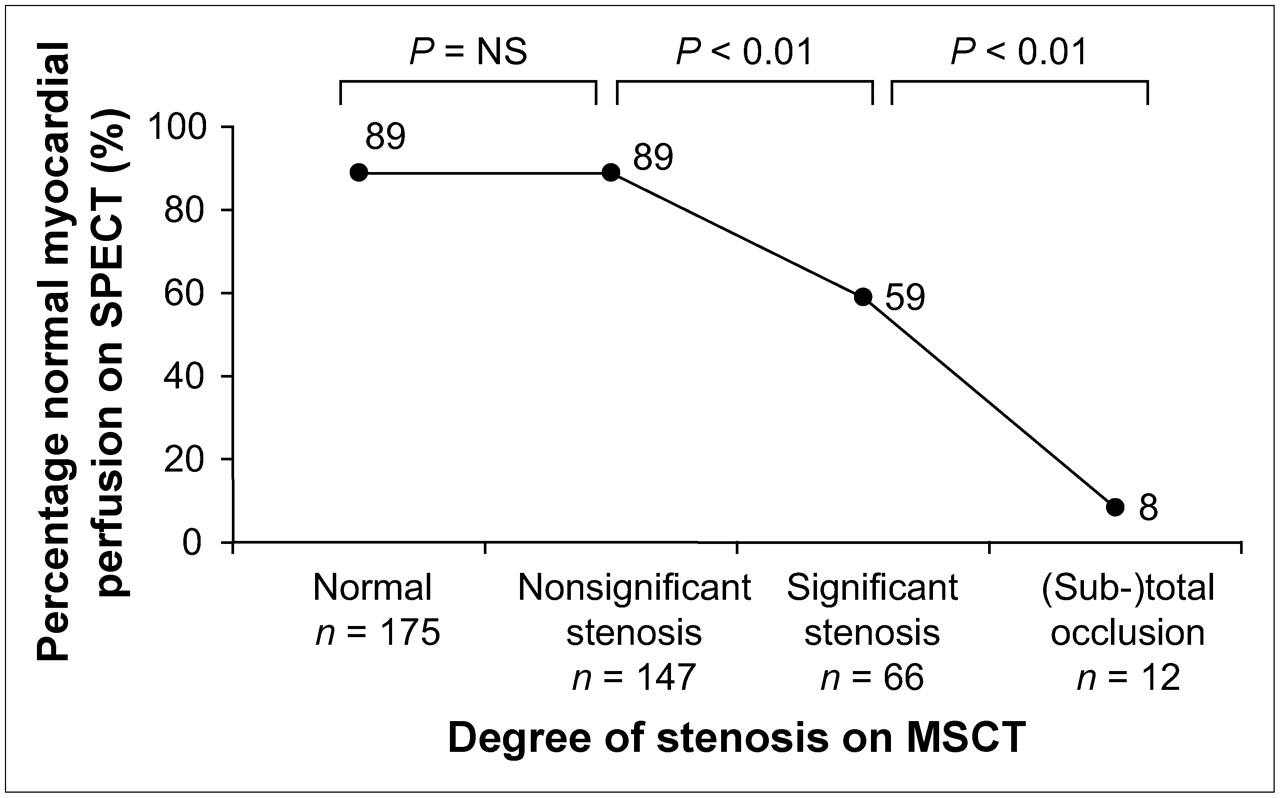
Relationship between stenosis severity on multislice CT (MSCT) and myocardial perfusion on SPECT.
Thus, a normal coronary artery on multislice CT had a high predictive value for normal myocardial perfusion (89%, Fig. 6A); however, normal perfusion on SPECT did not exclude abnormalities on multislice CT, and the value of normal perfusion on SPECT to predict a normal artery on multislice CT was only 48% (Fig. 6B).

Relationship between multislice CT (MSCT) and SPECT: prediction of normal and abnormal perfusion (A) and prediction of normal and significantly or insignificantly stenosed coronary arteries (B).
In Figure 7, the relationship between multislice CT and SPECT is depicted per coronary artery/vascular territory. No significant differences were observed between the different coronary arteries. However, significant stenoses in the right coronary artery tended to result more frequently in abnormal myocardial perfusion on SPECT than did significant stenoses in the left anterior descending and left circumflex coronary arteries, although no statistical significance was reached (P = 0.056).
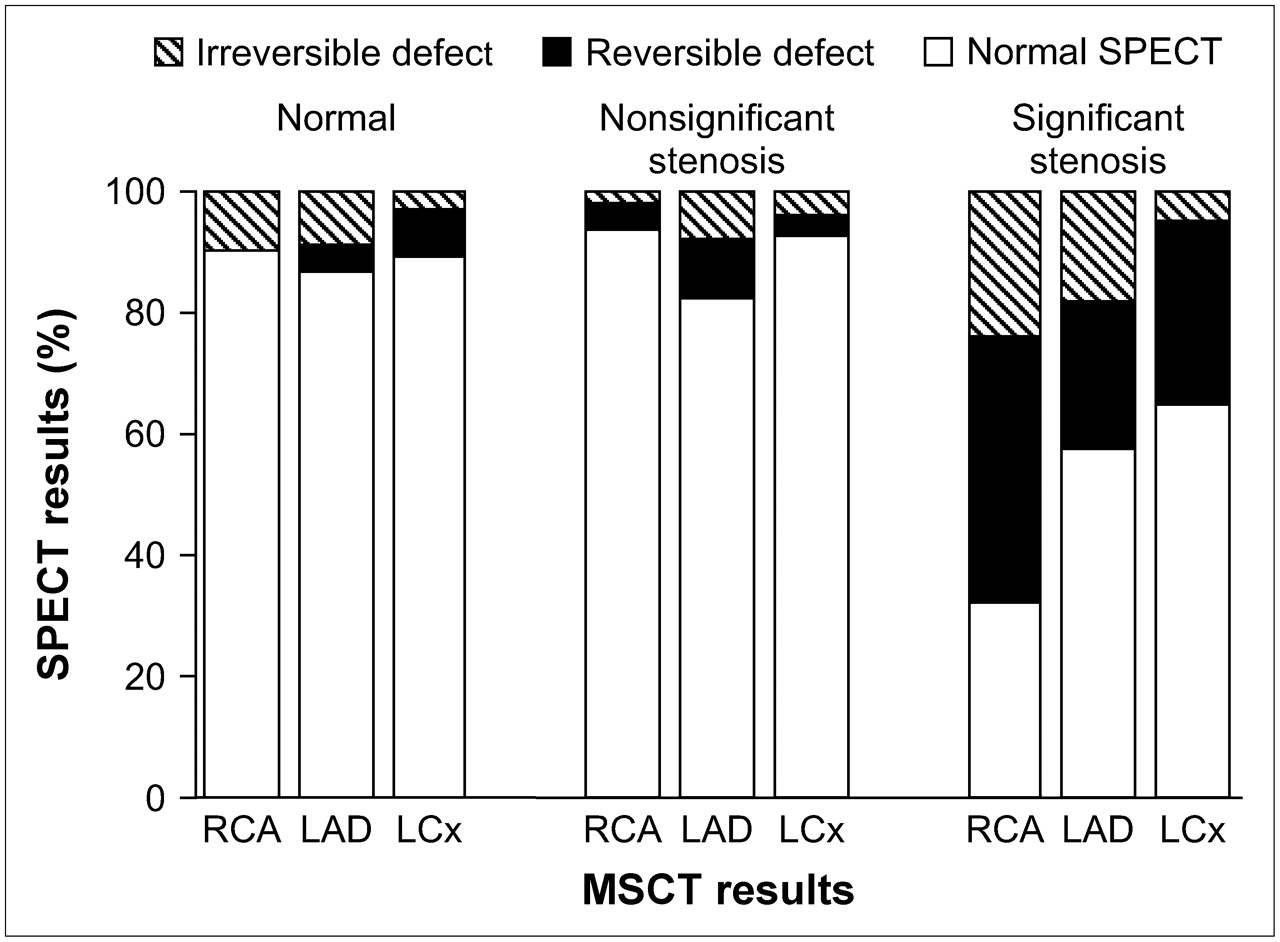
Relationship between multislice CT (MSCT) and SPECT per coronary artery/vascular territory.
Disagreement Between Multislice CT Angiography and SPECT
Normal on Multislice CT Angiography but Abnormal on SPECT.
In 19 vascular territories (5%), abnormal myocardial perfusion was observed whereas multislice CT showed no atherosclerosis in the corresponding coronary artery. In the majority of these vascular territories with abnormal perfusion on SPECT, the observed abnormality was predominantly a small fixed defect (n = 12, or 63%; Fig. 7), with an inferior location in 6 patients and a septal location in 4 patients.
Normal on SPECT but Abnormal on Multislice CT Angiography.
Only 48% of vascular territories with normal perfusion on SPECT corresponded to normal coronary arteries. In most abnormal coronary arteries with normal perfusion (131, or 77%), lesions were insignificant and did not result in ischemia. In 40 vascular territories (10%), myocardial perfusion was completely normal despite significant lesions in the corresponding coronary artery on multislice CT. In these cases, coronary lesions may not have been hemodynamically relevant. Importantly, in 2 patients with a discrepancy between multislice CT and SPECT on a vessel basis, stenosis of both the right coronary artery and the left main coronary artery was present, but only the lesion in the right coronary artery was detected by abnormal perfusion. Finally, in 2 patients with completely normal perfusion on SPECT, 3-vessel disease was demonstrated on multislice CT.
Analysis on a Patient Basis
Multislice CT and SPECT Findings.
The average coronary calcium score per patient was 310 ± 775 (range, 0–6,264). Multislice CT coronary angiography showed normal findings in 43 patients (31%), whereas nonobstructive and obstructive CAD was noted in, respectively, 51 patients (36%) and 46 patients (33%). Normal perfusion on SPECT was noted in 77 patients (55%), whereas abnormal perfusion was noted in 63 patients (45%), corresponding to previous myocardial infarction in 15 patients (11%).
Stenoses on Multislice CT Angiography Versus Coronary Artery Calcium Score.
The average coronary artery calcium score was 3.8 ± 11 for patients with normal coronary arteries and increased to 207 ± 271 and 726 ± 1,239 for patients with insignificant and significant stenoses, respectively (P < 0.001, Kruskal–Wallis). In most patients (n = 45, or 88%) with a coronary calcium score of 10 or less, no significant stenoses were demonstrated. In 20 (35%) of the 57 patients with a calcium score between 11 and 400, significant stenoses were present. This percentage further increased to 65% in patients with a calcium score above 400.
Perfusion on SPECT Versus Coronary Artery Calcium Score.
The average calcium score for patients with normal myocardial perfusion on SPECT was 162 ± 332, whereas a significantly higher calcium score of 580 ± 1,232 was noted for patients with abnormal perfusion on SPECT (P < 0.05, Mann–Whitney).
In most patients without extensive calcium (score ≤ 100) (n = 49, or 78%), perfusion on SPECT was normal. The percentage with normal perfusion was slightly lower (60%) in patients with a calcium score between 101 and 400 (P = NS). Of coronary arteries with calcium scores above 400, the percentage showing normal myocardial perfusion on SPECT was even lower (41%, P = NS).
Perfusion on SPECT Versus Stenoses on Multislice CT Angiography.
In most patients with normal arteries on multislice CT angiography, perfusion on the corresponding SPECT study was normal as well (37/43, or 86%). Of the patients with insignificant stenoses on multislice CT angiography (n = 38, with the exclusion of 13 patients with abnormal perfusion corresponding to previous myocardial infarction), myocardial perfusion on SPECT was normal in 24 (63%). The percentage of SPECT studies showing normal perfusion further decreased to 36% in patients with at least 1 significant stenosis (P < 0.05). Thus, a normal artery on multislice CT angiography had a high predictive value for normal myocardial perfusion on SPECT (86%). However, similar to the vessel-based analysis, normal perfusion on SPECT did not exclude abnormalities on multislice CT angiography, because a normal artery on multislice CT angiography was found in only 37 (48%) of 77 patients with normal perfusion on SPECT.
DISCUSSION
In the present study, imaging of atherosclerosis on multislice CT was compared with imaging of myocardial perfusion on gated SPECT on a coronary-artery basis and a corresponding-vascular-territory basis. Normal coronary arteries on multislice CT were associated with normal perfusion on SPECT in most vascular territories (89%). Moreover, the likelihood of abnormal perfusion on SPECT increased gradually in relation to increasing abnormalities on multislice CT; of the CT studies showing total or subtotal occlusion, 92% were associated with abnormal perfusion on SPECT. Still, 76% of the coronary arteries with atherosclerosis on multislice CT did not exhibit perfusion abnormalities on SPECT, indicating that atherosclerosis frequently does not result in ischemia. Normal perfusion on SPECT was associated with normal arteries on multislice CT in only 48% of vascular territories; 52% of territories with normal perfusion on SPECT had atherosclerosis on multislice CT, with 40% having nonobstructive and 12% having obstructive CAD.
These observations highlight the fact that normal perfusion on SPECT does not exclude atherosclerosis. Accordingly, multislice CT and gated SPECT provide complementary rather than redundant information, because the techniques reflect distinct functional and anatomic pathophysiologic processes.
An Abnormal Artery on Multislice CT Does Not Necessarily Imply Ischemia
Most lesions (76%) on multislice CT did not result in perfusion abnormalities or ischemia on SPECT. In particular, 89% of nonobstructive lesions on multislice CT were not associated with perfusion abnormalities on SPECT. This observation underscores the ability of multislice CT to detect CAD at an earlier stage than can SPECT: Atherosclerosis is detected while perfusion is not yet compromised. Similar results were reported recently for 16-slice CT by Hacker et al., who demonstrated in 25 patients that only 8 (47%) of 17 significant stenoses on multislice CT resulted in abnormal perfusion on SPECT (2). Yet, in the present study, a stepwise increase in the incidence of perfusion abnormalities on SPECT was observed in relation to an increasing severity of atherosclerotic abnormalities on multislice CT (Fig. 5). In particular, total or subtotal occlusions were in 92% of cases associated with abnormal myocardial perfusion on SPECT. Also, less severe but still significant lesions resulted in abnormal perfusion in 41% of vascular territories. These findings illustrate the relationship between the severity of stenosis on multislice CT and the hemodynamic consequences as assessed by SPECT, but the results simultaneously highlight the discrepancy between atherosclerotic plaque burden and ischemia. As a result of variations in stenosis length, composition, angle, and location, as well as the presence or absence of collateral vessels, a stenosis may be incapable of producing symptoms in one patient whereas an apparently identical stenosis causes severe ischemia in another. Indeed, several studies comparing invasive coronary angiography findings with functional testing findings revealed at best a fair agreement, with approximately half the significant lesions showing abnormal myocardial perfusion (2,6). This, by virtue of its relative nature, detects severe reductions in coronary flow reserve while modest reductions in flow reserve may not result in detectable defects (7). Thus, abnormal findings on multislice CT do not necessarily result in abnormal perfusion on SPECT but may more frequently represent nonobstructive atherosclerosis. In patients with abnormal findings on multislice CT, functional testing is therefore mandatory to determine the hemodynamic consequences of those abnormalities.
Normal Perfusion on SPECT Does Not Exclude CAD
In the present study, atherosclerosis was present in 52% of coronary arteries with normal perfusion on SPECT. Moreover, advanced CAD with at least 1 significant, obstructive lesion was noted in 12% of territories with normal perfusion, underlining the fact that normal SPECT findings do not invariably exclude the presence of CAD. Indeed, studies correlating atherosclerosis assessment (based on coronary artery calcium scoring) to SPECT revealed similar observations, namely that extensive coronary calcifications are frequently observed in patients with normal perfusion on SPECT (8,9). These observations may initially appear to be in conflict with the extremely low annual event rate associated with normal SPECT findings—approximately 0.6% for patients without known CAD (10). Nonetheless, among patients with normal SPECT findings, certain subgroups, including patients referred for pharmacologic testing or with substantial comorbidity, have been identified that may actually be at an elevated risk (1.2%–2.0%) (11). In addition, patients with subclinical CAD, as demonstrated by multislice CT, may constitute another category that may have an elevated long-term risk of experiencing coronary events despite normal perfusion on SPECT; this hypothesis needs to be addressed by further outcome-based studies. However, knowledge of the presence and extent of subclinical CAD is still relevant and will help to identify patients who show normal perfusion on SPECT yet have atherosclerosis, thus requiring optimized medical therapy and aggressive lifestyle modification, in contrast to patients who show normal perfusion on SPECT and have no atherosclerosis, who may be reassured without the need for further routine visits to outpatient clinics.
Regional Analysis
Concerning the different coronary arteries and corresponding vascular territories, a relatively larger plaque burden, as reflected by a higher coronary calcium score, was observed in the left anterior descending coronary artery than in the right and left circumflex coronary artery. Also, slightly more abnormalities were encountered in the left anterior descending coronary artery and corresponding vascular territory during coronary angiography and perfusion imaging, respectively. Nonetheless, in the present study, significant stenoses in the right coronary artery tended to result most frequently in abnormal myocardial perfusion on SPECT, as may be attributable to the higher frequency of severe, total or subtotal occlusions in this coronary artery than in the left anterior and left circumflex coronary arteries.
Limitations
Some limitations need to be defined. First, this study related myocardial perfusion on SPECT to atherosclerosis in coronary arteries on multislice CT, and perfect alignment between these methods is difficult because variations in coronary anatomy hamper the precise definition of vascular territories. Also, a threshold of 50% luminal narrowing on multislice CT was applied, whereas a threshold of 70% might have resulted in increased agreement between the 2 techniques. Second, the study population consisted of patients with various clinical presentations, including both suspected and known CAD. Studies performed on more homogeneous populations may provide more uniform results, yet those results may not be generalizable to a “real-life” population referred for evaluation of CAD, such as the one included in the present study. Similarly, the applied stress protocols for gated SPECT were not identical, because they were performed as part of standard clinical routine.
Other limitations included the lack of attenuation correction for SPECT, which may partially explain the (albeit infrequent) abnormal SPECT findings in the presence of completely normal multislice CT findings. Also, no comparison to conventional coronary angiography was available. In addition, data were acquired with 2 different generations of multislice CT scanners, whereas ideally all patients would have been evaluated with 64-slice CT. Finally, several limitations of multislice CT in general need to be acknowledged. The technique involves radiation, and further technical developments are needed to lower the radiation burden. Also, motion artifacts and severe coronary calcifications have been shown to reduce diagnostic accuracy (12,13).
CONCLUSION
The current analysis on a regional basis emphasizes that although a relationship exists between the 2 modalities, multislice CT and SPECT provide complementary information, namely the presence of subclinical atherosclerosis versus the presence of ischemia. Further studies should address how these 2 modalities may be integrated to optimize patient management.
Acknowledgments
This work was financially supported by grant 2002B105 from The Netherlands Heart Foundation.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 16, 2006.
- Accepted for publication August 23, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Coronary Artery Calcium Distribution Is an Independent Predictor of Incident Major Coronary Heart Disease Events: Results From the Framingham Heart Study
- Combined Quantitative Assessment of Myocardial Perfusion and Coronary Artery Calcium Score by Hybrid 82Rb PET/CT Improves Detection of Coronary Artery Disease
- Baseline Subclinical Atherosclerosis Burden and Distribution Are Associated With Frequency and Mode of Future Coronary Revascularization: Multi-Ethnic Study of Atherosclerosis
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Very high coronary calcium score unmasks obstructive coronary artery disease in patients with normal SPECT MPI
- Predictive Value of Multislice Computed Tomography Variables of Atherosclerosis for Ischemia on Stress-Rest Single-Photon Emission Computed Tomography
- Dual-phase multi-detector computed tomography assesses jeopardised and infarcted myocardium subtending infarct-related artery early after acute myocardial infarction
- Combining dual-source computed tomography coronary angiography and calcium scoring: added value for the assessment of coronary artery disease
- The Year in Cardiac Imaging
- Noninvasive Assessment of Plaque Characteristics With Multislice Computed Tomography Coronary Angiography in Symptomatic Diabetic Patients