

Abstract
Metastatic malignancies have limited management strategies and variable treatment responses. Cancer cells develop beside and depend on the complex tumor microenvironment. Cancer-associated fibroblasts, with their complex interaction with tumor and immune cells, are involved in various steps of tumorigenesis, such as growth, invasion, metastasis, and treatment resistance. Prooncogenic cancer-associated fibroblasts emerged as attractive therapeutic targets. However, clinical trials have achieved suboptimal success. Fibroblast activation protein (FAP) inhibitor–based molecular imaging has shown encouraging results in cancer diagnosis, making them innovative targets for FAP inhibitor–based radionuclide therapies. This review summarizes the results of preclinical and clinical FAP-based radionuclide therapies. We will describe advances and FAP molecule modification in this novel therapy, as well as its dosimetry, safety profile, and efficacy. This summary may guide future research directions and optimize clinical decision-making in this emerging field.
- cancer-associated fibroblasts
- fibroblast activation protein
- radionuclide therapy
- PET/CT
- cancer management
- FAPI
Cancer remains a significant cause of mortality and morbidity despite early detection and management advancements. Functional cancer imaging is crucial in staging, response evaluation, restaging, and prognostication. The commonly used molecular imaging radiopharmaceuticals target metabolism (glucose, amino acid, or lipid) and cell surface receptors (e.g., somatostatins and prostate-specific membrane antigen). However, another approach to tumor imaging and novel therapies has recently created interest—that is, targeting of the tumor stroma. As tumors grow, the tumor microenvironment (TME) stimulates the growth of adjacent nonmalignant cells, which play a complex role in tumor pathogenesis.
Cancer-associated fibroblasts (CAFs) are a critical and abundant component of TME. These are involved in tumor progression, including tumorigenesis, neoangiogenesis, metastasis, immunosuppression, and drug resistance (1,2). Activated CAFs have fibroblast activation protein (FAP) α receptors, which are imaged using several small FAP inhibitors (FAPIs). This approach has shown superiority to [18F]-FDG in diagnosing various neoplasms (3–5). However, it is premature to conclude that there is an advantage over [18F]-FDG regarding diagnostic ability, management changes, and cost effectiveness. [68Ga]-FAPI PET/CT shows a remarkably high tumor-to-background ratio. Consequently, a new approach to noninvasive TME characterization, tumor staging, and radioligand therapy has commenced (6). Several preclinical and clinical studies have investigated the role of FAPI-based radionuclide therapy in various malignancies. Preliminary results have shown safety in all studies and efficacy to a variable extent (7–28).
This review provides nuclear medicine physicians with a concise overview of TME, CAFs, and FAPI and their role in tumorigenesis. There is heterogeneity in the origin of CAFs, their subtypes, and their functions. CAFs differ in biomarkers and FAP expression (2,29). These factors become pertinent in deciding the targets for imaging and therapy. The current literature on targeting of CAFs is reviewed, including preliminary results from preclinical and clinical FAPI-based radionuclide therapies. Potential future research areas include selective FAP targeting, FAPI radiopharmaceuticals, the choice of optimal radioisotopes, and follow-up strategies. The evolving role of concurrent chemotherapy and immunotherapy therapy is also covered.
NONTUMOR COMPONENT OF CANCER
TME
Malignant tissue consists of tumor cells and several noncancer components. TME includes nonmalignant components supporting continuous tumor progression and dissemination. TME comprises CAFs, myeloid-derived suppressor cells, immune cells, the extracellular matrix, endothelial cells, and pericytes (1). TME is active and has several tumor–stroma interactions directed by a complex system of cytokines, chemokines, inflammatory molecules, and matrix-remodeling enzymes (30). TME is proposed as an indispensable soil for developing malignant tumor seeds (1).
Origin and Role of CAFs in Tumor Pathogenesis (Fig. 1)
CAFs interact with and evolve with tumor cells. They transform into a protumor phenotype, which enables them to survive, populate, and contribute to tumor development (31). CAFs are derived from normal tissue fibroblasts that are activated by tumor cells. This activation involves stimuli such as oxidative stress, hypoxia, and growth factors from the tumor and immune cells. They may also be recruited from the bone marrow (32). Sometimes CAFs develop from a nonfibroblastic origin by epithelial-to-mesenchymal or endothelial-to-mesenchymal transition (33). Transforming growth factor β (TGF-β), epidermal growth factor, platelet-derived growth factor, and fibroblast growth factor 2 are pivotal to CAF activation (32). Usually, fibroblasts have inhibitory effects on the in vitro proliferation and motility of tumor cells (34), but these modified fibroblasts stimulate tumor progression (1). Modified CAFs help in paracrine signaling, tumorigenesis, neoangiogenesis, metastases, and drug resistance (1). There is heterogeneity in the CAF population. CD146-negative CAFs suppress estrogen receptor expression, and estrogen responsiveness of tumor cells results in tamoxifen resistance. In contrast, CD146-positive CAFs lead to estrogen-dependent proliferation and tamoxifen sensitivity (35). CAFs perform complex functions, and apart from the protumorigenic effect, subsets of CAFs demonstrate a substantial tumor-suppressive effect (36).
NOTEWORTHY
CAFs are abundant cells in TME. There is an increased awareness of the origin, function, and role of CAFs in tumorigenesis.
Novel radionuclides targeting FAP have shown excellent accuracy and tumor-to-background ratios in PET/CT imaging of malignancies.
Preliminary preclinical and clinical studies have demonstrated the potential role of FAPI-based radionuclide therapy in metastasized cancers. The initial result promises safety and an antitumoral effect.
Selective targeting of tumor-promoting CAFs, use of specific FAPI radionuclides with better pharmacokinetic and pharmacodynamic properties, and application of concurrent treatment may open an era in personalized oncology.

Activating pathways, sources, and important functions of CAFs in TME. CAFs may arise from quiescent fibroblasts by physiologic stresses and inflammatory signals, including TGF-β, platelet-derived growth factor, fibroblast growth factor 2, interleukins, and tumor-necrosis factor. Proinflammatory conditions (TGF-β and reactive oxygen species) cause deficiency in base excision repair. This deficiency generates unrepaired DNA strand breaks and may reprogram fibroblasts into CAFs. Other differentiation pathways involve adipocytes, pericytes, and smooth muscle cells. Mesenchymal stem cells may transform into CAFs by epithelial–mesenchymal transition. This pathway involves stimulating molecules such as TGF-β, C–C chemokine ligand 2, C–C chemokine ligand 5, and C-X-C chemokine ligand 12. Endothelial and epithelial cells may also be transformed into CAFs through endothelial-to-mesenchymal transition and epithelial-to-mesenchymal transition. These activated CAFs interact with tumor and immune cells to produce prooncogenic environment. CCL = chemokine ligand; CXCL = C-X-C chemokine ligand; FGF = fibroblast growth factor; IL = interleukin; PDGF = platelet-derived growth factor; PDGFR = platelet-derived growth factor receptor; TNF = tumor-necrosis factor.
CAF Receptors, with Highlights on FAP
Activated CAFs have several upregulated receptors, including FAP, platelet-derived growth factor receptor ß, caveolin 1, CD10, and G-protein–coupled receptors (1). FAP is a type II transmembrane serine protease, and pioneer research was done by Rettig et al. (37). FAP has low expression in normal tissues and appears to be a redundant or nonessential protease in developmental processes. However, it upregulates during various malignant and nonmalignant pathologic processes, including healing, inflammation, and fibrosis. FAP expression has been implicated in various cancer-related signaling pathways. It contributes to tumor progression, invasion, metastasis, immunosuppression, and chemotherapy resistance (38).
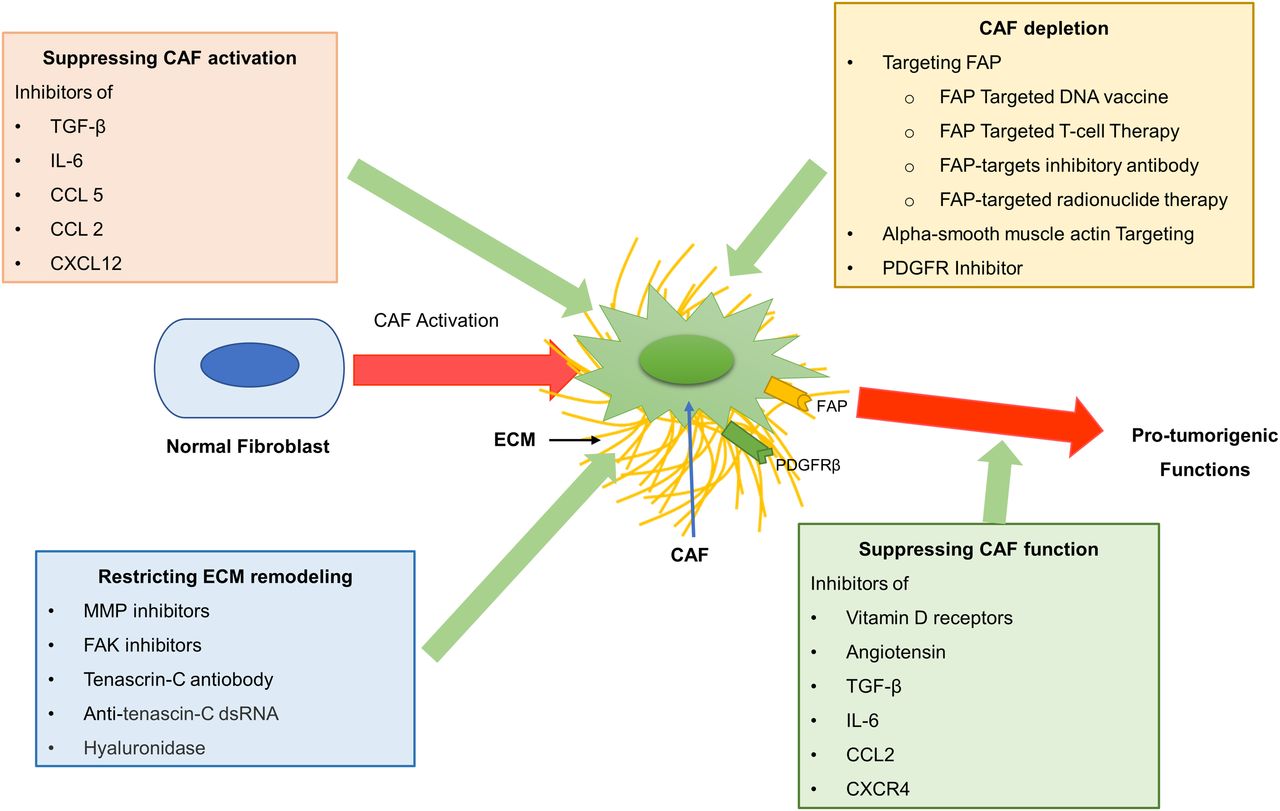
TARGETING OF CAFS AS AN ANTITUMOR TREATMENT (Fig. 2)
Nonradionuclide Targeting Strategies
The role of CAFs in oncogenesis led to research on the development of CAF-directed therapy. Various FAP-targeting strategies have been tried, including anti-FAP monoclonal antibodies (39–41), blocking of FAP enzymatic activity (42), FAP-antigen vaccination (43), genetic deletion (42), and CAR-T cells directed against FAP (44). Sibrotuzumab (antibody against FAP) has been studied in colorectal and non–small cell lung carcinoma. It was well tolerated and safe (40,41). Another possible approach is anticytokine therapy against interleukin-6, C-X-C motif chemokine ligand 12, and TGF-β. These reduce recruitment and CAF activation, decreasing CAF-secreted cytokines and chemokines (1,45). The extracellular matrix is a physical barrier to tumor drug delivery. Targeting of extracellular matrix protein production or degradation of the extracellular matrix favors drug delivery and may enhance the tumoricidal effect (46). AVA6000 is a doxorubicin prodrug that FAP activates and is expected to have enhanced tumor killing with fewer systemic side effects (NCT04969835, Avacta Life Sciences Ltd. A Phase 1, Open Label, Dose-Escalation and Expansion Study to Evaluate the Safety, Pharmacokinetics and Initial Therapeutic Activity of AVA6000, a Novel FAP-activated Doxorubicin Prodrug Administered Intravenously in Patients With Locally Advanced or Metastatic Selected Solid Tumours [Internet]. clinicaltrials.gov; 2023 Apr [cited 2023 Apr 13]. Report No.: NCT04969835. Available from: https://clinicaltrials.gov/ct2/show/NCT04969835). Despite a trial of several drugs, an improved outcome has been shown in only a few preclinical studies. Those drugs that underwent clinical trials had limited success. FAP-targeting immunotherapy has demonstrated a nonselective recognition of FAP-reactive T cells on pluripotent bone marrow stem cells. It led to lethal bone marrow hypocellularity, necrosis, and cachexia (47). The current status of anti-CAF therapies is still in an early-phase clinical trial (48).

{kind=link}
{kind=link}
CAF-targeting strategies for anti-CAF therapies. CAF activation and function can be suppressed by inhibiting signaling pathways leading to activation. These include TGF-β, interleukin-6, C–C chemokine ligand 2, C–C chemokine ligand 5, and C-X-C chemokine ligand 12. CAF depletion may be achieved by targeting FAP, α-smooth muscle actin, and platelet-derived growth factor receptors. Another strategy is to restrict extracellular matrix remodeling by targeting matrix proteins such as matrix metalloproteinases, hyaluronan, tenascin-C, and focal adhesion kinase. CCL = chemokine ligand; CXCL = C-X-C chemokine ligand; dsRNA = double-stranded RNA; ECM = extracellular matrix; FAK = focal adhesion kinase; IL = interleukin; MMP = matrix metalloproteinase; PDGFR = platelet-derived growth factor receptor.
Principle of Targeting CAFs with FAPI-Based Radionuclide Therapy
Other CAF-directed therapy approaches are the radiolabeling of FAPI, peptides, and small-molecule radioconjugates targeting FAP (23,49,50). Radiopharmaceuticals are internalized by CAFs and emit α- or β-particles. α-emitters have theoretic advantages over β-particles for tumoricidal effect. α-emitters create dense ionization, leading to double-strand DNA breaks and unrepairable complex chromosomal rearrangements. This tumoricidal effect is independent of the cell cycle and oxygen level. Treatment with α-emitters may overcome resistance toward β- or γ-irradiation. Short-range α-particles have minimal effects on normal tissues (51). Some tumor cells also express FAP, such as pancreas (52), stomach (53), breast (54), and sarcoma (55). In these scenarios, α-therapy may have a direct tumoricidal effect. However, for other tumors, the radiopharmaceuticals are deposited in CAFs close to targeted tumor cells. Crossfire and bystander effects from long-range, β-particle–emitting radiopharmaceuticals may affect the tumor cells (56). The crossfire effect is particle-induced destruction of cells neighboring tracer-accumulating cells. The radiation-induced bystander effect on cells not exposed to ionizing radiation occurs through free-radical diffusion and stress signal factors from irradiated cells, leading to lethal changes (57).
PRELIMINARY RESULTS ON FAPI-BASED RADIONUCLIDE THERAPY
Lessons from Preclinical Studies
Preclinical in vitro and animal studies aim to accurately model a drug’s desired biologic effect to predict efficacy, safety, and potential toxicities. These studies assess pharmacokinetics, pharmacodynamics, dosing, dosimetry, and side effects. Even after testing of safety in animal studies, high toxicity–related failure rates are noted in human drug trials (58). Tranel et al. compared absorbed dose estimates in 3-dimensional cellular models with CAFs and tumors intermingling (55). The efficacy of [225Ac] decreases as tumor cluster size increases. In such situations, [177Lu] (β-emitter with a longer range) may be more effective because of the crossfire effect. However, with larger (>600–700 μm) cluster sizes, the benefit of 177Lu was also limited (55). The theranostic potential of radionuclide FAPI therapy has been evaluated in preclinical studies. Studies have used FAPI-based radionuclide therapy with 131I (7), 177Lu (8,9,11), and 225Ac (8,10). Several FAPI agents such as FAPI-02 (7), FAPI-04 (10), FAPI-46 (8,9), FAP-2286 (9), and EB-FAPI B1-B4 (11) were used (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). All the studies have shown variable tumor size reduction. However, tumoral uptake, clearance, and tracer retention varied with the agent and tumor type. Watabe et al. used 34 kBq of [225Ac]-FAPI-04 per mouse (10). That corresponds to the 1.5 MBq/kg human dose, higher than the 50–200 kBq/kg dose given for other 225Ac therapies. It shows rapid urinary excretion (89% at 3 h), resulting in low residual radiopharmaceutical for potential therapeutic effect (10). In another mouse study, [177Lu]-FAPI-46 and [225Ac]-FAPI-46 also showed low tumor uptake at 3 h (0.3 percentage injected dose [%ID]/g) and 24 h (0.1 %ID/g), respectively (8). A novel class of FAP-targeting modalities using cyclic peptides as binding motifs has been proposed. FAP-2286 is linked to DOTA and has better binding affinity, selectivity, and plasma stability. It showed a 12- and 9-fold higher time-integrated activity coefficient and tumor-absorbed dose than FAPI-46 (9). The Evans blue–conjugated FAPI-02–based radiotracer [177Lu]-EB-FAPI-B1 has excellent FAP-targeting specificity and tumor retention. It showed remarkable tumor growth suppression in U87MG tumor–bearing mice, with negligible side effects (11).
Preliminary Knowledge from Clinical Studies
Current knowledge on FAPI radionuclide therapy in humans is limited to case reports, case series, and small prospective studies (Supplemental Table 2) (12,14–24,26–28,59,60). The studies have used the β-emitters 90Y, 177Lu, and 153Sm. FAPI agents include FAPI-04 (12,20), FAPI-46 (14,15,20–22,24,26,59), FAP-2286 (23,28), 3BP-3940 (27), SA.FAPI, and (SA.FAPi)2 (17–19). Recently, Baum et al. used 225Ac-based radionuclide therapy in combination with 90Y and 177Lu (27). Patients with diverse malignancies were included in all studies except that of Ballal et al., which included thyroid cancer (19). Overall, the therapy appears safe, with few toxicities and no reportable allergic reactions. Some studies have found grade 3 and 4 hematologic and hepatobiliary toxicities (23,24,26). Toxicities should be interpreted cautiously, given the inclusion of heavily pretreated patients with metastases. Repeated therapy was feasible and safe. Few studies performed posttherapy scanning and dosimetry. In most studies, the dose-limiting organ was the colon or kidneys, with no safety concerns. The average radiation dose of [90Y]-FAPI-46 for kidney and bone marrow was comparable to that of [177Lu]-FAP-2286 and [177Lu]-FAPI-46 (16,23,26). Tumor dosimetry (Supplemental Table 3) varied among the studies and among metastatic lesions in the same patient (16–20,23,24,26). Some studies found poor tumoral uptake and rapid washout (60). Absorbed dose and effective half-life differ among the various FAPI agents.
Early studies reported disease progression or stable disease (15–17,21–25). Recent studies have reported partial responses to novel therapy (19,26,28). Fendler et al. evaluated RECIST/PERCIST responses up to 18 mo after radionuclide therapy (26). Median overall survival was significantly longer for RECIST responders (P = 0.013). Higher survival was noted in those with a partial response or stable disease (14.4 mo) than in those with progressive disease (6.6 mo) after [90Y]-FAPI-46 therapy. However, a partial response and stable disease were seen in sarcoma patients (26). The fact that sarcomas express FAP receptors on tumor cells could result in a higher tumor dose and tumoricidal effect. A complete response to FAPI therapy has not been documented. However, some published images have shown promising results (19,28). Some studies have reported follow-up imaging with [68Ga]-FAPI PET/CT. Only Fendler et al. used [18F]-FDG PET/CT in the follow-up (26). Tumor marker (serum thyroglobulin) correlation is available only for the study that included thyroid cancer patients (19).
Limitations of Existing Research and Literature
[68Ga]-FAPI PET/CT has shown excellent accuracy in detecting malignant lesions. Several studies have shown advantages over [18F]-FDG PET/CT (3–6). Most studies have not been histopathologically validated. Tumors can have variable expression of CAFs and FAP. Mona et al. studied FAP expression using immunohistochemistry on a pan-cancer human tissue microarray (61). FAP was expressed across several cancer types with variable intensity and frequency, ranging from 25% to 100% (mean, 76.6% ± 25.3%). Low expression of FAP in the tumor may lead to a false-negative scan. Microscopic metastases, lesions near the physiologic uptake site, and small lesion size can be causes of a false-negative scan (61–63). Several trials (NCT04504110, Peking Union Medical College Hospital. A Prospective Study to Evaluate 68Ga-FAPI-04 and 18F-FDG PET/CT in Patients With Epithelial Ovarian Cancer: Compared With Histological Findings [Internet]. clinicaltrials.gov; 2020 Aug [cited 2023 Apr 13]. Report No.: NCT04504110. Available from: https://clinicaltrials.gov/ct2/show/NCT04504110; NCT04459273, Jonsson Comprehensive Cancer Center. PET Biodistribution Study of 68Ga-FAPI-46 in Patients With Different Malignancies: An Exploratory Biodistribution Study With Histopathology Validation [Internet]. clinicaltrials.gov; 2023 Mar [cited 2023 Apr 13]. Report No.: NCT04459273. Available from: https://clinicaltrials.gov/ct2/show/NCT04459273; NCT04457232, Jonsson Comprehensive Cancer Center. PET Biodistribution Study of 68Ga-FAPI-46 in Patients With Prostate Cancer: A Prospective Exploratory Biodistribution Study With Histopathology Validation [Internet]. clinicaltrials.gov; 2023 Mar [cited 2023 Apr 13]. Report No.: NCT04457232. Available from: https://clinicaltrials.gov/ct2/show/NCT04457232; and NCT05209750, The Netherlands Cancer Institute. Pilot Study of FAPI PET/CT for Locoregional (re)Staging of Lymph Nodes in Colorectal Carcinoma [Internet]. clinicaltrials.gov; 2022 Aug [cited 2023 Apr 13]. Report No.: NCT05209750. Available from: https://clinicaltrials.gov/ct2/show/NCT05209750) are exploring the role of [68Ga]-FAPI PET/CT along with histopathologic validation for assessing diagnostic accuracy. A multimodal imaging approach and careful interpretation of clinical and pathologic data are essential to ensure accurate cancer diagnosis and management. The current understanding of FAP radionuclide therapy is based on small studies with limited follow-up. The main goal was to evaluate safety and perform a preliminary assessment of efficacy. It is difficult to draw meaningful conclusions because of the patient diversity, type of tumor, metastatic burden, previous therapies, FAPI ligand used, and radionuclide used. Patients have had suboptimal performance scores and poor expected survival. Long-term follow-up data are unavailable to evaluate disease progression, morbidity, and mortality.
CHALLENGES AHEAD AND POTENTIAL AREAS OF FUTURE RESEARCH
Selective Targeting of Tumor-Promoting CAFs and FAP Receptors
Most currently available anticancer agents target tumor cells, ignoring TME. Interest in TME-directed imaging and therapy research is expanding because of recognition of the importance of TME (48). Significant heterogeneity in origin, biomarkers, subtype, FAP expression, and CAF functions have been noted (29). CAF subsets are noted in triple-negative breast cancer, with various properties and levels of activation. The CAF-S1 subset is associated with an immunosuppressive microenvironment and expresses FAP. However, CAF-S2, CAF-S3, and CAF-S4 do not express FAP (2). Özdemir et al. observed that depleting the myofibroblast population in pancreatic ductal adenocarcinoma led to immunosuppression in animal models (36). It resulted in cancer progression with poor survival (36). This observation suggests that nonselective targeting of tumor-suppressive CAFs may be ineffective or even deleterious (1).
FAP expression is heterogeneous among tumors and even among different metastatic sites. Normal fibroblasts show minimal FAP expression. Uterus and breast usually show mild FAP expression but have sometimes shown intense uptake (64). Colon and pancreatic cancers have shown high desmoplastic reactions but moderate [68Ga]-FAPI uptake (6). FAP expression is also associated with several benign etiologies. These include cardiovascular (myocardial infarction, atherosclerosis), musculoskeletal (degenerative disease), hepatobiliary (focal nodular hyperplasia, pancreatic lesions), and IgG4-related diseases (65). It is prudent for theranostics to rule out the benign and inflammatory FAP expression that may occur in healing, chronic inflammation, and physiologic uptake (65,66).
Changes in Structure and Properties of FAPI Radiopharmaceuticals
Diagnostic and therapeutic applications of radiopharmaceuticals need specific and rapid tracer uptake. Small-molecule FAPIs (UAMC-1110) are based on the 4-quinolinyl-glycyl-2-cyanopyrrolidine scaffold and have overcome the disadvantages of pyrrolidine-2-boronic acid derivatives of FAP antibody B12 IgG. They have nanomolar FAP affinity with high selectivity (67). Recent research has focused on chemical modification to achieve superior pharmacokinetics (5). It resulted in rapid internalization and fast circulatory clearance, with high-contrast imaging even 10 min after administration (5).
Pharmacokinetic prerequisites for therapeutic radiopharmaceuticals include prolonged blood circulation, serum stability, lessened nonspecific uptake, and persistent tumor retention. These characteristics result in a high effective half-life and tumor radiation dose, facilitating minimization of the radiation dose to healthy surrounding tissue and systemic toxicity and allowing higher administered doses to patients. The pharmacokinetics of FAPI-01 and FAPI-02 were reported in 2018. FAPI-02 had improved binding affinity to human FAP compared with FAPI-01 (68). Lindner et al. did a preclinical pharmacokinetics study on tumor-bearing animals, studying 15 synthesized FAPIs (FAPI-02 to FAPI-15) (12). They found FAPI-04 to be the most promising tracer for clinical application. Given the low FAPI retention time of FAPI-02 and FAPI-04, Loktev et al. further developed several other derivatives (69). FAPI-21, FAPI-36, FAPI-46, and FAPI-55 demonstrated higher tumor uptake than FAPI-04. Progressively increasing tumor uptake was noted in FAPI-21 from 1 to 4 h. FAPI-21 revealed the highest 24-h tumor retention (6.03 ± 0.68 %ID/g), followed by FAPI-35 and FAPI-46. Slow clearance and high retention were noted for FAPI-21 at 24 h (64% of the maximum tumor activity), followed by FAPI-35 (37%), FAPI-46, and FAPI-55 (∼20% each). However, FAPI-21 had physiologic uptake in oral mucosa, thyroid, and salivary glands (69). FAPI-46 has better pharmacokinetics than FAPI-04. DOTA ligand is used as a chelator for FAPI-46, which makes it a suitable agent to label with 90Y, 177Lu, and 153Sm (13–16,21,22,24,25).
Moon et al. reported FAPI derivatives (DOTA.SA.FAPI and DATA5m.SA.FAPI) created by replacing the heterocyclic nitrogen portion of FAPI-04 to form a squaramide unit (70). The Moon et al. group reported transforming FAPI into a homodimeric system (70). DOTA (SA.FAPI)2 and DOTAGA (SA.FAPI) have 2 inhibitor groups. Compared with monomers, these have an excellent affinity to FAP, slower renal excretion, and longer blood pool retention (70). Ballal et al. have studied these in various cancers (17–19). [68Ga]-FAP-2286 showed tumor uptake similar to that of [68Ga]-FAPI-46. However, [177Lu]-FAPI-2286 showed excellent retention at 24 and 72 h compared with [177Lu]-FAPI-46 (15.8 vs. 3.8 %ID/g, respectively [P = 0.001], and 16.4 vs. 1.6 %ID/g, respectively [P = 0.002]). Significantly sustained suppressed tumor growth was seen in FAP-2286–treated animals compared with FAPI-46–treated animals (metabolic tumor volumes, 12 vs. 1,210 mm3; P < 0.0001) (71). The tumor half-life of FAP-2286 (44 h for bone metastases) is prolonged compared with FAPI-02 and FAPI-04. Nevertheless, the effective tumor half-life is still shorter than the tumor half-life of PSMA-based radioligand therapy (23,72).
Albumin-binding FAPIs (TE-FAPI-01 to TE-FAPI-04) have an increased blood concentration and delayed excretion and are stable in saline and plasma. They have high FAP-binding affinity with minimum physiologic uptake. TE-FAPI-03 and TE-FAPI-04 exhibited persistent tumor accumulation 24 h after administration (2.84 ± 1.19 %ID/g and 3.86 ± 1.15 %ID/g, respectively) (73). Albumin binder–truncated Evans blue ([177Lu]-EB-FAPI-B1) has shown excellent pharmacokinetics and tumoricidal effect (11). Zhao et al. have synthesized DOTA-2P(FAPI)2 with 2 FAPI-46 monomers (74). Multimerization increased tumor uptake and retention compared with [68Ga]-FAPI-46. There is a need for a pan-tumor-imaging–specific FAP radiopharmaceutical that localizes in protumor CAF subpopulations and precludes tumor-suppressive CAFs and inflammatory fibroblasts.
Choice of Radionuclide for Radionuclide Therapy
The radiation dose delivered to the target depends on type of particle, range, half-life, and energy. α-particle–based therapy might kill the CAFs but may have a minimal direct effect on tumor cells. At the same time, the inverse is true for β-particles. Another ideal characteristic is to have a radionuclide’s half-life coincide with a radiopharmaceutical’s retention half-life. Otherwise, the result would be a higher radiation dose and possible side effects once the radioligand is released from the target. The initial FAPI molecules had a short retention time. Thus, 90Y, which has a higher energy per decay and a shorter half-life, was more suitable for labeling (26). With improvement in tumor retention in newer FAPI tracers, the radionuclides with a longer half-life, such as 177Lu, 131I, or 225Ac, will be helpful. Combined use of α- and β-emitting compounds is also proposed. This strategy involves one carrier molecule labeled with both emitters. However, superiority over the single emitter remains unexplored (56). Rosar et al. evaluated treatment responses of [225Ac]-PSMA-617/[177Lu]-PSMA-617 tandem therapy in prostate cancer patients who had progressed on [177Lu]-PSMA-617 monotherapy (75). A partial response and stable disease were noted in 5 (29.4%) and 7 (41.2%) patients, respectively. Baum et al. reported the human results of a theranostic approach using combinations (177Lu + 225Ac and 90Y + 225Ac) with the FAP-binding peptide 3BP-3940 (27). The preliminary result showed safety and feasibility. However, the superiority of the α-particle–based therapy over β-emitters may not be replicated in FAPI-based therapy. Animal studies have shown marginal superiority for [177Lu]-FAPI-46 compared with [225Ac]-FAPI-46. A likely explanation is the inefficient energy transfer by α-emission from the stroma to the tumor (8).
Assessment of Response to Radionuclide Therapy, Follow-up Imaging, and Selection of Endpoint of Therapy
There are several ongoing trials for FAPI therapy (Supplemental Table 4). Most include a heterogeneous patient population with different malignancies and multiple tracers. These trials are phases I and II and evaluate feasibility and safety. However, tumor response assessment and survival analysis will be complex and challenging. Repetitive invasive biopsy for primary tumors and metastatic disease is impractical. Assessing the tumor size seems straightforward. However, RECIST for response assessment has significant pitfalls, including baseline selection of lesions and reassessment of the target, nontarget, and new lesions (76). After FAPI radionuclide therapy, size may decrease as CAFs form a significant part of tumor. Tumor cell number may remain unchanged. Some preclinical studies have noted an initial decrease in size followed by rapid tumor growth (8). Response evaluation with the FAPI-based diagnostic tracer may not reflect tumor burden if there is a transient fall in CAFs or FAP expression. Another surrogate tumor marker, such as [18F]-FDG PET/CT, might give a holistic evaluation. There is a possibility of obtaining false-positive results from ongoing inflammation after radionuclide therapy.
Concurrent Treatment Options for Synergistic Effect
The role of TME in treatment resistance and disease recurrence is largely ignored in cancer management. Dense fibrosis hinders drug delivery by creating an extracellular matrix barrier, elevated interstitial pressure, and stromal cytochrome P450–mediated drug degradation. CAFs suppress immune cells. Drug resistance may be due to decreased hormonal receptors in prostate and breast cancer (48). Targeting CAFs by inhibiting surface markers (FAP and α-smooth muscle actin) has been tested in phase I clinical trials of colorectal and lung carcinoma. Sibrotuzumab (antibody against FAP) was safe, with limited efficacy (40,41). Similarly, Val-boroPro (inhibitor of FAP enzymatic activity; Talabostat, Point Therapeutics, Boston, MA) was used in phase II trials in patients with metastatic colorectal cancer, with minimal clinical activity (77). Several trials have combined antitumor treatment and CAF inhibitors to overcome these obstacles. Metastatic pancreatic cancer patients who are not responding to gemcitabine were given ruxolitinib (JAK1/JAK2 inhibitor) combined with capecitabine. The patients had longer overall survival with better prognoses (78). Depletion of FAP-positive CAFs demonstrated the enhanced antitumor effects of programmed-death ligand 1 immunotherapy. T-cell accumulation was noted in the autochthonous model of pancreatic ductal adenocarcinoma, resulting in diminished cancer cells (79). These findings indirectly indicated that treatment strategies targeting CAFs alone may be less effective.
Many ongoing nonradionuclide therapy trials have proposed a combination of treatment strategies. Clinical trials targeting Wnt/b-catenin signaling related to CAFs in colorectal cancer (NCT04094688, Alliance for Clinical Trials in Oncology. Randomized Double-Blind Phase III Trial of Vitamin D3 Supplementation in Patients With Previously Untreated Metastatic Colorectal Cancer (SOLARIS) [Internet]. clinicaltrials.gov; 2023 Mar [cited 2023 Apr 13]. Report No.: NCT04094688. Available from: https://clinicaltrials.gov/ct2/show/NCT04094688; high-dose vitamin D3 with FOLFOX/FOLFIRI and bevacizumab), pancreatic cancer (NCT03520790, MD KP. Vitamin D Receptor Agonist Paricalcitol Plus Gemcitabine and Nab-paclitaxel in Patients With Metastatic Pancreatic Cancer [Internet]. clinicaltrials.gov; 2023 Jan [cited 2023 Apr 13]. Report No.: NCT03520790. Available from: https://clinicaltrials.gov/ct2/show/NCT03520790; paricalcitol with gemcitabine and nab-paclitaxel), and gynecologic cancer (NCT03192059, University Hospital, Ghent. A Phase II Investigation of Pembrolizumab (Keytruda) in Combination With Radiation and an Immune Modulatory Cocktail in Patients With Cervical and Uterine Cancer (PRIMMO Trial) [Internet]. clinicaltrials.gov; 2021 Sep [cited 2023 Apr 13]. Report No.: NCT03192059. Available from: https://clinicaltrials.gov/ct2/show/NCT03192059; cyclophosphamide with lansoprazole, pembrolizumab, and radiotherapy) have incorporated various chemotherapeutic agents. Pathways involving interleukin-6 and TGF-β have been targeted by the anti–interleukin-6 antibody tocilizumab in pancreatic cancer (NCT02767557, MD IC. A Multinational, Randomized, Phase II Study of the Combination of Nab-Paclitaxel and Gemcitabine With or Without Tocilizumab, an IL-6R Inhibitor, as First-line Treatment in Patients With Locally Advanced or Metastatic Pancreatic Cancer. [Internet]. clinicaltrials.gov; 2023 Feb [cited 2023 Apr 13]. Report No.: NCT02767557. Available from: https://clinicaltrials.gov/ct2/show/NCT02767557, with nab-paclitaxel and gemcitabine), melanoma (NCT03999749, NYU Langone Health. A Phase II Study of the Interleukin-6 Receptor Inhibitor Tocilizumab in Combination With Ipilimumab and Nivolumab in Patients With Unresectable Stage III or Stage IV Melanoma [Internet]. clinicaltrials.gov; 2023 Jan [cited 2023 Apr 13]. Report No.: NCT03999749. Available from: https://clinicaltrials.gov/ct2/show/NCT03999749, with nivolumab and ipilimumab), and prostate cancer (NCT03821246, Fong L. An Open-Label Multi-Center Phase II Study of Neoadjuvant Atezolizumab-Based Combination Therapy in Men With Localized Prostate Cancer Prior to Radical Prostatectomy [Internet]. clinicaltrials.gov; 2022 Oct [cited 2023 Apr 13]. Report No.: NCT03821246. Available from: https://clinicaltrials.gov/ct2/show/NCT03821246, with atezolizumab and etrumadenant). Bintrafusp, a bifunctional antibody against TGF-β and programmed-death ligand 1, is being studied in esophageal cancer (NCT04481256, Laarhoven HWM van. TGF-β And PDL-1 Inhibition in Esophageal Squamous Cell Carcinoma Combined With Chemoradiation TheRapY [Internet]. clinicaltrials.gov; 2022 Dec [cited 2023 Apr 13]. Report No.: NCT04481256. Available from: https://clinicaltrials.gov/ct2/show/NCT04481256) along with paclitaxel, carboplatin, and radiotherapy. Simlukafusp alfa (RO6874281) immunocytokine is being tried in combination with pembrolizumab in melanoma (NCT03875079, Hoffmann-La Roche. An Open-Label, Multicenter, Phase Ib Study To Evaluate Safety And Therapeutic Activity Of RO6874281, An Immunocytokine, Consisting Of Interleukin-2 Variant (IL-2v) Targeting Fibroblast Activation Protein-A (FAP), In Combination With Pembrolizumab (Anti-PD-1), In Participants With Advanced Or Metastatic Melanoma [Internet]. clinicaltrials.gov; 2023 Mar [cited 2023 Apr 13]. Report No.: NCT03875079. Available from: https://clinicaltrials.gov/ct2/show/NCT03875079). Results from these trials may reshape advanced tumor management. Investigating radionuclide therapy in conjunction with chemotherapy and immunotherapy will be worthwhile.
CONCLUSION
CAFs remain a dominant cell type in TME and are a worthwhile target for novel anticancer therapies. Nonradioisotopic and FAP-based radionuclide approaches against CAFs have shown variable responses in preclinical and clinical studies. FAPI-based radionuclide therapy has shown encouraging outcomes despite CAF heterogeneity, variable FAP expression, radiopharmaceutical challenges, diversity in patient selection, and advanced malignancies. We are only beginning to understand the potential of FAP-based radionuclide therapy. Extensive research on FAPI ligands is under way. Combining FAP radionuclide therapy with chemotherapy and immunotherapies remains an unexplored research area. Detailed insight into CAF biology, radiopharmacy, and dosimetry may open a new area of precise and personalized oncology.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 1, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- Received for publication February 13, 2023.
- Revision received March 30, 2023.