

Abstract
ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) established the prognostic significance of 123I-metaiodobenzylguanidine (123I-MIBG) imaging in heart failure subjects (median follow-up, 17 mo) using a composite endpoint dominated by heart failure progression. The ADMIRE-HF extension (ADMIRE-HFX) extended follow-up to a median of 24 mo and used mortality as the primary endpoint. The objective of these analyses was to use multiple multivariate risk modeling techniques to determine the independent predictive ability of 123I-MIBG imaging for mortality outcomes. Methods: Data from 964 New York Heart Association class II–III subjects in ADMIRE-HFX were included. All-cause mortality and a composite endpoint of death or death-equivalent events (resuscitated arrest, successful defibrillation for ventricular tachycardia or ventricular fibrillation) were analyzed with multivariate Cox proportional hazards and logistic regression techniques using demographic and clinical variables and the 123I-MIBG heart-to-mediastinum ratio (H/M). The incremental value of H/M was also examined for the logistic regression models using receiver-operating-characteristic curve methods and for the proportional hazards models using net reclassification improvement. Results: There were 101 deaths, and 136 subjects had a composite event during follow-up. H/M was significant in all multivariate proportional hazards and logistic regression models for the 2 mortality endpoints, both models developed with only clinical variables and those including left ventricular ejection fraction and b-type natriuretic peptide (BNP). For baseline models including BNP, the addition of H/M did not significantly increase receiver-operating-characteristic curve area. However, there was significant net reclassification improvement with the addition of H/M to a proportional hazards model containing BNP and left ventricular ejection fraction. Conclusion: The multivariate Cox proportional hazards and logistic regression analyses demonstrated consistent significance for H/M when added to the baseline risk models for mortality and mortality-equivalent events.
- cardiac 123I metaiodobenzylguanidine imaging
- neurohormones
- prognosis
- ventricular arrhythmias
Heart failure (HF) is associated with damage to sympathetic neurons, with resultant deleterious alterations in the homeostatic regulation of heart rate, blood pressure, and myocardial contractile function (1). The potential utility of assessing myocardial sympathetic neurons with nuclear imaging using the norepinephrine analog 123I-metaiodobenzylguanidine (123I-MIBG) (2,3) has been extensively evaluated as a prognostic indicator in HF patients (4–8). The largest prospective study to demonstrate prognostic significance for the planar heart-to-mediastinum ratio (H/M) in HF subjects was ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) (9).
Although ADMIRE-HF met its primary and key secondary efficacy endpoints, concerns about the significant reliance on HF progression, a relatively subjective endpoint, persist. Despite the importance of cardiac sympathetic innervation for HF patient morbidity and mortality (1,10,11), there remain questions about how the imaging results and associated risk estimates can be incorporated into patient-management decision making. These questions led to the performance of new primary analyses based on all-cause mortality, the endpoint that is most relevant and least subject to bias. These analyses were supplemented with additional analyses of a composite mortality endpoint including events that likely would have resulted in death in the absence of intervention.
The new analyses of the ADMIRE-HF extension (ADMIRE-HFX) study (12), which focused specifically on mortality prediction, were designed to determine, first, whether planar H/M, as a global measure of myocardial uptake, was a reliable indicator of mortality risk; second, the relative importance of cardiac sympathetic innervation as an indicator of mortality risk versus other established clinical measurements; and third, whether 123I-MIBG imaging had utility beyond that of currently used prognostic markers. The present analyses used 2 different coprimary analysis methods (proportional hazards and logistic regression) suggested by the U.S. Food and Drug Administration, to which the results were submitted before U.S. approval of 123I-MIBG for cardiac imaging in 2013.
MATERIALS AND METHODS
Patient Population
The ADMIRE-HF efficacy population has been described in previous publications (12,13). The population consisted of 964 New York Heart Association class (NYHA) II–III HF patients on guideline-recommended medical therapy and on-site determination of a left ventricular ejection fraction (LVEF) of no more than 35%. The trial was closed after the prespecified number of events had been achieved at a median subject follow-up of 17 mo (from the date of 123I-MIBG imaging). In ADMIRE-HFX, 470 surviving patients who had not reached 2 y of follow-up provided new informed consent and underwent additional data collection until 2 y. One hundred forty-nine other potentially eligible subjects did not provide informed consent, for the following reasons: 70 were originally enrolled at sites that did not participate in ADMIRE-HFX; 34 declined participation; 16 could not be located; 25 whose last contact in ADMIRE-HF was between 21 and 23 mo after 123I-MIBG administration were not approached; and 3 died shortly after termination of the original study. For all 56 participating centers in ADMIRE-HFX, the study was approved by the Institutional Review Boards or Ethics Committees. The combined dataset from the original and extension trials was used for the present analyses.
Data Collection and Data Analyses
As previously described, all subjects received 370 MBq (10 mCi ± 10%) of 123I-MIBG (AdreView; GE Healthcare) and underwent planar imaging of the anterior thorax on a nuclear camera equipped with low-energy, high-resolution collimators (13). Derived consensus H/M results from 3 independent masked interpretations of 4-h planar images (10-min scans that began at 3 h 50 min) were used in all analyses (9).
All demographic, medical history, and medication usage data were collected before administration of 123I-MIBG. LVEF was based on on-site interpretation of echocardiograms (n = 865; 90%), electrocardiography-gated SPECT myocardial perfusion imaging (n = 81; 8%), and other techniques (n = 18; 2%). Blood samples for b-type natriuretic peptide (BNP) were drawn at screening and were processed at a central core laboratory. However, the blood samples for 38 subjects were damaged or lost in transit; therefore, determinations of BNP were available for 926 subjects (96%).
The primary endpoint was all-cause mortality; the clinical adjudication committee of HF cardiologists (5 in ADMIRE-HF, 4 of the same 5 in ADMIRE-HFX) reviewed all death records, categorized all deaths as either cardiac or noncardiac, and subcategorized cardiac deaths as due to progressive HF, sudden death, myocardial infarction, or other causes. Exploratory analyses used the composite endpoint of all-cause mortality, resuscitated cardiac arrest, and defibrillation for ventricular tachycardia or fibrillation. The latter events were determined from source documents, including implantable cardioverter-defibrillator (ICD) interrogation reports. This composite endpoint was judged the closest approximation for estimating what all-cause mortality rates would have been in the absence of life-saving intervention (14).
Two series of multivariate analyses were performed for each endpoint. In each series, an analysis was performed using clinical and laboratory variables only, and then the analysis was repeated with H/M (treated as a continuous variable) included. The first analyses used the following variables, designated the “primary list of factors,” with all variables but age and body mass index treated as categoric: age, sex, race (white, black, or other), history of hypertension, history of dyslipidemia, current or past smoking, diabetes, etiology of HF (ischemic or nonischemic), body mass index, use of an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker at baseline, use of a β blocker at baseline, use of lipid-lowering drugs at baseline, and NYHA class. The second analyses used the primary list of factors with the addition of LVEF and plasma BNP (treated as continuous variables), with the augmented list designated the “secondary list of factors.” Because of the large range of BNP values (2.5 to >3,900 ng/L), a logarithmic transformation was used for this variable.
Two coprimary analyses were performed. The first was a multivariable Cox proportional hazards regression model for time-to-mortality event with and without H/M (with H/M hazard ratios [HRs] based on a 1-unit change in this parameter). The second was a multivariable logistic regression model for time-to-mortality event, including comparison of the area under the curve (AUC) of the receiver-operating-characteristic (ROC) curves for the models with and without H/M (15,16). For these latter analyses, subjects censored alive before the minimum follow-up time were excluded. Because 24-mo follow-up was defined as 24 mo ± 30 d, subjects with a minimum of 23 mo of follow-up were included in the 2-y logistic regression analyses. A backward-elimination stepwise procedure was used in building each model. Factors significant at a probability level of less than 0.05 were retained in the final models. Relative risks (with 95% confidence limits) were also calculated.
Net reclassification improvement was calculated for Cox proportional hazards models without and with H/M (17).
Kaplan–Meier survival analyses were also performed, both using H/M as a categoric variable with 0.1-unit increments (reflecting an estimate of precision of the measurement to a single decimal place) and using categories based on the population H/M mean and SD rather than the prospectively defined dichotomy at an H/M of 1.60 (9). All statistical analyses were performed using SAS software, version 9.2 or higher (SAS Institute).
RESULTS
Clinical Characteristics
Three subjects did not have derived consensus H/Ms (2 subjects without core laboratory image interpretations and 1 subject with a consensus interpretation of nondiagnostic). Therefore, analyses based on clinical variables included a maximum of 964 subjects, whereas analyses including H/M had a maximum of 961. Median follow-up was 24 mo. Four hundred twelve subjects (43%) had an ICD at some time during the study, including 188 (19%) at study entry. During follow-up, there were 101 deaths (10.5%).
On the basis of demographic and clinical information (Table 1), subjects who died were older and had a lower LVEF, a longer QRS duration, and worse renal function than survivors. Survival probability was 94.6% at 1 y and 88.3% at 2 y.
Baseline Clinical Characteristics of Study Subjects
All-Cause Mortality
Cox Proportional Hazards Analysis
The univariate HR for H/M was 0.07 (95% confidence interval [CI], 0.02–0.21; P < 0.001). Multivariate analyses are summarized in Table 2. Age was the only significant predictor in the primary list of factors (HR, 1.04). H/M was a significant additional predictor (HR, 0.08; P < 0.001). In the secondary list of factors, the model contained 2 variables: age (HR, 1.02) and log BNP (HR, 4.80). H/M was a significant additional predictor (HR, 0.23; P = 0.016).
Cox Proportional Hazards Analysis for All-Cause Mortality
Multivariate Logistic Regression with ROC Curve Comparisons
The logistic regression analyses are summarized in Tables 3 and 4. In all 1- and 2-y analyses, H/M was a significant additional predictor. However, only for models with the primary list of factors did the addition of H/M improve the AUC of the ROC (P = 0.027 at 1 y, P = 0.058 at 2 y). The addition of H/M did not significantly increase the AUCs for models including log BNP.
Multivariate Logistic Regression Model and ROC Curve Analysis for 1-Year All-Cause Mortality
Multivariate Logistic Regression Model and ROC Curve Analysis for 2-Year All-Cause Mortality
Composite Endpoint of All-Cause Mortality, Resuscitated Cardiac Arrest, and ICD Defibrillation Therapy for Ventricular Tachycardia or Fibrillation
Among the 964 HF subjects in the population, the composite endpoint occurred in 136 (14.1%), including 7 subjects with resuscitated cardiac arrest and 36 with ICD defibrillations. The 101 subjects who died included 2 who underwent resuscitation and 6 with ICD defibrillation as a first event. Among the 961 subjects with H/Ms, 135 (14.0%) had a composite event (1 subject without H/M had ICD defibrillation).
Multivariate Cox Proportional Hazards Analysis
For the primary list of factors, the baseline model (without H/M) included age (P = 0.001), sex (male) (P = 0.014), race (black) (P = 0.037), and NYHA class (P = 0.049). H/M was a significant addition to the model (P < 0.001), with age (P = 0.003) and sex (P = 0.025) remaining significant. For the secondary list, only LVEF and log BNP were significant variables (Table 5). With the addition of H/M, the statistically significant predictors were log BNP (P < 0.001), H/M (P = 0.008), and LVEF (P = 0.004).
Multivariate Cox Proportional Hazards Model for Composite of All-Cause Mortality, Resuscitation, and ICD Defibrillation Using Secondary List of Factors
Multivariate Logistic Regression Analysis with ROC Curve Comparison for 2-Year Outcomes
Using the primary list of factors, the baseline model included 5 predictors: age (P = 0.001), sex (P = 0.008), race (black vs. other [P = 0.005]), lipid-lowering drugs at baseline (P = 0.027), and NYHA class (P = 0.019). H/M was a significant predictor (P < 0.001), and all the previous factors except NYHA class (P = 0.091) remained significant: age (P = 0.002), sex (P = 0.016), lipid-lowering drugs at baseline (P = 0.027), and race (black vs. other [P = 0.024]). The difference in ROC curve AUCs between the 2 models was significant (0.680 vs. 0.643, P = 0.018).
For the secondary list of factors (Table 6), the model included log BNP, LVEF, history of hypertension, and lipid-lowering medications. H/M was a significant additional predictor (P = 0.014). The AUC difference between the 2 models was not statistically significant.
Multivariate Logistic Regression Model for 2-Year Composite of All-Cause Mortality, Resuscitation, and ICD Defibrillation Using Secondary List of Factors
Net Reclassification Improvement Analysis
Net reclassification improvement analysis was applied to proportional hazards models for the composite endpoint (924 subjects with results for H/M, LVEF, and BNP) (Table 7). The 2-y event rate was 13% at the mean of the 2 covariates LVEF and BNP. Two-year event probability was defined as low if less than 8%, as intermediate if between 8% and 24% (approximately ±50% from the population average [50%–150%]), and as high if more than 24%. The addition of H/M significantly improved net reclassification (0.114, P = 0.002). The greatest benefit was in downward reclassification of risk among subjects who did not have events. Examples of subjects with improved risk classification after the addition of H/M are shown in Figure 1.
Net Reclassification Improvement Analysis
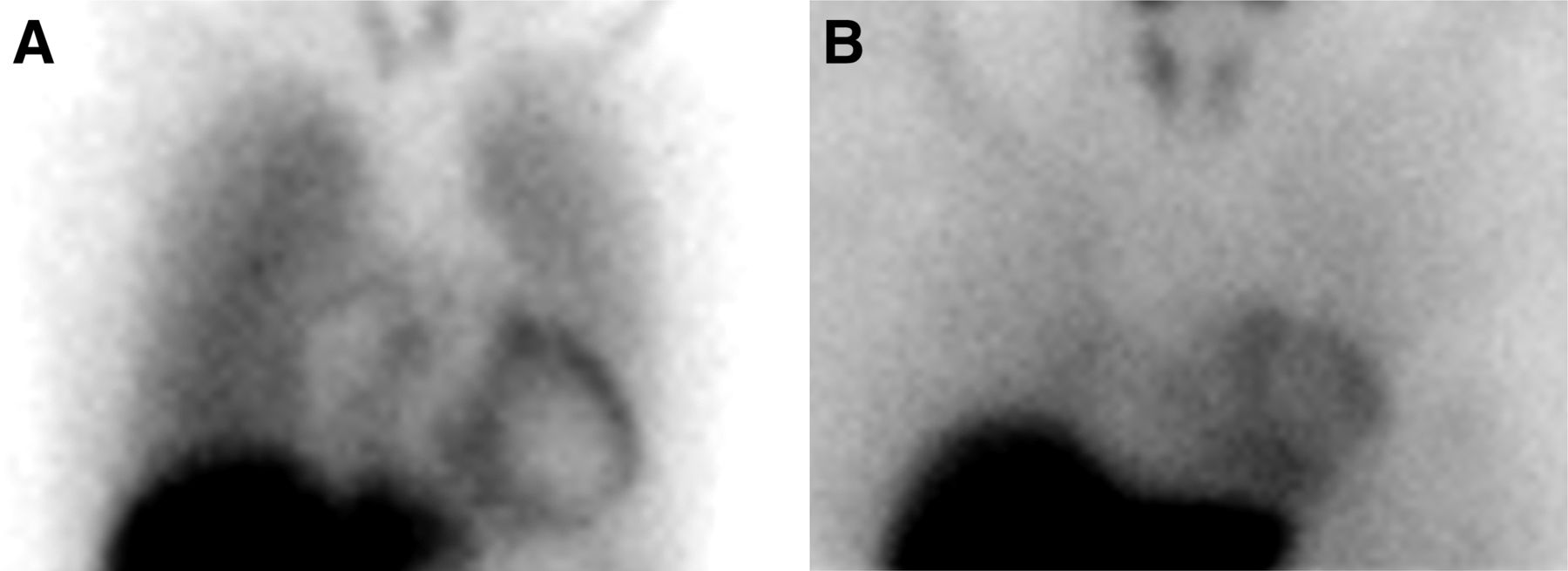
Lower mortality risk based on preserved myocardial innervation. Prediction of risk for composite endpoint of death or death-equivalent event is improved with addition of H/M. (A) Image from 37-y-old man with nonischemic cardiomyopathy, LVEF of 28%, and BNP of 378 ng/mL. Baseline 2-variable model predicted 21% (intermediate) 2-y risk. 123I-MIBG H/M was 1.69. Three-variable model (LVEF, BNP, and H/M) predicted 14% (intermediate) risk. Risk for all-cause mortality based on H/M alone (Fig. 4) was 6% (low). (B) Image from 51-y-old woman with ischemic HF, LVEF of 30%, and BNP of 166 ng/mL. Baseline 2-variable model estimated 13% (intermediate) 2-y risk for composite mortality endpoint. H/M was 1.80. Three-variable model (LVEF, BNP, and H/M) estimated 7% (low) risk. No subject in trial with H/M ≥ 1.80 experienced all-cause mortality.
Survival Analyses
Results for the 3 groups based on the mean H/M (1.44; n = 961) and SD (0.20) are shown in Figure 2. The 2-y mortality rate in the group with an H/M of at least 1.65 was significantly lower than that for the remainder of the HF population; similar results were obtained using an H/M of at least 1.60.

Kaplan–Meier all-cause mortality survival curves based on H/Ms of <1.25, 1.25–1.64, and ≥1.65. Mortality risk is significantly stratified by dividing population on the basis of mean H/M (1.44) ± SD (0.20). Two-year mortality was 3.1% for H/M ≥ 1.65 (n = 147), 11.8% for H/M = 1.25–1.64 (n = 660), and 19.1% for H/M < 1.25 (n = 154).
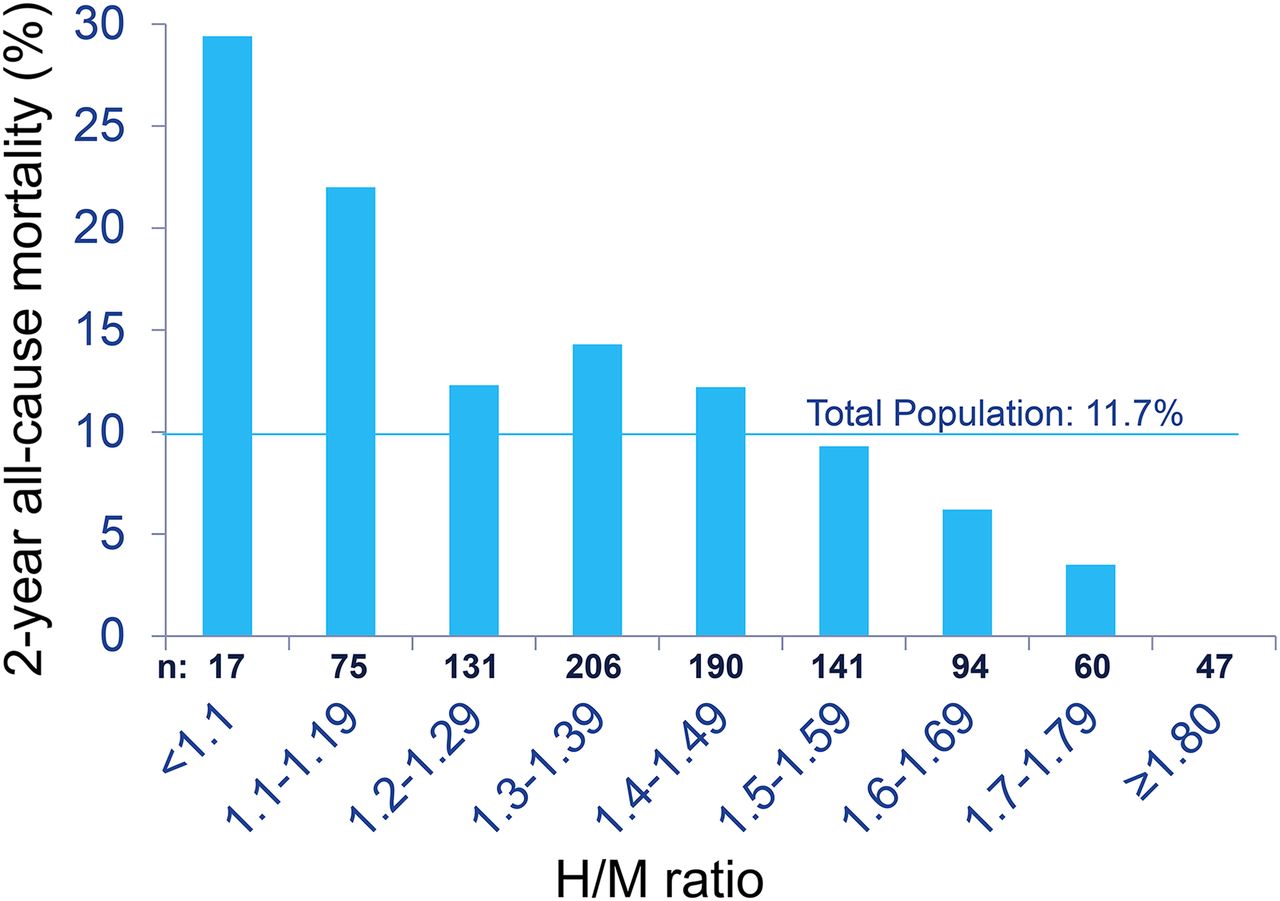
Two-year survival estimates for sequential 0.1 increments of H/M are shown in Figure 3. There was a progressive decrease in all-cause mortality rate as cardiac uptake increased from virtually none (H/M < 1.10) to normal (H/M ≥ 1.80).

Two-year all-cause mortality rate in relation to H/M intervals. Two-year all-cause mortality rates based on 0.1 increments of H/M show progressive decline from maximum of 29.4% for H/M < 1.10. There were no deaths among 47 subjects with H/M ≥ 1.80.
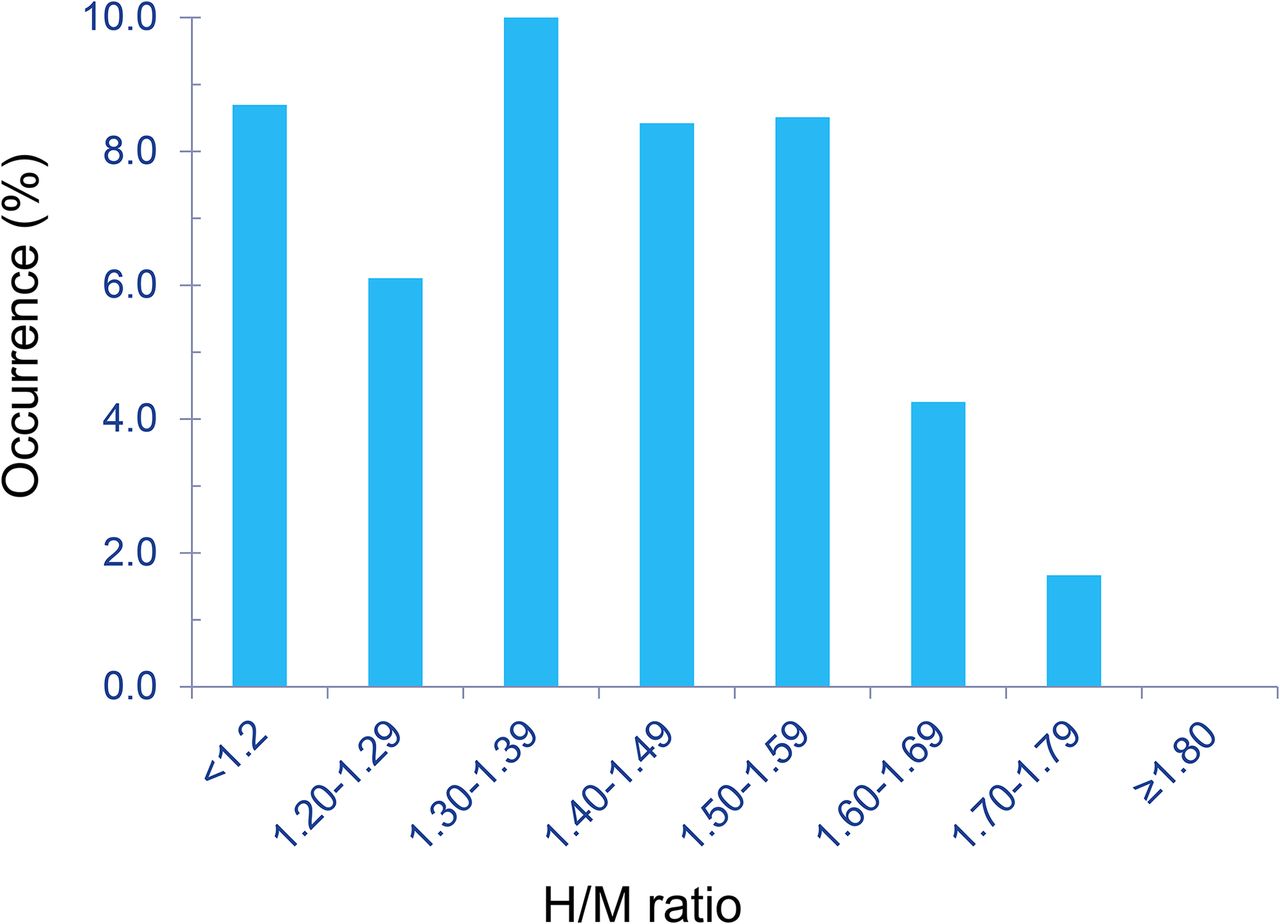
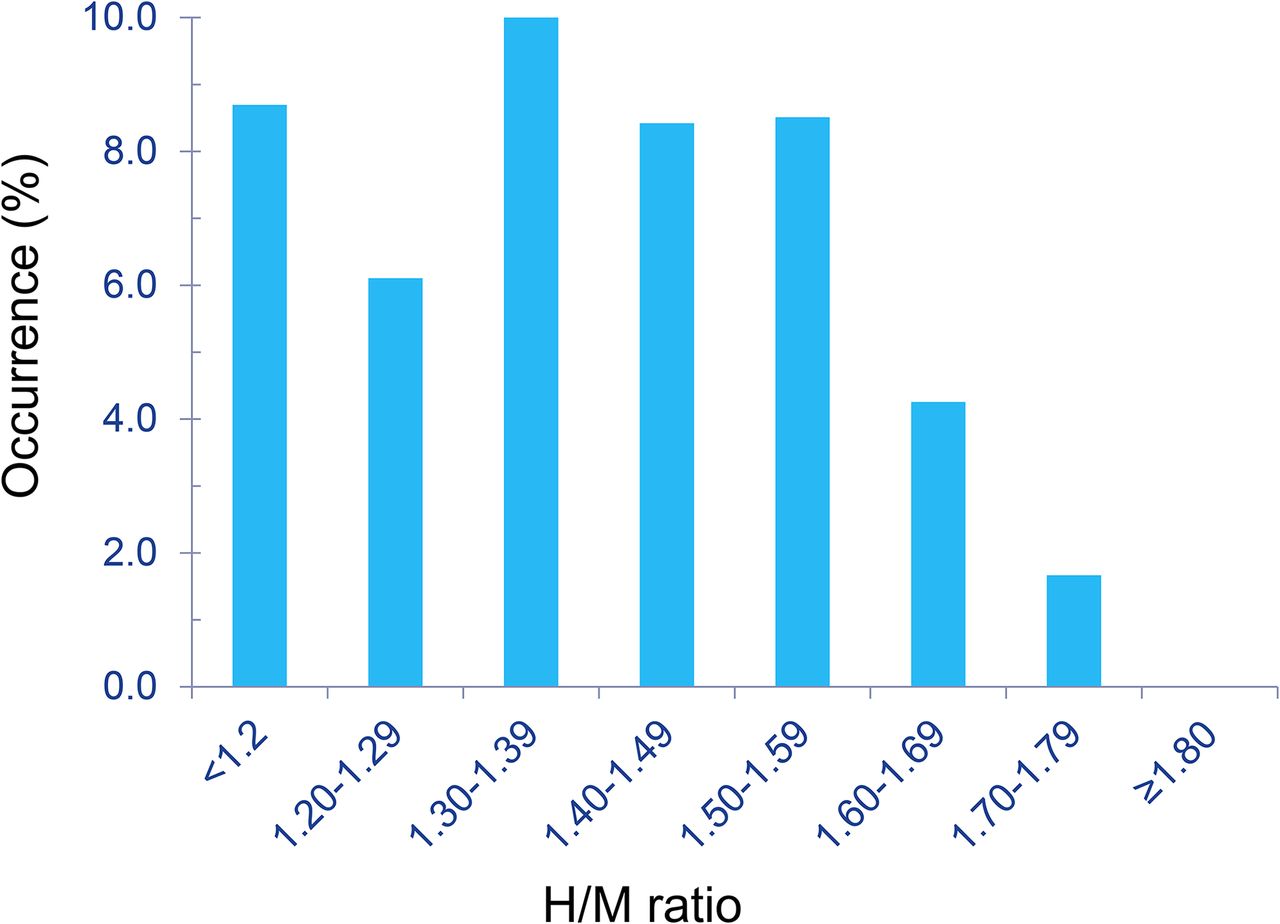
Fatal and Potentially Fatal Arrhythmic Events
The occurrence of fatal and potentially fatal arrhythmic events (sudden cardiac death, resuscitated cardiac arrest, and appropriate ICD defibrillation) in relation to H/Ms is shown in Figure 4. No subject with an H/M of at least 1.8 (n = 47; 5% of the study population) experienced an event. In contrast, arrhythmic events occurred in 6%–10% of subjects with an H/M of less than 1.6.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Occurrence of fatal and potentially fatal arrhythmic events (sudden death, resuscitated arrest, ICD defibrillation) (n = 70) in relation to H/M. Peak occurrence was in 1.30–1.39 range, with progressive decline for higher H/Ms. There were no fatal or potentially fatal arrhythmic events among subjects with H/M ≥ 1.80.
DISCUSSION
The first objective of the new analyses of ADMIRE-HFX was to determine whether planar H/M, a global measure of myocardial uptake, was a reliable indicator of mortality risk. The results confirmed the prognostic significance of H/M in relation to standard demographic and medical history variables, validating the extensive published literature from primarily uncontrolled experience (4,6,7,18).
The second objective was to determine the relative importance of cardiac sympathetic innervation as an indicator of mortality risk versus other clinical measurements often used for this purpose. 123I-MIBG imaging results remained a significant predictor of all-cause mortality in the multivariate analyses using the secondary list of factors, which included BNP and LVEF. Although BNP was a powerful predictor of mortality, there was only a weak negative correlation between this measurement and H/M (r = −0.25, P < 0.0001), indicating that the 2 parameters reflected different attributes of the heart. The status of the cardiac sympathetic nerves is an important indicator of risk for adverse consequences in HF patients, which may include the effects of more complex interactions with other body systems (e.g., kidneys, lungs, or immune system) that often fail in this population.
The third objective was to demonstrate that 123I-MIBG imaging had utility beyond that of currently used prognostic markers, thereby supporting the addition of this procedure to current clinical practice. Given the substantial number of multivariate analyses that demonstrated the significance of H/M as an independent predictor of death (both all-cause and all-cause equivalent [including defibrillation and resuscitated cardiac arrest]), it is evident that 123I-MIBG imaging provides additional prognostic capability when used in combination with other standard markers.
H/M improved the estimation of the probability that an HF patient would die in the near-term. Both proportional hazards and survival analyses consistently showed event risk decreasing with increasing H/M. In addition, when H/M was added to logistic regression models, the models were significantly improved, even though the shift in the ROC curves often did not result in differences in AUCs. Interestingly, increases in AUC were greater for 1-y than 2-y regression analyses, suggesting that the supplementary information provided by 123I-MIBG imaging at a single point in time has greater potential utility for early decision making, given that interval changes in therapy and disease progression can affect myocardial neuronal status and therefore the prognostic relevance of previous 123I-MIBG imaging results. The addition of H/M did provide a statistically significant net reclassification improvement for the 2-y composite endpoint.
For assessments that involve multivariate risk models for events such as death, time-to-event techniques such as Cox proportional hazards produce more meaningful results than probability-based methods such as logistic regression (16,19,20). Even among more severely ill patients (e.g., NYHA class III), the annual event rate of all-cause mortality is less than 20%, such that even a significant increase in AUC may not be associated with much improvement in sensitivity or selectivity. Furthermore, the area under the ROC curve is so indirectly related to the medical question being posed that a test of hypothesis based on it cannot be expected to have adequate statistical power to detect the effect being sought without studying a very large number of patients (16).
This study had a number of limitations. As a continuation of ADMIRE-HF, ADMIRE-HFX added further follow-up but not new experience with 123I-MIBG imaging. As before, only planar ADMIRE-HF 123I-MIBG data were used (9), thus leaving exploration of potential roles for quantitative SPECT to future investigators. The fact that new follow-up data were not collected on about 25% of potentially eligible subjects (15% of the total study population) could have introduced bias, although the clinical characteristics of that group were similar to those of the other subjects. The primary list of factors included only readily available clinical and demographic data and not laboratory and other measurements that can be prognostic in HF patients (12). As in the original analyses, changes in clinical condition, medication use, and other therapies that occurred during follow-up were not considered. The relatively low event rates reflect the lower-risk character of the ADMIRE-HF population, which limits application of the study results in many HF patients, such as those recently discharged from the hospital. These low event rates may also have contributed to the lack of significant AUC differences in some ROC curve comparisons. Use of the composite endpoint to identify all subjects who might have died without intervention is only an approximation given that most ICD activations, including defibrillations, are not lifesaving (21,22), but it was judged a better approach than selecting a subset of ICD activations either randomly or on the basis of other arrhythmic event risk markers. Finally, future research and clinical studies are still needed to demonstrate outcome improvements in patients with H/M data.
CONCLUSION
This study demonstrated that 123I-MIBG imaging provides independent prognostic information for determining the risk of death in HF patients that is additive to currently available risk stratification procedures. The specific insight provided by cardiac 123I-MIBG imaging could be particularly important for intermediate-risk NYHA class II–III HF patients for whom a significant change in estimated mortality risk could change the perceived need for an aggressive management strategy. Future development of nomograms or computer programs using the models developed in this study could facilitate use of 123I-MIBG imaging results in clinical patient assessment. Although the results of 123I-MIBG imaging will not be the single determining factor for a treatment decision (just as is the case with LVEF or BNP measurements), more complete information on the patient’s condition and future prognosis can only improve the clinician’s ability to select the most effective management approach.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. ADMIRE-HFX was sponsored by GE Healthcare. Dr. Narula has received research support from GE Healthcare in the form of a grant of equipment to his institution. Drs. Gerson and Thomas have received research support from GE Healthcare. Dr. Cerqueira is a consultant for GE Healthcare. Dr. Jacobson was an employee of GE Healthcare at the time the presented analyses were performed. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 11, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- Received for publication February 24, 2015.
- Accepted for publication May 5, 2015.