


Abstract
TS26
Introduction: 10 CFR 20.1101 states that Nuclear Regulatory Commisson (NRC) licensees implement a radiation protection program including information on radioactivity spills (1). NUREG-1556 Appendix N includes suggestions on spill kit inventory and procedures for handling major and minor spills (2). NUREG-1556 does not specify separate kits be created for major and minor spills, suggest the number of spill kits, or offer suggestions for quality control of the spill kits. Items suggested for a spill kit are disposable head coverings, shoe covers, and absorbent paper with plastic backing, as well as masking tape, trash bags with twist ties, “radioactive material (RM)” tape, marking pen, prestrung RM tags, wipes, “Emergency Procedures” instructions, clipboard with a Radioactive Spill Report Form, pencil, and appropriate survey instruments. This research aims to provide an analysis of current spill kit procedures in local healthcare systems.
Methods: 8 Nuclear Medicine Departments (NMDs) were asked to provide information on their spill kits. All are acute care hospitals with inpatient/outpatient services. PET Departments and Radiation Oncology departments that administer NM Therapy were excluded. 6 responded to the following questions: 1) Do you have a spill kit? 2) Does your department purchase a commercial spill kit or create your own? 3) Is the kit provided by your department or an outside department like Radiation Safety? 4)Do you have more than one type of spill kit (minor vs major)? 5)How often are the contents of the spill kit checked? 6)Who checks the contents of the spill kit? 7) In the last year, how many times has the kit been used? 8)What therapies are provided in your NMD?
NMDs were asked to provide images of their spill kit(s), displaying contents.
Results: 2/6 do not administer any therapeutics, 2/6 only administer therapeutic I-131 capsules, and 2/6 administer I-131 capsules and intravenous therapeutics.
6/6 sites have spill kits. Three NMDs had 1, two NMDs had 2 and one had 6. Of the three NMDs that had 1 kit, 1 was commercially purchased and 2 were department created. Of the NMDs that had 2 kits, one NMD created both and one NMD purchased 1 commercially and created the second. The NMD that had 6 kits created all the kits.
5 reported that the NMD supplies the kits. 1 NMD kit is supplied by Radiation Safety.
2 reported having kits that could address both major and minor spills. 4 reported kits that were to address minor spills.
2 check kits annually, 3 check as needed, quarterly, or monthly. 1 reported that the kit is not checked as this kit is stored in cardboard and the plastic bag seal cannot be broken due to the Joint Commission compliance. 3 used their kit once in the past year. 3/6 have not used their kits in the last year.
The kits are checked differently at each site: a physicist group contracted by the hospital, a technologist, charge technologist, radiation safety team, or department supervisor and chief technologist.
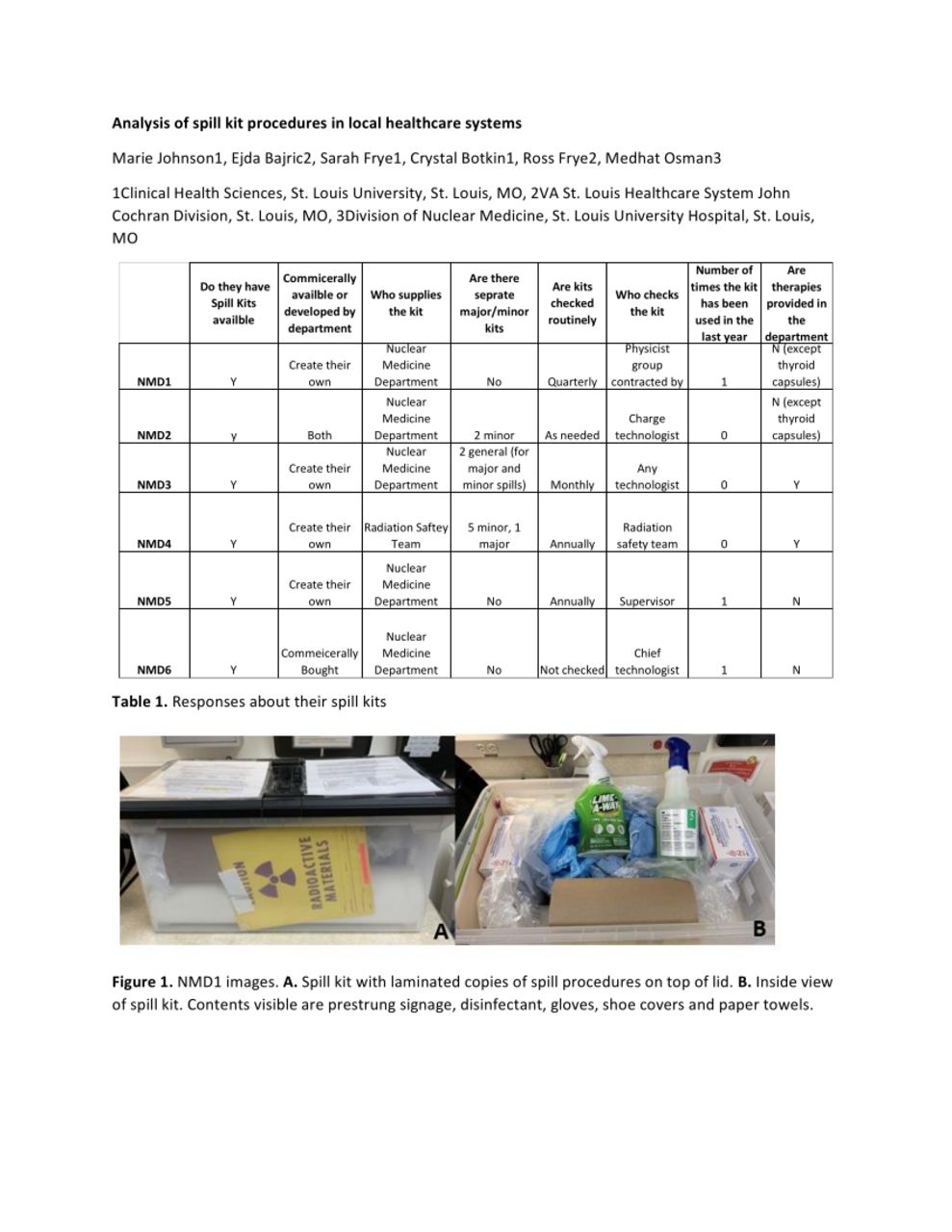
Table 1 shows responses to questions (NMDs1-6). Figs. 1-7 show photos from each NMD showing spill kits and their contents.
Conclusions: NMDs have high standards for safety concerning radioactivity handling to keep patients and workers safe. Accidents occur which can lead to RM contamination. In the event of a RM spill, training on response is key. The results of this research show a wide variety of approaches to equip NMDs with spill kits. The lack of overall standardization of kit policies and procedures between NMDs made the goal of this research difficult.
The higher activity of radiotherapies and their increasing use in hospitals pose a risk for major spills. These procedures also occur in other departments such as Radiation Oncology, which may not be familiar with spill kits. This research may demonstrate a need for more order surrounding kits and the training to use them for future technologists where radiotherapies may play more of a role in NMDs. Less ambiguity for spill kits could help ensure a safer work environment.




In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.