


Abstract
Many centers use techniques for localizing the sentinel lymph node (SLN) associated with a breast tumor. Protocols involve the use of an intraoperative probe and blue dye but may or may not include scintigraphy. Methods: Three methods of body-outline imaging were investigated to aid SLN localization. Body outlines were acquired using a handheld source; a transmission image was acquired from a 57Co-flood source; and, finally, a new method is described using a 153Gd-line source attenuation correction for body outline. Results: Method 1 images were of low quality, although 83% of SLNs were visualized. Body outline was unsatisfactory for surgical localization. Method 2 was unsatisfactory because of the lack of a lateral image. Method 3 enabled good presurgical visualization of the SLN (73%) and speeded surgical localization. Conclusion: The 153Gd-line source consistently gives optimal-quality body-outline images. This source is simple, quick, and clearly locates the SLN on multiple projections.
Sentinel lymph node (SLN) biopsy is becoming an important technique in surgical management of patients with breast carcinoma. SLN detection involves an injection of radiolabeled particles at and around the tumor site before surgery (1). A collimated γ-probe is used in the theater to localize the node. Blue dye may also be injected at the time of surgery for visual identification of the nodes. The identified nodes undergo biopsy and are examined microscopically for the presence of tumor cells. Nuclear medicine gamma camera imaging before breast surgery has a high rate of SLN detection; however, its real value is to provide accurate localization of nodes within the body to aid the surgeon. Such accuracy requires a body-outline view that clearly identifies the location of the nodes. The aim of this study was to provide a technique that can achieve this body-outline view on both anterior and lateral projections. In addition to aiding quick identification by probe during surgery, the gamma camera images may identify SLNs at unsuspected areas such as internal mammary nodes and may thus have a profound effect on the surgical approach.
MATERIALS AND METHODS
The patient was injected on the ward with 20–40 MBq of 99mTc-nanocolloid (Nanocoll; Nycomed Amersham Imaging, Princeton, NJ) into 4 sites around the tumor intradermally if palpable or at mammography if not. Three hours later, the patient was brought to the Nuclear Medicine Department for gamma camera imaging before surgery. In the operating room, the probe (Navigator GPS; RMD Instruments, LLC, Watertown, MA) and blue dye were used for detection of the SLN.
Three methods of determining body outline were used in this study. Manual body outline was used initially on 24 patients. Images were acquired on a single-head Basicam camera (Siemens Medical Systems, Inc., Hoffman Estates, IL) fitted with a general-purpose collimator. Two 300-s acquisitions were performed in the anterior and oblique projections of the affected breast. After the anterior acquisition, a body-outline image was collected by holding a small source (2 MBq of 99mTc in point source) and manually moving it around the affected breast and edge of the body while acquiring the image (Fig. 1).
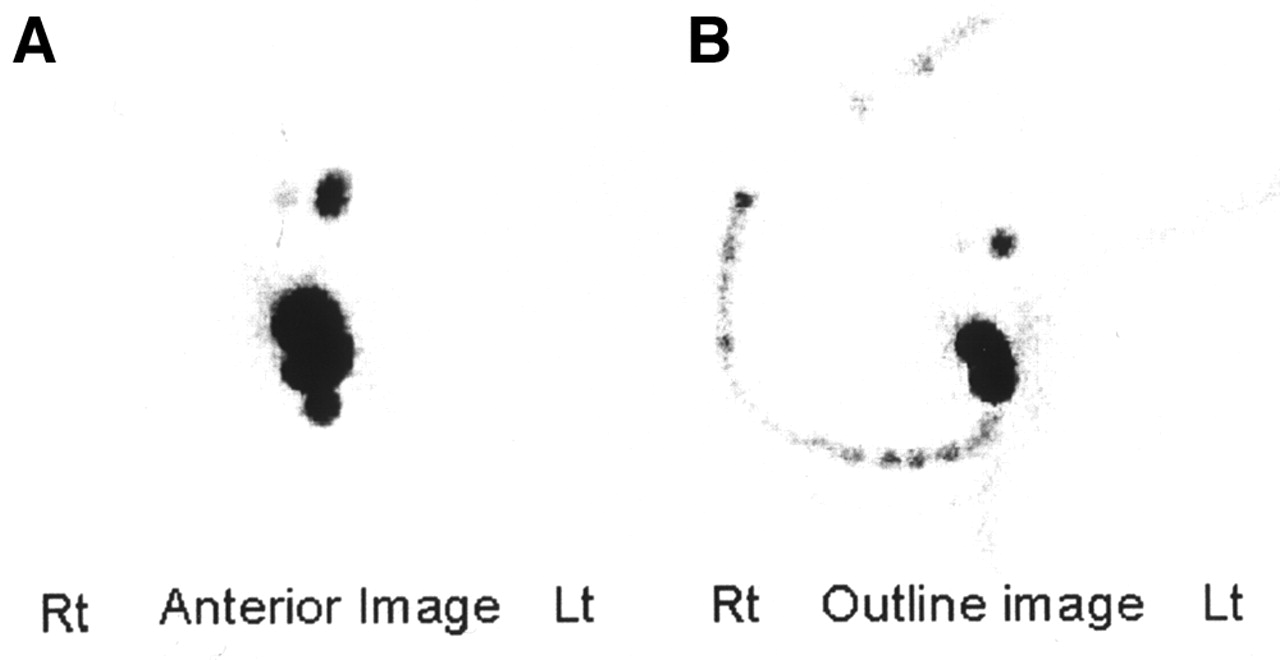
Example of SLN image (A) with body outline (B) on single-head camera. Lt = left; Rt = right.
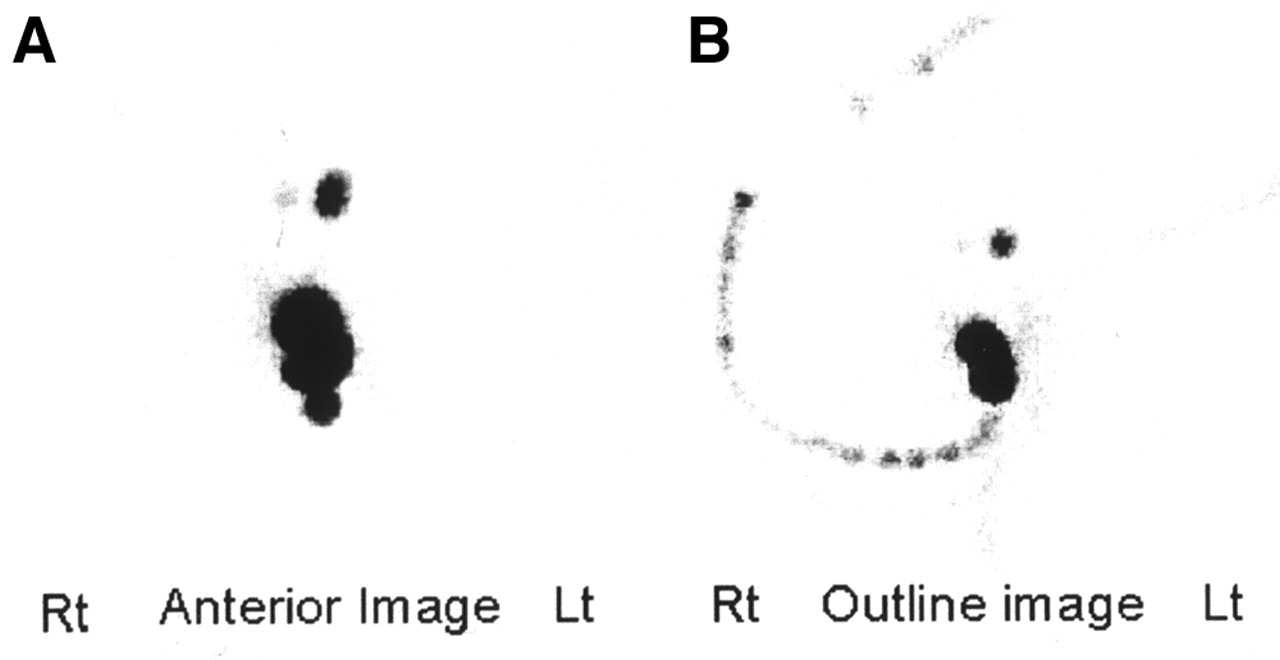
As an alternative, a 57Co-flood source was used for the body outline on 1 patient. The anterior and lateral images were acquired. The flood source was placed on the lower camera head of a dual-head camera, underneath the patient, and an anterior body-outline image was acquired on the upper head (Fig. 2). No lateral transmission view was obtained.

SLN emission image (A) with 57Co-flood source transmission (B). Lt = left; Rt = right.
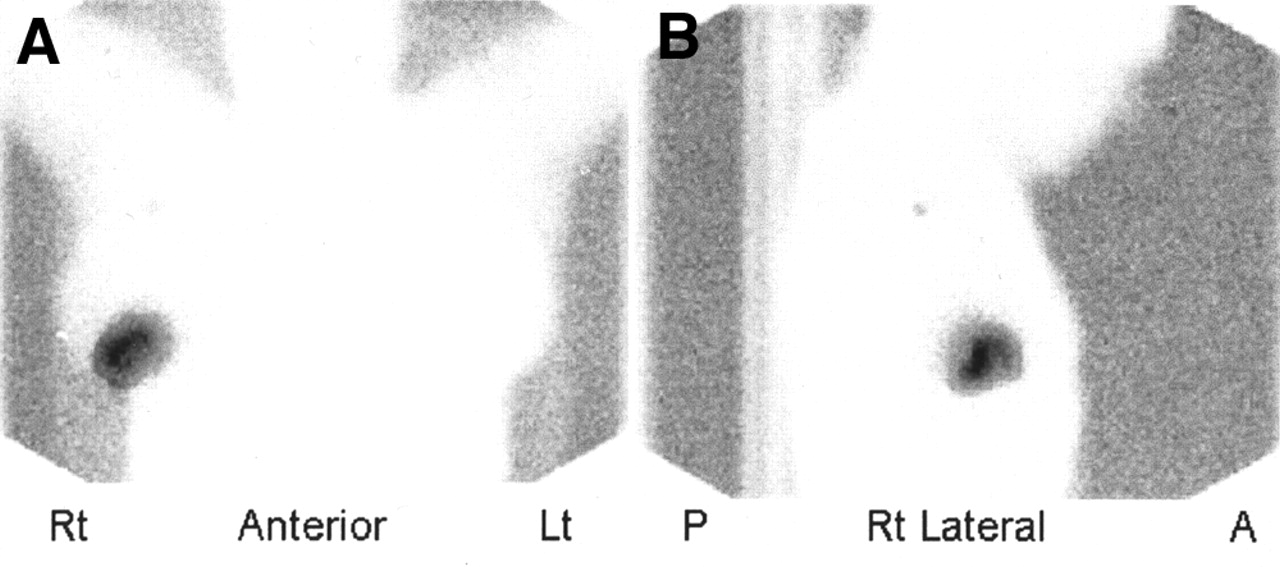
Finally, a 153Gd-line source transmission body outline was used on 25 patients as an alternative to a 57Co-flood source. The PRISM 2000 gamma camera (Marconi Medical Systems, Cleveland, OH) is fitted with a 153Gd-line source, which is used normally for attenuation correction for tomographic studies. Using this source transmission and emission images can be acquired simultaneously using a 99mTc window (140 keV) and a 153Gd window (159 keV). To perform a breast SLN study, head 1 (lower) was fitted with the attenuation correction collimator, which contains the line source. Head 2 (upper) was fitted with a high-resolution collimator. Emission images were acquired on head 2 for 300 s. At the same time, a 120-s transmission image was also acquired in both anterior and lateral projections.
Because the counts around the injection sites in the tumor area in the emission view were high, the image was rescaled to optimize the image for SLN detection. This scaled image was then added to the transmission image to achieve the final display images for both anterior and lateral projections (Fig. 3).

SLN images on dual-head camera with 153Gd-line source transmission. A = anterior; Lt = left; P = posterior; Rt = right.
RESULTS
Although the SLN can be identified using manual body outlines (method 1), the images and, particularly, the body-outline images were of low quality in all 24 studies. The same experienced technologist, assisted by the surgical registrar, performed all studies, and each still remained unsatisfactory. In this group, 83% of SLNs were identified by imaging, 100% by the probe and 83% by the blue-dye technique. The surgeons did not find the images helpful in localizing the SLNs and had to rely on intraoperative methods only.
A 57Co-flood source transmission outline (method 2) was adopted to enhance the image quality and SLN localization. Although the SLN was identified and the outline image quality was improved, surgeons were dissatisfied because only an anterior transmission view was possible.
With the use of a 153Gd-line source transmission outline (method 3), it was possible to obtain transmission images in all positions. Good-quality body-outline images were achieved for both anterior and lateral views with a superimposed SLN image for all patients.
In this group, 73% of SLNs were visualized by imaging, 96% by the probe and 68% by the blue dye. The surgeons asked for anterior and lateral views and found that localization of the SLN with these images was helpful for their approach and speed of localization. Their mean localization and SLN resection time was 14 min.
DISCUSSION
A body outline using a handheld point source has been used for many years. The method can achieve good, identifiable outlines; however, the quality of images even at the hand of a good operator is variable and depends on the speed of movement of the source, the patient, and the type of source. The radiation dose from a 2-MBq point source to the patient is negligible.
A 57Co body outline has been used for transmission for both SLN and lung studies in the past. Drawbacks include a high radiation dose to the patient and operator and limitation to a single view with a 57Co-source placed under the imaging bed. Most surgeons find oblique or lateral views more helpful than anterior views alone for lymph node identification.
A 153Gd-line source (or alternative point or line source) is available on most dual-head cameras for attenuation correction of tomographic images. The source produces body-outline transmission images that have helped us more clearly localize the SLN nodes before surgery than was previously possible. SLN and transmission images are acquired simultaneously, and images can be acquired in any angle desired. Our surgeons preferred lateral and anterior views; however, oblique views with a body outline can be acquired if requested.
A 153Gd-line source gives a clear, crisp body-outline image. This technique also gives a low radiation dose to the patient and none to the operator. The radiation dose to the patient for an SLN study is approximately 200–400 μSv. The extra radiation dose to the patient from the 153Gd-source is 3 μSv per view (2), 1% of the total patient dose from the SLN study. The dose from the 57Co-flood source is 70 μSv (3), a 25% increase in total patient study dose. The line source transmission technique described is simple and quick and can be performed on most dual-head cameras with attenuation correction capability. The technique can also be used to acquire images from any aspect. Body-outline images were consistently of good quality regardless of the experience of the technologist.
CONCLUSION
Presurgical localizing of the sentinel nodes has become more accurate and is being performed with greater confidence with the line source technique. The overall sensitivity of the study for visualization remains the same with each technique, but presentation is far superior. We recommend the line source technique as the method of choice to provide clear “user-friendly” images for the surgeons.
Acknowledgments
The authors are grateful to Fiona Hoar for her clinical input during this study.
Footnotes
Received Dec. 26, 2001; revision accepted May 21, 2002.
For correspondence or reprints contact: Elizabeth Clarke, HTEC, City Hospital NHS Trust, Dudley Rd., Birmingham B18 7QH, U.K.
E-mail: elizabeth.clarke{at}cityhospbham.wmids.nhs.uk
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transmission Imaging in Lymphoscintigraphy with a 153Gd Flood Source
- Optimal 57Co Flood Source Activity and Acquisition Time for Lymphoscintigraphy Localization Images
- Reducing Exposure from 57Co Sources During Breast Lymphoscintigraphy by Optimizing Energy Windows and Other Suggested Enhancements of Acquisition and the Display of Images
- Methods to Outline the Patient During Lymphoscintigraphy