


Abstract
145
Introduction: Advanced non-small cell lung cancer (NSCLC) can be treated with epidermal growth factor tyrosine kinase inhibitors (EGFR TKI). Clinical response to EGFR TKI is best in tumors with an activating EGFR mutation as compared to those with wild type (WT) EGFR1-2. Activating EGFR mutations can be subdivided in common (e.g. exon 19 deletions, EGFR com+ ) and uncommon mutations (e.g. exon 18 G719X point mutation, EGFR uncom+)3. Typically, all EGFR TKI have shown efficacy in EGFR com+. However, only afatinib, a second-generation irreversible EGFR TKI, has shown efficacy in EGFR uncom+4-5. Identifying patients who will benefit from EGFR TKI therapy is challenging as 1. representative tumor biopsies can be impossible to obtain due to tumor localization, 2. there may be intra- and interlesional differences between tumor lesions. These challenges may be overcome by performing positron emission tomography (PET) scans using radiolabeled afatinib ([18F]afatinib). For [18F]afatinib , we established the 2-tissue, irreversible (2T3K) model as the preferred pharmacokinetic model with Ki as parameter for quantification of tumor [18F]afatinib uptake6. Ki was able to detect differences in tumor [18F]afatinib uptake between WT and both EGFR com+ and uncom+ tumors6. In this study, we aimed to assess whether tumor [18F]afatinib uptake was predictive of tumor response in patients with WT, EGFR com+ and EGFR uncom+ tumors.
Methods: 8 advanced stage NSCLC patients were included in this study. Mutational status of each patient was assessed by tumor DNA sequencing prior to inclusion. A low-dose CT was performed for baseline measurement (BM) of each tumor. 20-minute, dynamic [15O]H2O (370MBq) PET scans were performed in all patients prior to [18F]afatinib scanning to assess tumor perfusion. Patients underwent a dynamic PET scan 60-90-minutes after intravenous injection of [18F]afatinib (370MBq) and started afatinib treatment (30mg or 40mg daily) within 24hrs post-scanning. Ki values were determined for each lesion using the 2T3K model using both plasma and image-derived input function (IDIF) input. Response measurement (RM) was performed after 6-8 weeks of treatment using contrast-enhanced thoracic CT. The longest axis in the axial plane was used to measure each tumor. The fraction of change (FC): (RM-BM)/BM was determined for each tumor.
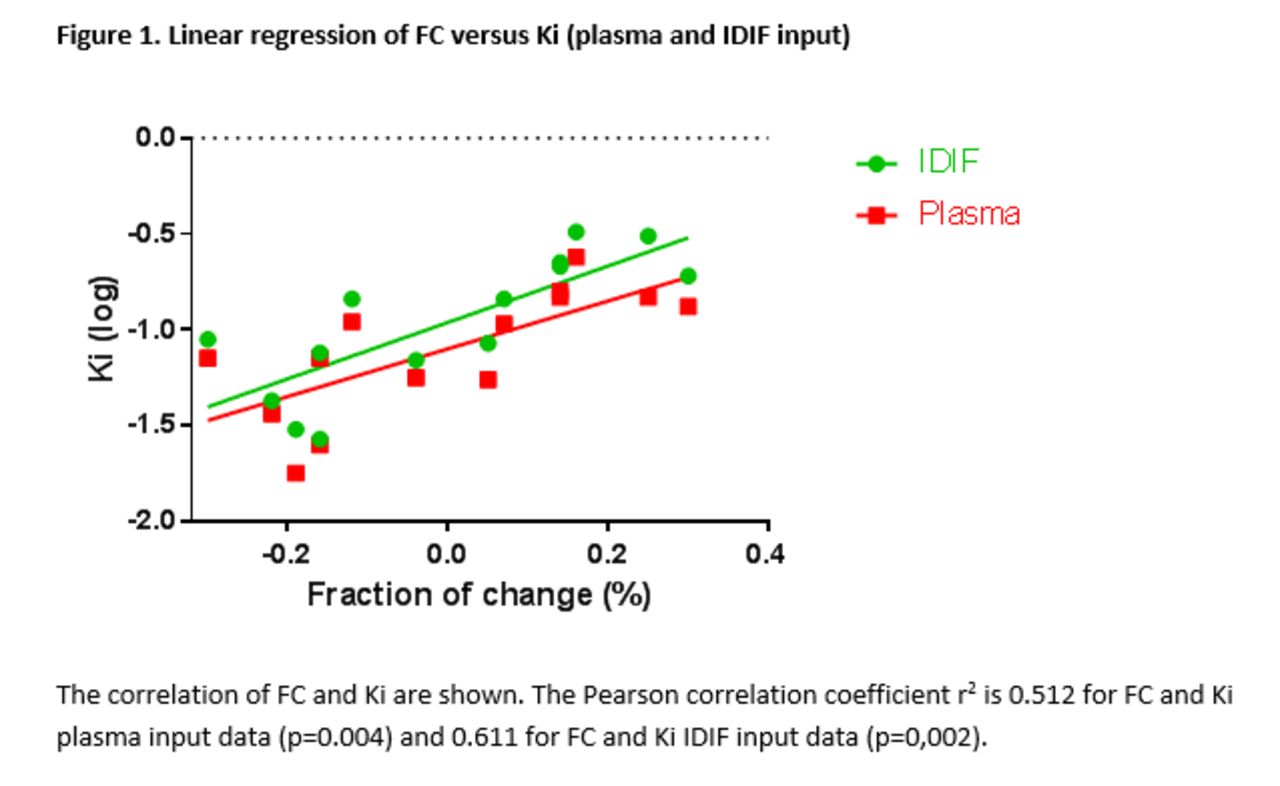
Results: All tumor lesions (N=19) in 8 patients were identified as target lesions at baseline. 1 patient (WT) died before response evaluation due to disease progression. 1 patient (EGFR com+) was lost to follow-up. A total of 14 lesions in 6 patients were included in this analysis (7 WT, 2 EGFR com+, 5 EGFR uncom+). FC was significantly correlated to Ki using both plasma and IDIF input (fig 1; r2=0.52 and 0.61; p= 0.004 and 0.002, resp), indicating that increased [18F]afatinib uptake was associated with tumor response to afatinib therapy. FC was also significantly different between mutational status (table 1), with increased tumor responses to afatinib in the EGFR uncom+ and EGFR com+ groups.
Conclusions: Tumor [18 F]afatinib uptake is strongly correlated with treatment response. EGFR uncom+ tumors resemble EGFR com+ tumors in both [18 F]afatinib uptake and FC on afatinib therapy, further confirming the role of afatinib in the treatment of patients harboring these mutations. Therefore, [18F]afatinib PET is a promising new means for selecting the right patient for treatment with afatinib.
Table 1. Post hoc univariate analysis of FC compared to EGFR mutational status (Tukey HSD test)

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.