


Visual Abstract
Abstract
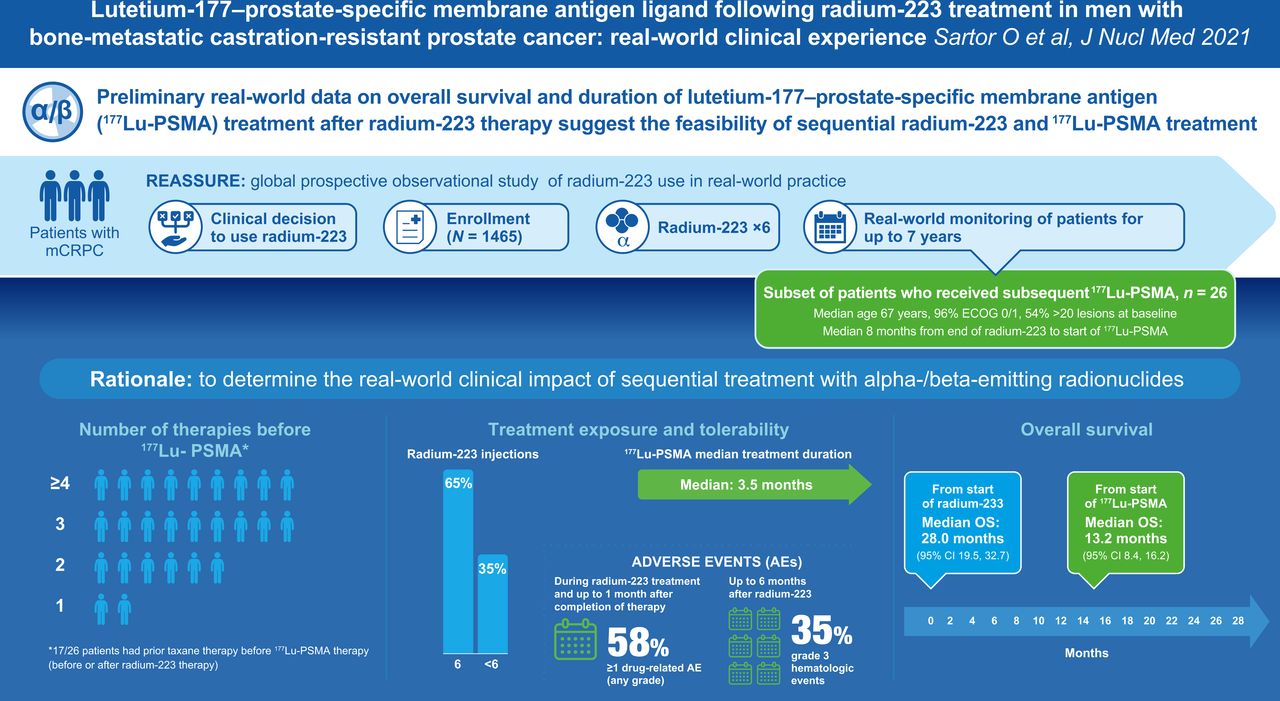
We analyzed real-world clinical outcomes of sequential α-/β-emitter therapy for metastatic castration-resistant prostate cancer (mCRPC). Methods: We assessed safety and overall survival in 26 patients who received 177Lu-prostate-specific membrane antigen ligand (177Lu-PSMA) after 223Ra in the ongoing noninterventional REASSURE study (223Ra α-Emitter Agent in Nonintervention Safety Study in mCRPC Population for Long-Term Evaluation; NCT02141438). Results: Patients received 223Ra for a median of 6 injections and subsequent 177Lu-PSMA for a median of 3.5 mo (≥ the fourth therapy in 69%). The median time between 223Ra and 177Lu-PSMA treatment was 8 mo (range, 1–31 mo). Grade 3 hematologic events occurred in 9 of 26 patients (during or after 177Lu-PSMA treatment in 5/9 patients; 8/9 patients had also received docetaxel). Median overall survival was 28.0 mo from the 223Ra start and 13.2 mo from the 177Lu-PSMA start. Conclusion: Although the small sample size precludes definitive conclusions, these preliminary data, especially the 177Lu-PSMA treatment duration, suggest that the use of 177Lu-PSMA after 223Ra is feasible in this real-world setting.
- 177Lu-prostate-specific membrane antigen
- metastatic castration-resistant prostate cancer
- 223Ra
- real-world evidence
- treatment sequence
The α-emitter 223Ra demonstrated significantly prolonged overall survival and a favorable safety profile versus placebo in men with metastatic castration-resistant prostate cancer (mCRPC) in the phase 3 ALSYMPCA trial (1). 177Lu-prostate-specific membrane antigen ligand (177Lu-PSMA) is an investigational β-emitting radioligand with accumulating evidence of clinical efficacy and acceptable toxicity in men with advanced-stage mCRPC (2–5).
Early experience in patients who have received both 223Ra and 177Lu-PSMA indicates tolerable safety and therapeutic response with this sequence (6–8). We sought to add to the evidence base on sequential α-/β-emitting therapy, using data from participants in an ongoing global, prospective, observational study of 223Ra who received subsequent 177Lu-PSMA.
MATERIALS AND METHODS
Patients with mCRPC involving bone and who were scheduled to receive 223Ra in clinical practice were included in REASSURE (223Ra α-Emitter Agent in Nonintervention Safety Study in mCRPC Population for Long-Term Evaluation; NCT02141438). Primary outcomes included short-term and long-term safety. Methods and results from a previous interim analysis have been reported (9). This paper is based on the second prespecified interim analysis (data cutoff, March 20, 2019).
Disease characteristics, adverse events after 223Ra treatment, and overall survival are described for patients who received the experimental drug 177Lu-PSMA in compassionate-use or investigational settings after 223Ra. Treatment-emergent serious adverse events and drug-related adverse events were recorded during 223Ra treatment or up to 30 d after the last 223Ra dose. Grade 3 or 4 hematologic adverse events were systematically collected up to 6 mo after 223Ra; neutropenic fever or hemorrhage were recorded in patients with subsequent chemotherapy up to 6 mo after the last dose of chemotherapy. Drug-related serious adverse events continued to be recorded until the end of follow-up (maximum, 7 y). Adverse events during and after 177Lu-PSMA therapy were not systematically recorded unless they met the above criteria.
The study conduct complied with the requirements of the European Medicines Agency, the U.S. Food and Drug Administration, applicable local laws and regulations, and International Conference on Harmonization good-clinical-practice guidance. Participants provided written informed consent, and ethics committee or institutional review board approvals were obtained according to local laws in participating countries.
RESULTS
Twenty-six patients in the United States, Germany, Austria, Italy, and Israel received 177Lu-PSMA after 223Ra. Their median age was 67 y, 96% (25/26) had an Eastern Cooperative Oncology Group performance status of 0 or 1, and 54% (13/24 with baseline scans) had more than 20 lesions at baseline (Table 1).
Baseline Disease Characteristics
Before starting 223Ra, 85% of patients (22/26) received at least 1 life-prolonging systemic anticancer therapy (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org), including androgen receptor–targeted therapy (enzalutamide and/or abiraterone acetate) in 65% (17/26) and docetaxel in 42% (11/26).
Before starting 177Lu-PSMA, 92% of patients (24/26) had received at least 2 life-prolonging therapies, 69% (18/26) had received at least 3 therapies, 8% (2/26) had received only 223Ra, 65% (17/26) had received prior docetaxel, 8% (2/26) had also received cabazitaxel between 223Ra and 177Lu-PSMA treatment, and 50% (13/26) had received no other life-prolonging treatment between 223Ra and 177Lu-PSMA (Fig. 1; Supplemental Fig. 1).
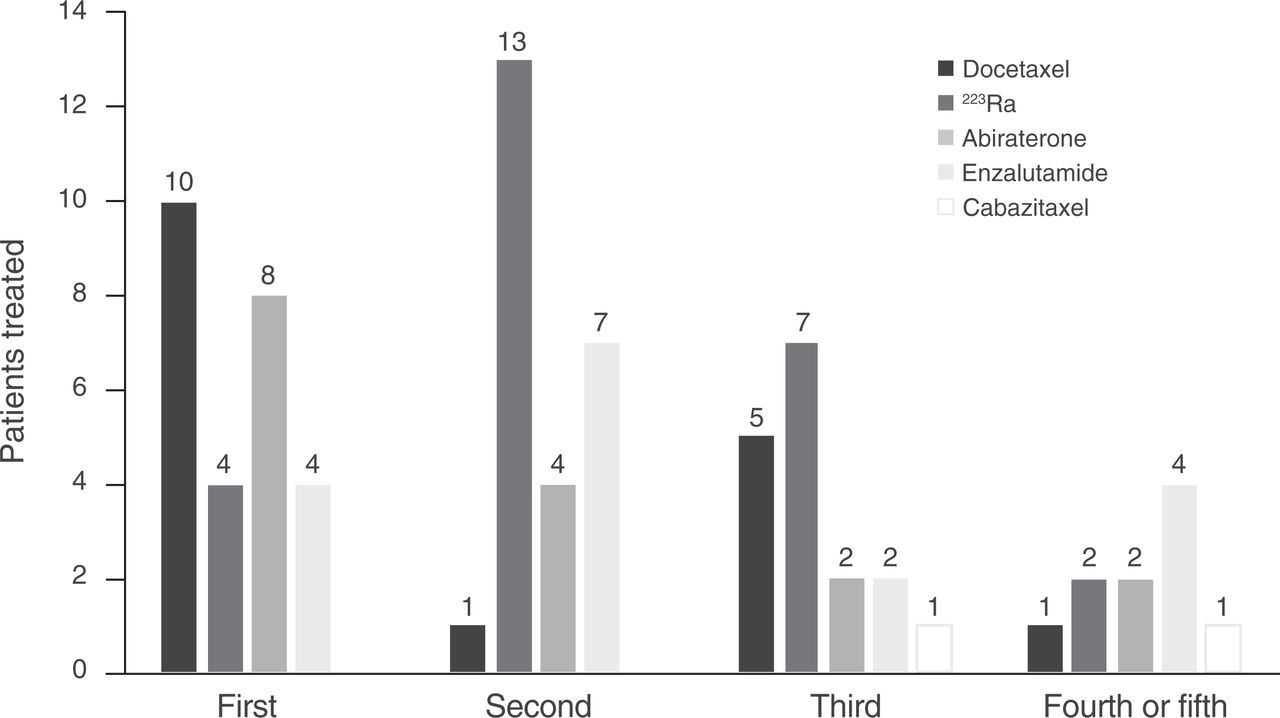
Anticancer therapies administered before 177Lu–PSMA. All patients received 223Ra.
The median number of 223Ra injections was 6 (range, 1–6); 17 of 26 patients (65%) received 6 injections. The median time from the end of 223Ra to the start of 177Lu-PSMA treatment was 8 mo (range, 1–31 mo; Fig. 2). The median duration of 177Lu-PSMA treatment was 3.5 mo (range, 0.5–21.2 mo; Fig. 2).
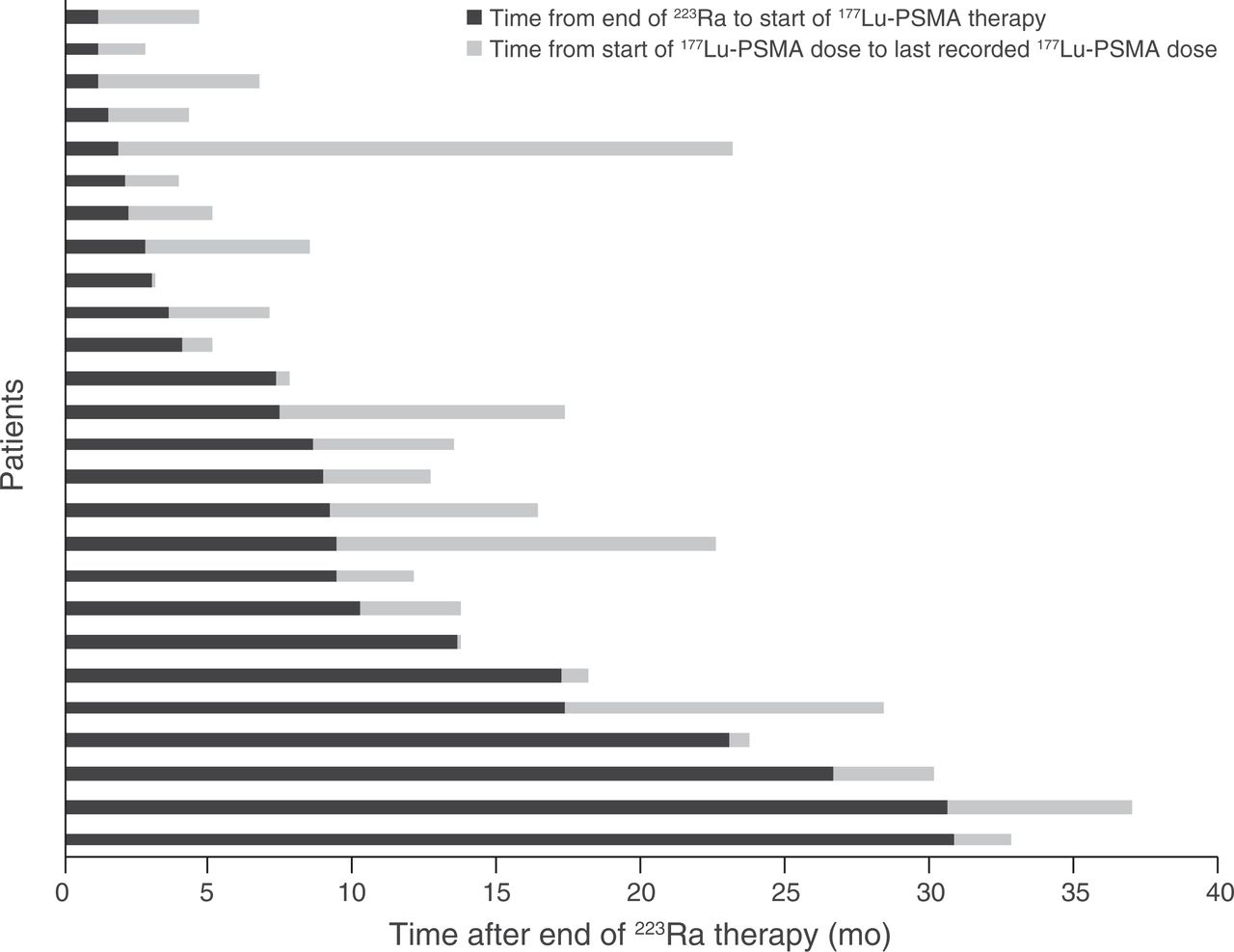
Time since end of 223Ra to start of 177Lu-PSMA ligand and duration of 177Lu-PSMA therapy.
Fifteen patients (58%) experienced treatment-emergent drug-related adverse events during 223Ra treatment (Table 2). Nine patients (35%) had grade 3 hematologic toxicities (Table 3); 8 of 9 patients had previously received docetaxel, before (n = 5) or after (n = 3) 223Ra therapy, and 2 of 9 patients had also received cabazitaxel after 223Ra. The hematologic toxicities developed during or after 177Lu-PSMA treatment in 5 patients (6 events). No grade 4 hematologic events were recorded.
Adverse Events During and After 223Ra Treatment
Grade 3 Hematologic Adverse Events After Start of 223Ra Therapy*
Median overall survival was 28.0 mo (95% CI, 19.5–32.7 mo) from the start of 223Ra therapy and 13.2 mo (95% CI, 8.4–16.2 mo) from the start of 177Lu-PSMA therapy.
DISCUSSION
Although 177Lu-PSMA is not yet approved for patients with mCRPC, patients are increasingly receiving this investigational treatment in clinical trials or compassionate-use programs. Most patients receive 177Lu-PSMA after multiple prior systemic anticancer therapies, including 223Ra in some cases, as recorded in the REASSURE study. This subgroup analysis of REASSURE, which reflects real-world clinical practice, adds to the evidence for the feasibility of sequential 223Ra and 177Lu-PSMA treatment, with a median overall survival of more than 1 y from the start of 177Lu-PSMA therapy. Only 3 patients had serious adverse events related to 223Ra, and the reported (albeit incompletely) incidence of grade 3 hematologic events was acceptable, mostly consisting of anemia, which may be partially explained by increasing disease burden. Furthermore, the treatment duration for 177Lu-PSMA (median, 3.5 mo) indicates that several patients were able to receive multiple cycles, even though most patients had received at least 3 prior life-prolonging therapies, including taxane chemotherapy.
The 13-mo median overall survival in our analysis is consistent with a retrospective multicenter study in which median overall survival from the start of 177Lu-PSMA therapy was around 11 mo in 85 patients with prior 223Ra (7) and 16.4 mo in patients with 6–20 bone lesions treated with 223Ra and 177Lu-PSMA (10). In another analysis, rates of grade 3 hematologic toxicity were low in patients with or without prior 223Ra therapy (anemia, 1/20 [5%] vs. 3/29 [10%]; thrombocytopenia, 1/20 [5%] vs. 2/29 [7%]) (6), a result that again supports our findings, although we did not systematically assess hematologic toxicity in all patients during 177Lu-PSMA treatment—a limitation of our study.
Additional limitations are the small sample size, reflecting the experimental status of 177Lu-PSMA, and the lack of a randomized control group. Because 177Lu-PSMA is still an investigational agent, treatment was likely undertaken in academic settings (e.g., university hospital cancer centers); it is therefore unknown whether the findings can be extrapolated to real-world community settings. The treatment duration and overall survival after 177Lu-PSMA initiation indicate that its use after 223Ra in heavily pretreated mCRPC patients is feasible, but interpretation is hindered by lack of a comparator arm, and possibly only the fittest patients were selected for 177Lu-PSMA treatment. Nevertheless, this interim analysis of an ongoing real-world study provides clinically meaningful evidence in patients with mCRPC who successfully received sequential α-/β-emitting treatments.
CONCLUSION
In this real-world population of heavily pretreated patients with mCRPC, a treatment sequence of targeted α-therapy with 223Ra followed by the β-emitter 177Lu-PSMA seemed feasible, based on the duration of 177Lu-PSMA therapy, although definitive conclusions cannot be drawn.
DISCLOSURE
Oliver Sartor reports grants or fees from Amgen, Bayer, Sanofi, AstraZeneca, Dendreon, Constellation Pharmaceuticals, Advanced Accelerator Applications, Endocyte, Pfizer, Bristol Myers Squibb, Bavarian Nordic, EMD Serono, Astellas Pharma, Progenics, Blue Earth Diagnostics, Merck, Invitae, Astellas, Endocyte, Myovant Sciences, Myriad Genetics, Novartis, Clarity Pharmaceuticals, Fusion Pharmaceuticals, Isotopen Technologien, Janssen, Noxopharm, Clovis Oncology, Taiho, Noria Therapeutics, Point Biopharma, TeneoBio, Telix Pharmaceuticals, and Theragnostics. Christian la Fougère serves as a consultant/adviser for Bayer and Sanofi-Aventis. Markus Essler reports research funding from Novartis; is a consultant/adviser for Bayer, Novartis, and Ipsen; and receives travel expenses from Ipsen and Sirtex. Samer Ezziddin reports travel expenses from Ipsen. Jörg Ellinger serves as a consultant for Bayer. John Sylvester reports employment at 21st Century Oncology; research funding from Prostatak (via 21st Century Oncology); stock in Augmenix; patents, royalties, or other intellectual properties with Myriad; and honoraria from Decipher and Theragenics. John Sylvester also serves as a consultant/adviser for, receives travel expenses from, and is on the speakers’ bureau for Theragenics. Avivit Peer serves as a consultant/adviser for Pfizer, BMS, Roche, Eisai, MSD, Janssen, Astellas, Novartis, Medison, AstraZeneca, and Bayer. Jeffrey Meltzer, Per Sandström, and Frank Verholen are employees of Bayer. Daniel Song reports research funding from Bayer, Advantagene, Bristol Myers Squibb, and BioProtect and serves as a consultant/adviser for BioProtect. This work was supported by Bayer Healthcare Pharmaceuticals Inc., Whippany, NJ, USA. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is it feasible to treat men with mCRPC with sequential α- and β-emitting therapies?
PERTINENT FINDINGS: Subgroup analysis of a global observational study of 223Ra therapy indicated a low rate of serious adverse events and hematologic toxicities in patients who also received 177Lu-PSMA, and many patients were able to receive multiple doses of 177Lu-PSMA (a marker of tolerability). This sequence provides overall survival of more than 2 y from the initiation of 223Ra and more than 1 y from the initiation of 177Lu-PMSA, even in heavily pretreated patients.
IMPLICATIONS FOR PATIENT CARE: Sequential use of α- and β-emitters appears to be feasible in selected patients, on the basis of the known safety profile of 223Ra and the duration of subsequent 177Lu-PSMA; this sequence warrants further investigation.
ACKNOWLEDGMENTS
David Murdoch (BSc Hons) and Sara Black (ISMPP CMPP™), of OPEN Health Communications, London, U.K., provided medical writing assistance, funded by Bayer HealthCare.
Footnotes
Published online July 24, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Immediate Open Access: Creative Commons Attribution 4.0 International License (CC BY) allows users to share and adapt with attribution, excluding materials credited to previous publications. License: https://creativecommons.org/licenses/by/4.0/. Details: http://jnm.snmjournals.org/site/misc/permission.xhtml.
REFERENCES
- Received for publication March 12, 2021.
- Revision received June 8, 2021.





{kind=link}
{kind=link}
{kind=link}