


Abstract
Pulmonary hypertension (PH) in adults with sickle cell disease (SCD) is associated with early mortality. Chronic thromboembolic PH (CTEPH) is an important complication and contributor to PH in SCD but is likely underappreciated. Guidelines recommend ventilation–perfusion (V/Q) scintigraphy as the imaging modality of choice to exclude CTEPH. Data on V/Q scanning are limited in SCD. Our objective was to compare the performance of V/Q scanning with that of CT pulmonary angiography (CTPA) and to report clinical outcomes associated with abnormal V/Q findings. Methods: Laboratory data, echocardiography, 6-min-walk testing, V/Q scanning, CTPA, and right heart catheterization (RHC) were prospectively obtained. High-probability and intermediate-probability V/Q findings were considered to be abnormal. Included for analysis were 142 SCD adults (aged 40.1 ± 13.7 y, 83 women, 87% hemoglobin SS) in a stable state enrolled consecutively between March 13, 2002, and June 8, 2017. Results: V/Q results were abnormal in 65 of 142 patients (45.8%). CTPA was positive for pulmonary embolism in 16 of 60 (26.7%). RHC confirmed PH (mean pulmonary artery pressure ≥ 25 mmHg) in 46 of 64 (71.9%), of whom 34 (73.9%) had abnormal V/Q findings. Among those without PH by RHC (n = 18), 2 of 18 patients had abnormal V/Q findings. Thirty-three patients had a complete dataset (V/Q scanning, CTPA, and RHC); 29 of 33 had abnormal RHC findings, of whom 26 had abnormal V/Q findings, compared with 11 who had abnormal CTPA findings. There was greater concordance between V/Q findings and RHC (κ-value = 0.53; P < 0.001) than between CTPA and RHC (κ-value = 0.13; P = 0.065). The sensitivity and specificity for V/Q scanning was 89.7% and 75.0%, respectively, whereas CTPA had sensitivity of 37.3% and specificity of 100%. Abnormal V/Q finding swere associated with hemodynamic severity (mean pulmonary artery pressure, 35.2 ± 9.6 vs. 26.9 ± 10.5 mm Hg, P = 0.002; transpulmonary gradient, 21.5 ± 9.7 vs. 12.16 ± 11 mmHg, P = 0.005; and pulmonary vascular resistance, 226.5 ± 135 vs. 140.7 ± 123.7 dynes⋅s⋅cm−5, P = 0.013) and exercise capacity (6-min-walk distance, 382.8 ± 122.3 vs. 442.3 ± 110.6 m, P < 0.010). Thirty-four deaths were observed over 15 y. All-cause mortality was higher in the abnormal-V/Q group (21 [61.8%]) than in the normal-V/Q group (13 [38.2%]) (log-rank test, P = 0.006; hazard ratio, 2.54). Conclusion: V/Q scanning is superior to CTPA in detecting thrombotic events in SCD. Abnormal V/Q findings are associated with PH, worse hemodynamics, lower functional capacity, and higher mortality. Despite high sensitivity in detecting CTEPH, V/Q scanning is underutilized. We recommend the use of V/Q scanning in the evaluation of dyspnea in adult SCD patients given the important implications toward management.
Pulmonary hypertension (PH), defined as a mean pulmonary artery pressure (mPAP) of at least 25 mm Hg as measured by right heart catheterization (RHC), affects 6.2%–10.4% of adults with sickle cell disease (SCD), for which it is a leading cause of morbidity and early mortality. An early and accurate diagnosis of the cause of PH guides management and prognosis, particularly in SCD, for which the etiology is often multifactorial, including chronic thromboembolism (1–6).
In a study using data on 1,804,000 SCD admissions from the National Hospital Discharge Survey, the prevalence of pulmonary embolism (PE) was approximately 3.5 times higher in hospitalized SCD adults than in African–American controls (7). A second inpatient study demonstrated a 50- to 100-fold increase in the annual incidence of PE in hospitalized SCD patients compared with non-SCD adults (8). Another cross-sectional study (9) has reported that 25% of SCD adult have a history of venous thromboembolism (VTE), with a median age of 30 y at the first event. These prevalence data are like those observed in family cohorts of patients with high-risk thrombophilia (10) and underscore the potent thrombophilic environment of SCD. Despite the heightened risk of VTE (11,12) accompanied by an increased recurrence rate (12,13), VTE is often overlooked as a major complication in adults with SCD.
Multiple factors contribute to the increased risk of VTE in SCD (14). Not only traditional factors, such as indwelling central venous catheters and frequent hospitalization, but also many SCD-specific factors, such as thrombophilic defects and loss of splenic function, increase the risk of VTE (15). Chronic thromboembolic PH (CTEPH), although not generally considered a major cause of PH, has been reported in patients with SCD (16–18) and in autopsy studies (19,20). Thus, CTEPH may be more common than realized in patients with SCD. Recently, successful surgical experience was published for a large case series of patients with hemoglobinopathies and CTEPH (21).
Identifying chronic thromboembolic pulmonary disease as a cause of PH has major clinical implications because these patients should be receiving indefinite anticoagulation therapy and could also potentially be offered a surgical cure. Ventilation–perfusion (V/Q) scintigraphy has been shown to have a higher sensitivity than CT pulmonary angiography (CTPA) in detecting CTEPH (22); however, to date we are not aware of any large studies that have characterized the value of V/Q in RHC-defined PH in SCD. In this study, we report a retrospective analysis of V/Q and CTPA findings for assessing PH as validated by RHC. We also report associated outcomes between the V/Q findings and prospectively collected data from adult SCD patients.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board at the National Institutes of Health. All subjects provided written informed consent to one or more studies (ClinicalTrials.gov identifiers NCT00011648, NCT00081523, NCT00023296, and NCT00352430). Consecutive subjects with SCD who had been enrolled between March 13, 2002, and June 8, 2017, were included in the study. Investigations included V/Q scanning, CTPA, echocardiography, 6-min-walk testing, and RHC; however, not all patients underwent the complete set of investigations.
Each patient underwent a V/Q scan using up to 1,110 MBq (30 mCi) of 133Xe gas and 148 MBq (4 mCi) of 99mTc-macroaggregated albumin. The V/Q results were analyzed according to the criteria of the Prospective Investigation of Pulmonary Embolism Diagnosis (23). For this analysis, the scores for normal, low, and very low probabilities were combined into the category of negative or normal V/Q. The scores for intermediate and high probabilities were categorized as positive or abnormal V/Q. Patients with normal kidney function and no contrast allergy underwent CTPA (n = 60), the results of which were considered suggestive of chronic thromboembolic pulmonary disease if they revealed the thrombus or webs, recanalization, perfusion abnormalities, stenosis, or strictures. Of the 142 patients,106 underwent a 6-min-walk test in accordance with the American Thoracic Society guidelines (24,25).
On the basis of clinical suspicion of PH (tricuspid regurgitant velocity [TRV] ≥ 2.8 m/s on echocardiography and a distance of <500 m on the 6-min-walk test or unexplained dyspnea or desaturation), 64 of the 142 SCD subjects underwent RHC. Subjects with abnormal V/Q findings were compared with those with normal V/Q findings. Laboratory values, 6-min-walk distance, echocardiography (TRV, right ventricular systolic pressure), RHC-derived hemodynamics, and overall survival were used as comparison parameters. Survival time from the date of the V/Q test was also determined, with life status being ascertained from clinical records, contact with subject or family members, the Social Security Death Index, and state death certificates. All causes of death were considered for survival analysis.
Statistical Analysis
Continuous variables are shown as mean ± SD or median with interquartile range for highly skewed data, and categoric variables are shown as frequencies and percentages. For continuous variables, the Wilcoxon rank-sum test and the Kruskal–Wallis test were used to compare 2 and 3 groups, respectively (26). For categoric variables, the χ2 test or the Fisher exact test was used, as appropriate. The Cohen κ-statistic and sensitivity and specificity tests were used to determine how well V/Q scanning and CTPA agreed with RHC. Survival curves were estimated using the Kaplan–Meier method and compared by the log-rank test.
All tests were 2-sided, and a P value of less than 0.05 was considered to indicate statistical significance. Analysis was performed using SPSS software, version 19 (IBM), or SAS statistical software, version 9.2 (SAS Institute Inc.).
RESULTS
One hundred forty-two subjects—58.4% women, 98% of African descent, and 87% with hemoglobin SS—were included (Tables 1 and 2). Their mean age was 40.1 ± 13.7 y. V/Q findings were abnormal in 65 patients (45.8%) (high probability and intermediate probability in 31 [21.8%] and 34 [23.9%], respectively) and normal in 77 patients (54.2%). As shown in Table 1, demographic characteristics, SCD genotype, and basic laboratory values were similar between the groups. However, subjects with abnormal V/Q findings demonstrated significantly abnormal cardiopulmonary markers of clinical severity (Table 2), including a higher TRV (3.2 ± 0.7 vs. 2.7 ± 0.5 m/s, P < 0.001), lower exercise capacity (6-min-walk distance, 382.8 ± 122.3 vs. 442.3 ± 110.6 m, P < 0.010), and increased likelihood of a history of PE (33 [73.3%] vs. 12 [26.7%]; P < 0.0001). The 2 V/Q groups did not significantly differ in history of deep-vein thrombosis or history of acute chest syndrome.
Baseline Clinical Characteristics by V/Q Results
Six-Minute Walk: Imaging and Clinical Characteristics According to V/Q Results
Sixty of the 142 subjects underwent CTPA; a pulmonary embolus was detected in 16 (26.7%). Patients with abnormal CTPA findings were more likely to have abnormal V/Q findings (14 [87.5%] abnormal vs. 2 [12.5%] normal V/Q; P = 0.034) (Table 3). In total, 64 patients underwent RHC, confirming PH (mPAP ≥ 25 mmHg) in 46, of whom 34 had abnormal and 12 had normal V/Q findings (P = 0.0001). Among those patients with no PH by RHC (n = 18), only 2 had abnormal V/Q findings whereas 16 had normal V/Q findings (P < 0.001) (Table 3).
Comparison of V/Q, CTPA, and RHC
Thirty-three patients had a complete dataset (V/Q, CTPA, and RHC) (Table 4). RHC confirmed PH in 29 of these patients, and of the 29, 26 had abnormal V/Q results and 11 had abnormal CTPA results. On the other hand, of the 4 patients with normal RHC results, 3 had normal V/Q results and one had abnormal V/Q results (P = 0.002). Using RHC as a benchmark for PH, results were more concordant between RHC and V/Q scanning than between RHC and CTPA. A higher level of agreement was observed between V/Q scanning and RHC (κ-value = 0.53; P < 0.001) than between CTPA and RHC (κ-value = 0.13; P = 0.065) (Table 5). The sensitivity and specificity for V/Q scanning were 89.7% and 75.0%, respectively, whereas CTPA had a lower sensitivity of 37.3% and a specificity of 100% (Table 6).
Comparison of V/Q, CTPA, and RHC
Measure of Agreement of V/Q and CTPA with RHC
Sensitivity and Specificity of V/Q and CTPA
Sixty-four subjects had both V/Q and RHC data. Subjects with abnormal V/Q results demonstrated significantly worse hemodynamic severity, such as a higher mPAP (35.2 ± 9.6 vs. 26.9 ± 10.5 mm Hg, P = 0.002), a higher transpulmonary gradient (21.5 ± 9.7 vs. 12.16 ± 11 mmHg, P = 0.005), and a higher pulmonary vascular resistance (226.5 ± 135 vs. 140.7 ± 123.7 dynes⋅s⋅cm−5, P = 0.013) (Table 7).
Hemodynamic Characteristics of Patients According to V/Q Results
Over a median follow-up of 6 y with a maximum of 15 y, 34 deaths occurred. The all-cause mortality was higher in the abnormal-V/Q group (21 [61.8%]) than in the normal-V/Q group (13 [38.2%]) (log-rank test, P = 0.006; hazard ratio, 2.54) (Fig. 1A). Among those who underwent RHC, the mortality was higher for those with PH (20/46 [43.5%]) than for those without PH (2/18 [11.1%]) (log-rank test, P = 0.003; hazard ratio, 7.5) (Fig. 1B).
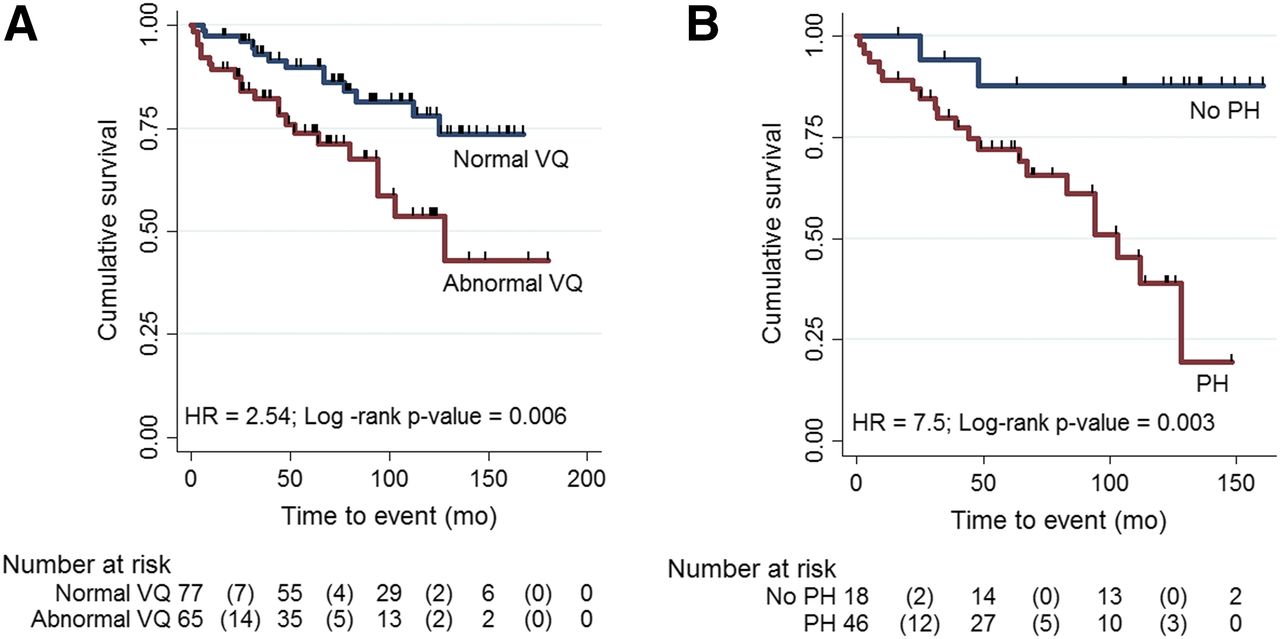
Kaplan–Meier estimates of survival for patients with SCD: overall survival curve by V/Q status (A) and overall survival by PH status (B). HR = hazard ratio.
DISCUSSION
Few studies have addressed V/Q scanning in SCD-related PH, and to our knowledge, no study to date has compared the performance of V/Q scanning with CTPA in diagnosing CTEPH. Here, we investigated the potential value of V/Q scanning in detecting CTEPH in 142 ambulatory adult SCD patients studied prospectively and consecutively.
V/Q scanning was of intermediate or high probability in 65 of 142 patients (45.8%). Thirty-three of the 142 patients had a full dataset (RHC, V/Q scanning, and CTPA). Using RHC as a benchmark for diagnosis of PH, results were more concordant between V/Q scanning and RHC. Comparing the 64 patients with both RHC and V/Q data, 34 of 46 (73.9%) with PH by RHC had abnormal V/Q findings (either intermediate- or high-probability V/Q results) whereas in patients with no PH by RHC (n = 18), only 2 (11.1%) had abnormal V/Q findings. Only one previous study has compared RHC-defined PH with V/Q scanning; high-probability V/Q results were reported in 3 of the 26 cases of RHC-confirmed PH (27). Mokhtar et al. performed echocardiography and V/Q scanning on 40 patients with SCD. Fifteen had an elevated TRV (>2.5 m/s), and 25 had a normal TRV. Ten had abnormal V/Q findings (either high- or intermediate-probability V/Q results), of whom 7 had elevated TRV (>2.5 m/s) but 3 had normal TRV (28). In another study, which performed V/Q scanning on 83 adult SCD patients and echocardiography on 77, intermediate- or high-probability V/Q results were found in 3 (12.0%) of the 25 patients with an elevated TRV (TRV > 2.5 m/s) and in 3 (6.0%) of the 52 patients with a TRV of less than 2.5 m/s (29). The differences in concordance rate between our study and the others could be due to differences in patient population or methodology. Our study defined PH using the gold standard of RHC, whereas the other studies used Doppler echocardiography. Echocardiography is reliable in the presence of severe PH but is not a sensitive marker in mild-to-moderate PH. This fact has been illustrated by a study of SCD patients with a PH prevalence of 6%; the positive predictive value for PH was only 25% among patients with a TRV of at least 2.5 m/s (30).
We showed that V/Q scanning bears a higher sensitivity, at 90%, than CTPA, at 37%—findings that are similar to those of previous studies reporting that V/Q effectively excludes CTEPH with a sensitivity of 90%–100% and a specificity of 94%–100%, compared with CTPA, which yields a sensitivity of 50% (22,31). The V/Q scan also has a higher sensitivity than CTPA in detecting distal forms of vascular disease (32), a phenomenon that is commonly observed in SCD (19,33).
Patients with abnormal V/Q results had lower functional capacity, worse physiologic indicators of precapillary PH severity, higher mPAP, higher transpulmonary gradient, and higher pulmonary vascular resistance—known hemodynamic markers reported to independently predict mortality in SCD patients with PH (34). PH in SCD is characterized by a relatively modest elevation of mPAP and pulmonary vascular resistance and a high cardiac output as seen in this study and others (27,35). Despite these seemingly favorable hemodynamic findings, the subjects with SCD and PH had a marked reduction in their functional capacity as measured by 6-min-walk distance and higher mortality, suggesting that any level of PH in SCD portends a poor prognosis. Over a median follow-up of 6 y with a maximum of 15 y, 34 deaths occurred. The all-cause-mortality hazard ratio was 2.5 for abnormal V/Q to normal V/Q, increasing to 7.5 for PH present to PH absent. The increased mortality risk among SCD PH in our study agrees with those previous RHC studies (30,36,37) that reported PH to be a risk factor for early mortality and others that showed untreated CTEPH to be associated with significant mortality (31,38).
Despite high sensitivity in detecting CTEPH. the V/Q scan is underutilized. CTPA is often used instead, in part because it is more readily available (39) and in part because providers have thought V/Q not to be relevant (40). For example, analysis of a PH registry revealed that 43% of patients diagnosed with PAH never received a V/Q scan during their evaluation (40), indicating the need for ongoing education of providers.
Our findings differ from a recent similarly sized comparison of V/Q and CTPA. Tivnan et al. (41) retrospectively analyzed 154 V/Q scans with 91 CTPAs performed for suspected acute PE in an SCD cohort. Only 4.1% were positive for PE using either modality—a lower thromboembolic prevalence than what has been published, although the authors reported 11% in subsequent testing done for clinical suspicion over the 17-y study period. Nonetheless, V/Q scanning performed comparably to CTPA in their study, making V/Q a reasonable first choice for acute PE diagnosis in SCD patients. We believe the difference in findings between these 2 studies reflects differences in methodology and populations, given the lower thromboembolic events in their cohort and perhaps the sicker population referred for clinical trials at the National Institutes of Health.
Several limitations must be noted regarding this study. First, our registry study was performed at a single center, with a retrospective analysis of prevalent and incident cases. Therefore, the prevalence of CTEPH could have been overestimated because of referral bias. An additional limitation is that CTPA and RHC were not performed on every subject; sensitivity and specificity were calculated from a subset of 33 subjects on whom all three tests (V/Q, CTPA, and RHC) were performed. Hence, selection bias cannot be excluded.
Nonetheless, using RHC as the benchmark, our data demonstrate that an abnormal V/Q finding is associated with PH and is superior to CTPA in detecting thromboembolic disease in adults with SCD. Additionally, abnormal V/Q results are associated with worse hemodynamics by RHC, poor functional capacity, and increased all-cause mortality.
Given the increased risk and increased recurrence of VTE in SCD (9,13) and the associated increased risk of early death, the identification of treatable causes or aggravating factors of PH in SCD is paramount (42). In adults with SCD, we showed that because of the high sensitivity of V/Q scanning, it is the imaging modality of choice for screening patients with suspected thromboembolism and CTEPH.
CONCLUSION
V/Q scanning is superior to CTPA in detecting thrombotic events in SCD. Abnormal V/Q findings are associated with PH, worse hemodynamics, lower functional capacity, and higher mortality. Despite high sensitivity in detecting CTEPH, V/Q scanning is underutilized. We recommend the use of V/Q scanning in the evaluation of dyspnea in adult SCD patients given the important implications toward management.
DISCLOSURE
Norris Igbineweka was supported by a Fulbright Scholarship. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
This research could not have been possible without all the subjects who participated in this study.
Footnotes
Published online Jun. 7, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 13, 2018.
- Accepted for publication May 23, 2018.





{kind=link}