


Abstract
Therapeutic options in advanced medullary thyroid carcinoma (MTC) have markedly improved since the introduction of tyrosine kinase inhibitors (TKIs). We aimed to assess the role of metabolic imaging using 18F-FDG PET/CT shortly before and 3 mo after initiation of TKI treatment. Methods: Eighteen patients with advanced and progressive MTC scheduled for vandetanib treatment underwent baseline 18F-FDG PET/CT before and 3 mo after TKI treatment initiation. During follow-up, CT scans were obtained every 3 mo and analyzed according to RECIST. The predictive value for estimating progression-free survival (PFS) and overall survival (OS) was examined by investigating the 18F-FDG SUVmean/max of the metabolically most active lesion, as well as by analyzing clinical parameters (tumor marker doubling times [calcitonin, carcinoembryonic antigen], prior therapies, rearranged-during-transfection mutational status, and disease type). Results: Within a median follow-up of 5.2 y, 9 patients experienced disease progression after a median interval of 2.1 y, whereas the remainder had ongoing disease control (5 with a partial response and 4 with stable disease). Eight of the 9 patients with progressive disease died from MTC after a median of 3.5 y after TKI initiation. A pretherapeutic SUVmean of more than 4.0 predicted a significantly shorter PFS (1.9 y vs. 5.2 y, P = 0.04). Furthermore, sustained high 18F-FDG uptake at 3 mo with a SUVmean of more than 2.8 tended to portend an unfavorable prognosis, with a PFS of 1.9 y (vs. 3.5 y, P = 0.3). Prolonged carcinoembryonic antigen doubling times were significantly correlated with longer PFS (r = 0.7) and OS (r = 0.76, P < 0.01). None of the other clinical parameters had prognostic significance. Conclusion: Pretherapeutic 18F-FDG PET/CT provides prognostic information in patients with advanced MTC scheduled for treatment with the TKI vandetanib. A low tumor metabolism with an SUVmean of less than 4.0 before treatment predicts a longer PFS.
- medullary thyroid carcinoma
- tyrosine kinase inhibitor
- vandetanib
- 2-deoxy-2-(18F)fluoro-d-glucose
- 18F-FDG
- positron emission tomography
Medullary thyroid carcinoma (MTC), which originates from parafollicular, calcitonin-secreting cells, accounts for approximately 5% of all thyroid cancers (1). Because MTC cells do not accumulate radioiodine (1), surgery represents the only curative strategy in early disease stages. In advanced disease stages, the only treatment option formerly available was cytotoxic chemotherapy, which is associated with low response rates (2,3). In the last decade, however, tyrosine kinase inhibitors (TKIs) have led to a paradigm shift: vandetanib and cabozantinib were approved for the treatment of advanced MTC after successful phase 3 trials (4–6). In one of these trials, for example, vandetanib demonstrated favorable antitumor activity, with disease control rates in 73% of patients and confirmed objective partial responses in 20% (4). However, there was no prolongation of overall survival (OS) (4), and adverse effects, including diarrhea, cutaneous reactions, hypertension, and even life-threatening cardiac arrhythmias, have been described and demand close patient monitoring (7). Given the more widespread use of TKI, reliable predictors of TKI responders before treatment initiation are intensely sought after (8).
The prognostic value of baseline 18F-FDG PET/CT assessment before TKI initiation has been shown in several types of cancers, such as renal cell carcinoma and gastrointestinal stromal tumor (9,10). Additionally, in iodine-refractory differentiated thyroid cancer scheduled for sunitinib treatment, early reduction of metabolic activity was associated with a morphologic response (11,12).
In this bicentric study, we aimed to elucidate the prognostic role of 18F-FDG PET/CT in MTC patients at the start of vandetanib treatment.
MATERIALS AND METHODS
Patient Population
All patients underwent imaging for clinical purposes and gave written informed consent to the diagnostic and therapeutic procedures. The requirement for additional approval was waived by the local institutional review boards because of the retrospective character of this study. All patients also gave written informed consent for the recording and anonymized analysis of their data. Parts of this cohort received vandetanib in a clinical trial (5).
Between April 2007 and July 2016, 18 patients (12 men and 6 women; median age, 48 y; range, 28–78 y) with advanced, progressive MTC were started on vandetanib (300 mg orally per day) at the University Hospital of Würzburg (n = 14) or the Hospital of Augsburg (n = 4), Germany. All patients had undergone previous therapies, including surgery (all patients), external-beam radiation therapy (4/18, 22.2%), chemotherapy (3/18, 16.7%), transarterial chemoembolization (2/18, 11.1%), radioiodine therapy (1/18, 5.6%; patient 16, initially misclassified as having differentiated thyroid cancer), or sorafenib (1/18, 5.6%). Detailed patient information is given in Table 1.
Detailed Patient Characteristics
Imaging-Based Response Assessment
Treatment response was assessed every 3 mo according to RECIST, version 1.1, based on CT findings (13), and the RECIST measurements were confirmed by an attending radiologist (14). During follow-up, the best response achieved by CT criteria (complete response, partial response, stable disease, or progressive disease) was evaluated. Progression-free survival (PFS) was defined according to RECIST by serial radiologic assessment starting from the time of TKI initiation (13). For OS, the interval between the start of treatment and the date of death was used. Data were censored on August 1, 2016.
Imaging
In 4 (22.2%) of 18 patients, dedicated PET was performed on a stand-alone lutetium oxyorthosilicate full-ring PET scanner (ECAT Exact 47; Siemens Medical Solutions). In the remaining patients, integrated PET/CT was performed. Twelve (85.7%) of 14 patients were scanned on a Biograph mCT PET/CT system (Siemens Medical Solutions), and 2 (14.3%) of 14 were scanned on a Gemini TF 16 PET/CT system (Philips). Before image acquisition, the patients fasted for at least 6 h, and their blood glucose levels were less than 160 mg/dL. 18F-FDG was injected intravenously. After 60 min, transmission data were acquired from the base of the skull to the proximal thighs using 68Ge rod sources (in the case of the stand-alone PET scanner) or spiral CT, either with intravenous contrast enhancement (13 patients [92.9%], dose modulation with a quality reference of 210 mAs, 120 kV, 512 × 512 matrix, and 5-mm slice thickness) or without intravenous contrast enhancement (1 patient [7.1%], 80 mAs, 120 kV, 512 × 512 matrix, and 5-mm slice thickness). Consecutively, the PET emission data were acquired. After decay and scatter correction, the PET data were reconstructed iteratively with attenuation correction, using the algorithm supplied by the scanner manufacturer.
After 3 mo, 18F-FDG PET/CT was performed on 16 (88.9%) of 18 patients, and CT was performed on 1 (5.6%) of 18 patients. In the remaining patient, imaging-based follow-up was not available because of early therapy termination due to adverse events.
Imaging Interpretation
For both the baseline and the follow-up scans, the axial PET image slice displaying the maximum uptake was selected, and a 3-dimensional volume of interest was drawn around the whole tumor area. A standardized 15-mm circular region of interest was then placed over the area with the peak activity. This region of interest was used to derive the respective SUVmean and SUVmax. The radiotracer concentration in the region of interest was decay-corrected and normalized to the injected dose per kilogram of patient body weight.
Tumor Markers
Serum levels of carcinoembryonic antigen (CEA, mg/L) and calcitonin (pg/mL) were measured before baseline using dedicated radioimmunoassays (14). Between 3 and 22 determinations (median, 6 determinations) were available per patient. Tumor marker doubling times were calculated using the American Thyroid Association calculator (3).
Clinical Parameters
The following clinical parameters were obtained: sex, age, metastatic sites at time of baseline PET, prior therapy, and tumoral rearranged-during-transfection (RET) mutation status (Table 1).
Analysis and Statistics
Statistical analyses were performed using PASW Statistics software (version 22.0; SPSS, Inc.). Quantitative values were expressed as mean ± SD and range as appropriate. The 2-tailed paired Student t test was used to compare differences between dependent groups, and the 2-tailed independent Student t test was used to compare differences between independent groups. Cox multiparametric regression analysis was applied to determine independent prognostic parameters. Cutoffs for the prediction of imaging-based PFS and OS were determined by receiver-operating-characteristic (ROC) analysis using the Youden Index for maximization of specificity and sensitivity (15,16). Pearson correlation was used to determine the association of tumor marker levels with other PET parameters and with PFS and OS. Kaplan–Meier analysis was performed using thresholds established by ROC analysis when the ROC analysis showed statistically significant results. Nonparametric log-rank tests were used to assess differences in the Kaplan–Meier curves. A P value of 0.05 or less was considered statistically significant. To adjust for multiple testing, Bonferroni adjustment was performed.
RESULTS
Baseline 18F-FDG PET results were positive in all patients. Of the 18 patients, 17 (94.4%) presented with lymph node metastases; 10 (55.6%), with lung metastases; 9 (50.0%), with liver lesions; 9 (50.0%), with bone lesions; 2 (11.1%), with soft-tissue metastases; and 1 (5.6%), with tumor infiltration of the pancreas.
One patient had hereditary medullary thyroid cancer (patient 6, with multiple endocrine neoplasia 2A syndrome). In the nonhereditary cases, somatic RET mutations were detected in 3 (37.5%) of 8 patients, in whom somatic RET mutational status was determined (Table 1).
The best morphologic response according to RECIST was classified as follows: stable disease in 8 (44.4%) of 18, partial response in 8 (44.4%) of 18, and complete response in 1 (5.6%) of 18. In the remaining patient, response could not be assessed because of early therapy termination. During follow-up (median, 5.2 y; range, 1.8–9.3 y), 9 patients (50%) experienced disease progression after a median of 2.1 y (range, 3 mo–9.1 y), whereas the remainder exhibited ongoing disease control. Eight of the progressive-disease patients died from their disease (median, 3.5 y; range, 11 mo–9.1 y) during follow-up.
Correlation of Serum Tumor Marker Doubling Times and Clinical Parameters with PFS and OS
The doubling times were highly variable among patients and ranged from 1.7 mo to 2.4 y for calcitonin and 1.4 mo to 5.1 y for CEA. The median calcitonin and CEA doubling times were 6.8 and 8.3 mo, respectively. Longer CEA doubling times were significantly related to a longer PFS and OS (r = 0.7 and 0.76, respectively; P < 0.01), whereas no correlation was observed for calcitonin.
The investigated clinical parameters (sex, age, metastatic sites at time of baseline PET, prior therapy, and RET mutation status) as given in Table 1 did not significantly correlate with PFS or OS.
Imaging-Based Findings of 18F-FDG Baseline and Follow-up PET
At baseline, 10 lymph node and 6 visceral metastases were identified as the metabolically most active lesions. Median SUVmean/max was 4.6 (range, 3.2–27.4) and 7.4 (range, 3.8–37.5), respectively.
As derived by ROC analysis, an SUVmean of more than 4.0 at baseline was correlated with a PFS significantly shorter (1.9 y) than that (5.2 y) for patients with lower metabolic activity (P = 0.04; area under the curve, 0.76), whereas no significant correlation was observed for SUVmax (P = 0.06). Both parameters failed to predict OS (SUVmean, P = 0.2; SUVmax, P = 0.3).
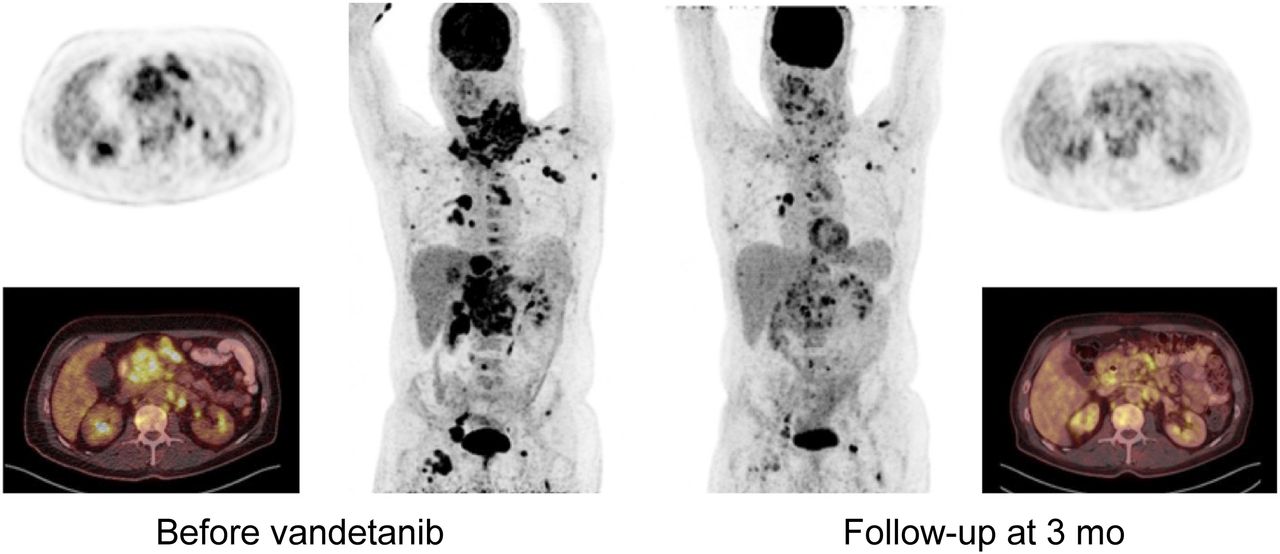
At follow-up, the above-mentioned lymph node and visceral metastases were reanalyzed. SUVmean dropped to a median of 3.0 (range, 2.1–6.6), with a median reduction of 26.9%. For SUVmax, a 25.6% reduction to a median of 3.8 (range, 2.2–16.3) was observed (Fig. 1; Table 2; Supplemental Table 1 [supplemental materials are available at http://jnm.snmjournals.org]).
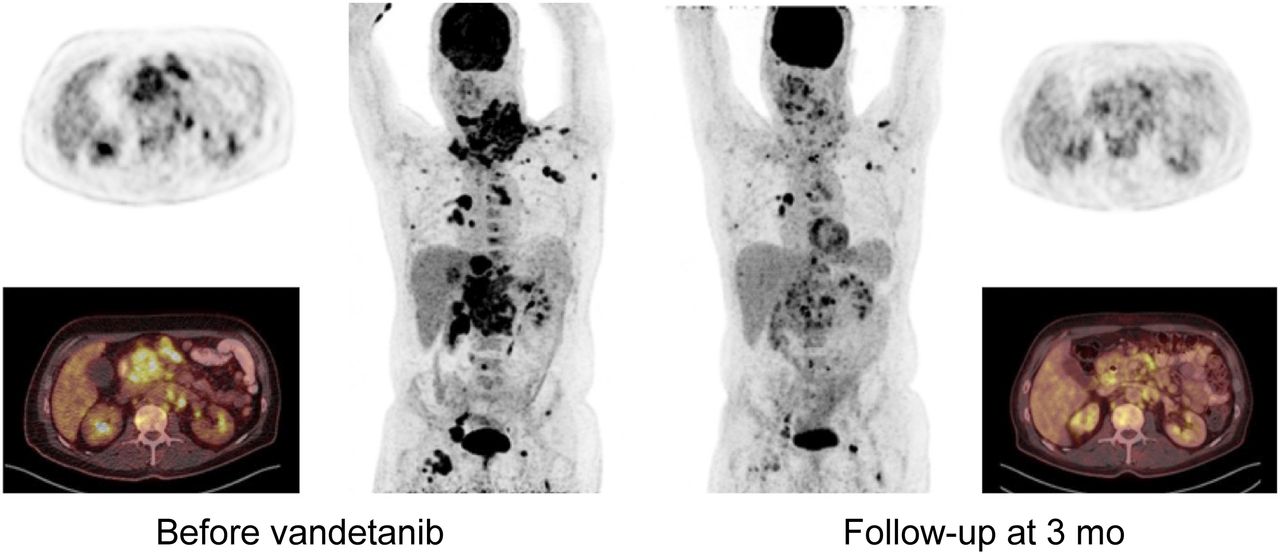
A 47-y-old man (patient 12) with extensive tumor load. Before TKI initiation, patient presented with highly aggressive disease on 18F-FDG PET, with SUVmean of 13.4 for hottest lesion (right clavicular lymph node). After 3 mo of vandetanib, partial response could be detected, with 54.5% decline in metabolic activity (SUVmean, 6.1). However, because of disease aggressiveness, patient died 11 mo after start of treatment.
SUVmean/max of Baseline and Follow-up 18F-FDG PET Scans and Changes Between Them
Whereas sustained high 18F-FDG uptake with an SUVmean of more than 2.8 tended to correlate with a shorter PFS of 1.9 y (vs. 3.5 y for SUVmean < 2.8; P = 0.3), the differences did not reach statistical significance. In parallel to baseline, no significant correlation was observed for SUVmax (P = 0.2), and both SUVmean and SUVmax failed to predict OS (P = 0.3, P = 0.2, respectively).
In addition, the extent of metabolic activity reduction between baseline and 3-mo follow-up PET was not predictive for either PFS (P = 0.2) or OS (P = 0.4).
The results of ROC analysis, including the area under the curve, sensitivity, specificity, and dedicated thresholds for each group (>cutoff vs. <cutoff), can be found in Table 3.
Results of ROC Analysis for SUVmean and SUVmax as Obtained by 18F-FDG PET
Kaplan–Meier Analysis
Kaplan–Meier analysis revealed a significant distinction between high- and low-risk patients for PFS using a threshold of 4 for SUVmean on baseline PET as derived by ROC analysis (P < 0.05); the respective Kaplan–Meier-plots are given in Figure 2.

Kaplan–Meier plots for probability of PFS using SUVmean of baseline 18F-FDG PET. High-risk group is indicated by solid line. Cutoff of 4 derived by ROC analysis was used (Table 3).
DISCUSSION
In this the largest, but still relatively small, patient cohort published to date, we report on the prognostic value of 18F-FDG in patients with advanced MTC at the start of TKI treatment. Interestingly, even though MTC is known to have a variable (and often even negative) 18F-FDG uptake in tumor lesions (17,18), all patients of our cohort had at least 1 hypermetabolic metastatic lesion.
A high 18F-FDG uptake at baseline had prognostic implications in terms of a significantly shorter PFS. An SUVmean of more than 4.0 for the metabolically most active lesion was associated with an almost 2.7-fold shorter PFS (1.9 vs. 5.2 y). The percentage of tumor metabolism reduction after 3 mo of TKI treatment did not offer prognostic value, and 18F-FDG failed to predict OS. This finding may be explained by the limited number of patients enrolled in this study. Additionally, vandetanib leads to reduced tumor proliferation, angiogenesis, and metastasis by inhibition of various tyrosine kinases but does not necessarily induce cell death (19,20).
In line with this consideration, Walter et al. have demonstrated the early transcriptional downregulation of key genes in glycolysis pathways such as STAT3 and Grb7/10 as soon as 3 d after vandetanib treatment initiation (20). However, this decline did not seem to be related to cell death, as no increase in apoptotic cells was detected in vitro (20). Since the main aim of vandetanib treatment is disease stabilization rather than cure, 18F-FDG PET/CT could be used as a noninvasive tool to identify high-risk patients with more aggressive disease who need to be monitored more closely than those with low 18F-FDG uptake at baseline.
Interestingly, clinical parameters such as age, sex, sites of metastases, prior therapy, and RET mutation status failed to predict response. The usefulness of analysis of serum marker doubling times as indicators of disease aggressiveness has been shown by several studies (21,22); however, in our study, only pretherapeutic CEA doubling times were strongly correlated with both PFS and OS, whereas no relation to calcitonin was observed, perhaps also because of the small sample size.
Like 18F-FDG in our cohort, serum marker follow-up of thyroid cancer patients undergoing TKI treatment has been reported to be complicated by the phenomenon of tumor marker fluctuations not necessarily denoting true tumor escape. In contrast, morphologically measurable disease progression could be confirmed only after a series of subsequent rises in serum markers (14,23,24). Given the earlier time point of response prediction obtainable, 18F-FDG PET might serve treating physicians outside the scenario of controlled studies as a suitable tool for therapy monitoring and patient-tailored decisions.
Additionally, in comparison with the cohort of an earlier phase 3 vandetanib trial by Wells et al. (5), our study population had more advanced and progressive disease, since our PFS was shorter than that in the prior study (30.5 mo). Moreover, fairly short median calcitonin and CEA doubling times of 6.8 and 8.3 mo, respectively, before initiation of treatment were found in our patient cohort. Hence, because more aggressive tumors were treated in our study than in the phase 3 trial (5), we could achieve a response rate of up to 50% (8 partial responses and 1 complete response). This rate indicates that vandetanib leads to tumor control and that the included patients most likely benefited from the treatment; however, this possibility cannot be verified in the absence of a control arm. In addition, even in a patient with a slightly increased SUVmean at baseline (patient 18, Supplemental Table 1), vandetanib initiation led to a complete disappearance of tumor burden. However, because of the underlying tumor biology, such an achieved response may persist only briefly.
This study had several limitations. Limiting its statistical power is the fact that only a small number of patients could be enrolled. Because the study was retrospective and bicentric, different PET scanners were used and the imaging protocols differed slightly between imaging centers. No additional partial-volume correction to reduce noise, including normalizing values to body surface area or to plasma glucose level, was performed. A future larger, multicentric prospective study is warranted to strengthen our preliminary results.
Additionally, in most the cases we did not determine the RET mutation status, which may represent another suitable predictor of PFS.
Last, potential intraindividual intertumoral heterogeneity regarding 18F-FDG–negative, 68Ga-DOTATATE–positive disease and its response to TKI treatment could not be assessed in this study but might be an interesting approach for further research (25).
CONCLUSION
18F-FDG PET/CT can serve as a prognostic tool in patients with advanced MTC scheduled to undergo vandetanib treatment. An elevated glucose consumption as assessed by baseline PET was related to a shorter PFS; therefore, these patients need to be monitored more closely than those with a low 18F-FDG uptake at baseline. Changes in 18F-FDG uptake after 3 mo in this small group of patients failed to predict PFS and OS.
DISCLOSURE
This project received funding from the European Union’s Framework Programme for Research and Innovation Horizon 2020 (2014–2020, no. 701983) under the Marie Skłodowska-Curie Grant Agreement. This project also received funding from the German Research Foundation (DFG) and the University of Wuerzburg in the funding program Open Access Publishing. Parts of this cohort received vandetanib while participating in the ZACTIMA trial. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all members of the laboratory and the PET teams of the nuclear medicine departments at Würzburg and Augsburg for their assistance. Additionally, we express our gratitude to Dr. Dirk O. Mügge (independent statistician, Göttingen, Germany) for his support in statistical analysis and to Johanna Vogt (Department of Nuclear Medicine, University Hospital Würzburg) for her assistance in data collection.
Footnotes
↵* Contributed equally to this work.
Published online Oct. 12, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 25, 2017.
- Accepted for publication October 4, 2017.





{kind=link}
{kind=link}