


Abstract
The G protein–coupled protein receptor C-X-C chemokine receptor 4 (CXCR4) is an attractive target for cancer diagnosis and treatment, as it is overexpressed in many solid and hematologic cancers. Binding of its ligand, C-X-C chemokine ligand 12 (CXCL12), results in receptor internalization and activation of several signal transduction pathways, such as phosphoinositide 3-kinase/protein kinase B, which are critical in cell proliferation, angiogenesis, development of metastasis, and survival. Also, the CXCR4–CXCL12 axis is involved in the interaction between hematopoietic stem cells (as well as hematologic and solid tumor cells) and their protective microenvironment. This interaction can be disrupted by CXCR4 antagonists. This concept is being used clinically to harvest hematopoietic stem or progenitor cells from bone marrow and to sensitize cancer cells to conventional chemotherapy and radiotherapy, and the potential to overcome tumor microenvironment–driven immunosuppression is being explored. This review focuses on new strategies for improvement of cancer treatment by targeting of the CXCR4–CXCL12 interaction. Because of its critical role in cancer, many peptidic and nonpeptidic ligands with different modes of antagonistic activity against the CXCR4–CXCL12 axis have been developed, with some of them reaching clinical trials. Molecular imaging with recently developed radiolabeled CXCR4 ligands could facilitate the selection of patients who might benefit from directed targeted therapy, including CXCR4-directed endoradiotherapy.
Chemokine receptors form a large family of proteins that mediate the chemotaxis of cells toward a gradient of chemokines. C-X-C chemokine receptor 4 (CXCR4) is a G protein–coupled chemokine receptor encoded on chromosome 2 (1). The receptor has a 7-transmembrane structure with 7 helical regions connected by 6 extramembrane loops (2). CXCR4 exerts its biologic effect by binding its ligand, C-X-C chemokine ligand 12 (CXCL12) (3,4), and activating the downstream signaling pathway; these actions lead to an alteration of gene expression, actin polymerization, cell skeleton rearrangement, and cell migration (Fig. 1) (5).

Some key signaling pathways thought to be involved in CXCR4–CXCL12 signaling. On agonistic binding to CXCR4, CXCL12 is internalized and finally subjected to lysosomal degradation. Activation of CXCR4 induces β-arrestin–mediated signaling. On the basis of their sequence similarity, Gα subunits are divided into 4 families (Gαs, Gαi, Gαq, and Gα12) that regulate G protein–coupled receptor signals via different routes.
CXCR4 expression plays a key role during embryonic development, as CXCR4 expression on progenitor cells allows migration from their place of origin to their destination, where they will differentiate into organs and tissues. The CXCR4 pathway is important in neoangiogenesis, immunity, and infections (6,7). In the late 1990s, CXCR4 expressed on cluster of differentiation 4–positive (CD4+) T cells was discovered to serve as a coentry receptor for HIV type 1 (8). The role of CXCR4 in numerous physiologic and pathologic circumstances, such as systemic lupus erythematosus, rheumatoid arthritis, and multiple sclerosis, has been elucidated (5). CXCR4 and CXCL12 play decisive roles in tumorigenesis, including the enhancement of cell proliferation, migration, and invasion; cancer cell–tumor microenvironment interactions; and angiogenesis (9–11).
TARGETING OF CXCR4–CXCL12 AXIS
Multiple agents with different modes of antagonistic activity against CXCR4–CXCL12 have been developed. In general, 4 major classes of CXCR4 antagonists and agonists can be distinguished: nonpeptide CXCR4 antagonists, such as the bicyclam derivative AMD3100; small-peptide CXCR4 antagonists, such as T140 and even smaller cyclic peptides; antibodies to CXCR4; and modified agonists and antagonists for CXCL12 (12).
The bicyclam derivative AMD3100 (plerixafor injection; Mozobil [Sanofi]), previously called JM3100, acts as a specific antagonist by blocking the binding pocket of CXCR4 (13,14). The first clinical trials with AMD3100 were designed for the treatment of HIV. Interestingly, an increased amount of white blood cells was observed in healthy volunteers in phase 1 clinical trials (15). This finding led to the discovery that AMD3100 mobilizes CD34+ human hematopoietic stem and progenitor cells from the bone marrow to peripheral blood (16). Finally, AMD3100 was approved by the U.S. Food and Drug Administration as a mobilizer of hematopoietic CD34+ cells from the bone marrow to the circulation (17,18). Orally available CXCR4 antagonists include AMD070 (19,20).
The earliest efforts to find CXCR4 antagonists focused mainly on peptide derivatives (21), including [Tyr5,12,Lys7]polyphemusin II, which was designated T22 (22); the highly potent CXCR4 antagonist T140, a 14-mer peptide with a disulfide bridge; and its smaller derivative, the cyclic pentapeptide FC131 (23,24). These efforts were followed by the development of antibodies specifically directed against CXCR4. Müller et al. described decreased metastasis in murine breast cancer models when a neutralizing antibody against CXCR4 was used (10). In addition to inhibition of metastasis, the discovery of a direct apoptotic effect of antibodies suggested that direct killing may be a mechanism for tumor growth inhibition.
BMS-936564/MDX-1338 is a fully human anti–human CXCR4 IgG4 monoclonal antibody that is currently in phase 1 trials for the treatment of relapsed or refractory acute myeloid leukemia, chronic lymphatic leukemia, non-Hodgkin lymphoma, and multiple myeloma (25). Neutralization of the interaction between CXCL12 and CXCR4 by use of the anti-CXCR4 antibody 12G5 significantly inhibited HIV infection and tumor cell migration in vitro (26). Recently, the development of a fully human single-domain antibodylike scaffold (termed an i-body) with activity against human CXCR4 was reported (27). Another CXCR4-targeting agent is CTCE-9908, a 17-amino-acid-sequence peptide analog of CXCL12 with inhibitory capacity and approved for clinical use in patients with osteosarcoma (28,29). Other agents or strategies for interfering with the CXCR4–CXCL12 axis include the anti-CXCL12 aptamer NOX-A12 (Noxxon Pharma AG), CCX2066, and RNA interference (30,31).
ROLE OF CXCR4–CXCL12 IN TUMOR CELL–MICROENVIRONMENT INTERACTIONS
Classic chemotherapeutic anticancer treatments induce cell death through DNA damage by taking advantage of the proliferative behavior of cancer cells. An alternative approach strikes at the critical driving forces of cancer cells. The importance of the microenvironment in the tumorigenic potential of epithelial cells is well established (32,33). The tumor microenvironment contains numerous cell types in addition to cancer cells—including stromal fibroblasts, endothelial cells, immune cells, connective tissue, and extracellular matrix—that support tumor structure, angiogenesis, and growth (33).
High levels of CXCL12 expressed by cancer cells and tumor-associated stromal cells directly stimulated the proliferation and invasiveness of breast cancer cells in autocrine and paracrine manners (9,33). Moreover, in mouse models of human breast cancer (9) and prostate cancer (33), high CXCL12 levels in the tumors attracted CXCR4-positive inflammatory, vascular, and stromal cells to the tumor mass, where they would eventually support tumor growth by secreting growth factors, cytokines, chemokines, and proangiogenic factors.
In the bone marrow, constitutive CXCL12 secretion by stromal cells is crucial for homing and sustaining CXCR4-expressing hematopoietic stem and progenitor cells in their niches (34,35). As shown in acute myeloid leukemia human xenotransplant mouse models, leukemic cells also localize in CXCL12-rich niches of bone marrow, where the protective microenvironment favors their growth and survival during cytotoxic treatment (36). As shown in murine models of chronic myelogenous leukemia (37), acute myeloid leukemia (38), and chronic lymphocytic leukemia (39), CXCR4 antagonists can disrupt tumor–stroma interactions and mobilize leukemic cells to the peripheral blood, making them more sensitive to conventional anticancer drugs (40–46).
CXCR4 antagonists have also been evaluated for inhibition of the cross talk between tumor and stromal cells and for mobilization of cancer cells from the protective microenvironment of solid tumors, making them more sensitive to conventional chemotherapy or radiotherapy and antiangiogenic therapy (3,34,47–49).
In a glioblastoma mouse model, combined vascular endothelial growth factor and CXCR4 antagonism targeting the glioblastoma stem cell population resulted in improved survival (50). Glioblastoma recurrence involves the persistence of a subpopulation of cells that have enhanced tumor-initiating capacity and that reside within the perivascular space, or niche. Antiangiogenic therapies may prevent the formation of new perivascular space but have not prevented recurrence in clinical trials (51,52), suggesting that they cannot abrogate tumor-initiating capacity. Anti–vascular endothelial growth factor and CXCR4 treatment indicates that targeting the structure and function of the perivascular space, or niche, has a superior antitumor effect. This concept was set to be evaluated in a clinical trial aiming to explore the efficacy of plerixafor and bevacizumab (ClinicalTrials.gov identifier: NCT01339039); however, the study was terminated because of a low accrual rate.
Another CXCR4 inhibitor, USL311, is currently under investigation alone and in combination with lomustine in a phase 1/2, dose escalation and dose expansion study in subjects with advanced solid tumors (phase 1) and subjects with relapsing or recurrent glioblastoma (phase 2). The study is designed to explore the safety, tolerability, pharmacokinetics, and preliminary efficacy of USL311 alone and in combination with lomustine (ClinicalTrials.gov identifier: NCT02765165).
ROLE OF CXCR4–CXCL12 IN IMMUNITY IN TUMOR MICROENVIRONMENT
Immune checkpoints consisting of inhibitory pathways are a part of the immune system that is crucial for maintaining self-tolerance and modulating the duration and amplitude of physiologic immune responses in peripheral tissues to minimize collateral tissue damage. Tumors coopt certain immune checkpoint pathways as a major mechanism of immune resistance, particularly against T cells that are specific for tumor antigens (53). Cytotoxic T-lymphocyte–associated antigen 4 antibodies, programmed cell death protein 1 (PD-1), and programmed cell death ligand 1 antibodies promote the killing of cancer cells by cytotoxic T cells and have been successful in subsets of patients with melanoma, non–small cell lung cancer, urothelial bladder cancer, renal cell cancer, and head and neck cancer (54–60). Nevertheless, it has become apparent that even if these T-cell checkpoint antagonists overcome some of the immunosuppressive effects of the tumor microenvironment, other, more fundamental inhibitory reactions in the tumor microenvironment may explain why most patients—especially those with microsatellite stable colorectal cancer, ovarian cancer, prostate cancer, and pancreatic ductal adenocarcinoma—rarely exhibit objective responses to these therapies (34,55,61).
Effective immunotherapy requires that these T cells physically contact cancer cells. Cancer-associated fibroblasts were shown to exclude T cells by mediating the extracellular matrix (60,62). Live-cell imaging of lung tumor tissue slices from patients revealed active T-cell motility in regions of loose fibronectin and collagen, whereas T cells migrated poorly in dense matrix areas surrounding tumor nests (63). When collagenase was added to reduce matrix rigidity or when the chemokine CCL5 was experimentally produced by tumor cells, increased T-cell movement out of the stromal regions and into contact with cancer cells was observed. Also, cancer-associated fibroblasts excluded T cells by biosynthesis of CXCL12. The administration of AMD3100 in an autochthonous pancreatic ductal adenocarcinoma mouse model induced rapid T-cell accumulation among cancer cells and acted synergistically with anti–programmed cell death ligand 1 to diminish cancer cells (64).
The stromal cell–derived factor 1α/CXCR4 pathway mediated stroma polarization toward an immunosuppressive microenvironment and contributed to systemic disease progression after antiangiogenic treatment in a hepatocellular mouse model (65). AMD3100 prevented this immunosuppressive microenvironment after sorafenib treatment, inhibited tumor growth, reduced lung metastasis, and improved survival (66). In treatment-naive tumors in mice with orthotopic hepatocellular cancer, CXCR4 inhibition in the tumor microenvironment was demonstrated to facilitate anti–PD-1 immunotherapy. In an in vivo lung metastatic mouse model of human melanoma, the CXCR4 antagonist T22 sensitized melanoma cells for immunity–augmenting low-dose cyclophosphamide and anticytotoxic T-lymphocyte–associated antigen 4 monoclonal antibody therapy, resulting in 70% and 50% fewer lung metastases, respectively, than cyclophosphamide and anticytotoxic T-lymphocyte–associated antigen 4 monoclonal antibody therapy alone (67).
The concept of inhibition of the CXCL12–CXCR4 axis in combination with treatment with an immune checkpoint inhibitor is currently being tested in a phase 1a/b trial evaluating the safety and tolerability of CXCR4 peptide antagonist LY2510924 in combination with a monoclonal antibody targeting programmed cell death ligand 1 durvalumab in patients with advanced refractory solid tumors.
CXCR4 RECEPTOR IMAGING AND CXCR4-DIRECTED RADIONUCLIDE THERAPY
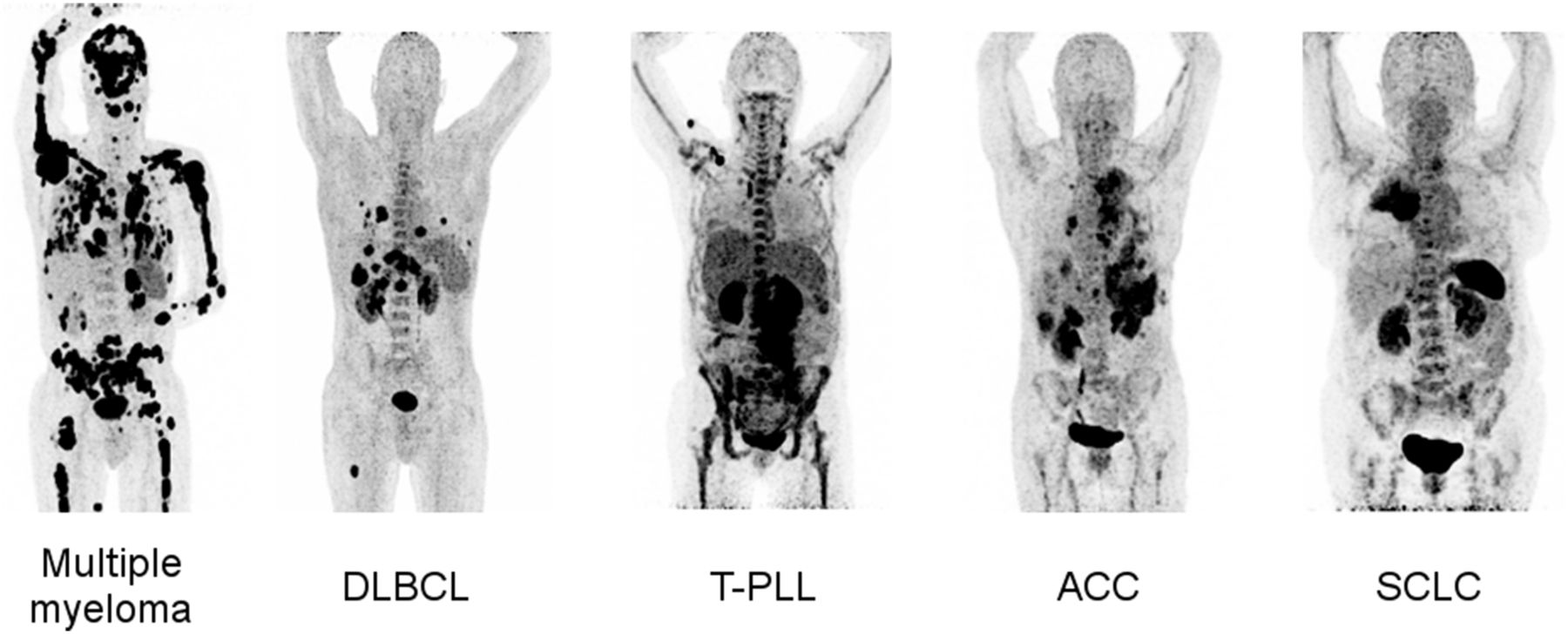
Given the paramount importance of the CXCL12–CXCR4 axis in a multitude of tumors, the chemokine receptor represents a promising target for imaging and therapy. Recently, noninvasive molecular imaging of CXCR4 expression was made feasible by the introduction of radiolabeled receptor ligands that allow for whole-body SPECT or PET (68–73). For example, labeling of AMD3100 with 99mTc resulted in specific binding in organs with high levels of CXCR4 expression and CXCR4-positive tumors (71). The development of 68Ga-pentixafor can be regarded as a milestone for clinical PET imaging of CXCR4 expression (69,70). Proof-of-concept visualization with this tracer could be demonstrated not only for several different hematologic and other neoplasms—including leukemia, lymphoma, multiple myeloma, adrenocortical carcinoma, and small cell lung cancer (Fig. 2) (72–77)—but also for other solid tumors and disease conditions—such as splenosis, stroke, atherosclerosis, and myocardial infarction (78–84).
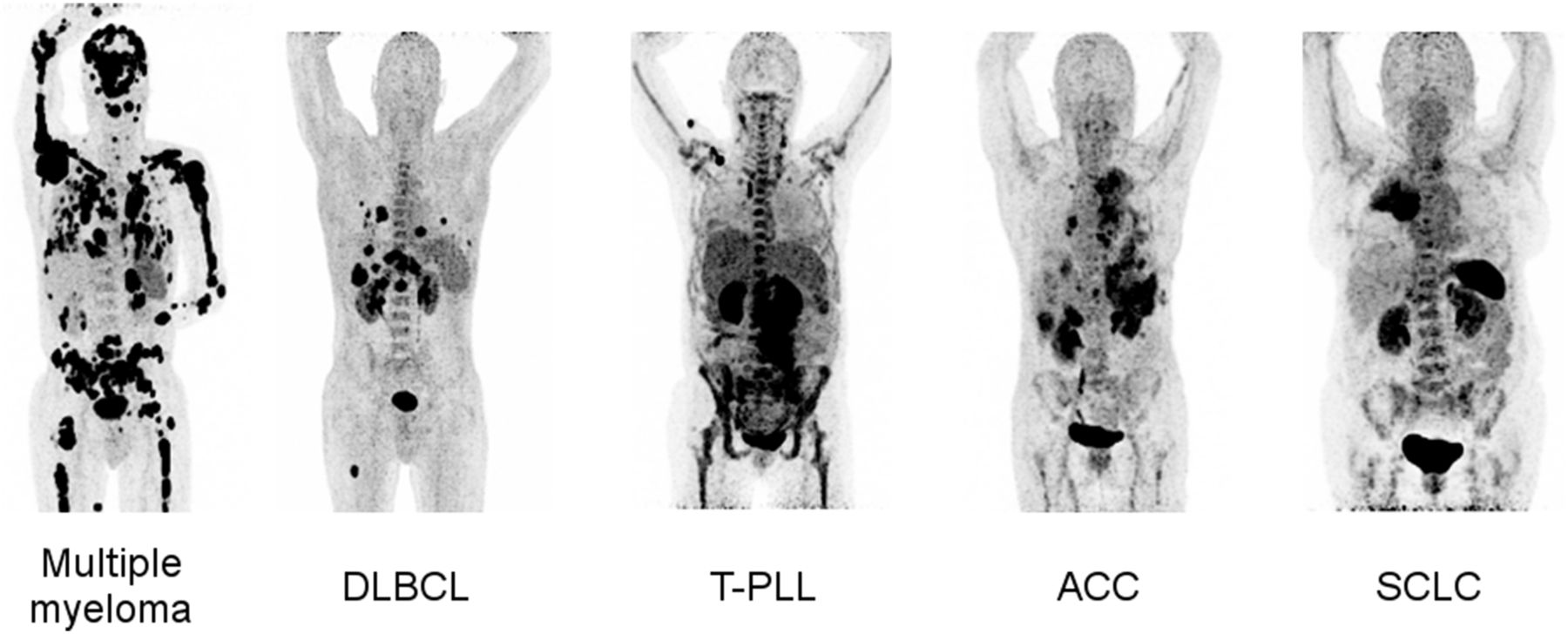
Maximum-intensity projections of different tumor entities undergoing 68Ga-pentixafor PET/CT: multiple myeloma, diffuse large B-cell lymphoma (DLBCL), T-cell prolymphocytic leukemia (T-PLL), adrenocortical carcinoma (ACC), and small cell lung cancer (SCLC).
Interestingly, patients can present with striking inter- and intraindividual receptor expression heterogeneity. Solid tumors, in particular, have demonstrated lower levels of in vivo CXCR4 expression, as is generally described for in vitro expression profiles (78). As a potential explanation, differences between either transcript or whole-protein level analysis of CXCR4 expression and membrane-associated tracer binding in the primary tumor and metastases have been considered (85). Additionally, chemokine receptor expression on the cell surface has been shown to be a dynamic process that is responsive to concomitant or intermittent therapy (Constantin Lapa, unpublished data, 2017). Future studies should investigate the underlying mechanisms and biologic implications (76). So far, the main value of CXCR4 imaging in oncology is not staging of disease but identification of suitable candidates for chemokine receptor–targeted treatment, including radiolabeled and nonradiolabeled options. Most available data concern multiple myeloma, with about two thirds of patients having CXCR4-positive disease (76).
Recently, a peptide ligand that can be labeled with α- or β-emitters (pentixather) and that represents a therapeutic counterpart to the diagnostic PET/SPECT agents was developed (86). Thus, the so-called theranostic concept known from neuroendocrine tumors or even thyroid carcinoma can be applied to various diseases, offering new, exciting options for individualized medicine in terms of endoradiotherapy. The first encouraging results were obtained from small pilot studies with end-stage multiple myeloma patients, in whom CXCR4-directed endoradiotherapy resulted in high initial response rates (87,88). However, given the ultra-high-risk patient population, the duration of the response was relatively short, with median progression-free and overall survival times of 54 and 223 d, respectively (88).
Experience and promising data have also been gained for other hematologic malignancies, such as (relapsed or refractory) acute myeloid leukemia and diffuse large B-cell lymphoma, which could also be effectively targeted by radionuclide therapy (Constantin Lapa, unpublished data, 2015–2017). Up to now, more than 30 therapies have been safely performed and have been well tolerated, without any significant adverse reaction in most cases. However, tumor lysis syndrome was observed in a single case with a high tumor burden and highly dedifferentiated myeloma (88). In all cases, endoradiotherapy was added to standard high-dose chemotherapy as part of the conditioning regimen before stem cell transplantation to augment tumor cell killing and to mediate (expected) CXCR4-directed therapy–induced myeloablation due to receptor expression on the tumor and on physiologic bone marrow progenitor cells. Therefore, endoradiotherapy is especially suitable for hematologic disease, in which tumor and bone marrow ablation is highly desirable and stem cell rescue is not a concern.
Whereas side effects in bone marrow have prevented the use of radionuclide therapy for solid cancers so far, endoradiotherapy could be considered an option for malignancies such as adrenocortical cancer or small cell lung cancer, given the intense receptor expression in relapsed stages and an otherwise dismal prognosis. Future trials will investigate the benefit of endoradiotherapy in patients with multiple myeloma or lymphoma at earlier disease stages (COLPRIT trial; European Union Drug Regulating Authorities Clinical Trials number 2015-001817-28). Future research will also focus on combinations of endoradiotherapy and “conventional” therapies, which could lead to synergistic effects. Both preclinical studies in myeloma cell lines and clinical observations in patients with various diseases (such as myeloma, diffuse large B-cell lymphoma, and acute myeloid leukemia) have suggested the possibility of up- or downregulating CXCR4 on the cell surface. 68Ga-pentixafor could prove to be a useful tool for studying the spatial and temporal orchestration of CXCR4 biology in the process of metastasis, response to and acquisition of resistance to treatment, or disease relapse.
CONCLUSION
CXCR4, a surface receptor that is overexpressed in multiple cancer types, plays a role in various stages of tumor progression and other diseases. CXCR4 inhibitors are in clinical use as bone marrow stem cell or progenitor cell mobilizers and are being investigated either alone or in combination with other systemic treatments in numerous clinical trials. The next major development may be CXCR4-directed endoradiotherapy, for which the results of clinical trials are eagerly awaited.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.
- 57.
- 58.
- 59.
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- Received for publication March 24, 2017.
- Accepted for publication June 2, 2017.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- ERK signaling drives evolutionary expansion of the mammalian cerebral cortex
- CXCR4/ACKR3/CXCL12 axis in the lymphatic metastasis of vulvar squamous cell carcinoma
- Biokinetics and Dosimetry of 177Lu-Pentixather
- Theranostics: Leveraging Molecular Imaging and Therapy to Impact Patient Management and Secure the Future of Nuclear Medicine
- VLA-4 phosphorylation during tumor and immune cell migration relies on its coupling to VEGFR2 and CXCR4 by syndecan-1
- PET Radiopharmaceuticals: Whats New, Whats Reimbursed, and Whats Next?
- Theranostic Concepts: More Than Just a Fashion Trend--Introduction and Overview