


Abstract
The aim of this study was to evaluate the relevance of PET/CT and 18F-FDG as a strategy for response evaluation after chemoradiotherapy for anal cancer. For this, the performance of posttreatment 18F-FDG PET/CT, the impact on patient care, and the predictive value of metabolic response were assessed. Methods: This was a retrospective and multicenter analysis of 87 patients treated by chemoradiotherapy for anal squamous cell carcinoma between October 2007 and October 2013. All patients underwent systematic posttreatment 18F-FDG PET/CT and were followed with at least a clinical examination every 4 mo for 2 y and every 6 mo thereafter. Disease progression was confirmed by biopsy for all patients in the case of local recurrence before surgery. Kaplan–Meier and Cox regression models were used to test for associations between metabolic or clinical endpoints and progression-free survival (PFS) or cause-specific survival (CSS). Results: The median follow-up was 25 mo. 18F-FDG PET/CT was performed 1–8 mo (median, 4 mo) after completion of chemoradiotherapy. Overall, 25 patients relapsed and 13 died. The posttherapy 18F-FDG PET/CT did not show any abnormal 18F-FDG uptake (complete metabolic response [CMR]) in 55 patients whereas 32 displayed incomplete response (non-CMR): 15 patients with partial response and 17 with disease progression. The sensitivity of 18F-FDG PET/CT to detect residual tumor tissue was 92% (95% confidence interval [CI], 75%–97%), specificity was 85% (95% CI, 75%–92%), positive predictive value was 72% (95% CI, 61%–90%), and negative predictive value was 96.4% (95% CI, 90%–98.7%). The 2-y PFS was 96% (95% CI, 90–100) for patients with CMR and 28% (95% CI, 14–47) for non-CMR patients (P < 0.0001). The 2-y CSS was 100% for patients with CMR and 59% (95% CI, 42–84) for those without CMR (P < 0.0001). 18F-FDG PET/CT changed patient management in 14 cases (16%), with relevant modifications in 12 (14%). A Cox proportional hazards model of survival outcome indicated that a CMR was the only significant predictor of PFS and CSS (P < 0.0001). Conclusion: 18F-FDG PET/CT shows good accuracy in posttreatment evaluation of anal cancer and has a relevant impact on patient management. Moreover, CMR is associated with good survival outcome. Thus, 18F-FDG PET/CT may play a significant role during posttreatment follow-up of anal cancer.
Anal carcinoma accounts for 1.5% of cancers of the digestive tract and has a worldwide incidence of 1 in 100,000 persons (1). Remarkably, over the last decades the incidence has increased in developed countries, in particular among younger homosexual men and persons with immunodeficiency (e.g., AIDS, organ graft recipients) (2). This is in relation to the association of anal carcinoma with human papillomavirus, and immunodeficiency facilitates the human papillomavirus–induced malignant transformation (3). Squamous cell carcinoma is the most common histologic type. The standard treatment combines external-beam radiotherapy and chemotherapy with 5-fluorouracil and mitomycin C (4,5). Therapy generally achieves good outcomes: the 5-y disease-free survival rate is 67% (6). Surgery is recommended only for salvage treatment in the case of local failure or recurrence and consists of abdomino-perineal resection and permanent colostomy. Approximately 30% of patients relapse within 2 y after the end of treatment (7). Evaluating the response to treatment is challenging. The current guidelines for posttreatment follow-up include clinical examination and digital rectal examination (8). However, frequent posttreatment anatomic modifications, such as edema, residual fibrosis, or scar tissue, are barely distinguishable from persistent or recurrent disease, even with endo-anal ultrasounds, MRI, and CT imaging. Moreover, posttherapeutic biopsies are associated with a risk of radionecrosis, and their interpretation remains challenging. 18F-FDG PET/CT is recommended as a noninvasive option for initial diagnosis and staging of primary disease by the National Comprehensive Cancer Network guidelines (9–11). Despite conflicting results, pretreatment 18F-FDG PET/CT has been considered as predictive of prognosis in recent studies (12–14).
However, few studies have investigated 18F-FDG PET/CT in evaluating the therapeutic response (15–17). To address this, a retrospective study was performed to evaluate the predictive value of systematic 18F-FDG PET/CT performed after chemoradiotherapy for anal cancer and the impact of this strategy on patient management.
MATERIALS AND METHODS
Patients
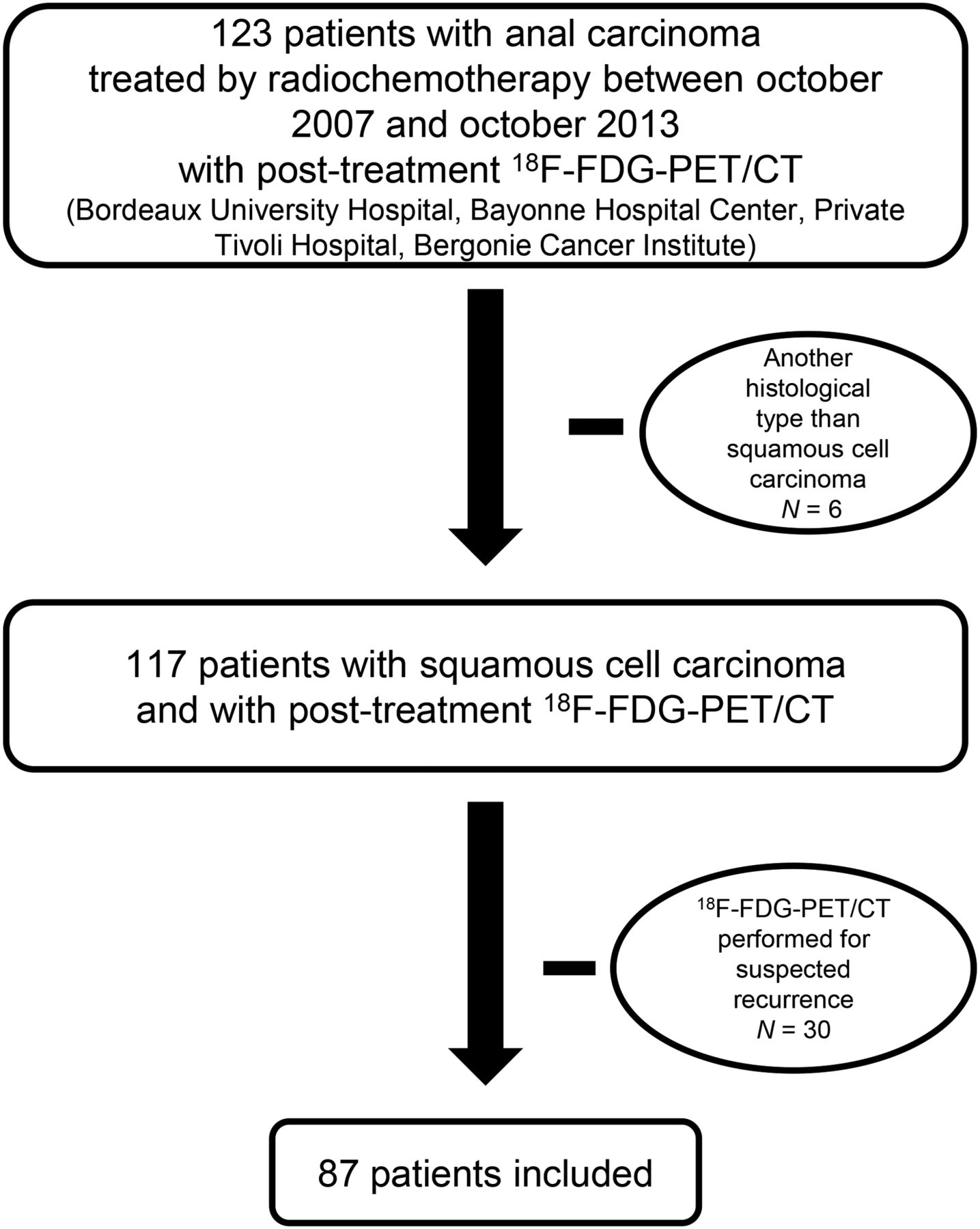
In this retrospective multicenter study, all patients treated with chemoradiotherapy between October 2007 and October 2013 and who had undergone at least 1 systematic 18F-FDG PET/CT during follow-up were included. Patients who had undergone 18F-FDG PET/CT for suspected recurrence were excluded to avoid bias. One hundred twenty-three consecutive patients with biopsy-proven squamous cell cancer of the anal canal were referred to the Bordeaux University Hospital, the Bergonie Cancer Institute (Bordeaux), the Bayonne Hospital Center, and the private Tivoli Hospital (Bordeaux) between October 2007 and October 2013. Thirty-six patients were excluded because they had another histologic type of cancer (n = 6) or because 18F-FDG PET/CT was performed for suspected recurrence (n = 30). The remaining 87 patients were included in this multicenter and retrospective study (Fig. 1). The study was approved by the institutional review board, and the need for written informed consent was waived because it was an observational noninterventional study. All patients underwent pretreatment staging including medical history, physical examination, CT imaging, rectal endosonography, pelvic MRI, and 18F-FDG PET/CT. Tumors were staged according to the Tumor Nodes Metastasis Classification of Malignant Tumors, seventh edition. Treatment consisted of chemoradiotherapy. Chemotherapy combined 5-fluorouracil (5-FU) and mitomycin C for 27 patients, 5-FU and cisplatin for 55 patients, cisplatin and capecitabine for 1 patient, and eloxatine and 5-FU (Folfox regimen) for 1 patient. Two patients received capecitabine only. One patient was not eligible for chemotherapy because his tumor was classified as T1N0M0; he was treated by radiotherapy only.

Study flowchart.
Radiotherapy consisted of external-beam conformational or intensity-modulated radiotherapy to the pelvic nodes, bilateral inguinal nodes, and tumor burden with a mean dose of 45 Gy and an additional boost dose to positive nodal sites and primary tumor based on the physical examination and imaging results. The mean dose on the primary tumor was 62 Gy (range, 45–70.4 Gy; 1.8 Gy per fraction, 5 d per wk).
Image Acquisition and Reconstruction
All patients fasted for 6 h before 18F-FDG administration to achieve a blood glucose level between 0.6 and 1.5 g/L. 18F-FDG was injected intravenously (3.5–4.5 MBq/kg). Imaging was performed between 55 and 90 min (median, 70 min) after 18F-FDG administration, using a Discovery 690 (GE Healthcare) or a Gemini TOF 16 (Philips Healthcare) in 3 different nuclear medicine departments. PET/CT imaging lasted 2–4 min per bed position, depending on patient weight. Patients were administered furosemide intravenously 30 min before imaging to minimize bladder activity.
Transmission and emission scans were obtained from the lower neck to the upper thighs. Emission data were processed using ordered-subset expectation maximization reconstruction. Attenuation correction was performed using the CT data. CT (5-mm slices, 100–130 kV and 100–150 mAs) was performed without administration of intravenous contrast agent. PET data were displayed using commercial software (Advantage Windows PET/CT fusion Workstation 4.6; GE Healthcare) merged with coregistered CT images in coronal, sagittal, and transaxial slices.
Image Interpretation
Images were centrally reviewed by 2 experienced nuclear physicians who had no knowledge of the medical history or patient symptoms. A complete metabolic response (CMR) to treatment was defined as the visual absence of pathologic 18F-FDG uptake (corresponding to an uptake level equivalent to or lower than that in the normal surrounding organ, as previously described), or the presence of a minimal residual uptake, consistent with nonpathologic origin: postradiotherapy inflammatory changes, physiologic uptake in the digestive tract (15) in all baseline lesions identified on baseline imaging workup (pelvis MRI and CT imaging).
Partial metabolic response was defined as any persistent pathologic 18F-FDG uptake in the lesions visible at the baseline imaging workup, including those cases in which the scans were equivocal and residual disease could not be ruled out.
Progressive disease was defined as an area of 18F-FDG uptake within baseline lesions identified on initial imaging workup consistent with tumor growth, or development of a new site of disease. Patients were sorted using the worst response at any site.
Follow-up
Patients had a medical visit at least once a week during the course of treatment. After completing therapy, they were evaluated clinically every 4 mo for the first 2 y, then every 6 mo for the next 3 y. All patients underwent CT imaging (of the chest, abdomen, and pelvis) and pelvic MRI within 6 mo after therapy, then at least once a year. Disease progression was confirmed on biopsies for all patients with local recurrence before surgery and by imaging or biopsy in the case of distant metastases.
Gold Standard, Determination of Diagnostic Performance, and Impact on Patient Care
The diagnostic characteristics of 18F-FDG PET/CT results were evaluated using histologic data (obtained during surgery or by biopsy) and imaging as the gold standard for disease recurrence diagnosis or event-free standard follow-up for complete remission. On this basis, each 18F-FDG PET/CT result was qualified as true-positive, true-negative, false-positive, or false-negative.
18F-FDG PET/CT was considered to have an impact on patient management if it led to additional diagnostic investigations or therapeutic intervention.
Statistical Analysis
Statistical analyses were performed with R Core Team (2014) software (18). Differences in means were compared using a 2-tailed Student t test. χ2 or Fisher exact tests were used for categoric data. Results were considered statistically significant when the P value was less than 0.05. Cause-specific survival (CSS) was defined as the period from the beginning of the treatment to the date of death by anal carcinoma. Progression-free survival (PFS) was defined as the interval from the beginning of the treatment to the date when local or distant disease was diagnosed. The Kaplan–Meier method was used to estimate survival probability. The level of significance was estimated using the log-rank test. A Cox proportional hazards model of survival outcome was performed to evaluate the pretreatment tumor size, pretreatment nodal status (by 18F-FDG PET/CT), HIV status, and posttherapy 18F-FDG PET/CT response (CMR vs. non-CMR) as predictors of disease progression and survival.
RESULTS
Patient and Tumor Characteristics
Among the 87 patients included (median age, 62 y; age range, 35–89 y; 68 women and 19 men), 11 (13%) were HIV-positive, 43 (49%) had a T1 or T2 tumor, and 44 (51%) had a T3 or T4 tumor. Thirty-eight patients (44%) were N0, 50 were N+ (57.5%), and 5 patients had liver metastases (5.7%, Table 1).
Patients and Tumor Characteristics
Follow-up
The median follow-up from treatment initiation was 25 mo (range, 8–76.9 mo); mean follow-up was 29.3 mo (±SD, 15.6). No patient had less than a 6-mo follow-up period. At the end of follow-up, 62 patients (71%) were alive, without evidence of recurrence: in this group, mean follow-up from treatment initiation was 29.7 mo (±SD, 14.1), meaning that 37 patients had more than a 24-mo follow-up, 20 patients had between 12 and 24 mo follow-up, and only 5 patients had between 10 and 12 mo. Twenty-five patients (29%) relapsed: 12 (13.8%) at the locoregional level, 2 (2.3%) had both locoregional and distant recurrence, and 11 (12.6%) had only distant metastases. The 11 metastatic patients displayed several metastatic sites: distant lymph nodes (paraaortic, pulmonary hilum, sus-clavicular; 5 cases), liver metastases (5 cases), peritoneal carcinomatosis (5 cases), pulmonary metastases (3 cases), skin metastases (1 case), and a periureteral mass (1 case). A case of pericarditis carcinomatosis, a case of bone metastasis located in the jaw, and a case in the brain were also diagnosed. Recurrence occurred between 2 mo and 1 y of follow-up. The median time to recurrence was 7 mo. Thirteen patients died from disease progression.
18F-FDG PET/CT and Metabolic Response
Posttreatment 18F-FDG PET/CT was performed 18 mo (median, 4 mo) after the end of treatment. Fifty-five patients (63%) had CMR (Fig. 2), with a mean of 4.6 mo (±SD, 2.0) between the end of treatment and 18F-FDG PET/CT. Thirty-two patients (37%) had persistent abnormal 18F-FDG uptake, with a mean 5.5 mo (±SD, 1.8) between the completion of treatment and 18F-FDG PET/CT; 15 patients (17%) had partial metabolic response (Fig. 3), and 17 (19.5%) had progressive disease (Table 2).

Example of CMR. (A) Pretreatment 18F-FDG PET/CT shows anal tumor on axial slices. Corresponding images, obtained on posttreatment 18F-FDG PET/CT performed 3 mo after chemoradiotherapy (B), show low 18F-FDG uptake (CMR). At end of follow-up, patient was alive and without evidence of recurrence.
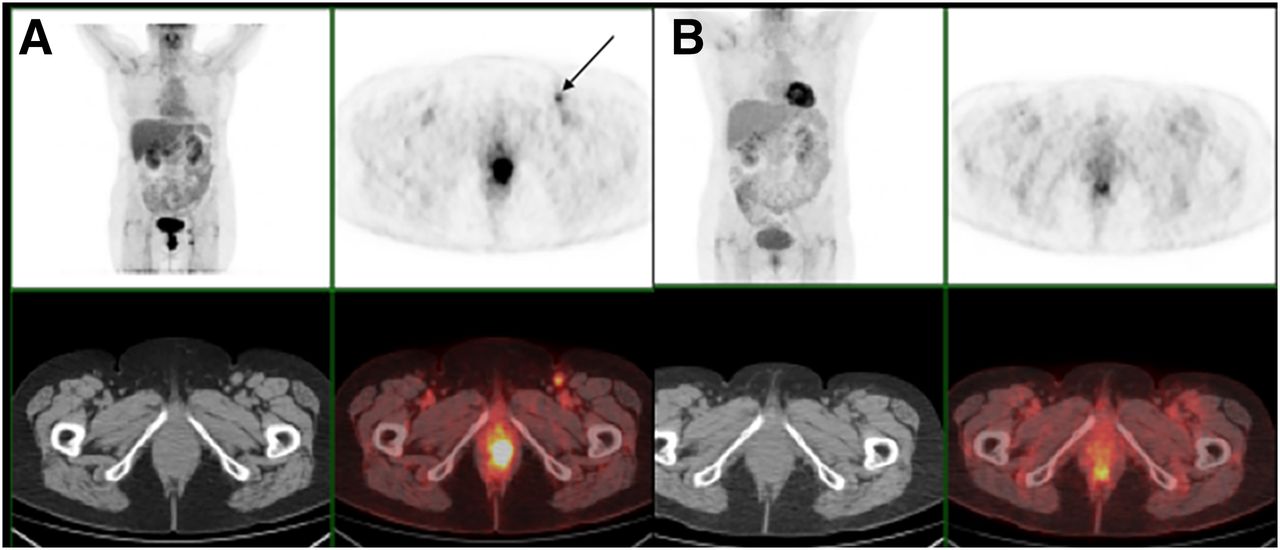
Example of partial metabolic response. (A) Pretreatment 18F-FDG PET/CT shows anal tumor on axial slices and shows left inguinal node (black arrow). Corresponding images, obtained on posttreatment 18F-FDG PET/CT realized 4 mo after chemoradiotherapy (B), show persistent increased 18F-FDG uptake in anal canal (considered as non-CMR), but complete regression of inguinal node uptake. Persistent disease was proven by biopsy.
Cox Multivariate Analysis
Diagnostic Performance of 18F-FDG PET/CT
The mean follow-up after posttherapy 18F-FDG PET/CT was 22.4 mo (±SD, 15.2). For those with recurrence, there was a mean 3.2 mo (±SD, 1.7) between posttherapy 18F-FDG PET/CT and surgery or clinical validation of the 18F-FDG PET/CT findings. For those without recurrence, there was a mean 23.5 mo (±SD, 14.7) between posttherapy 18F-FDG PET/CT and last known status.
Among the 55 patients with CMR, 2 had false-negative 18F-FDG PET/CT results at the primary tumor site. The first patient underwent 18F-FDG PET/CT 1 mo after the end of treatment and biopsy was performed because of clinical symptoms. For the second patient, the 18F-FDG PET/CT performed 5 mo after treatment completion was negative and recurrence occurred at 11 mo. Among the 32 non-CMR patients (with either partial metabolic response or progressive disease), 9 had false-positive 18F-FDG PET/CT results. Two patients had lung uptake, which was later diagnosed as lung adenocarcinoma by biopsy. One immunocompromised patient had increased 18F-FDG uptake in several lymph nodes, but biopsies were negative. Six patients had significant 18F-FDG uptake in the anal canal 3–6 mo after therapy completion, but no actual recurrence was observed at follow-up. In this group, 2 of the 6 patients had negative biopsy. The sensitivity of 18F-FDG PET/CT to detect residual tumor tissue was 92% (95% confidence interval [CI], 75%–97%), specificity 85% (95% CI, 75%–92%), positive predictive value 72% (95% CI, 61%–90%), and negative predictive value 96.4% (95% CI, 90%–98.7%).
Metabolic Response and Survival
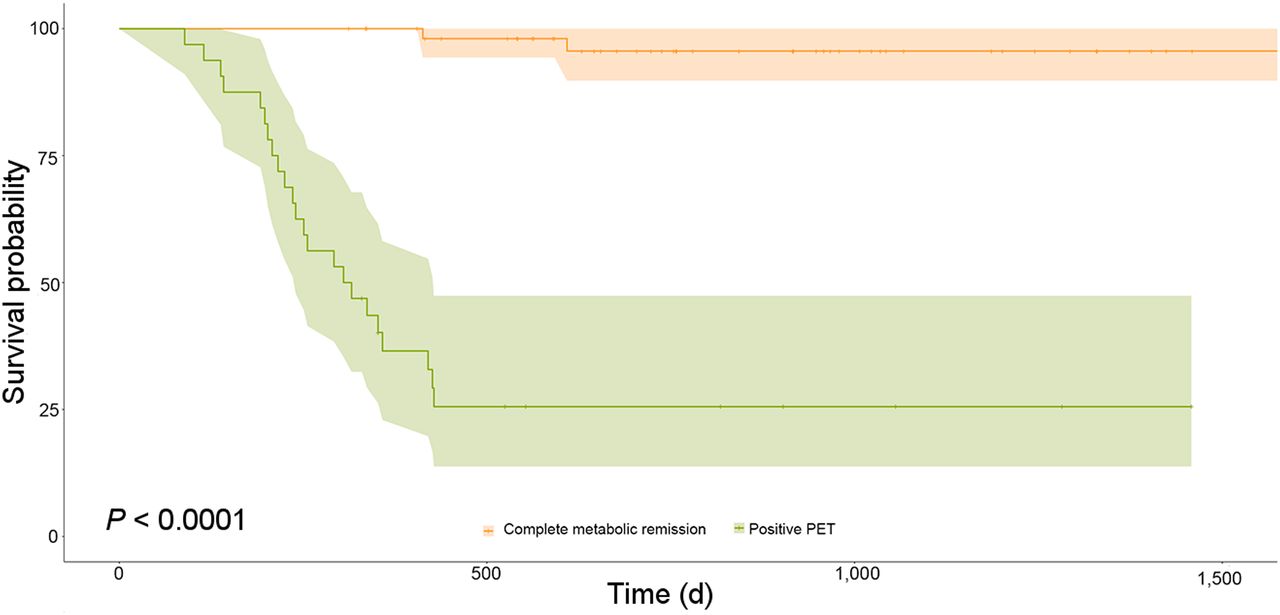
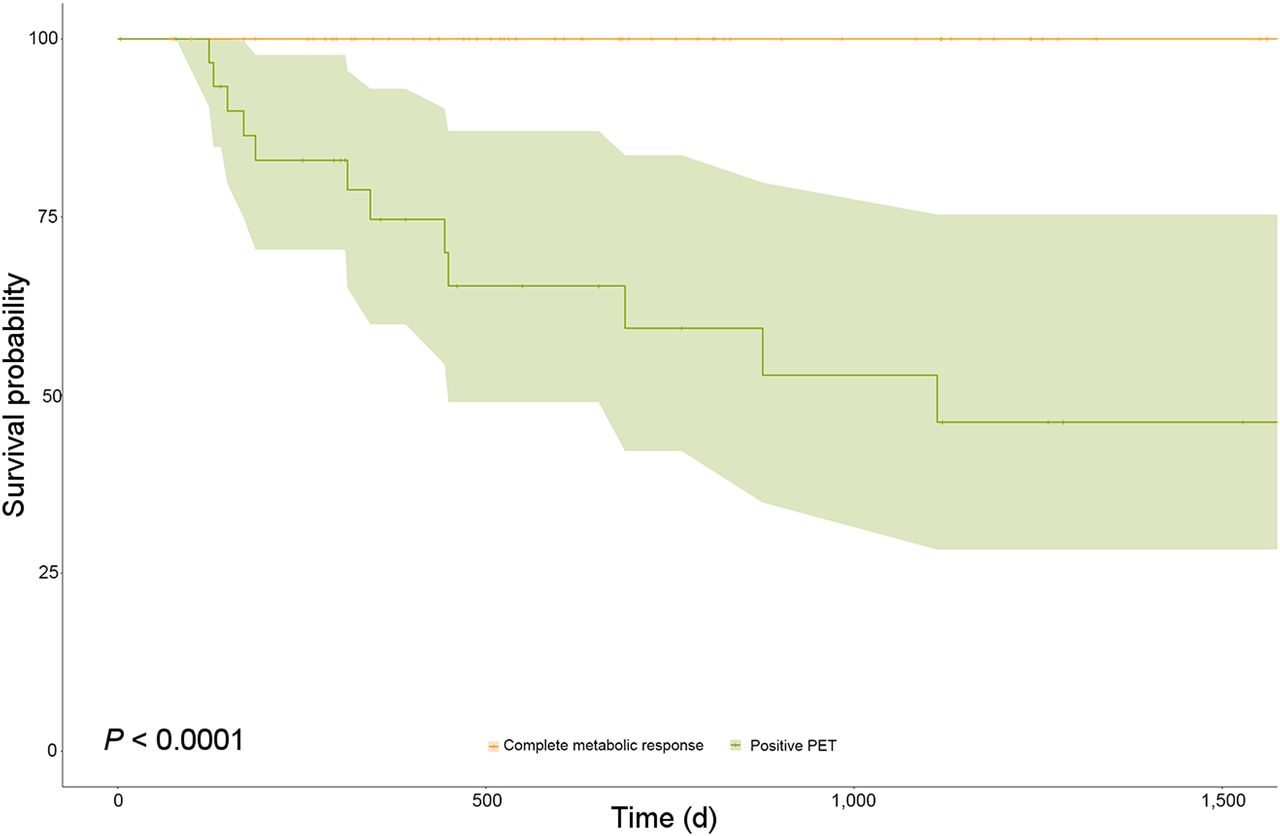
There was a significant association between PFS and tumor response: the 2-y PFS rate was 96% (95% CI, 90–100) for patients with CMR and 28% (95% CI, 14–47) for non-CMR patients (P < 0.0001; Fig. 4). The 2-y CSS rate was 100% for patients with CMR and 59% (95% CI, 42–84) for non-CMR patients (P < 0.0001; Fig. 5).

PFS for patients with CMR on posttreatment 18F-FDG PET/CT and those with abnormal sites of 18F-FDG uptake (partial response, distant recurrence, local and distant recurrence, local recurrence); P < 0.0001.
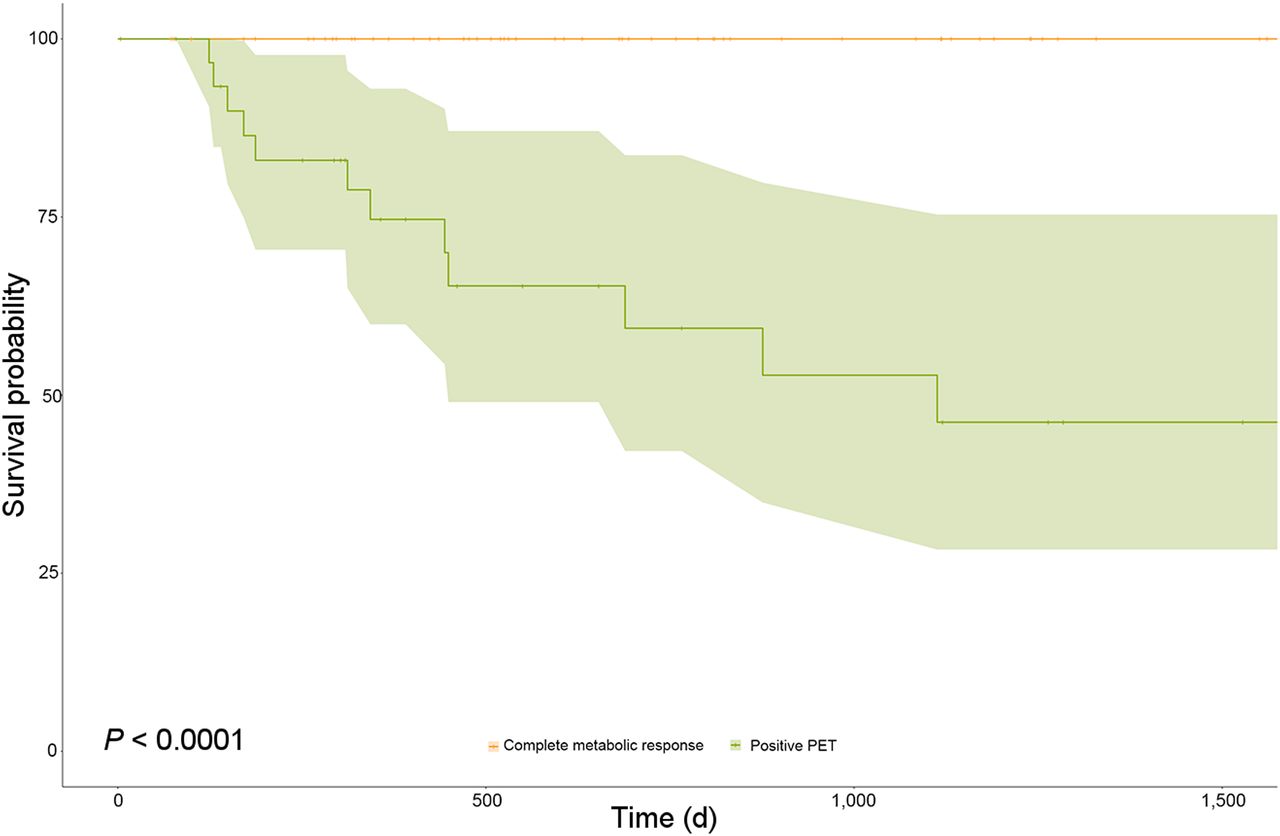
CSS for patients with CMR on posttreatment 18F-FDG PET/CT and those with abnormal sites of 18F-FDG uptake (partial response, distant recurrence, local and distant recurrence, local recurrence); P < 00001.
Impact of 18F-FDG PET/CT on Patient Care
18F-FDG PET/CT changed patient management in 14 cases (16%), with relevant modifications in 12 (14%). Unnecessary biopsy was avoided for 1 patient, despite an inconclusive clinical examination and a positive MRI. Conversely, abdominal–perineal resection was performed in 8 patients who had no suspicious clinical or morphologic results but showed recurrence by pathologic uptake on 18F-FDG PET/CT, which was later confirmed by biopsy. In 2 cases, 18F-FDG PET/CT detected liver metastases, not visible on CT imaging, triggering chemotherapy. 18F-FDG PET/CT found a pulmonary hilar lymph node in 1 patient, who was successfully treated by radiofrequency: histopathologic analysis of the biopsy performed during radiofrequency confirmed a nodal recurrence of the anal cancer. 18F-FDG PET/CT led to unneeded biopsies for 2 patients.
Multivariable Analysis
A Cox proportional hazards model of survival outcome indicated that posttherapy 18F-FDG PET/CT response was the main significant predictor of PFS and CSS (P < 0.0001) whereas initial staging T or N were not significantly associated with PFS or CSS. Positive HIV status was associated with CSS (P = 0.006) (Table 2).
DISCUSSION
18F-FDG PET/CT has been recently used after completion of therapy to assess treatment response of several tumors, including head and neck and cervical squamous cell carcinomas (19–21). For anal cancer, some studies have examined the value of posttreatment 18F-FDG PET/CT (15,22,23), yet they are limited by their small number of patients. To our knowledge, this multicenter study is one of the largest investigations that aimed to assess treatment response and the predictive value of 18F-FDG PET/CT after chemoradiotherapy for patients with anal squamous cell carcinoma with the recently published report (17). In the present study, posttreatment 18F-FDG PET/CT had a high sensitivity (92%) and a high negative predictive value (96.4%), which is consistent with published data (17,22,24,25). This high negative predictive value may prevent unnecessary biopsies or surgery for patients with postradiotherapy modifications, which is particularly clinically relevant because biopsies are associated with a significant risk of necrosis. However, 2 patients had false-negative results at the primary tumor site (18F-FDG PET/CT was performed at 1 and 5 mo) and subsequently relapsed several months after 18F-FDG PET/CT. For the patient who underwent 18F-FDG PET/CT 1 mo after treatment completion, this time frame was probably not optimal. To detect recurrent disease after an initial complete response, longer-term surveillance with 18F-FDG PET/CT could be warranted. The specificity (85%) and positive predictive value (72%) were also similar to published results (17,22,24). Because our intention was to study the place of systematic PET/CT in posttherapeutic evaluation, we decided to exclude patients referred for suspicion of recurrence, considering it would have introduced a major bias. However, this exclusion could have potentially increased the negative predictive value and decreased the positive predictive value. Furthermore, we considered as false-positive the 2 patients presenting lung uptake who were later diagnosed with lung carcinoma by biopsy. In the literature, it is reported that postradiotherapy inflammation or infection may lower the specificity of 18F-FDG PET/CT through concentration of 18F-FDG in activated leukocytes (26). One false-positive was observed in the lymph nodes of an HIV-positive patient. HIV infection or other immunecompromised backgrounds may be associated with persistent generalized lymphadenopathy. In such cases, lymph node biopsy would reveal benign reactive changes with a pattern of follicular hyperplasia (26). 18F-FDG PET/CT scans that were found to be 6 local false-positive results were performed 3–6 mo after treatment. Thus, it is likely that the false-positive uptake of 18F-FDG was not due to early posttreatment inflammation. This illustrates that the optimal timing for 18F-FDG PET/CT to assess tumor response remains a major question, and this is related to the slow decrease in size of anal cancer after therapy, which may take up to 3–6 mo. The Act II trial, a prospective randomized trial including 940 patients, found that 83% of patients had complete response 26 wk after the end of treatment, although 60% of them were considered in partial response at 4 wk (27). In their prospective study of 53 patients, evaluating 18F-FDG PET/CT performed 1 and 3 mo after the end of treatment, Mistrangelo et al. found that 18F-FDG PET/CT at 3 mo had better sensitivity and specificity than 18F-FDG PET/CT at 1 mo (22). These results have been confirmed by the recent study reported by Goldman et al. who found a better predictive value of 18F-FDG PET/CT performed after 12 wk (17). Additional multicenter prospective studies are needed to determine the optimal timing of the posttherapy evaluation.
18F-FDG PET/CT led to relevant therapeutic changes most notably by the detection of local recurrences that were not seen with clinical examination in 8 patients, which were later confirmed by biopsy and led to salvage surgery. This is of particular interest because patients presenting local recurrence can be offered salvage surgical treatment. Recent studies have emphasized the role of complete resection, which correlates with best disease-free survival and CSS: therefore, it is highly beneficial to diagnose recurrence when the tumor is still resectable (8).
It was found that a CMR was associated with significantly improved PFS and CSS, compared with non-CMR. These results are in agreement with previous studies that report that CMR was highly predictive of long-term clinical outcome and more predictive of the survival outcome than T and N status (15,17,23). Surprisingly, we found that T and N staging was not significantly associated with PFS or CSS although these associations have been previously reported (28). It is possible that the high proportion of locally advanced cancers in the present series (T3-T4: 51% vs. 27% in the RTOG 98-11 trial, for instance; N+: 56% vs. 26%) minimizes the importance of T and N status.
Limitations include the retrospective nature resulting in some heterogeneity regarding treatments, 18F-FDG PET/CT protocols (in 3 different nuclear medicine departments), and referral strategies. To minimize heterogeneity, all 18F-FDG PET/CT images have been centrally reviewed by 2 experienced nuclear physicians, without knowledge of clinical results. Patients were treated at 4 different institutions, using conformal 3-dimensional (3D) or intensity-modulated radiotherapy and different protocols regarding chemotherapy. However, even if intensity-modulated radiotherapy can result in a decrease in acute toxicity as compared with conformal 3D (29), it is not proven to increase treatment efficacy. Concerning chemotherapy, all protocols were 5-FU–based differing only by use of platinum-based regimens or mitomycin C. Furthermore, overall results (71% complete response, 29% recurrence) are consistent with the literature (6,28). Regarding referral strategies, practices can differ between physicians, meaning that some physicians prescribe systematically 18F-FDG PET/CT after completion of treatment, whereas others prescribe only 18F-FDG PET/CT in the case of suspicion of residual tumor: to minimize bias, only systematic 18F-FDG PET/CT performed to assess the response has been studied. However, heterogeneity in the timing of posttherapeutic 18F-FDG PET/CT could not be avoided and might be of influence on the results. Another point is that 18F-FDG PET/CT results were evaluated using histologic data (during surgery or by biopsy) and imaging as the gold standard for disease recurrence diagnosis or event-free standard follow-up for complete remission. Therefore, an important question might be whether there was sufficient follow-up in the group without recurrence, knowing that more than 80% of recurrences occur in the first 2 y (ACT II trial) and that 60% of the patients had more than 24 mo-follow-up in our study (7). However, the main strength of this study is its observational nature, which reflects our current medical practice. The recently published metaanalysis suggests that 18F-FDG PET/CT might be valuable during posttreatment follow-up of anal cancer, although more studies are needed to confirm this strategy. The present study, showing significant value of 18F-FDG PET/CT, adds strong evidence to the literature. Furthermore, this approach is currently being investigated in a larger prospective ongoing French national multicentric cohort study (ANABASE; authorization number, 915622), which may provide more precise results. Yet it is still necessary to determine the optimal timing of the posttherapy 18F-FDG PET/CT.
CONCLUSION
This retrospective multicenter study found that 18F-FDG PET/CT has good accuracy in the posttreatment evaluation of anal cancer and has a beneficial impact on patient care. Moreover, CMR was associated with good survival outcome. Taken together, 18F-FDG PET/CT may become an important asset for posttreatment follow-up of anal cancer.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 9, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 12, 2016.
- Accepted for publication February 10, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}