


Abstract
The aim of this study was to explore the ability of 18F-fluoroestradiol (18F-FES) PET/CT imaging to predict pathologic response to neoadjuvant therapy in postmenopausal women with estrogen receptor (ER)–rich breast cancer. Methods: This was a prospective, single-center study conducted as a substudy of the neoadjuvant study of chemotherapy versus endocrine therapy in postmenopausal patients with primary breast cancer (NEOCENT) trial. Patients with ER-rich breast cancer were randomized to neoadjuvant chemotherapy (NC) or neoadjuvant endocrine therapy (NET). The baseline SUVmax of 18F-FES PET/CT was measured. The pathologic response was assessed by the Miller–Payne system as nonresponse (grades 1 and 2) and response (grades 3–5). Results: Twenty-six patients were enrolled, with pathologic response achieved in 25 (NC, 12; NET, 13). Two patients achieved pathologic complete response after NC, but the remaining 23 patients had residual disease after NC or NET. Eight of 12 patients responded to NC, and 4 of 13 to NET; the difference was marginally significant (P = 0.07). In the NC group, the 2 patients with 18F-FES–negative tumors and none of the 10 patients with 18F-FES–avid tumors achieved pathologic complete response (P = 0.02). No difference in the SUVmax between responders and nonresponders was observed in either group. However, 5 of 7 NC patients with a baseline SUVmax of less than 7.3 achieved pathologic response, whereas none of the 5 NET patients with an SUVmax of less than 7.3 were responders (P = 0.03). The SUVmax values of the NC group were negatively correlated with percentage reduction of tumor cellularity (r = −0.63, P = 0.03), whereas those of the NET group showed positive correlation (r = 0.62, P = 0.02). During the median follow-up of 74 mo (range, 44–85 mo), recurrence occurred in only 4 NET patients. In patients with an SUVmax of less than 7.3, recurrence occurred in none of the 8 NC patients and 2 of the 5 NET patients (P = 0.13). Conclusion: Postmenopausal women who are ER-positive, but 18F-FES–negative, may benefit from NC rather than NET. 18F-FES PET/CT has the potential to predict response to neoadjuvant therapy in postmenopausal women with ER-rich breast cancer.
See an invited perspective on this article on page 560.
Neoadjuvant chemotherapy (NC) increases breast-conserving surgery rates and reduces the extent of surgery (1). However, patients with estrogen receptor (ER)–positive tumors have decreased clinical and pathologic response rates to NC compared with those with other subtypes (2). For postmenopausal women with large or locally advanced ER-positive tumors, neoadjuvant endocrine therapy (NET) is an alternative to NC (1). Individual responses to NC or NET vary, ranging from no reduction in tumor size or cellularity to pathologic complete response (pCR). This variability in response may be associated with the heterogeneity of ER-positive operable breast cancer (3). Biomarkers that could help predict response include the degree of ER expression (4,5) and the Ki-67 labeling index (6,7). Conflicting results were reported for the utility of these factors in predicting response (3).
Immunohistochemical testing is currently the most commonly used method for determining ER positivity in clinical practice (8) and is the strongest predictor of endocrine therapy response. However, a subset of ER-positive tumors fails to respond to endocrine therapy (5,9). Tumors with ER splice variants (10,11) and ESR1 ligand-binding domain mutations (12) are identified as ER-positive by immunohistochemical testing, but may lack a functional response to endocrine therapy. A more accurate method of measuring ER function may be valuable for predicting treatment response; this would allow avoidance of ineffective endocrine therapy and instigate switching to more effective treatment.
18F-fluoroestradiol (18F-FES) PET/CT can measure the in vivo binding of estrogens and thus can be used to assess the biologic activity of ER. Earlier studies reported a high positive and negative percentage agreement of 18F-FES PET (87% and 91%, respectively) with ER determined by immunohistochemical testing (13–19). However, the correlation may be lower than that between 18F-FES uptake and in vitro ER concentration determined by radioligand binding (17,20). In vivo radioligand binding measured by 18F-FES PET may differ from in vitro immunohistochemical testing in respect to the ER epitopes determined. 18F-FES PET appears to add further predictive capability, even in patients whose tumors are shown to express ER by in vitro assays (13,16,17).
The neoadjuvant study of chemotherapy versus endocrine therapy in postmenopausal patients with primary breast cancer (NEOCENT) was a phase III, multicenter, randomized trial (ClinicalTrial.gov identifier, NCT00963729) (21). NEOCENT was designed to investigate the efficacy and tolerability of NC versus NET for the downstaging of ER-rich postmenopausal primary breast cancer. We planned an 18F-FES PET/CT substudy, embedded within the NEOCENT trial. The objective was to explore the ability of 18F-FES PET/CT imaging to predict pathologic response to NC and NET in postmenopausal patients with ER-rich breast cancer.
MATERIALS AND METHODS
Study Design
Details on the study design of NEOCENT were reported previously (21). Ethical approval was given by the institutional review board, and the NEOCENT study was conducted in accordance with the Helsinki Declaration. All patients provided written informed consent before participation in NEOCENT. The study on the value of 18F-FES PET/CT, within the larger NEOCENT trial, was undertaken at Asan Medical Center. 18F-FES PET/CT was not used to allocate patients to study groups and had only an ancillary role in the main study, in that its data were not fundamental to the successful completion of NEOCENT. Follow-up data were collected until March 2016.
Patient Eligibility
Postmenopausal patients, aged 70 y or younger, with ER-positive biopsy-proven primary invasive breast cancer (Allred score ≥ 6) were eligible (22). Tumor or nodal burden had to be 2 cm or more by mammogram or ultrasound. Exclusion criteria included the inability to undergo 18F-FES PET/CT imaging due to physical inability, claustrophobia, or mental illness.
Treatments
Patients were randomized to NC or NET (21). NC consisted of 5-fluorouracil, epirubicin, and cyclophosphamide (FEC) administered at 3 weekly intervals for 6 cycles. A switch to docetaxel for 3 cycles was required after 3 cycles if the disease was considered either stable or progressive. This assessment was determined either clinically or by ultrasound, according to RECIST guidelines, version 1.1 (23). For patients allocated to NET, letrozole was administered orally once daily for 18–23 wk until the day before the operation. All patients underwent surgery after NC or NET.
Radiopharmaceutical Preparation
18F-FES was produced as described previously (24). The injectable dose of 18F-FES for this study was 111–222 MBq, with a specific activity greater than 6.3 GBq/μmol (usually > 74 GBq/μmol) at the time of injection. The amount of injected drug was 5 μg or less (≤17 nmol) of 18F-FES.
18F-FES PET/CT Procedure
Baseline 18F-FES PET/CT was performed before NC or NET, and as close to the start of therapy as possible (preferably < 2 wk). 18F-FES imaging was obtained using a PET/CT scanner with a spatial resolution of 4.2 mm (Biograph TruePoint 40; Siemens Healthcare) 90 min after intravenous administration of 18F-FES. Breast tumor PET/CT imaging was acquired with the patient prone, using a breast-positioning aid in 3-dimensional mode. Images were processed with the manufacturer-provided scatter-correction software. Data were reconstructed using True X reconstruction with 3 iterations and 16 subsets and a 336 × 336 matrix with a 2-mm pixel size and slice thickness. A low-dose CT (120 kV CARE Dose4D [Siemens], 50 mAs) scan was acquired, without contrast medium administration, for attenuation correction and lesion localization of the PET scan.
Image Analysis
18F-FES PET/CT images were visually assessed by the consensus of 2 board-certified nuclear medicine physicians who were masked to patient-specific information, treatment assignment, and patient outcome. They were only aware of the location of the breast cancer and were not informed of any other characteristics of the clinical and laboratory findings.
The intensity of 18F-FES PET/CT uptake was categorized as increased, equal to, or decreased, relative to the background uptake in normal comparative tissue. A finding of 18F-FES uptake above background (increased intensity) in the primary breast tumor or lymph node was interpreted as being 18F-FES–avid. 18F-FES PET/CT was regarded as negative if all lesions had equal to, or decreased, uptake relative to background. The SUV was normalized to the injected dose and the patient’s body weight. The SUVmax was defined as the highest single maximum pixel value within the primary tumor and lymph nodes.
Pathologic Assessment
All archived hematoxylin and eosin–stained core-needle biopsy and surgical samples were reviewed by 2 or more pathologists. Semiquantitative ER and progesterone receptor expression was evaluated according to the Allred score (22). The tumors were defined as human epidermal receptor 2 (HER2)–positive if they had an immunohistochemical score of 3+. HER2 amplification by fluorescence in situ hybridization or silver in situ hybridization was not performed.
Percentage reduction of cellularity between pretreatment core-needle biopsies and posttreatment surgical specimens was measured. Pathologic response was assessed using the Miller–Payne grading system based on percentage reduction of cellularity (25). Patients showing Miller–Payne grades 3–5 were grouped as responders and patients with grade 1 or 2 as nonresponders. pCR was defined as the absence of residual invasive cancer on hematoxylin and eosin evaluation of the complete resected breast specimen and all sampled regional lymph nodes (ypT0/Tis ypN0).
Statistical Analysis
Data are reported as mean and SD. Positive percentage agreement between immunohistochemical testing and 18F-FES PET/CT was defined as the proportion of patients with 18F-FES–avid uptake among those whose cancer was ER-positive by immunohistochemical testing. Quantitative parameters were compared using a t test. Comparison of categoric data was conducted using a χ2 or Fisher exact test. The correlation of 18F-FES uptake with the rate of reduction in tumor cellularity was assessed using the Pearson correlation coefficient. Two-tailed P values of less than 0.05 were considered significant. Disease-free survival was defined as the interval between randomization and occurrence of a first event, last follow-up, or death. The significance of differences between Kaplan–Meier survival curves was determined using the log-rank test. All statistical tests were conducted using IBM SPSS Statistics version 21 for Windows (SPSS, Inc./IBM Co.).
RESULTS
Patients and Treatment
Forty-two postmenopausal patients were screened for eligibility at Asan Medical Center between November 2008 and March 2011 (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). Of these, 27 patients met the eligibility criteria and were randomized to NC or NET. One patient who was randomized to NET declined to undergo 18F-FES PET/CT because of claustrophobia. This left 26 patients for the full analysis (NC, 13; NET, 13). Baseline characteristics were similar in both treatment arms (Table 1). Seven NC patients received all 6 cycles of FEC, but 6 patients were switched to docetaxel after 3 cycles of FEC. All NET patients took letrozole up to the day of surgery.
Baseline Characteristics of Patients and Pathologic Response After Neoadjuvant Therapy
18F-FES PET/CT, Surgery, and Pathologic Response
The specific activity of formulated 18F-FES for intravenous administration was 162.1 ± 80.0 (mean ± SD) GBq/μmol (range, 77.3–338.0 GBq/μmol). The decay-corrected radiochemical yield was 27.7% ± 3.2%, and the radiochemical purity was 98.4% ± 2.5%. The time interval between the diagnosis of breast cancer and 18F-FES PET/CT was 16.3 ± 6.1 d. 18F-FES PET/CT was performed within 3 d (median, 0; range, 0−3 d) before commencement of NC or NET. The administered activity of 18F-FES was 204 ± 18 MBq. The time interval between injection of 18F-FES and PET/CT imaging was 91.0 ± 5.2 min.
Twenty-four patients had 18F-FES–avid uptake, and 2 had negative 18F-FES accumulation with agreement between the 2 readers. Positive percentage agreement between immunohistochemical testing and visual 18F-FES PET/CT was 92.3% (24/26 patients). The SUVmax of 18F-FES PET/CT was 9.3 ± 7.5 (range, 1.2−38.9). There was a marginal difference in the baseline SUVmax of 18F-FES between the 2 groups (P = 0.06, Table 1).
Pathologic response was not assessed in 1 patient because her pretreatment biopsy specimen was not available. There were no differences in the type of surgery performed and the pathologic response between the NC and NET groups (Table 1; Supplemental Table 1). Two patients achieved pCR after NC; however, the rest of the 23 patients had residual disease after NC or NET. Eight of 12 patients responded to NC (Miller–Payne grade 3, 4, or 5) and 4 of 13 to NET; the difference between the groups was marginally significant (P = 0.07). However, the percentage reduction of tumor cellularity was higher after NC than after NET (Table 1). There was no significant difference in the incidence of HER2 positivity between responders and nonresponders in both arms (P > 0.05).
18F-FES Uptake and Correlation with Pathologic Response and Survival
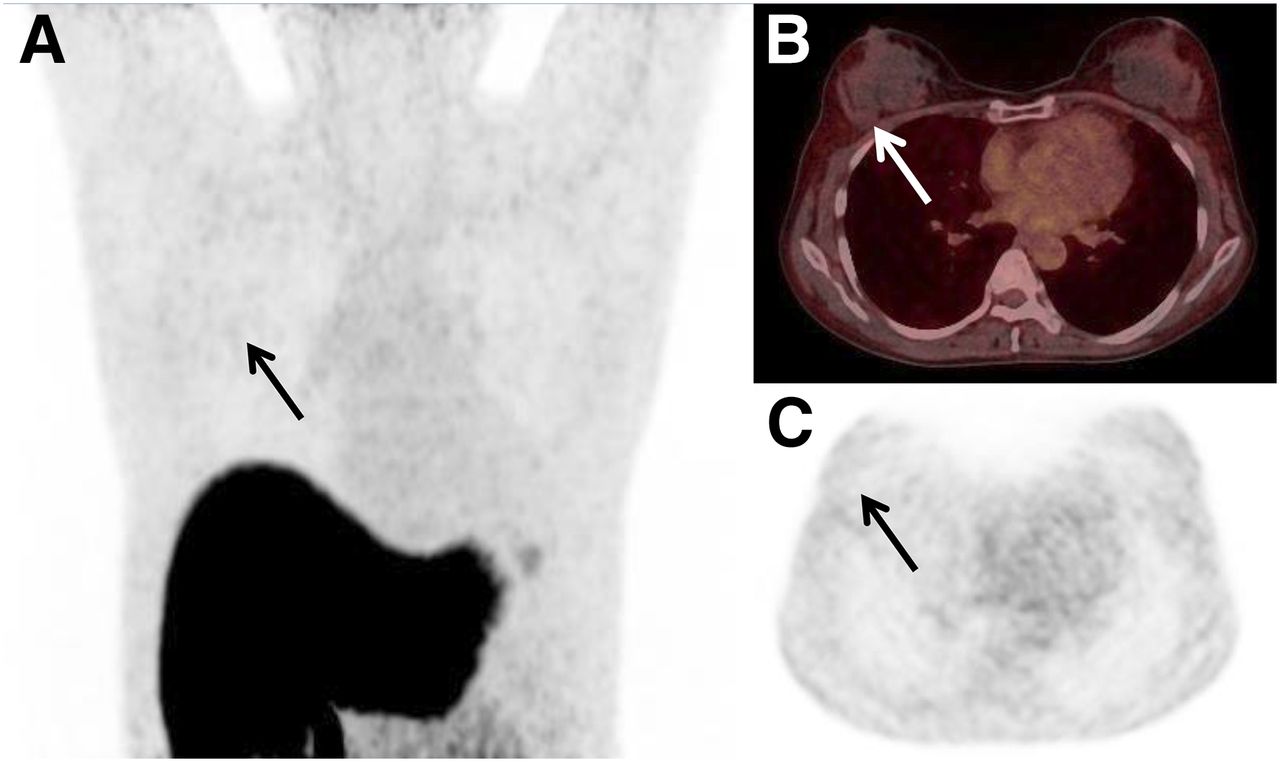
In the NC group, the 2 patients with 18F-FES–negative tumors achieved pCR (Fig. 1; Supplemental Fig. 2), whereas none of the 10 18F-FES–avid patients achieved pCR (P = 0.02). No difference in the SUVmax between responders and nonresponders was observed (Fig. 2). However, SUVmax and percentage reduction of tumor cellularity showed a negative correlation (r = −0.63, P = 0.03, Fig. 3). No differences in the SUVmax, percentage reduction of cellularity, or pathologic response were observed between patients who received FEC only and those who received FEC with docetaxel.
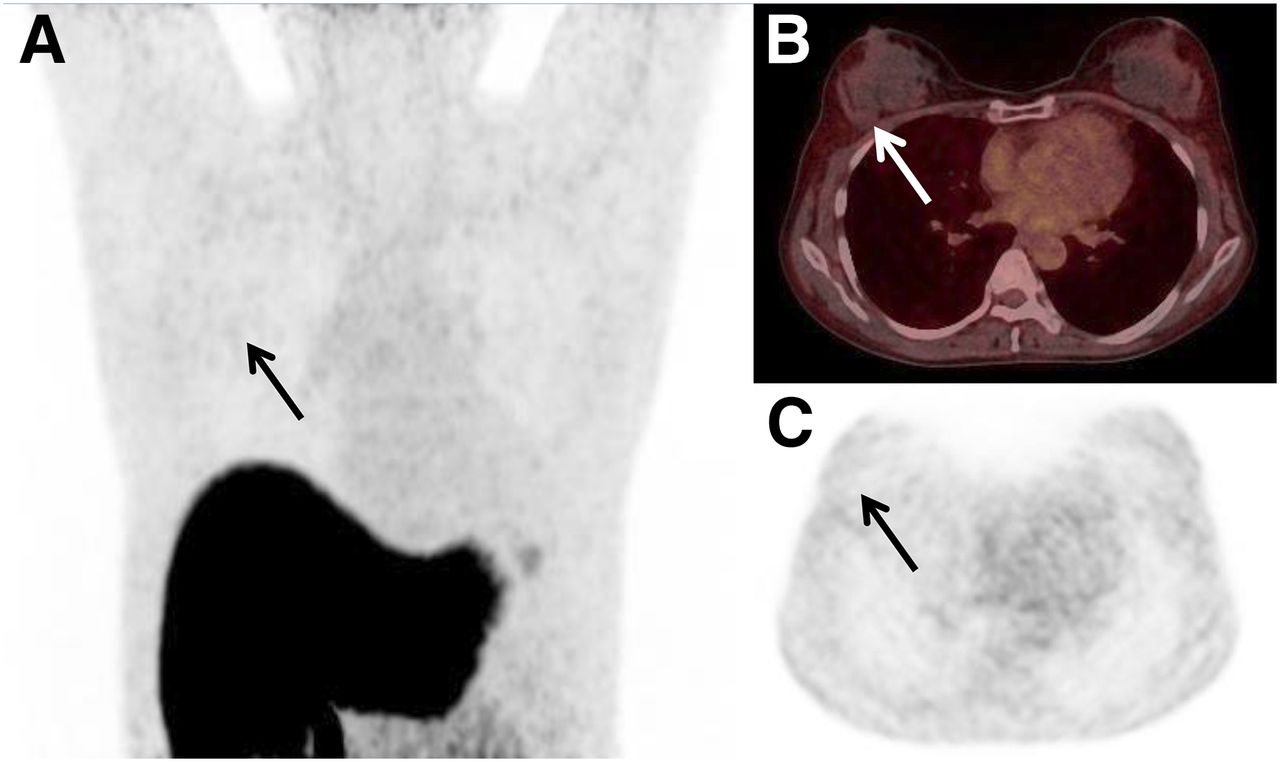
A 52-y-old female patient with histologic grade 2, ER-positive (Allred score, 8), progesterone receptor–negative and HER2-negative, right-breast cancer. Maximum-intensity-projection (A) and transverse PET/CT (B and C) images show negative 18F-FES uptake (arrows: SUVmax = 1.2), which is equal to background activity. pCR was achieved after NC.

Distribution of SUVmax of 18F-FES PET/CT according to pathologic response. There were no differences in 18F-FES uptake between responders and nonresponders in either NC (A) or NET (B) arms. Five of 7 NC patients with baseline SUVmax < 7.3 (A, below the dashed line) achieved a pathologic response, but none of the 5 NET patients with SUVmax < 7.3 (B, below the dashed line) responded to treatment (P = 0.03).

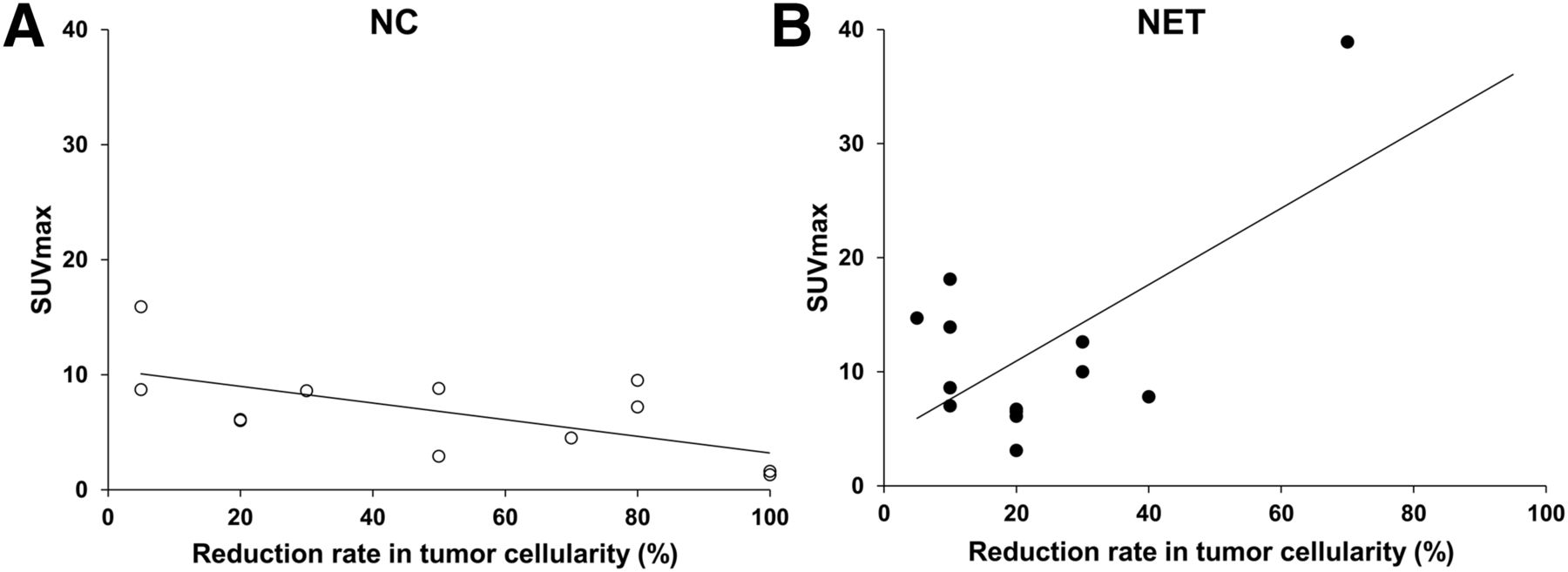
Relationship between SUVmax of 18F-FES uptake and percentage reduction of tumor cellularity in NC (A) and NET (B) groups. SUVmax in NC group negatively correlates with reduction rates in tumor cellularity (r = −0.63, P = 0.03), whereas positive correlation is seen in NET group (r = 0.62, P = 0.02).
All 13 patients who received NET had 18F-FES–avid uptake, but none achieved pCR (Fig. 4). As with the NC group, there was no significant difference in SUVmax between responders and nonresponders after NET (Fig. 2). In contrast to those in the NC group, SUVmax in the NET group was positively correlated with percentage reduction of tumor cellularity (r = 0.62, P = 0.02, Fig. 3). We found a similar correlation after removal of HER2-positive patients (Supplemental Fig. 3).

A 68-y-old female patient with histologic grade 2, ER-positive (Allred score, 8), progesterone receptor–negative and HER2-negative, left-breast cancer. Maximum-intensity-projection and transverse PET/CT images show 18F-FES–avid uptake in both left-breast cancer (A, B, and C, solid arrows) and left axillary lymph node (A, D, and E, dotted arrows). SUVmax values of left-breast cancer and left axillary lymph node are 17.0 and 38.9, respectively. Pathologic response of Miller–Payne grade 3 was achieved after NET.
When the cutoff was chosen to maximize nonresponders to NET, 5 of 7 NC patients with a baseline SUVmax of less than 7.3 achieved a pathologic response, but none of the 5 NET patients with an SUVmax of less than 7.3 responded to treatment (P = 0.03, Fig. 2). In patients with a high SUVmax of 7.3 or more, there was no difference in pathologic response between the 2 treatment groups (Fig. 2).
During the median follow-up of 74 mo (range, 44–85 mo), recurrence occurred in only 4 patients with NET, and 1 died after recurrence. NC was associated with significantly higher rates of disease-free survival than NET (P = 0.04, Supplemental Fig. 4). Recurrence occurred in none of 8 NC patients and in 2 of 5 NET patients with an SUVmax of less than 7.3 (P = 0.13).
DISCUSSION
In this study, 2 of 26 patients lacked qualitative 18F-FES accumulation. The SUVmax of 18F-FES PET/CT was highly variable, ranging from 1.2 to 38.9. Patients with 18F-FES–negative tumors achieved significantly increased rates of pCR after NC compared with those with 18F-FES–avid tumors. A low baseline SUVmax of less than 7.3 predicted a pathologic response to NC but a lack of pathologic response to NET. SUVmax and percentage reduction of tumor cellularity were negatively correlated with NC but positively correlated with NET. This study indicates that there may be an interaction between 18F-FES uptake status and treatment. In tumors with a low 18F-FES uptake, pathologic response with NC may be superior to that with NET, whereas in the patients with a high 18F-FES uptake, the pathologic response may not differ.
Currently, pCR is used as a surrogate endpoint for the evaluation of the efficacy of novel neoadjuvant systemic therapies for invasive breast cancer (26). However, there are no acceptable surrogate endpoints for ER-positive breast cancer because of the lower rates of pCR and weaker association with event-free survival (2,27). Furthermore, patients with ER-positive tumors have a more favorable long-term prognosis and are more likely to be cured with currently available therapy. Nevertheless, in ER-positive breast cancer, achieving a pCR after NC predicts favorable survival, as it does in high-risk subtypes (2,27). Therefore, an important finding was that postmenopausal women who were ER-positive, but 18F-FES–negative, achieved a significantly increased rate of pCR after NC compared with those who were 18F-FES–avid. A negative 18F-FES examination may guide clinicians to consider NC rather than NET, which may translate into an improved outcome.
Our results indicate that a subgroup of patients with ER-positive breast cancer have nonfunctional ER and might benefit from NC. A similar result was reported in 5 patients who had breast cancer that was ER-positive by immunohistochemical testing and 18F-FES–negative (13). Of the 4 patients who were treated with chemotherapy, 2 complete responses and 1 partial response were achieved. Recently, Yang et al. reported that pretreatment 18F-FES uptake was significantly lower in responders than in nonresponders (28). In contrast to previous studies, the current study included ER-rich breast cancer patients who were randomized to NC or NET. We are unable to conclusively explain why breast cancers may be ER-positive by immunohistochemical testing and 18F-FES–negative. However, besides ESR1 ligand-binding domain mutation, this may be related to luminal B (29) or nonluminal intrinsic subtypes (11,30). Future directions should include further refinement of 18F-FES PET/CT as a predictive marker in relation to immunohistochemistry or genetic studies.
This study used a standard 2-arm randomization design comparing NC and NET outcomes, which enabled us to minimize the effect of any potential bias. Importantly, this study allowed us to infer a treatment by diagnostic test result interaction. The results are novel in that we identified the value of 18F-FES uptake as a potential predictive marker for neoadjuvant therapeutic decision making in women with ER-rich breast cancer. 18F-FES PET/CT is promising and may help guide the choice of therapy in the neoadjuvant setting.
Our study is limited in that the pathologic response and correlation with 18F-FES uptake may have less prognostic relevance in patients with ER-rich breast cancer. However, one of the most important goals of NC or NET is to enable more limited surgery. The residual tumor extent, which is important for surgical planning after NC or NET, may not be accurately assessed by clinical examination and imaging studies in patients with ER-positive breast cancer (31). There may be clinical value in a pathologic partial response, allowing reduced surgery (1). Examination of the partial response may provide more information on the relationship between pathologic residual disease and clinical outcome than consideration of the pCR alone (32).
The low number of patients is a limitation of this study. Nonetheless, in this prospective randomized study, there were no potential sources of bias that might have led to the systematic over- or underestimation of the predictive value of 18F-FES PET/CT. An additional limitation may be the inclusion of patients with positive HER2 expression. However, endocrine therapy is also indicated for patients who are luminal B HER2-positive. The randomized design and lack of difference in HER2 positivity between the groups in this study might have minimized the effect of HER2 positivity on the study’s conclusion. Further large studies with a homogeneous study population should be performed. A final limitation is the lack of quantitative gene expression-based assays. We focused only on the functional heterogeneity of 18F-FES PET/CT-determined ER status in patients with homogeneous ER-rich expression as assessed by immunohistochemical testing. Evaluation of other predictive markers for treatment response and outcome was beyond the scope of this substudy of NEOCENT. Further studies should include competing genomic biomarkers such as the 21-gene assay to assess 18F-FES uptake as a predictive marker more precisely (33).
CONCLUSION
We found that in ER-rich patients with a low 18F-FES uptake, pathologic response with NC may be superior to that with NET. Therefore, 18F-FES PET/CT has potential clinical implications in the selection of either NC or NET in postmenopausal women with ER-rich breast cancer. Adequately powered prospective studies in a larger number of ER-positive patients are needed to establish the role of pretreatment 18F-FES PET/CT imaging as a predictive marker of therapeutic efficacy in the neoadjuvant setting.
DISCLOSURE
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HI06C0868). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank investigators in the NEOCENT trial (chaired by Professor R. Charles Coombes).
Footnotes
↵* Contributed equally to this work.
Published online Sep. 29, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 17, 2016.
- Accepted for publication September 3, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Fluoroestradiol PET/CT for Predicting Benefit from Endocrine Therapy in Patients with Estrogen Receptor-Positive Breast Cancer: A Systematic Review and Metaanalysis
- Impact of 18F-FES PET/CT on Clinical Decisions in the Management of Recurrent or Metastatic Breast Cancer
- Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16{alpha}-18F-Fluoro-17{beta}-Fluoroestradiol
- Breast Cancer: Evaluating Tumor Estrogen Receptor Status with Molecular Imaging to Increase Response to Therapy and Improve Patient Outcomes
- Recent Advances in Imaging Steroid Hormone Receptors in Breast Cancer