


Abstract
This study aimed to assess a hypothetical minimum administered activity of 124I required to achieve comparability between pretherapeutic radioiodine uptake (RAIU) measurements by 124I PET/CT and by 131I RAIU probe, the clinical standard. In addition, the impact of different reconstruction algorithms on 124I RAIU and the evaluation of pixel noise as a parameter for image quality were investigated. Methods: Different scan durations were simulated by different reconstruction intervals of 600-s list-mode PET datasets (including 15 intervals up to 600 s and 5 different reconstruction algorithms: filtered-backprojection and 4 iterative techniques) acquired 30 h after administration of 1 MBq of 124I. The Bland–Altman method was used to compare mean 124I RAIU levels versus mean 3-MBq 131I RAIU levels (clinical standard). The data of 37 patients with benign thyroid diseases were assessed. The impact of different reconstruction lengths on pixel noise was investigated for all 5 of the 124I PET reconstruction algorithms. A hypothetical minimum activity was sought by means of a proportion equation, considering that the length of a reconstruction interval equates to a hypothetical activity. Results: Mean 124I RAIU and 131I RAIU already showed high levels of agreement for reconstruction intervals of as short as 10 s, corresponding to a hypothetical minimum activity of 0.017 MBq of 124I. The iterative algorithms proved generally superior to the filtered-backprojection algorithm. 124I RAIU showed a trend toward higher levels than 131I RAIU if the influence of retrosternal tissue was not considered, which was proven to be the cause of a slight overestimation by 124I RAIU measurement. A hypothetical minimum activity of 0.5 MBq of 124I obtained with iterative reconstruction appeared sufficient both visually and with regard to pixel noise. Conclusion: This study confirms the potential of 124I RAIU measurement as an alternative method for 131I RAIU measurement in benign thyroid disease and suggests that reducing the administered activity is an option. CT information is particularly important in cases of retrosternal expansion. The results are relevant because 124I PET/CT allows additional diagnostic means, that is, the possibility of performing fusion imaging with ultrasound. 124I PET/CT might be an alternative, especially when hybrid 123I SPECT/CT is not available.
Radioiodine therapy (RAIT) with 131I is a relevant intervention because of the high prevalence of benign thyroid diseases (1). Although pretherapeutic radioiodine uptake (RAIU) measurement is usually performed with a 131I probe and is considered the clinical standard, a recent study on the correlation between 131I probe RAIU measurement and 124I PET/CT RAIU measurement has shown that application of as little as 1 MBq of 124I provides RAIU results comparable to those obtained with 3 MBq of 131I (2). Thus, 124I PET/CT may become a good alternative for routine evaluations of RAIU in patients with benign thyroid disease, especially because 124I PET/CT may provide additional diagnostic information. Indeed, the functional anatomy shown by 124I PET is superior to that shown by conventional 99mTcO4 thyroid scintigraphy (3). Also, the 124I RAIU method allows a time-efficient PET-based organ volumetry (4). In addition, there exists the possibility of performing PET/ultrasound image fusion (5–7).
Different activities in one patient can be simulated by obtaining a 124I PET/CT scan in list-mode technique and equating reduction of scan time with reduction of activity. The focus of this study was to assess only the uptake aspect of RAIU. No information was obtained about the effective half-life aspect of RAIU. The goals of this study were to assess a hypothetical minimum activity that will achieve comparable results between 124I RAIU measurement and the clinical standard, 131I RAIU measurement; to determine the influence of different reconstruction algorithms on 124I RAIU measurement; and to evaluate pixel noise as a parameter for image quality.
MATERIALS AND METHODS
Patients and Ethics
The study included consecutive patients with benign thyroid diseases referred to our institution from April 2012 to June 2014 in preparation for RAIT. The study was designed as a subanalysis within a larger prospective study approved by the local ethics committee and the German Federal Office of Radiation Protection. All participants signed a written informed consent form.
Study Protocol
Thyroid Diagnostics
The initial thyroid diagnostic was performed according to current guidelines (anamnesis; measurement of thyroid-stimulating hormone, free T3, and free T4; neck ultrasound; and planar 99mTc-pertechnetate scintigraphy) (8–10).
Inclusion and Exclusion Criteria
Criteria for inclusion were the diagnosis of a benign thyroid disease potentially requiring treatment (e.g., RAIT with the aim of volume reduction). Patients were excluded if they had received thyroid-specific treatment in the previous 12 wk, if their anamnesis was positive for iodine contamination, or if a relevant change in thyroid metabolism (as assessed by thyroid-stimulating hormone levels) occurred between the investigations.
Tracer Preparation
Sodium-131I solution (GE Healthcare) and sodium-124I tracer solution (BV Cyclotron VU) were poured into identical capsules (HGK, size 3; GE Healthcare) on a crystalline carrier. The tracer activity of the test capsules was measured using a dose calibrator (Isomed 2010; MED Nuklear-Medizintechnik).
Tracer Administration and RAIU Measurement Schedule
Oral administration of 131I capsules (3 MBq) was performed first; 124I capsules (1 MBq) were administered 7–14 d later. Each RAIU was measured 30 h after administration. Before this study, phantom experiments demonstrated that residual 131I does not interfere with quantification of 124I in PET/CT examination (2).
131I Probe Measurement
The activity in patients was measured using an ISOMED 2162 thyroid uptake counter (MED Nuklear-Medizintechnik). The measuring distance between detector and neck was kept at 45 cm using a spacer. The detector fitted with an NZ-136-01 collimator (MED Nuklear-Medizintechnik) had dimensions of 5 × 5 cm and was connected to a multichannel analyzer through a photomultiplier tube. For quality assurance purposes, each measurement was preceded by a check of the energy spectrum using a 137Cs test source, as well as by measurement of the background activity. The determined lower limit of detectability was 7 kBq.
124I PET/CT
124I PET/CT scans were acquired using a Biograph mCT 40 system (Siemens). The scans were scheduled late in the afternoon following clinical routine to ensure a high adherence to the appointed date. 124I PET imaging was performed in list-mode acquisition by continuous scanning for 600 s, with every measured value stored as raw data with an exact time stamp to allow reconstruction of intervals of different length as static images, simulating scan intervals of different length.
Patients were scanned supine at one bed position. The scan region included the whole neck and the upper thorax. Anatomic coregistration and attenuation correction were performed using a native CT scan at its lowest tube setting (30 mA), with 120-kV tube voltage, 3-mm scan slice width, and 1.2 pitch. The PET system showed a 3-dimensional sensitivity of 9.5 cps/kBq/mL. At 1 cm, the axial resolution was 4.4 mm and the transverse resolution 4.5 mm. The scatter fraction was below 36%. Quality control was performed daily and weekly according to the standards of the National Electrical Manufacturers Association.
124I PET Reconstruction Intervals (RI)
List-mode data were reconstructed using the software HD-TrueX (Siemens), with 15 RIs of different lengths, that is, 600 s, 540 s, 480 s, 420 s, 360 s, 300 s, 240 s, 180 s, 120 s, 60 s, 50 s, 40 s, 30 s, 20 s, and 10 s.
124I PET Reconstruction Algorithms
Images were reconstructed using 2 different processes, that is, filtered backprojection (FBP) and iterative technique (IT). The IT consisted of different combinations of the 4 reconstruction parameters, image matrix, iterations, subsets, and zoom. One or maximally 2 parameters were changed according to the locally established reconstruction algorithm (IT-1) (Table 1) (2–4). Each RI was reconstructed with the 5 different reconstruction algorithms.
Overview of Reconstruction Algorithms and Parameters
Quantitative Analysis
131I RAIU Measurement
The computer-based assessment proceeded by means of the dedicated standard software UPT 2000 (MED Nuklear-Medizintechnik). The thyroid activity was calculated as ratio of counts measured in the patients’ field of view versus the counts measured in a standard phantom, in both cases after subtraction of the background counting rate. 131I RAIU was calculated by dividing measured counts by applied activity, considering decay correction and calibration of the 131I probe.
124I RAIU Measurement
The 124I PET and CT datasets were fused using the software PMOD, version 3.408 (PMOD Technologies Ltd.), and quantified using the volume-of-interest (VOI) technique. A cylinder-shaped VOI was placed on the neck, ensuring that the mandible and any retrosternal thyroid parts were included, enabling the measurement of any activity within this region (Fig. 1) (2). Mean activity concentration (kBq/mL) and its SD were measured in each VOI. A background correction VOI was not used because of the high specific uptake within the thyroid compared with surrounding tissue. 124I RAIU was calculated by dividing measured activity within the VOI by applied activity. In analogy to other studies, a correction of the measured activities based on the difference in decay between 124I and 131I was performed, allowing a comparison of the activities of the two radionuclides (2).

Transversal (A) and sagittal (B) 124I PET/CT images (IT-1 reconstruction; 600 s), with cylinder-shaped VOI indicated by yellow line.
Data Analysis
Comparison of 131I RAIU and 124I RAIU
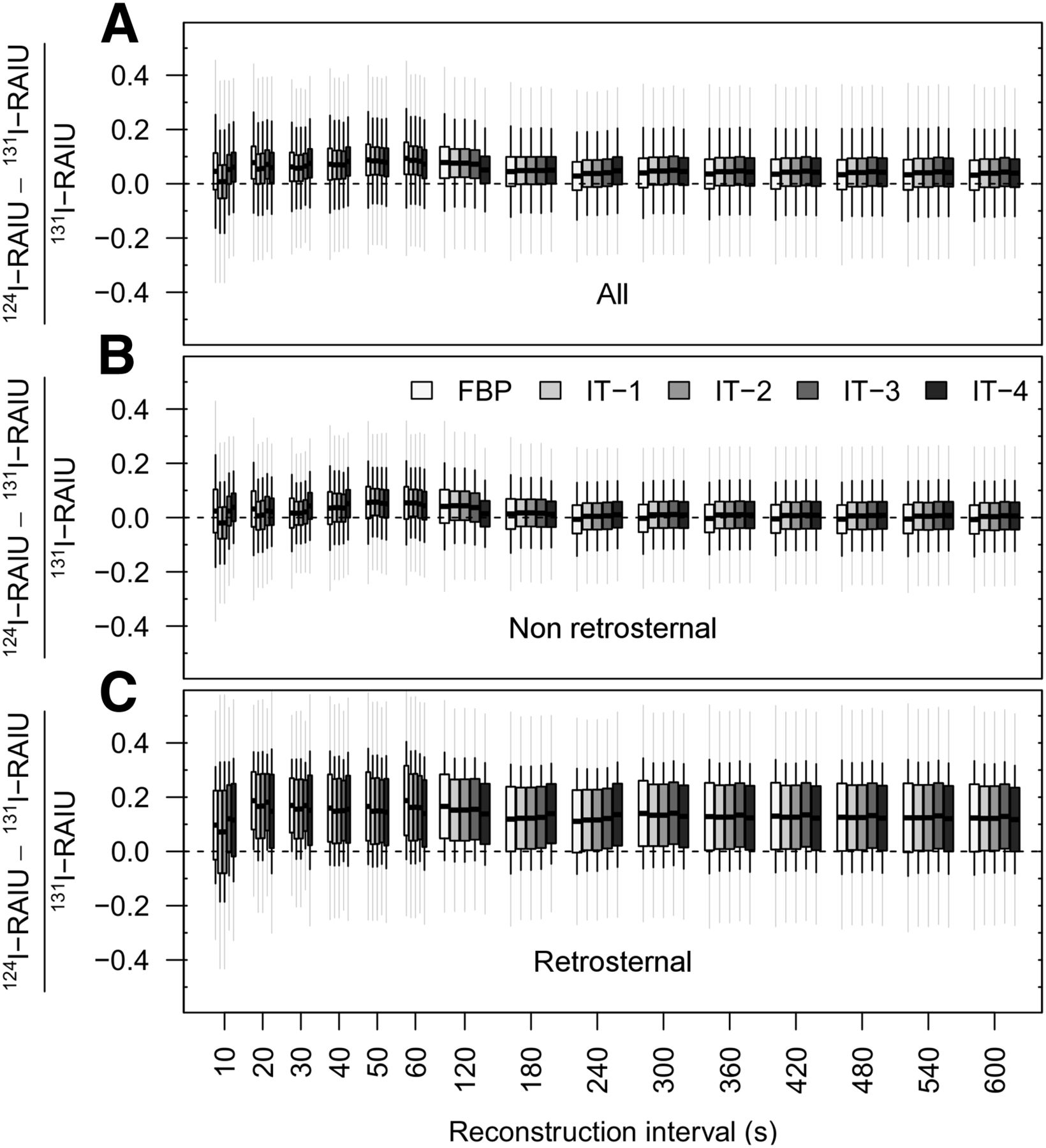
The impact of the length of RI (as a surrogate for the scanning duration) was assessed for the 5 124I PET reconstruction algorithms in terms of consistency with the 131I RAIU measurement (Fig. 2). A slightly modified version of the Bland–Altman method was applied to estimate the degree of consistency between the 131I RAIU and 124I RAIU determined by means of the 5 different reconstruction algorithms (11). In short, relative uptake differences were calculated between 124I RAIU and 131I RAIU. A subanalysis was performed splitting the patients into 2 subgroups, one without and the other with retrosternal thyroid tissue (Figs. 2B and 2C).

Modified Bland–Altman plots showing relative differences in uptake between 124I PET and 131I probe (clinical standard, line of equality at 0) for all patients (A) and for subgroups without (B) and with (C) retrosternal tissue, using 5 different 124I PET reconstruction algorithms at 15 RIs. Boxes and horizontal lines indicate mean and its 95% confidence interval. If box includes line of equality, there is no systematic over- or underestimation. Gray whiskers indicate 95% limits of agreement according to Bland–Altman (1.96-fold SD), whereas black whiskers indicate common SD.
Image Quality
Two image quality aspects were considered. First, visual inspection of the 124I PET/CT images was performed for the different RI and reconstruction algorithms but not routinely analyzed in terms of visual scoring, because visual assessment is subjective. Therefore, we decided to use a second, objective parameter.
It is generally accepted that high pixel noise contributes to low image quality (12). In our setting, reducing the RI leads to an increase in pixel noise and in turn a decrease in image quality. As an approach to objectify pixel noise, we measured the SD of the activity concentration within the VOI. Finally, SD and pixel noise were observed to increase in this study, corresponding with low image quality. This is exclusively influenced by length of RI and reconstruction algorithm. Since the experience in our institution shows that 1 MBq of 124I at a 600-s scan time provides sufficient images in all cases, it serves as a reference for image quality in this study (2,3). We tested a limit of 10% change in SD to obtain images with probable acceptable quality. The length of the RI at an SD increase of 10% or less was defined as the RI of acceptability (RIacc), and this corresponds to a hypothetical minimum activity (Fig. 3; Table 2). The image quality is proportional to the PET scanning time and the activity contained in the scan field of view. Doubling the activity of a PET radiopharmaceutical leads to halving the scanning time, and halving the activity contained in the scan volume requires doubling the scanning time, resulting in the same image quality (13). Accordingly, the determination of RIacc allows the calculation of a hypothetical minimum activity (Amin) by means of a proportion equation (Eq. 1): Therefore, in the presented setting of 600 s and 1 MBq of 124I, an RIacc of 300 s is equal to a hypothetical activity of 0.5 MBq of 124I.
Therefore, in the presented setting of 600 s and 1 MBq of 124I, an RIacc of 300 s is equal to a hypothetical activity of 0.5 MBq of 124I.

Difference between SD of 124I RAIU and SD of 124I RAIU at 600 s depending on length of RI and reconstruction algorithm. Each patient was plotted separately as single gray line. Image quality was considered acceptable if increase in SD of all scans remained ≤10%; length of RI at which this criterion was met was defined as RIacc.
RIacc and Calculated Hypothetical Minimum Activity for Different Reconstruction Algorithms
RESULTS
Patients
Of 97 patients screened, 56 fulfilled the inclusion criteria and 37 agreed to participate in the study (Table 3). Part of the data was reported in a previous study (2). All participants were fully examined according to protocol. The mean orally administered activities were 3.03 ± 0.13 MBq for 131I and 1.02 ± 0.03 MBq for 124I. The interval between administrations was 10.0 ± 3.1 d. On average, the 131I RAIU measurements took place at 30 h ± 2 min after oral administration of the tracer, and the 124I RAIU measurements took place at 30 h ± 5 min. The mean 131I RAIU measured after 30 h was 29.1% ± 9.8, and the mean 124I RAIU (IT-1; 600-s RI) measured after 30 h was 29.6% ± 9.1.
Patient Characteristics
Comparison of 131I RAIU and 124I RAIU
A comparison of 131I RAIU and 124I RAIU for all patients showed a trend toward overestimation by 124I PET/CT (Fig. 2A). Therefore, a subanalysis of patients without (Fig. 2B) and with (Fig. 2C) retrosternal tissue was performed. The nonretrosternal subgroup showed a good agreement between the 2 RAIU measurements. There was hardly any systematic variability irrespective of the RI and algorithm. The retrosternal subgroup displayed higher 124I RAIU levels for all reconstruction algorithms, revealing a systematic overestimation.
For 124I PET reconstruction algorithms in all patients (Fig. 2A) and in the non-retrosternal subgroup (Fig. 2B), the limits of agreement were fairly concordant; however, a slight enlargement was observed for the RI between 10 and 60 s. In general, the reconstruction data obtained with the FBP showed a more pronounced enlargement of the limits of agreement than did the data obtained by IT (Fig. 2).
Image Quality
Figure 3 shows an exponential increase in SD at shorter RIs. This increase was more pronounced for FBP than for IT. The RIacc was reached from 131 s to 456 s, and the calculated hypothetical minimum activity was reached from 0.22 MBq to 0.76 MBq (Fig. 3; Table 2). Image quality was still good at 300 s (Fig. 4A), but reducing the number of subsets (IT-4) as well as using FBP lowered image quality visually (Fig. 4B).
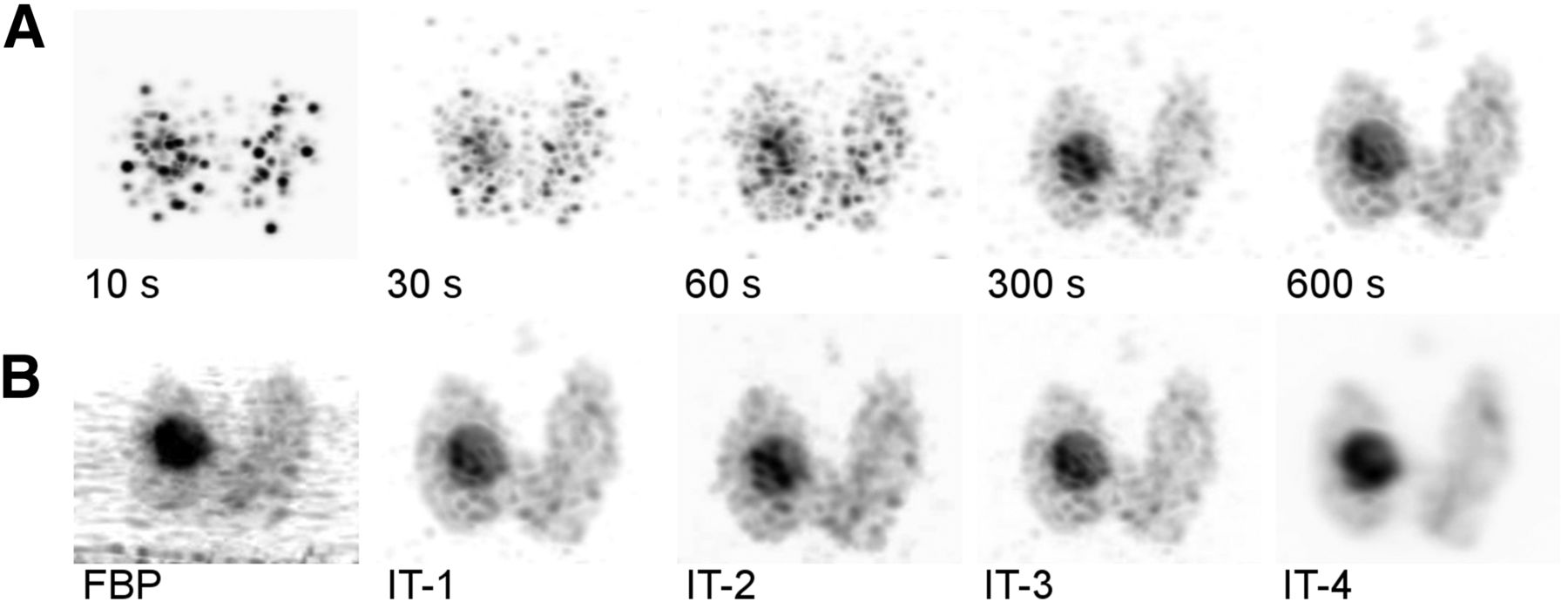
Maximum-intensity projection of 124I PET for patient with autonomous adenoma according to RI (A) and algorithm (B).
DISCUSSION
Different radioiodine isotopes are available for thyroid diagnostics. Hybrid imaging leads to additional benefits (connection between anatomic and functional imaging). 123I and 131I require a SPECT/CT scanner and 124I a PET/CT scanner. However, in many institutions only one of these two types of scanners is available. If it is not possible to use SPECT/CT, 124I PET/CT forms a suitable alternative.
As the thyroid RAIU is comparably specific and intense, 124I PET/CT images obtained with low activity are of good visual quality compared with 124I PET/CT performed in patients with metastasized differentiated thyroid cancer after thyroid removal or remnant ablation. Moreover, recent 124I RAIU measurement studies indicate that an activity of 1 MBq and a scan time of 600 s generate a visually sufficient image for diagnostics and allow reliable RAIU measurement (2,3). Concerning radiation exposure of 124I RAIU evaluation with 1 MBq, a thyroid uptake of 25% is associated with an effective whole-body equivalent dose of about 6.5 mSv considering that about 0.3 mSv is contributed by the low-dose CT and the thyroid organ dose is 260 mGy (8,14). In comparison, the effective whole-body equivalent dose resulting from 131I RAIU evaluation with 3 MBq is about 33 mSv, and the thyroid organ dose is 1,290 mGy (8,14). Therefore, radiation exposure caused by 124I RAIU measurement is approximately one fifth of that of 131I RAIU measurement. However, the radiation exposure aspect is somewhat relative concerning the following RAIT. Moreover, in the past, activities of as low as 0.2 MBq have been shown to be sufficient for 131I RAIU measurement (15). In the presented setting, standard activities of 3 MBq of 131I were used according to current guidelines (9,10). However, 124I activity reduction may be desirable for decreasing the inherent material costs. The present study sought to verify the effects of a hypothetical reduction of 124I activity on 124I RAIU and pixel noise, as well as the role of different reconstruction algorithms. The investigational use of different activities was not feasible because of the clear methodologic constraints caused by the additional exposure for individual participants; therefore, we chose an indirect methodologic approach determining hypothetical minimum activities.
Simulating different scan times with the help of list-mode data has already been used in studies aimed at assessing the optimal activity for pediatric 18F-FDG-PET; however, the reconstruction times were limited to 1–5 min (13). A phantom study with 18F-FDG examined the relationship between image quality and (simulated) acquisition times, but only at intervals of 1–4 min (16). The present study differed from those publications in that not only was 124I used but also a larger time span with more time intervals.
Comparison of 131I RAIU and 124I RAIU
Mean 124I RAIU and 131I RAIU were fairly concordant. Length of RI and reconstruction algorithms influenced neither the level of agreement nor the SD of the measured RAIU (Fig. 2). An RI of as short as 10 s (corresponding to an activity of 0.017 MBq of 124I; Eq. 1) did not show a difference between mean 124I RAIU and 131I RAIU. However, images of the 10-s RI are visually insufficient (Fig. 4A). Therefore, the difference between 124I RAIU and 131I RAIU cannot be used as a parameter to determine a reasonable lower limit for 124I activity.
The subgroup analysis separately investigating patients without and with retrosternal thyroid tissue proved that the slight trend toward higher 124I RAIU is caused by patients with retrosternal tissue only (Fig. 2). In fact, 131I RAIU measurement may be associated with some γ-absorption in the sternum and hence in underestimation of RAIU. In addition, 131I RAIU measurement may not completely include the whole retrosternal part because positioning is not image-guided, probably resulting again in underestimation of the RAIU. 124I RAIU measurement, in contrast, always identifies possible retrosternal portions and includes them in the RAIU measurement. The trend toward higher 124I RAIU was more pronounced at shorter RIs (10–60 s), leading to a slight statistical deviation. This finding is difficult to assess; a conceivable explanation lies in the IT calculation model.
Image Quality
The impact of the RI length on the increase in pixel noise was examined as a parameter of image quality, given that very short scanning times (simulated by short RIs) are associated with a higher background noise and poorer image quality (17–20). The concept of using an increase in SD as a parameter of image quality was chosen because an exact assessment of image quality with parameters such as spatial resolution, signal-to-noise ratio, or noise-equivalent counting rate was not applicable to the underlying in vivo data (21,22). These parameters can reliably be determined only by using a phantom with defined focal hot and cold spots of different sizes. A modified neck-shaped Jaszczak-phantom meeting the needs of the proposed study setting is currently being constructed in our clinic, and corresponding studies are planned.
During the last few years, we used 1 MBq of 124I for imaging of benign thyroid diseases in unclear situations with guideline-conforming thyroid diagnostics (2,3). Through these experiences, we know that activities of as low as 1 MBq produce high-quality PET/CT images that clearly depict thyroid metabolism and are sufficient for image fusion with ultrasound (23,24). Because a deviation of ±10% in terms of applied activity is usually accepted in nuclear medicine, we allowed a 10% increase in the SD of mean uptake with regard to the 600-s RI, which is the locally established reconstruction algorithm. An increase in SD was considered a surrogate parameter for pixel noise and, thus, representative of image quality. The length of the RI at which all patients show an SD increase of no more than 10% is 287 s for IT-1, and this corresponds to a hypothetical minimum activity of 0.48 MBq (Table 2). Thus, it can be concluded that activities of as low as 0.5 MBq might be sufficient for good-quality images.
Visual interpretation in terms of visual scoring was not a focus of the current study. However, it is important to look at these images because diagnostics rely on visual assessment. An example of the influence of different RI and reconstruction algorithms is shown for one patient in Figure 4. Given that 124I PET/CT can be used for PET/ultrasound fusion imaging, it is important to obtain a sufficiently high image quality (23,24). Images with an RI of 300 s still are appropriate to clearly define thyroid metabolism in the chosen example (Fig. 4A). Decreasing the RI length leads to a significant loss in image quality. As expected, it can be concluded that FBP is inferior to IT with regard to image quality, as has been extensively reported previously (25,26). Additionally, the reduction of equivalent iterations, that is, the product of iterations and subsets (IT-4), softens the image on the one hand but leads to increased blurring and therefore reduced image quality on the other hand (27–29). IT-1 to IT-3 do not differ with regard to image quality; therefore, we assume that zoom and matrix do not directly influence the image quality.
Limitations
The present study had some clear limitations. The number of patients was limited, and the benign thyroid diseases were of different types. Because this research was designed as an initial subanalysis within a larger study, results were valid only for a time point of 30 h after radioiodine administration. Kinetic information (i.e., information on effective half-life) that would be available in the case of multiple RAIU measurements was not obtained with the present data. Because a comparison with intratherapeutic measurements was not performed, conclusions on the superiority of 124I RAIU over 131I RAIU are not possible. Because the study focused on activity, the functional topography of hypo- or hyperfunctional areas was not systematically considered. These aspects are nonetheless important for the use of PET/CT or PET/ultrasound image fusion. Finally, a routine 124I RAIU measurement is hindered by several factors. The use of 124I PET/CT is complex and not ubiquitously available and, compared with a 131I probe, considerably more expensive regarding the length of the examination and the price of 124I, which in our institution is about 20% higher than the price of 131I. The use of very low activities might lower the cost (2).
CONCLUSION
The present study confirmed the potential of 124I PET/CT as an alternative method for RAIU measurement in patients with benign thyroid diseases, and this irrespective of additional benefits such as improved information on functional anatomy, reliable volumetry, and the possibility of performing image fusion with ultrasound. A hypothetical activity reduction to approximately 0.5 MBq of 124I obtained with the locally established reconstruction algorithm IT-1 appeared sufficient when considering pixel noise in parallel. Further studies with more time points, higher patient numbers, and clearly defined disease groups divided by uptake level are warranted, especially if validated by intratherapeutic measurements.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Dr. Ernesta Palombo-Kinne for help in reviewing and translating the manuscript, Dominik Driesch for analyzing the data, and Julian Westphal for providing support.
Footnotes
Published online Mar. 16, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 16, 2015.
- Accepted for publication February 21, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.