


Abstract
Myocardial perfusion imaging (MPI) with SPECT is a well-established tool for the diagnosis of coronary artery disease (CAD). However, soft-tissue attenuation is a common artifact that limits the diagnostic accuracy of MPI. The aim of this study was to determine whether attenuation correction (AC) improved the diagnostic performance of MPI, using coronary angiography as a reference standard. Methods: MEDLINE and EMBASE were searched until March 2015 for studies evaluating AC MPI for the diagnosis of CAD. Methodologic quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies tool. For each study, the sensitivity, specificity, and diagnostic odds ratio, along with 95% confidence intervals (CIs), were calculated to determine the diagnostic accuracy of AC versus non–attenuation-corrected (NAC) MPI. A bivariate mixed-effects model was applied for pooling the data. Results: Of 201 articles, 17 studies (1,701 patients) were identified, including 5 studies that used CT AC, 12 studies that used radionuclide source AC (RAC), and 15 studies that reported NAC results. The pooled sensitivities across studies were 0.80 (95% CI, 0.64–0.91), 0.85 (95% CI, 0.81–0.88), 0.84 (95% CI, 0.79–0.88), and 0.80 (95% CI, 0.75–0.85) for CT AC, RAC, all AC, and NAC, respectively. The pooled specificities were 0.83 (95% CI, 0.71–0.91), 0.81 (95% CI, 0.73–0.86), 0.80 (95% CI, 0.74–0.85), and 0.68 (95% CI, 0.61–0.74). Both sensitivities and specificities resulted in a pooled diagnostic odds ratio of 20 (95% CI, 12–34), 24 (95% CI, 13–43), 22 (95% CI, 13–35), and 9 (7–11). Significant differences in specificity and diagnostic odds ratios were noted when AC (including CT AC, RAC, and all AC) was compared with NAC. Conclusion: The results from this study suggested that AC should be applied to MPI to improve the diagnosis of CAD, especially the specificity.
- attenuation correction
- myocardial perfusion imaging
- single-photon emission tomography
- coronary artery disease
- meta-analysis
Coronary artery disease (CAD) is one of the major causes of morbidity and mortality throughout the world (1–3). To select those patients who will receive the greatest benefit from revascularization, accurate diagnosis and risk stratification of CAD, using noninvasive testing, is crucial (4). Myocardial perfusion imaging (MPI) with SPECT is a well-established tool for the diagnosis of CAD. Because it has good prognostic and net risk classification value, MPI is usually used as the gatekeeper for invasive coronary angiography (CAG) and evaluation of therapy effectiveness (5). However, artifacts degrade image quality and increase the risk of misinterpretation, and soft-tissue attenuation is one of the most common artifacts (6). An external radionuclide source has been used for attenuation correction (AC), which improved sensitivity and specificity from around 70% to above 80% (7–10). But routine AC plus image reconstruction is time-consuming. The development of hybrid SPECT/CT involves the use of CT for AC by converting Hounsfield units into attenuation coefficients (11,12). CT AC using hybrid SPECT/CT has significantly reduced scan time; however, registration errors between CT and SPECT images and radiation dose are still concerns (11).
Most MPI studies were heterogeneous with small sample size. Several meta-analyses evaluated the diagnostic performance of SPECT MPI (13–16) but did not focus on the specific role of AC in the diagnosis of CAD. Therefore, the aim of this study was to compare the diagnostic performance of AC with non–attenuation-corrected (NAC) MPI, using CAG as the reference standard. In addition, subgroup analyses (considering radionuclide source AC [RAC] vs. CT AC) were performed.
MATERIALS AND METHODS
Search Strategy
MEDLINE and EMBASE were searched for English-language literature published until March 2015. Key words included myocardial perfusion, SPECT, and AC. Conference articles were excluded because most conference articles lacked precise data (i.e., true-positive, false-positive, false-negative, and true-negative). Medical subject headings terms were used to maximize the sensitivity of the search.
Study Selection
Article titles and abstracts were reviewed for eligibility. A study was included if it met the following criteria: it assessed attenuation-corrected MPI as a diagnostic tool to evaluate patients for the presence of CAD; CAD was defined as at least 50% diameter or more stenosis on CAG; CAG was used as the reference test; and absolute numbers of true-positive, false-positive, true-negative, and false-negative were available or these data were derivable from the results presented. A study was excluded if it was a conference article, was a review or meta-analysis, was a study of risk stratification, used a reference test other than CAG, was a technology or image quality studiy, or was without diagnostic performance at the patient level.
Data Extraction
Two researchers independently performed data extraction. Extracted information included author, journal, year of publication, and country; details of study design; patient demographic features (such as numbers of patients, mean age, percentage of males, and indication for MPI); imaging technique (such as type of AC, type of perfusion radiotracer, stress type); imaging protocol (scatter correction, gated); brand of imaging device and interpretation method; CAD definition; and numbers of true-positive, false-positive, true-negative, and false-negative. Data were recorded at the patient level. If a study reported more than 1 pair of sensitivities and specificities at different cutoff points, different imaging techniques, different CAD definitions, or different experienced observers, the pair reported in the abstract (17) and the pair with the highest sensitivity (9,17–19) were extracted. One study (20) reported pairs of sensitivity and specificity by 3 independent operators with 4, 7, and 11 y of experience, respectively, and data from the most experienced physician were used in our analysis. Disagreement between the 2 researchers was resolved by consensus.
Quality Assessment
Methodologic quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS; scale, 0–14) tool (21). In brief, the assessment was based on 14 items, including covered patient spectrum, reference standard, disease progression bias, verification bias, review bias, clinical review bias, incorporation bias, test execution, study withdrawals, and indeterminate results. A score of 7 of 14 is high quality, and scores below 7 are low quality. The QUADAS tool is an evidence-based quality assessment tool to be used in systematic reviews of diagnostic accuracy studies.
Statistical Analysis
All data from each eligible study were extracted and sorted out by Cochrane’s Review Manager (version 5.3). Categoric variables were expressed as percentages, and continuous variables were expressed as mean values. On the basis of the extracted 2 × 2 contingency tables, pooled measures for diagnostic performance, including sensitivity, specificity, diagnostic odds ratio (ORs), summary receiver-operating-characteristic (ROC) curve, and area under the curve (AUC) with 95% confidence intervals (CIs), were calculated. Between-study statistical heterogeneity was assessed using I2 and the Cochrane Q test on the basis of the mixed-effects analysis (22). Publication bias was examined using the effective sample size funnel plot and associated regression test of asymmetry described by Deeks et al. (23), with a P value of less than 0.10 for the slope coefficient indicating significant asymmetry. The data were analyzed at the patient level using a bivariate mixed-effects regression model (24–26) to express the diagnostic performance measures across studies and comparisons between different index tests (25,27).
The assumption of the bivariate model is that the sensitivities from individual studies (after logit transformation) within a meta-analysis are approximately normally distributed around a mean value, with a certain amount of variability around this mean. The same is true for the specificities of these studies, leading to the bivariate normal distribution. These bivariate models can be analyzed using linear mixed-model techniques. The parameters of the bivariate model are estimated in a single model to incorporate the possible correlation between sensitivities and specificities (25). The summary ROC curves were also created using this model to estimate the AUC (28). Statistical analysis was performed using STATA (version 13; StataCorp LP) and SAS (version 9.4; SAS Institute Inc.).
RESULTS
Study Characteristics
A total of 441 articles were retrieved through the database from MEDLINE and EMBASE (Fig. 1). After conference articles, non-English articles, and those articles without abstracts were excluded, 201 articles remained. On the basis of title and abstract, an additional 158 articles were excluded. After full text review, 27 additional articles were excluded, and 1 study (17) was included after manual check from cited reference lists as shown in Figure 1, the flowchart of study selection.
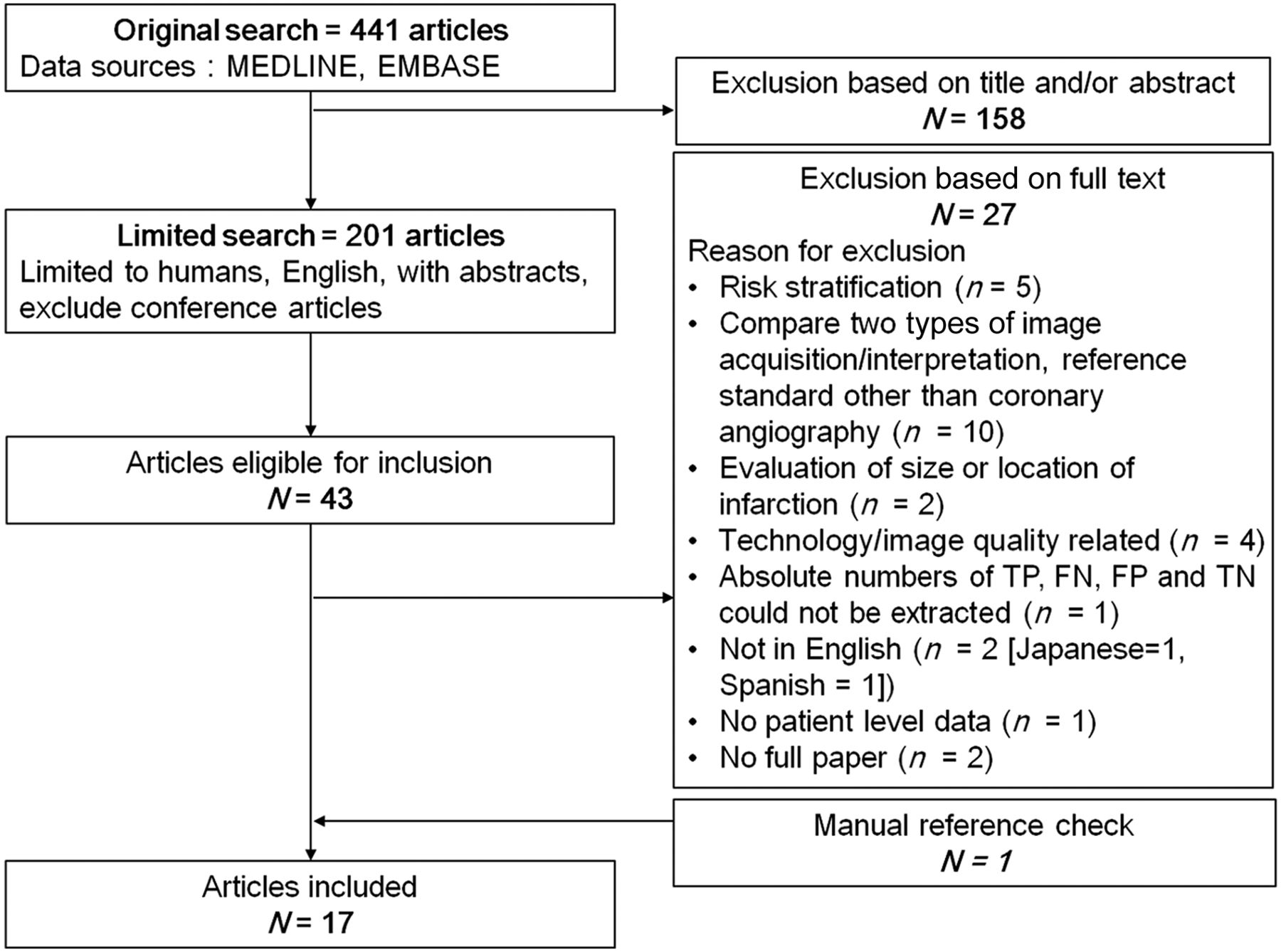
Flowchart of study selection. Limited search of MEDLINE and EMBASE yielded 201 articles. After exclusion, a total of 17 studies (1,701 patients) were included in final analysis. FN = false-negative; FP = false-positive; TN = true-negative; TP = true-positive.
The final analysis comprised 17 studies, with a total of 1,701 patients, including 5 studies (with 522 patients) that used CT AC, 12 studies (with 1,179 patients) that used RAC, and 15 studies (with 1,543 patients) that reported NAC results. A review of each study’s characteristics revealed many differences between the included studies (Table 1) (7–10,17–20,29–37), which could potentially affect the diagnostic performance of MPI.
Characteristics of Selected Studies
The methodologic quality of the 17 studies was assessed using the QUADAS tool. Review of the QUADAS checklist for all studies showed that most studies (16/17) were scored above 7, which is considered good quality (21). Only 1 study showed poor quality, with a QUADAS score of 3 (31). During QUADAS assessment, most studies were found to have problems with unclear masking during interpretation of the reference test; masked reading of the index test; lack of reporting for uninterpretable results; and lack of explanation of withdrawals, which may have resulted in bias.
The I2 index showed substantial heterogeneity with regards to sensitivity and specificity for all index tests. The highest was 92.3% for CT AC and the lowest was 59.2% for RAC when measuring sensitivity. The funnel plot and regression tests showed a statistically nonsignificant P value (0.51) for the slope coefficient, indicating symmetry in the data and a low likelihood of publication bias (23).
Diagnostic Performance
The pooled sensitivities across studies were 0.80 (95% CI, 0.64–0.91), 0.85 (95% CI, 0.81–0.88), 0.84 (95% CI, 0.79–0.88), and 0.80 (95% CI, 0.75–0.85) for CT AC, RAC, all AC (CT AC plus RAC), and NAC, respectively. The pooled specificities across studies were 0.83 (95% CI, 0.71–0.91), 0.81 (95% CI, 0.73–0.86), 0.80 (95% CI, 0.74–0.85), and 0.68 (95% CI, 0.61–0.74) for CT AC, RAC, all AC, and NAC, respectively. The pooled diagnostic ORs were 20 (95% CI, 12–34), 24 (95% CI, 13–43), 22 (95% CI, 13–35), and 9 (95% CI, 7–11) for CT AC, RAC, all AC, and NAC, which were regarded minimally affected by verification bias (15). The pooled diagnostic accuracies across studies were 0.79 (95% CI, 0.71–0.87), 0.84 (95% CI, 0.80–0.87), 0.82 (95% CI, 0.78–0.86), and 0.75 (95% CI, 0.73–0.78) for CT AC, RAC, all AC, and NAC, respectively. The pooled results are shown in Table 2. The summary ROC curves are shown in Figure 2. For CT AC, RAC, all AC, and NAC tests, the AUCs were 0.89 (95% CI, 0.86–0.91), 0.90 (95% CI, 0.87–0.92), 0.89 (95% CI, 0.86–0.92), and 0.81 (95% CI, 0.77–0.84), respectively.
Diagnostic Performance of MPI for Detection of CAD, Pooled Sensitivity, Specificity, and Diagnostic OR of CT AC, RAC, All AC, and NAC
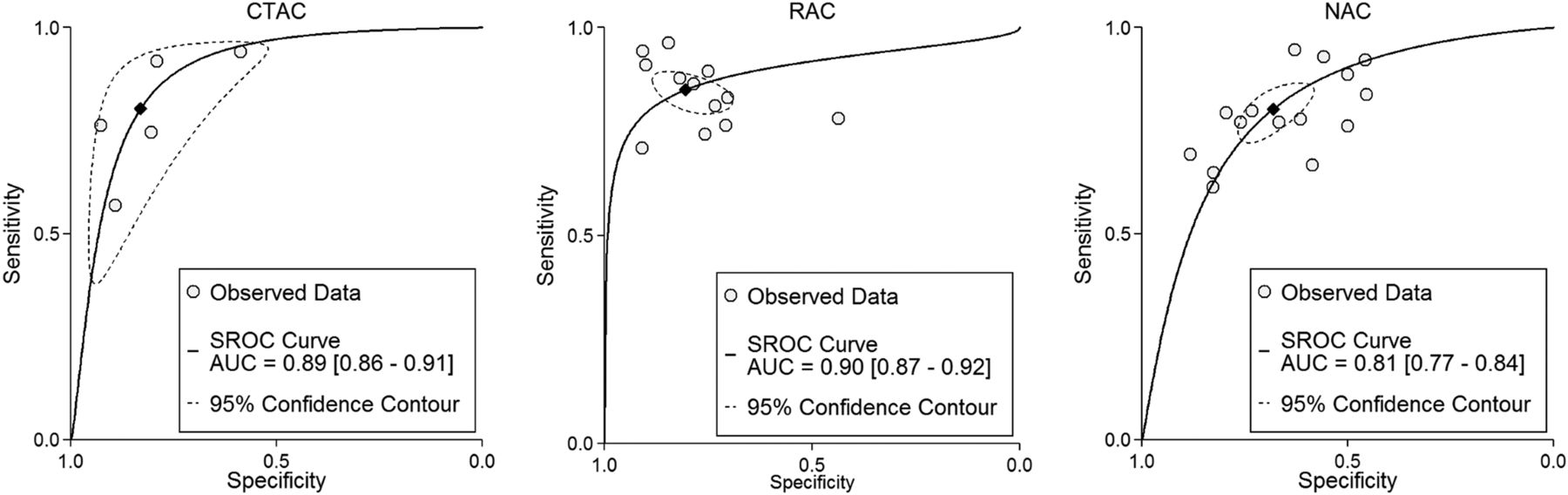
ROC curve for diagnosis of CAD using CT AC, RAC, or NAC. Each circle represents individual included study. Diamond represents summary operating point of pooled sensitivity and specificity. Dashed line represents 95% CIs. SROC = summary ROC.
There was no significant difference in sensitivity between 1-by-1 comparison among the 4 kinds of studies when the diagnostic performance of CT AC, RAC, all AC, and NAC was compared. There was no significant difference in specificity between CT AC and RAC (P = 0.60). There was a significant difference in specificity in all AC versus NAC (P = 0.008), as well as in the subgroup analysis for CT AC versus NAC (P = 0.028) and RAC versus NAC (P = 0.031). There were also significant differences in diagnostic ORs between all AC and NAC (P = 0.002), CT AC and NAC (P = 0.048), and RAC and NAC (P = 0.004).
Eight (2 CT AC and 6 RAC studies, all reported NAC data (9,10,17–19,31,35,36)) of the included studies provided information of normalcy. Considering these 8 studies, the pooled normalcies across studies were 0.95 (95% CI, 0.91–1.00), 0.95 (95% CI, 0.91–0.98), 0.95 (95% CI, 0.92–0.97), and 0.84 (95% CI, 0.78–0.90) for CT AC, RAC, all AC, and NAC, respectively.
DISCUSSION
This study showed no significant difference in sensitivity between CT AC, RAC, all AC, and NAC images but a significant difference in the specificity between all AC and NAC as well as in the subgroup analysis for CT AC versus NAC and RAC versus NAC, without compromising the sensitivity. Regarding the diagnostic OR, a significant difference between AC (CT AC, RAC, and all AC) and NAC was also noted.
Several meta-analyses had compared the diagnostic performance of SPECT/MPI and other modalities including echocardiography, cardiac CT, cardiac MR, and PET (13–16) in diagnosing CAD. These studies revealed a sensitivity of 0.88, 0.88, 0.83, and 0.74 and a specificity of 0.73, 0.61, 0.77, and 0.79, respectively, only for MPI (13–16). Jaarsma et al. performed subgroup analyses comparing AC and NAC, but only 5 studies concerned the diagnostic performance of AC MPI, whereas 100 studies concerned the diagnostic performance of NAC MPI, without overlapping studies. Their meta-analysis showed an increased specificity (0.60 vs. 0.78) but decreased sensitivity (0.89 vs. 0.80) of AC MPI versus NAC MPI. The overall diagnostic performance was compared using diagnostic OR and showed no difference between NC and AC (NC vs. AC, 15 vs. 13, P = 0.51) (14). However, in the current study, AC showed increased specificity without decreasing the sensitivity. This discrepancy in results may be due to the type of studies selected. In our meta-analysis, studies that compared the 2 imaging techniques within the same participants (i.e., 15 studies had NAC and AC results from the same subjects) were primarily used, whereas the AC and NAC results evaluated in the study by Jaarsma et al. were from different studies.
de Jong et al. selected studies published after 2000 that were more homogeneous, with inclusion of prospective studies with CAG as a reference test (irrespective of index test result). The detailed imaging protocols (such as AC or NAC), however, were not mentioned in their data extraction. They showed similar results in sensitivity (0.83) but higher specificity (0.77) compared with the NAC results from this current meta-analysis. The discrepancy could be partly explained by verification bias in the current study, which may have inflated the sensitivity and deflated the specificity (15,38). On the other hand, Takx et al. included 4 AC and 6 NAC studies and showed lower sensitivity (0.74) than but specificity (0.79) similar to the current study’s AC result (16). However, Takx et al. used a combination of luminal stenosis on CAG and fractional flow reserve as the diagnostic standard for CAD. In the current study, although the diagnostic sensitivity of CT AC and RAC (when compared with NAC) both failed to reach significance, CT AC and RAC both showed significant improvement in specificity when compared with NAC. No scatter correction was performed in all 5 CT AC studies whereas it was performed in RAC studies. In addition, the CT was used only for reconstructing attenuation maps and AC in these CT AC studies. We propose that if scatter correction (39) and anatomic information such as coronary calcium or angiography from CT (40,41) could be applied, the diagnostic performance may show even greater improvement.
Considerable heterogeneity was noted among the enrolled studies, including variations in the study population, scanning and processing protocols, different radionuclide tracers used, different stress modes, and different angiographic criteria for CAD. Underwood et al. had also evaluated the diagnostic performance of MPI using different tracers and types of stress protocols and found a sensitivity ranging from 0.64 to 1.00 and a specificity ranging from 0.33 to 1.00. Although their ranges were wide, no statistical difference between these various protocols was noted (42).
Significantly higher specificity and diagnostic ORs were found in both CT AC and RAC subgroup analyses in our study. When considering radiation, dose from radionuclide transmission sources is less than from SPECT/CT (11). However, a lower radiation dose from SPECT/CT has been achieved by reducing x-ray tube current and incorporating new reconstruction methods and new protocols (39,43,44). Also RAC is time consuming. SPECT/CT with faster scanning and reconstruction time makes CT AC more clinically practical.
The random-effects model of Der Simonian and Laird (45,46) was used to incorporate heterogeneity into the overall estimates. Because these conventional methods might introduce bias in meta-analyses of binary outcomes, such as sensitivity and specificity (47,48), and the normality assumption of estimates and its variance might not hold when dealing with few studies or sparse data (47,49), the current study used bivariate mixed effects for more reliable estimates of parameters.
To our knowledge, this is the first meta-analysis that focused on different imaging techniques (AC vs. NAC) in MPI. Fifteen studies with 1,543 patients evaluated both AC and NAC results in the same participants, because a precise comparison between different index tests requires the same original individual patient-level data. This is also the first study to perform pooled sensitivity and specificity of AC MPI to support their clinical usefulness. No publication bias was identified among the selected studies; therefore, the results can be considered robust.
This study had several limitations. Quantitative analyses of SPECT were not routinely used in the selected papers. Bias existed in the visual assessment, especially in those studies that used an unmasked method. In addition, gated SPECT or other nonperfusion parameters (such as lung uptake, right ventricular activity, or transient left ventricle dilatation after stress) were not routinely included for interpretation, which may have decreased the diagnostic accuracy of the study, especially in cases of multivessel disease. Verification bias may exist because results of MPI may have affected the clinical decision to use CAG. Only 1 study performed coronary angiography, irrespective of MPI results (35). The difference between the AUCs of AC and NAC could not be calculated because of limited information regarding relationships between AC and NAC in patients with CAD or not. Finally, using CAG as a reference may have underdiagnosed the presence of microvascular CAD.
CONCLUSION
Our study results suggested AC should be applied to MPI because it affects diagnostic certainty in CAD with significant improvement of the specificity.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported, in part, by the Ministry of Science and Technology of Taiwan (MOST101-2314-B-418-012-MY3). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Jul. 21, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 22, 2015.
- Accepted for publication June 27, 2016.





{kind=link}
{kind=link}