


Abstract
Early diagnosis of infective endocarditis (IE) is based on the yielding of blood cultures and echocardiographic findings. However, they have limitations and sometimes the diagnosis is inconclusive, particularly in patients with prosthetic valves (PVs) and implantable cardiac electronic devices (ICEDs). The primary aim of this study was to evaluate the diagnostic accuracy of 18F-FDG PET/CT in patients with suspected IE and ICED infection. Methods: A prospective study with 80 consecutive patients with suspected IE and ICED infection (65 men and 15 women with a mean age of 68 ± 13 y) between June 2013 and May 2015 was performed in our hospital. The inclusion criteria were clinically suspected IE and ICED infection at the following locations: native valve (NV) (n = 21), PV (n = 29), or ICED (n = 30) (automatic implantable defibrillator [n = 11] or pacemaker [n = 19]). Whole-body 18F-FDG PET/CT with a myocardial uptake suppression protocol with unfractionated heparin was performed in all patients. The final diagnosis of infection was established by the IE Study Group according to the clinical, echocardiographic, and microbiologic findings. Results: A final diagnosis of infection was confirmed in 31 patients: NV (n = 6), PV (n = 12), and ICED (n = 13). Sensitivity, specificity, positive predictive value, and negative predictive value for 18F-FDG PET/CT were 82%, 96%, 94%, and 87%, respectively. 18F-FDG PET/CT was false-negative in all cases with infected NV. 18F-FDG PET/CT was able to reclassify 63 of 70 (90%) patients initially classified as possible IE by modified Duke criteria. In 18 of 70 cases, 18F-FDG PET/CT changed possible to definite IE (26%) and in 45 of 70 cases changed possible to rejected IE (64%). Additionally, 18F-FDG PET/CT identified 8 cases of septic embolism and 3 of colorectal cancer in patients with a final diagnosis of IE. Conclusion: 18F-FDG PET/CT proved to be a useful diagnostic tool in suspected IE and ICED infection and should be included in the diagnostic algorithm for early diagnosis. 18F-FDG PET/CT is not useful in the diagnosis of IE in NV but should be also considered in the initial assessment of this complex scenario to rule out extracardiac complications and possible neoplasms.
- infective endocarditis
- implantable cardiac electronic devices
- prosthetic valve
- 18F-FDG-PET/CT
- septic embolisms
Infective endocarditis (IE) entails a high risk of mortality and severe complications (1). Moreover, early diagnosis and detection of possible complications of IE remain a challenge in clinical practice (2). To improve outcomes, the diagnosis and management of IE should be shared by well-coordinated diverse specialists working together as a multidisciplinary team (3). Blood cultures and echocardiographic findings are still the cornerstone in the suspicion and initial diagnosis of IE, which will be confirmed or rejected according to modified Duke criteria (4). However, the diagnostic yielding of current criteria is not optimal, with a large percentage of cases remaining as possible IE at the end of the episode (5). This is partially due to difficulties in the interpretation of echocardiographic findings in patients with intracardiac devices such as prosthetic valves (PVs) and implantable cardiac electronic devices (ICEDs) (6).
Early detection and drainage, if required, of embolic complications as well as enlarging the length of antibiotic therapy are crucial for improving immediate and late outcomes of IE, including relapses (7,8). Additionally, some microorganisms frequently causing IE such as bovis group streptococci are linked to underlying neoplasms (9). The detection of a neoplasm in the context of IE might significantly affect other therapeutic decisions and their timing, such as the parameters of cardiac surgery. Therefore, prospects in the approach of IE rely on available and easy-to-perform tests that provide data on different issues promptly, so that early measures could be applied.
18F-FDG PET/CT is an emerging image technique that has proven useful in the diagnosis of a variety of infectious diseases (10,11). Its utility is due to the ability of 18F-FDG to actively incorporate into activated leukocytes, macrophages, and CD4-positive T cells present at the sites of infection (12,13). Recent studies have reported encouraging results for 18F-FDG PET/CT in the diagnosis of IE and ICED infection (14–16) as well as in the detection of extracardiac complications (17,18). In the most recent guidelines (2015) of the European Society of Cardiology, 18F-FDG PET/CT has been included as a major criterion of PV endocarditis (PVE) diagnosis and also in the diagnostic algorithm for the detection of embolic events for both native valve IE (NVE) and PVE (7).
The primary aim of this study was to evaluate the diagnostic accuracy of 18F-FDG PET/CT in patients with suspected NVE, PVE, ICED IE, and other ICED-associated infections. The secondary aims were to evaluate the interobserver agreement and the added value of quantification using SUV in the diagnosis of infection.
MATERIALS AND METHODS
Patients and Design
Retrospective analysis of prospectively collected data from 80 consecutive patients (65 men and 15 women with a mean age of 68 ± 13 y) with suspected IE and ICED infection who were seen in our hospital from June 2013 to May 2015 was performed. Since 1979, all patients with IE attended at the Hospital Clinic of Barcelona have been managed by a multidisciplinary group that met for weekly meetings (19). We included patients with a clear suggestion of native or PV IE and ICED IE or infection, at least accomplishing Duke modified criteria to be initially considered as possible cases. After the diagnostic process, including 18F-FDG PET/CT and other tests, cases were classified according to modified Duke criteria (4) as rejected, definite, or possible. In the case of ICED, and due to the common management in all cases (removal of the device), we used the definitions provided by the last British Society for Antimicrobial Chemotherapy guidelines (20) for those cases not presenting vegetations (i.e., pocket infection and ICED lead infection). The final diagnosis of infection was established by the multidisciplinary working group according to the clinical, echocardiographic, and microbiologic findings. 18F-FDG PET/CT results were communicated to referring clinicians shortly after the test was done. Thus, 18F-FDG PET/CT was used as a diagnostic tool also, being a major criterion in the case of PVE, as recognized by the last European Society of Cardiology guidelines (7). In the case of ICED, 18F-FDG PET/CT was used in the cases in which the suspicion was high but none of the classic findings of ICED-associated infection was present (local inflammation of the generator pocket, bacteremia, or vegetations). Definitions of variables related to IE were collected in the clinical sheet of all patients. The following suspected episodes were included NVE (n = 21), PVE (n = 29), and ICED IE or ICED infection (n = 30) (automatic implantable defibrillator [n = 11] or pacemaker [n = 19]). All the patients were under antibiotic therapy. The baseline characteristics of the patients are shown in Table 1. The exclusion criteria included severe hemodynamic instability and indications for emergent surgery. All patients surviving the initial admission had at least a follow-up of 6 mo.
Baseline Characteristics of Study Group Patients
The institutional review board approved this study, and all subjects signed a written informed consent form.
PET/CT
Whole-body scans were obtained using a hybrid PET/CT scanner (Biograph mCT 64S; Siemens). A myocardial uptake suppression protocol was followed with a fasting period for at least 12 h and intravenous administration of 50 IU/kg of unfractionated heparin 15 min before the injection of 18F-FDG (4.0 MBq/kg). Blood glucose levels were required to be less than 150 mg/dL during a period of approximately 60 min before the administration of the 18F-FDG; during acquisitions, patients were supine with their arms raised above the head. Whole-body PET data were acquired in 3-dimensional mode and for 3 min per bed position.
Image Interpretation
Images were interpreted separately by 2 independent observers (2 nuclear medicine specialists trained on infection and 18F-FDG PET/CT who were masked to the clinical results). Disagreements were settled by consensus with a third nuclear medicine specialist. The criteria for infection were visual and considered positive when focal or heterogeneous increase in 18F-FDG activity related to the PV, NV, or ICED was identified in the attenuation-corrected and -uncorrected images. A semiquantitative analysis was made using the SUVmax in the area of suspected infection. The SUVmean was obtained in the blood pool (superior cava vein) and in the liver to establish SUV ratios. The SUV ratio was calculated by dividing the SUVmax of the area of interest by the blood-pool SUVmean (SUVmax ratio 1) and the liver SUVmean (SUVmax ratio 2).
Myocardial uptake suppression was classified in 3 categories as complete inhibition uptake (less or equal to liver uptake), partial inhibition (focally above to liver), and noninhibition (diffusely superior to liver uptake). Receiver-operating-characteristic curves with 2 different thresholds regarding total optimization and sensitivity optimization for SUVmax and SUVmax ratios have been obtained.
Statistical Analysis
The analyses were performed using SPSS (version 22.0; SPSS Inc.). Sensitivity, specificity, positive predictive value, and negative predictive value were calculated. Interagreement κ was obtained. Receiver-operating-characteristic curves and total and sensitivity optimization thresholds were calculated. P values of less than 0.05 were considered statistically significant. A Mann–Whitney U test for continuous variables and a Fisher exact test for nominal variables were used to assess differences between groups with P values of less than 0.05 considered statistically significant.
RESULTS
A final diagnosis of infection was established in 31 patients: NVE (n = 6), PVE (n = 12) (biologic valve [n = 5] or mechanical valve [n = 7]), ICED IE (n = 8), and ICED pocket or lead infection (n = 5) (automatic implantable defibrillator [n = 5] or pacemaker [n = 8]) (Figs. 1 and 2A). Forty-seven patients were rejected, and 2 patients remained as possible. In 28 of 31 episodes, causative microbial agents were identified, with Staphylococcus aureus (n = 8) and coagulase-negative staphylococci (n = 6) the most frequently isolated (Table 2). Sensitivity, specificity, positive predictive value, and negative predictive value for 18F-FDG PET/CT were 82%, 96%, 94%, and 87%, respectively. When suspected NVE was excluded from the analysis, these values changed to 96%, 94%, 93%, and 97%, respectively.

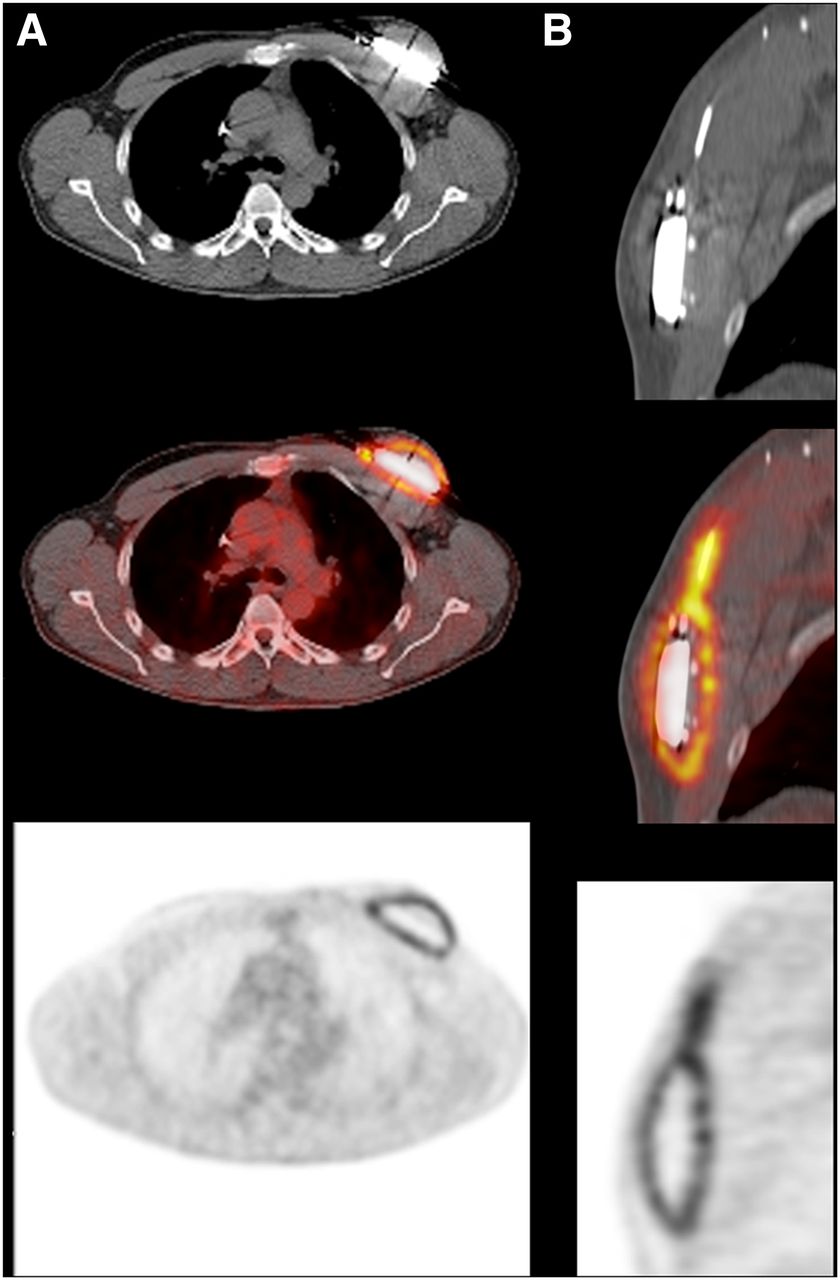
Pocket generator and lead infection in patient with automatic implantable defibrillator. Transverse (A) and sagittal (B) 18F-FDG PET/CT images. Device was removed. Both generator and lead cultures were positive for Staphylococcus aureus.

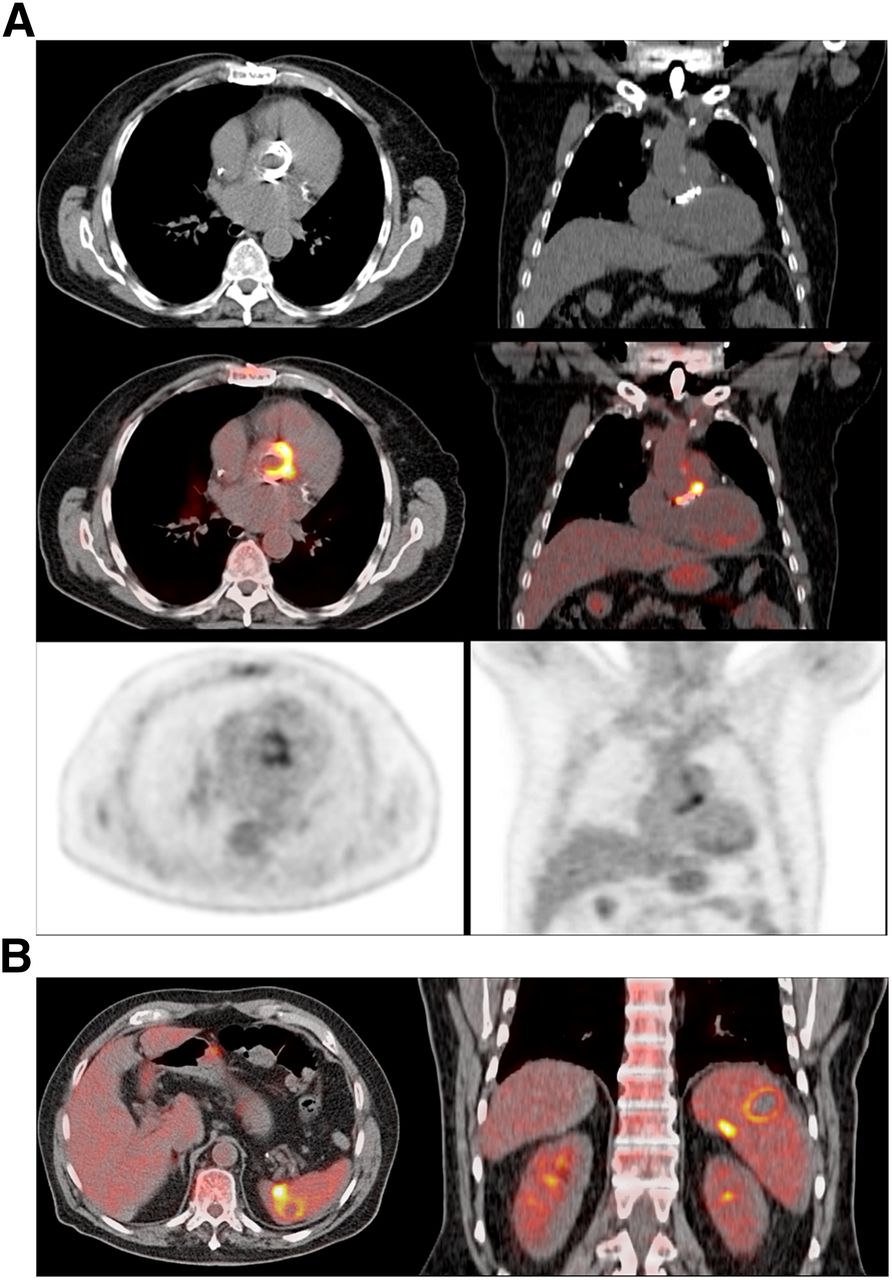
(A) Transverse and coronal 18F-FDG PET/CT images show infected prosthetic aortic valve. Culture after valve removal was positive for Propionibacterium acnes. (B) Fusion PET/CT images also demonstrate septic spleen embolisms.
Main Outcomes in Group of Patients with Final Diagnosis of IE and ICED Infection
In our series, 18F-FDG PET/CT was able to reclassify 63 of 70 cases (90%) initially classified as possible IE by modified Duke criteria. In 18 of 70 cases, 18F-FDG PET/CT changed possible to definite IE (26%) and in 45 of 70 cases changed possible to rejected IE (64%) (Table 3). Additionally, 18F-FDG PET/CT identified 8 cases of septic embolism (26%) in patients with a final diagnosis of IE (pulmonary, splenic, and vertebral in 4, 2, and 2 cases, respectively) (Fig. 2B) and 3 cases of colorectal cancer in patients with IE caused by Streptococcus bovis (n = 2) and Enterococcus faecalis (n = 1).
Classification According to Initial Diagnosis Criteria, 18F-FDG PET/CT Results, and Final Diagnosis Criteria
Among those patients with suspected IE or ICED infection whose diagnosis was eventually rejected, 18F-FDG PET/CT findings were pneumonia (n = 4), hip septic arthritis (n = 2), spondylodiskitis (n = 2), sternal osteomyelitis (n = 1), vascular aortic graft infection (n = 1), and lymphoma (n = 1). Interestingly, 18F-FDG PET/CT detected the source of infection in 7 of 15 patients (47%) with NV and rejected IE as a final diagnosis.
18F-FDG PET/CT retrieved 7 false-negative results in patients with definite IE, including all 6 cases with NVE and 1 case of PVE. There were no significant differences on the length of antibiotic therapy before 18F-FDG PET/CT performance between false-negative and true-positive results (P = 0.87). On the contrary, there were 2 18F-FDG PET/CT false-positive cases with suggestion of early PVE (1 and 8 mo after cardiac surgery, respectively).
The most valuable semiquantitative score to diagnose infection was SUVmax (Table 4). However, we did not find any significant improvement using semiquantitative scores in terms of sensitivity and specificity compared with visual analysis. Myocardial uptake inhibition was achieved in 75% of the patients (49 complete and 11 partial). Additionally, mean SUVmax in the group of patients with a complete inhibition of the myocardium and in the noninhibited group were 3.7 ± 1.3 and 12.3 ± 6.1 (P < 0.01), respectively (Fig. 3). The mean SUVmax in partially inhibited patients was 5.9 ± 1.4 (P = not significant).
Optimization of SUVmax and SUVmax Ratios Through Receiver-Operating-Characteristic Curves to Establish Most Appropriate Threshold to Diagnose IE/ICED Infection

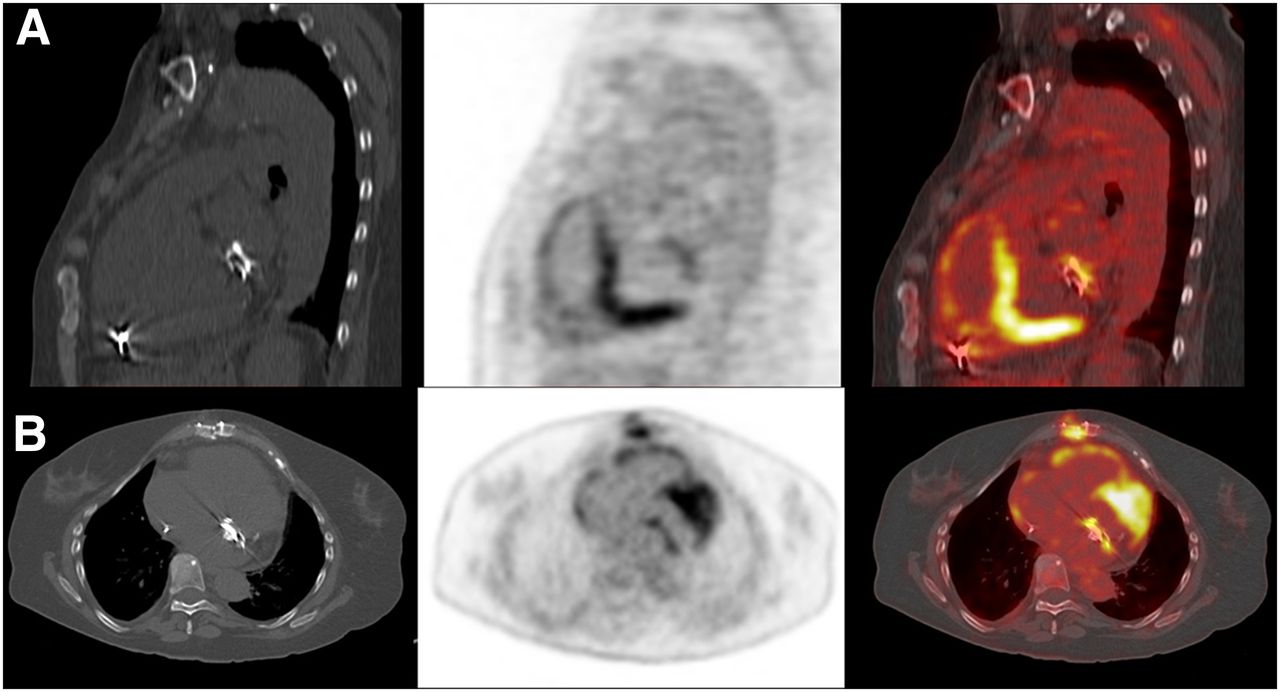
Sagittal (A) and transverse (B) 18F-FDG PET/CT images show infected prosthetic mitral valve. Culture was positive for coagulase-negative Staphylococcus. High background myocardial uptake was not cause of misdiagnosis.
There were 74 18F-FDG PET/CT concordant results of the 80 included cases corresponding to a 92% of agreement. The κ-statistics value to measure interrater agreement was 0.81 (P < 0.01).
DISCUSSION
Despite an accurate multidisciplinary approach, IE and ICED infections remains still underdiagnosed. As a consequence, the equivocal timing of empiric treatment instauration and consideration for cardiac surgery leads to poor prognosis in a considerable proportion of patients. The presence of PV and ICED consistently decreases the sensitivity and specificity of echocardiography, to about 20% for transthoracic echocardiography and around 90% (in the hands of experienced operators) for transesophageal echocardiography (6). Erba et al. (21) have demonstrated that 99mTc-HMPAO white blood cell–labeled scintigraphy is useful to locate the source of infection in patients with sepsis of different origins. However, this technique is time-consuming and its resolution is low, even using SPECT/CT images.
The earliest studies with 18F-FDG PET/CT in IE showed low sensitivities for detecting intracardiac infectious foci, which were attributed to the high myocardium physiologic uptake. Inspired by viability studies, several works have developed different strategies to inhibit myocardial uptake. In most studies, 18F-FDG PET/CT was performed after a long fasting period (at least 12 h) and a previous meal rich in fat and low in carbohydrates (14). In a series of 101 patients, Williams et al. showed that a high-fat, low-carbohydrate, protein-permitted meal eaten 3–6 h before 18F-FDG injection was useful, because the average SUVmax was significantly lower for the high-fat, low-carbohydrate, protein-permitted meal group than for the fasting group (8.8 ± 5.7 and 3.9 ± 3.6, respectively) (22). In our series, we found similar scores of mean SUVmax in the group of patients with a complete inhibition of the myocardium using heparin of 3.7 ± 1.3. However, we could only consider a complete myocardial uptake inhibition in 49 patients (61%) and partial inhibition in 11 patients (14%), so it would be of interest to compare both methods to define whether myocardial uptake suppression could be improved. The most accurate procedure described in the literature includes prolonged fasting with a low-carbohydrate diet and heparin injection (23).
There is an increasing amount of studies from groups waging to implement 18F-FDG PET/CT as an essential tool for IE and ICED infection diagnosis (14–16). Saby et al. suggested that the sensitivity of the modified Duke criteria to diagnose PVE can be enhanced if 18F-FDG PET/CT results are incorporated into a comprehensive approach including clinical, microbiologic, and echocardiographic parameters (14). Pizzi et al. found that the addition of 18F-FDG PET/CT as a major Duke criterion at admission significantly increased diagnostic sensitivity from 52% to 90.7%, with only a minor decrease in specificity, mainly due to a significant reduction in the number of possible IE cases (from 54% to 5%) (24). However, these authors included initially rejected patients by modified Duke criteria, probably making less cost-effective the indication of 18F-FDG PET/CT in suspected IE. Our study did not include initially rejected IE patients by modified Duke criteria showing a high specificity in all the indications in which 18F-FDG PET/CT was performed (including and excluding NV, specificities were 96% and 94%, respectively). Moreover, 18F-FDG PET/CT allowed reclassification of the 90% of our patients who were initially classified as possible IE. Pizzi et al. also recommended the use of hybrid electrocardiographic gating and contrast-enhanced PET/CT but they did not find significant differences in sensitivity and specificity between contrast and non–contrast-enhanced PET/CT. On the other hand, contrast-enhanced PET/CT represents an increase in both complexity of the procedure and dosimetry (increase of median effective radiation dose from 15.3 to 25.3 mSv) (24).
18F-FDG PET/CT may determine the surgical management of patients with IE, and simultaneous ICED and PV, because of its high negative predictive value (97% when NVE are excluded), was helpful in selecting which device should be removed. 18F-FDG PET/CT also was able to detect the source of infection in 7 of 15 patients (47%) with NV and rejected IE.
As it was pointed out by Chen et al., the myocardial uptake observed in the immediate postoperative period may be more likely related to persistent inflammatory changes rather than an ongoing infection (25). In our series we only found 2 false-positive cases, both suggestive of early PVE, in which 18F-FDG PET/CT was performed 1 and 8 mo after surgery, respectively. However, we have not found any false-positive case in the ICED group, even in the implanted devices for which it has been less than 1 y since implantation.
The presence of septic emboli is crucial for the correct management of patients with IE and ICED infection. Failure to identify metastatic infection complications may lead to early interruption of therapy, thus potentially triggering relapse and an unfavorable outcome. Infectious embolisms are not uncommon as they can appear between 20% and 50% of patients and can be asymptomatic and difficult to recognize (7,17,18). We were able to identify up to 8 cases of clinically unsuspected septic embolism situated mainly in the lung and in the bone. On the other hand, 18F-FDG PET/CT diagnosed 3 confirmed colorectal cancer cases linked to IE caused by Streptococcus bovis and Enterococcus faecalis (9).
Sarrazin et al. studied the value of a semiquantitative 4 grade-scale for 18F-FDG uptake, which failed to accurately discriminate infection in patients with ICED (16). In our series, we used SUVmax and 2 different SUV ratios with blood-pool SUVmean and the liver SUVmean, concluding that SUVmax is the most appropriate semiquantitative parameter, with a sensitivity and specificity both superior to 90%. However, there was no additional value of using SUVmax compared with visual analysis, so semiquantitative score should not be recommended for daily clinical practice for diagnosis of infection in these patients.
This study has several limitations. First, because results of 18F-FDG PET/CT were made available to clinicians immediately after the test was performed, subsequent treatment of the patients including decisions to perform surgery were influenced by the index test. Second, a complete myocardial uptake inhibition was not achieved in all patients, so our suggested preparation of prolonged fasting and heparin must be combined with a low-carbohydrate diet (23).
CONCLUSION
18F-FDG PET/CT proved to be a useful technique and should be included in the algorithm flowchart for early diagnosis of PVE, ICED IE, and ICED infection, reducing the rate of misdiagnosed patients. Furthermore, 18F-FDG PET/CT can simultaneously diagnose systemic complications such as septic emboli and unsuspected neoplasms, influencing substantially the clinical management of the patients. However, 18F-FDG PET/CT was not useful in the diagnosis of NVE, although in this group of patients 18F-FDG PET/CT does improve the detection of the potential source of infection. In addition, the interobserver agreement was excellent, and we did not find any significant improvement of quantification using SUV compared with visual analysis in diagnosis of infection in this series.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by AGAUR 2014 SGR 279. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
Members of the Hospital Clinic Endocarditis Study Group, Barcelona, Spain, are José M. Miró, Juan M. Pericás, Adrián Téllez, Juan Ambrosioni, Christian Manzardo, José M. Gatell, Asunción Moreno (Infectious Diseases Service); Cristina Garcia de la Mària, Yolanda Armero, Javier Garcia (Experimental Endocarditis Laboratory); Francesc Marco, Manel Almela, Jordi Vila (Microbiology Service); Eduard Quintana, Carlos Falces, Barbara Vidal, Juan C. Pare, José M. Tolosana, Elena Sandoval, Daniel Pereda, Ramon Cartaña, Salvador Ninot, Manel Azqueta, José L. Pomar, Jose Ortiz, Manuel Castella, Marta Sitges (Cardiovascular Institute); Guillermina Fita, Irene Rovira (Anesthesiology Department); David Fuster, Ulises Granados (Nuclear Medicine Service); Jose Ramírez (Pathology Department); Merce Brunet (Toxicology Service); Dolors Soy (Pharmacy Service); Pedro Castro (Intensive Care Unit); and Jaime Llopis (Department of Statistics, Faculty of Biology, University of Barcelona).
Footnotes
Published online Jun. 3, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 3, 2016.
- Accepted for publication April 12, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Comparison Between ESC and Duke Criteria for the Diagnosis of Prosthetic Valve Infective Endocarditis
- Imaging the Crevasse of Left Ventricular Assist Device Infection
- Approach to Diagnosis of Cardiovascular Implantable-Electronic-Device Infection
- Metabolic Imaging of Infection
- 18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography in Cardiac Implantable Electronic Devices Infection: Ready for Routine Care!
- 18F-FDG PET/CT in the Diagnostic Workup of Infective Endocarditis and Related Intracardiac Prosthetic Material: A Clear Message