


Abstract
The aim of this single-site, open-label clinical trial was to determine the biodistribution, pharmacokinetics, absorbed doses, and safety from 2 sequential weight-based administrations of 223Ra-dichloride in patients with bone metastases due to castration-refractory prostate cancer. Methods: Six patients received 2 intravenous injections of 223Ra-dichloride, 6 wk apart, at 100 kBq/kg of whole-body weight. The pharmacokinetics and biodistribution as a function of time were determined, and dosimetry was performed for a range of organs including bone surfaces, red marrow, kidneys, gut, and whole body using scintigraphic imaging; external counting; and blood, fecal, and urine collection. Safety was assessed from adverse events. Results: The injected activity cleared rapidly from blood, with 1.1% remaining at 24 h. The main route of excretion was via the gut, although no significant toxicity was reported. Most of the administered activity was taken up rapidly into bone (61% at 4 h). The range of absorbed doses delivered to the bone surfaces from α emissions was 2,331–13,118 mGy/MBq. The ranges of absorbed doses delivered to the red marrow were 177–994 and 1–5 mGy/MBq from activity on the bone surfaces and from activity in the blood, respectively. No activity-limiting toxicity was observed at these levels of administration. The absorbed doses from the second treatment were correlated significantly with the first for a combination of the whole body, bone surfaces, kidneys, and liver. Conclusion: A wide range of interpatient absorbed doses was delivered to normal organs. Intrapatient absorbed doses were significantly correlated between the 2 administrations for any given patient. The lack of gastrointestinal toxicity is likely due to the low absorbed doses delivered to the gut wall from the gut contents. The lack of adverse myelotoxicity implies that the absorbed dose delivered from the circulating activity may be a more relevant guide to the potential for marrow toxicity than that due to activity on the bone surfaces.
Prostate cancer is the most common male cancer worldwide and one of the leading causes of cancer-related morbidity and death. Castration-resistant prostate cancer has a poor prognosis, with a median survival of approximately 2 y. The limited treatment options available have done little to change the overall prognosis, and cytotoxic treatments are associated with substantial side effects. Approximately 90% of men with castration-resistant prostate cancer have radiologic evidence of bone metastases, which are the main cause of disability and death (1–4).
Several β-emitting radiopharmaceuticals, including 89Sr-chloride, 186Re-hydroxyethylidene disphosphonate, and 153Sm-ethylene diamine tetramethylene phosphonate, have been developed for palliation of bone pain due to metastases (5). These radiopharmaceuticals target the increased metabolism in areas of bone tumor and have demonstrated preferential uptake in metastases relative to normal bone. α-emitting radiopharmaceuticals are increasingly under evaluation and offer highly localized cytotoxic effects due to their short range and high linear energy transfer (6,7). 223Ra-dichloride is a novel, bone-seeking α emitter that has been administered to approximately 900 patients with bone metastases from castration-resistant prostate cancer in phase I–III clinical trials worldwide (8–14). It has demonstrated an antitumor effect on bone metastases in animal models (15). 223Ra has a half-life of 11.4 d and decays via a chain of α and β emissions into stable lead. Although the proportion of γ emissions from each 223Ra decay is only 1.1%, scanning and counting of patients and samples was shown to be feasible in a preliminary study to establish the basic parameters required for quantitative patient imaging of 223Ra-dichloride (16).
To date, only 1 study has reported the radiopharmacokinetics of 223Ra (12) based on clinical data, and 2 studies have calculated absorbed dose estimates based on the International Commission on Radiological Protection (ICRP) model for radium (17,18). However, to our knowledge, dosimetry results from a clinical study have not yet been published.
The primary aim of this phase 1 open-label clinical trial was to determine the biodistribution, pharmacokinetics, and dosimetry from 2 administrations of 223Ra-dichloride (100 kBq/kg) administered 6 wk apart, based on the quantitative imaging methodology developed previously (16); external counting; and blood, urine, and fecal collection.
MATERIALS AND METHODS
Patient Population
Six patients were enrolled into the study. Patients were assessed within 2 wk of 223Ra administration and were included if all the following criteria were satisfied: confirmed adenocarcinoma of the prostate, hormone-refractory disease with evidence of rising prostate-specific antigen, serum testosterone level ≤ 50 ng/dL, skeletal metastases confirmed by bone scintigraphy, Eastern Cooperative Oncology Group performance status of 0–2, life expectancy ≥ 6 mo, neutrophils ≥ 1.5 × 109/L, platelets ≥ 100 × 109/L, hemoglobin ≥ 95 g/L, normal total bilirubin, aspartate aminotransferase and alanine aminotransferase ≤ 2.5 times the upper limit of the reference range (ULN), and S-creatinine ≤ 1.5 × ULN, and the patient was able and willing to comply with the protocol and gave informed consent.
Patients were excluded for any of the following reasons: patient had received an investigational product in the 4 wk before 223Ra administration or was scheduled to receive one during the study period; patient had received chemotherapy, immunotherapy, or external radiotherapy in the 4 wk before 223Ra or was recovering from adverse events due to prior therapy; patient had previously received more than 1 regimen of cytotoxic chemotherapy; patient had prior hemibody radiotherapy; patient required immediate radiotherapy; patient had prior systemic radiotherapy with 223Ra, 89Sr, 153Sm, 186Re, or 188Re; bisphosphonates were started within 3 mo of 223Ra (unless dosage stable for ≥ 12 wk before 223Ra); patient had changes in systemic steroids within the week before 223Ra or during study period; and patient had other active malignancies (except nonmelanoma skin cancer), visceral metastases from prostate cancer, lymph node metastases with short-axis diameter > 2 cm; bulky locoregional disease; and any other serious illness or medical condition.
This clinical trial (NCT00667537) was approved by the appropriate ethics committees and was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All study subjects gave a signature of written informed consent.
Two intravenous injections of 223Ra-dichloride were administered 6 wk apart at an activity of 100 kBq per kg of whole-body weight. Patients remained in the hospital for approximately 48 h after each administration, at which time they were discharged.
Data Acquisition
The biodistribution, pharmacokinetics, and absorbed doses were determined from activity retention measurements in the whole body, individual organs, blood, urine, and feces. Safety was assessed from adverse events, which were graded according to Common Terminology Criteria for Adverse Events (version 3.0) (19).
Blood Samples
Approximately 3 mL of blood were taken from a vein in the arm contralateral to the injection site. Samples were taken before injection; immediately after injection; then at 15, 30, and 45 min and 1, 2, 4, 24, 48, 96, and 144 h after injection. One milliliter of whole blood was taken from each blood sample. The sample was then centrifuged, and 1 mL of plasma removed. The 1 mL of blood and plasma samples was measured in an automatic γ counter. A 1-mL calibration standard containing a known activity of 223Ra was counted with each set of samples.
Urine and Fecal Collection
A preinjection urine sample and first void after injection sample were collected separately. Thereafter, total urine output was collected separately for the time periods 0–4, 4–8, 8–24, and 24–48 h after injection. All feces excreted by each patient from injection to approximately 48 h were collected. Gamma spectroscopy of samples of urine and feces was performed using a whole-body counter, consisting of four 15-cm-diameter × 10-cm-thick NaI(Tl) detectors in fixed geometry located in a shielded room. Corrections were made for dead-time and sample volume.
Whole-Body Measurements
Whole-body measurements of patients were performed on a low-sensitivity whole-body counter that consisted of a single NaI detector, photomultiplier tube, and preamplifier housed in a diverging lead collimator, suspended 2 m above a bed. The counting system had 1,024 channels over an energy range of 2,048 keV. Measurements were taken immediately after injection, before first void, and then at 1 h and thereafter every 2 h during the first day, then at least twice daily until discharge. Subsequent measurements were taken at 96 and 144 h after injection.
γ-Camera Imaging
Scans were performed on the Philips Forte γ camera using the medium-energy general-purpose collimator according to a protocol previously detailed (16). Because there was an insufficient counting rate to acquire SPECT data in a time frame that was comfortable for the patient, whole-body and spot views were acquired for approximately 30 min each, using matrix sizes of 256 × 1,024 and 256 × 256 pixels, respectively. Imaging was performed using an energy window set at 82 keV with a 20% width to encompass counts from the 81- and the 84-keV emissions from 223Ra. The first scan was acquired within 0–4 h after injection, and subsequent scans were acquired at 24, 48, 96, and 144 h after injection. All images were acquired after voiding to reduce artifacts due to radioactivity in the bladder. The counting rate for all measurements was sufficiently low (<1 kcts/s over the entire spectrum counted by the camera) such that no correction was required for detector dead-time for any scans. Quantification and attenuation correction were performed as previously detailed (16).
Dosimetry
Regions of interest were delineated on the images over bone uptake with reference to the 99mTc-methylene diphosphonate bone scans acquired at pretreatment assessment. Activity in bone was calculated as the mean of the activity per unit mass in the right and left legs and skull, to avoid difficulties in interpretation due to gut and lesion uptake in the torso. The activity in bone was assumed to be distributed on the cortical and trabecular bone surfaces, in a ratio relative to the total bone surface (38% on cortical bone surfaces and 62% on trabecular bone) (20,21).
The activity in the red marrow was calculated from the blood sample measurements assuming a blood-to-bone marrow activity concentration ratio of 1.0 (22). The red marrow absorbed doses from activity on the bone surfaces and from blood were calculated separately.
No specific uptake was seen in the kidneys on the whole-body scans. The cumulated activity in the kidneys was therefore calculated from the kidney mass and measurements of the concentration of activity excreted in the urine. The activity in the urine over the first collection period (0 to ∼2 h after injection) was taken to be the activity measured at the end of this period. The activity in each subsequent collection was taken to be the average of the activity measured at the start and end of the collection period. The effective half-life after the last collection was extrapolated from the final data points. The cumulated activity in the bladder was calculated from the activity concentration determined from the collected urine.
The cumulated activity in the gut was derived from regions of interest drawn over the areas of gut uptake on the whole-body scans. In keeping with ICRP 100, the contribution of the α emission to the gut wall from the contents was taken to be 0 (23).
No specific uptake was seen in the liver on the whole-body scans. The activity in the liver was therefore estimated from the activity concentration measured in blood, under the worst-case assumption that the liver was entirely composed of blood. The blood activity concentration was multiplied by the mass of the liver to give an upper value of the activity in the liver at each time point.
The cumulated activity in the whole body was calculated from the patient’s counts measured on the low-sensitivity whole-body counter.
For imaged organs, cumulated activities were calculated by trapezoidal integration. The activity at time zero was assumed to equal the activity at the first image. The effective half-life as determined from the last 2 γ-camera images was used for extrapolation from the last measurement to infinity.
The absorbed doses delivered to normal organs were calculated with Olinda/EXM with an α quality-weighting factor of 1 (24,25). Patient-specific mass corrections were made to the Olinda S values for the whole body but not for other organs because of insufficient anatomic information for accurate mass determination. The total absorbed dose to the target region was calculated as the sum of the contributions from all source regions and included contributions from the decay of the daughter products of 223Ra.
Statistical Analysis
A statistical comparison was made between the intrapatient absorbed doses delivered at both administrations using the combined data from a representative organ for each method of data acquisition—that is, whole-body (external patient counting), liver (blood sampling), kidneys (excretion sample counting), and bone surfaces (quantitative imaging). A correlation coefficient and corresponding P value were calculated. Bladder wall absorbed doses were excluded from the comparison because they were derived from the same sample measurements as the kidney doses (i.e., the activity concentration in urine). Similarly, red marrow doses were excluded because they were derived from bone surface uptake and blood activity measurements. No absorbed dose comparisons were made in the case of the gut as no correspondence was expected because of differing excretion patterns after each administration.
Statistical analysis was performed using GraphPad Prism (GraphPad Software). The D’Agostino–Pearson test was used for normality. A statistically significant P value was considered to be less than 0.05. Descriptive statistics are presented either as mean ± SD, where data are normally distributed, or as median with the range. Mean or median absorbed doses are given as an average over all patients and both administrations.
RESULTS
Baseline and treatment characteristics for the 6 patients enrolled in the study are given in Table 1.
Patient Data
Pharmacokinetics and Biodistribution
The injected activity cleared rapidly from the blood, with 1.1% (range, 0.6%–5.1%) remaining at 24 h.
Specific uptake was seen on the γ-camera images in the whole body, bone, and gut (Fig. 1). Most of the administered activity was taken up rapidly into bone, with 61% ± 10% in the bone on the first scan 4 h after injection.
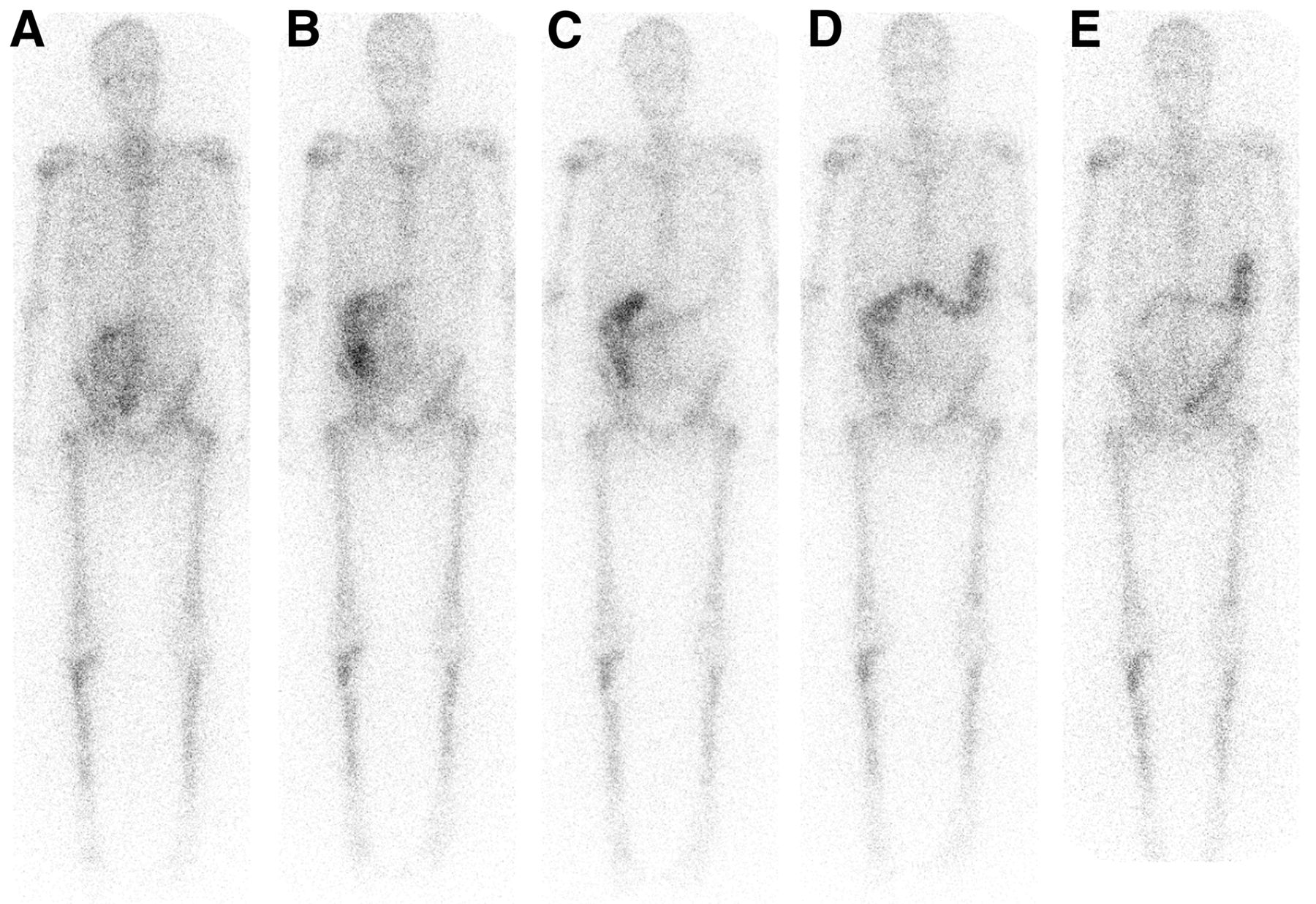
Whole-body anterior images for patient 3 acquired at 4 (A), 24 (B), 48 (C), 72 (D), and 144 h (E) after administration.
Activity passed rapidly into the small intestine (SI). For all patients, the maximum SI uptake had already occurred by the time of the first scan. At 4 h, 40% ± 19% of the administered activity was in the SI, and by 72 h all activity had cleared the SI. The maximum activity uptake in the upper large intestine (ULI) was 45% ± 16% at 24 h, decreasing to 4% (range, 0%–18%) at 1 wk. The maximum uptake in the lower large intestine (LLI) occurred at 24–72 h, with an uptake of 17% ± 11% at 48 h decreasing to 6% ± 4% at 1 wk after administration. Figure 2 shows an example of the transit of the activity through the gut.

Activity retention curves in SI, ULI, and LLI for patient 1 for administration 1 (A) and administration 2 (B). inj = injected.
Fecal excretion was the main route of elimination of activity from the body. Cumulative fecal excretion was 13% ± 12% at the time of discharge (∼48 h after injection). Excretion of activity in the urine was significantly lower than that in feces. At discharge, cumulative urine excretion was 2% ± 2% of the injected activity, and the rate of activity excretion was decreasing in all cases.
Dosimetry
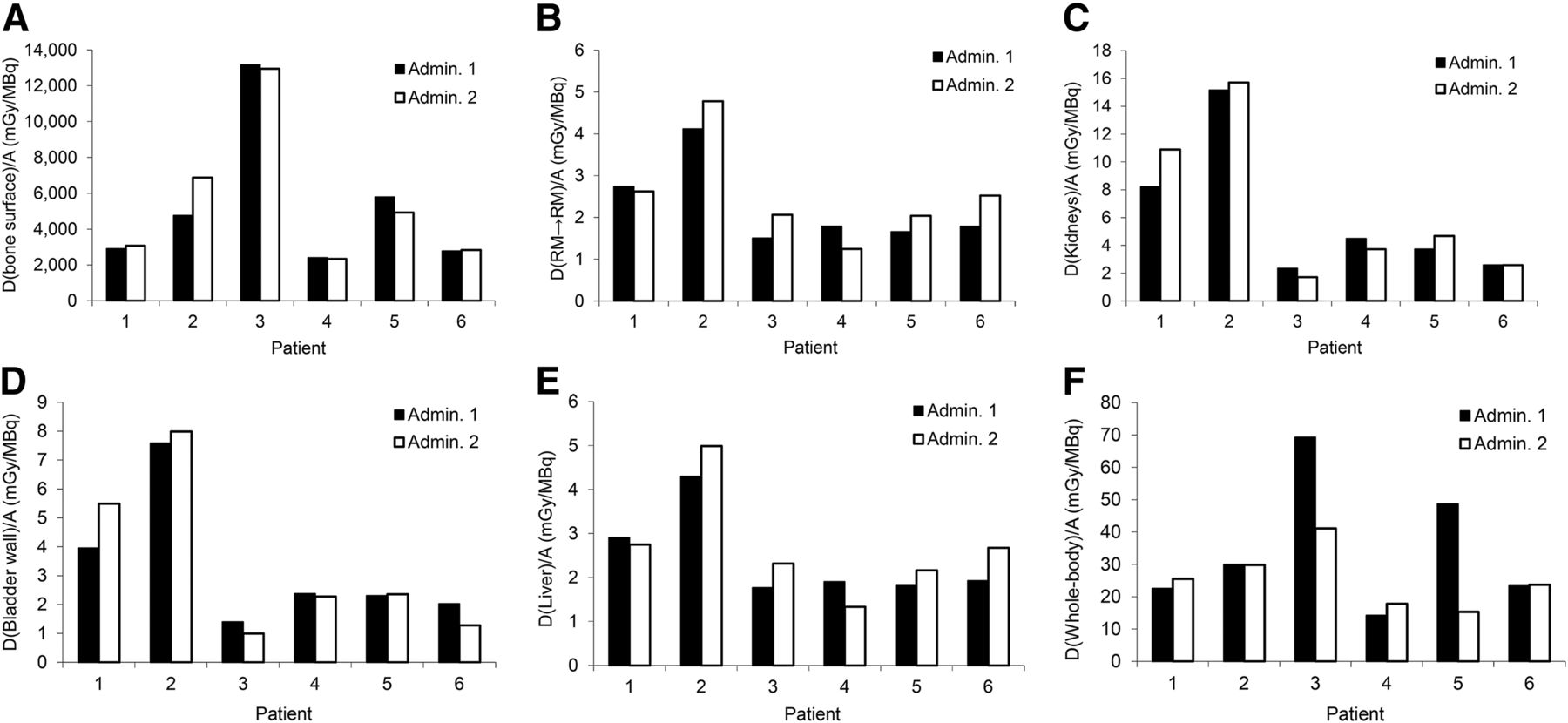
The absorbed doses per injected activity delivered to each organ are summarized in Table 2 and displayed in Figure 3. It can be see that the whole-body dose delivered from the second administration is within 30% of that delivered from the first, with the exception of 2 cases for which fecal excretion patterns differed. A statistical comparison between the intrapatient absorbed doses from the 2 administrations for the bone surfaces, kidneys, liver, and whole-body resulted in a correlation coefficient of 0.99 (P < 0.01), indicating a significant correspondence between the absorbed doses delivered at the 2 administrations. In contrast, the interpatient variability in the delivered absorbed doses per injected activity varied from a minimum of 150% for the liver absorbed dose to nearly 400% for the bone surfaces and red marrow.
Mean Residence Times and Absorbed Doses Delivered from Both Administrations
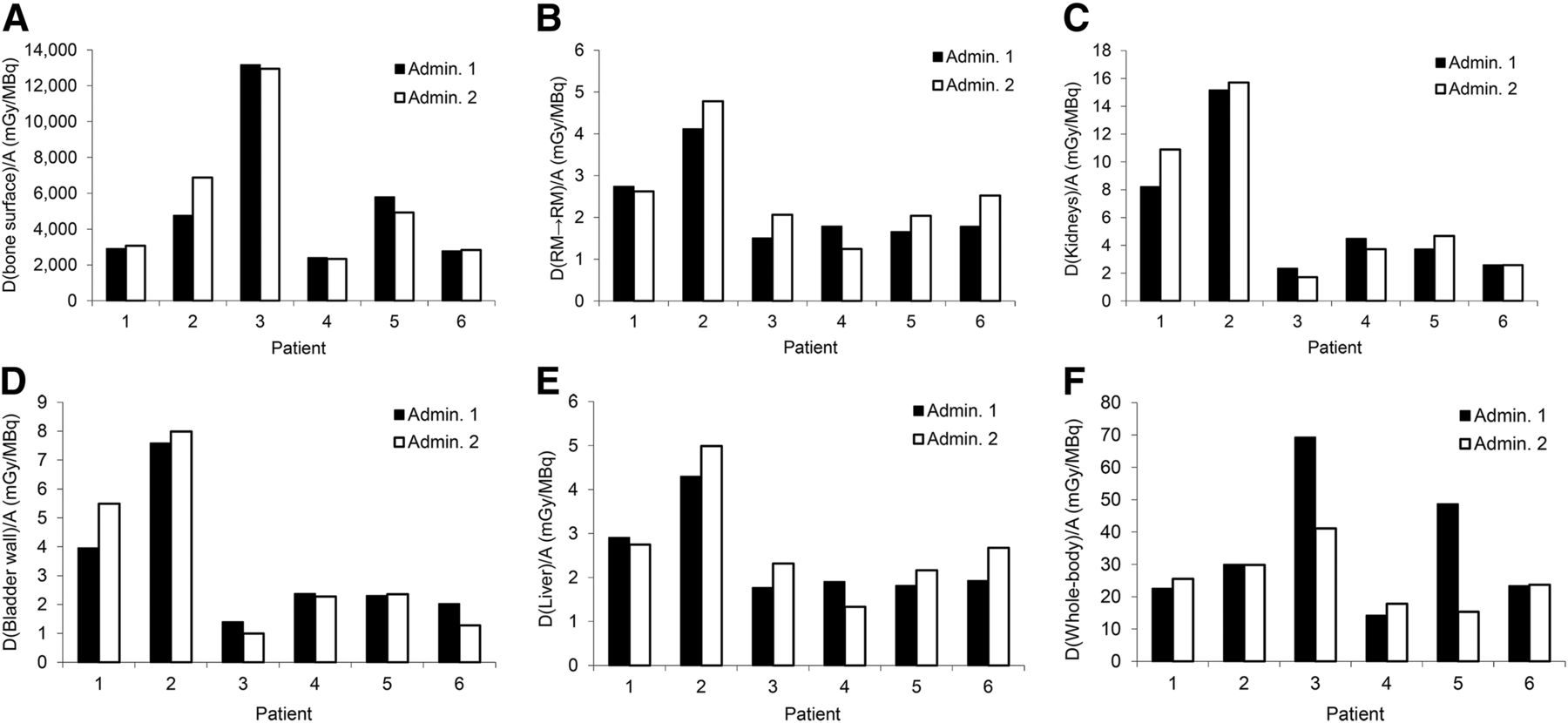
Absorbed dose (in mGy/MBq) for bone surfaces (A), red marrow from blood (B), kidneys (C), bladder wall (D), liver (E), and whole body (F). Admin. = administration.
Safety
All 6 patients experienced an adverse event during the study (Table 3). The most frequently reported adverse events were gastrointestinal (4 patients, 66.7%) and musculoskeletal and connective tissue disorders (3 patients, 50%).
Incidence of Adverse Events
DISCUSSION
The pharmacokinetic results of this trial demonstrated that the 223Ra-dichloride was rapidly cleared from the blood and taken up into bone, which supports previous findings (8,12). The main route of excretion was via the feces. The mechanism of transport from the blood into the SI is not currently understood but clearly took place rapidly because the maximum uptake in the SI had already occurred by the time of the first scan 4 h after administration as has been previously observed (12). Subsequent activity levels in the SI fell sharply, and activity appeared to pass into the LLI via the ULI.
It was assumed that the localization of all daughter products followed that of the 223Ra. However, as stated in ICRP 67 (26) it is possible that 211Pb (with a half-life of 36 min) may localize to liver, although the γ emissions from this daughter product are at the extreme of the range of the γ camera. The potential for 211Bi (with a half-life of 5 min) to localize in liver was explored by Carrasquillo et al. (12) by imaging of the 351-keV emission, with inconclusive results.
The biologic effect of absorbed doses received from α particles is poorly understood in a therapeutic context (27). Thus, although radiation weighting factors ranging from 5 to 20 are often applied to evaluate stochastic risks due to the high linear energy transfer of the emissions, for this study no weighting factor was applied.
With the exception of the gastrointestinal tract, the mean absorbed doses for each organ presented in Table 2 vary by up to an order of magnitude. The absorbed doses previously calculated based on ICRP models (18) fall within these ranges except for the red marrow, bone surfaces, and liver. Similar absorbed doses were delivered to the gastrointestinal tract although the major contribution demonstrated by Lassmann and Nosske (18) is from α irradiation, whereas this was set to 0 for this study according to the later ICRP model (23). The upper range of absorbed doses delivered to the red marrow and bone endosteum in this study are significantly higher (by up to a factor of 14) than those of Lassmann and Nosske (18). The absorbed dose to the liver was found to be significantly lower in this study.
In this study, mild adverse myelotoxicity was seen for only 1 patient, although anemia, leukopenia, neutropenia, and thrombocytopenia have been reported in other studies (8–13). Adverse myelotoxicity has not been seen at a level that might be expected from the high total absorbed doses determined in this study. Absorbed doses are primarily delivered to the red marrow from circulating blood and from uptake on the bone surfaces. However, α emissions will irradiate only a small fraction of the red marrow because of their short range (28). The absorbed dose delivered from the circulating activity may therefore be a more relevant guide to the potential for marrow toxicity than that due to activity on the bone surfaces. The large self-absorbed doses delivered to the bone surfaces are particularly of note and may prove in the long term to be the cause of dose-limiting toxicity.
Calculations of the mean absorbed dose delivered to the walls of the SI, ULI, and LLI were performed under the assumptions that all the activity was in the gut contents and that the contribution to the walls of the gut from α emissions was negligible, as stated by ICRP 100 (23). Although acute gastrointestinal toxicity from 223Ra-dichloride treatment has not been reported as a significant occurrence in other studies, diarrhea has been reported and indeed 1 patient in this study experienced diarrhea (8–13). If 223Ra is retained in the mucosa, the absorbed dose delivered to the walls of the gut may not be negligible and the above assumptions would result in an underestimation of gut doses.
Whole-body dosimetry can be calculated accurately and has proven to be a reliable surrogate for the absorbed dose delivered to the red marrow in studies of 131I-metaiodobenzylguanidine therapy (29). The relative simplicity of this procedure also facilitates its routine clinical use. However, a key assumption for organ-level dosimetry is uniform distribution of uptake, and only an average absorbed dose is calculated for a target organ. These assumptions are particularly erroneous for treatment with α emitters, and whole-body dosimetry may prove to be of limited value. Further studies are required to investigate this.
Interpatient comparisons indicate that a wide range of absorbed doses are delivered from weight-based administrations of activity whereas intrapatient results show that the absorbed doses delivered from a second administration closely follow those delivered from the first in most cases. Taken into consideration with the generally low-toxicity profile of the studies performed to date, the implication is that the option of personalized treatments could be explored.
CONCLUSION
This dosimetry study of 223Ra-dichloride has demonstrated a range of absorbed doses delivered to critical organs. Biodistribution, pharmacokinetics, and absorbed doses are largely consistent over 2 administrations for any given patient, which would facilitate personalized treatments.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Research funding was provided by Bayer Healthcare Pharmaceuticals and Algeta ASA. Christopher C. Parker consults for Bayer Healthcare Pharmaceuticals and Algeta ASA. NHS funding was provided to the NIHR Biomedical Research Centre at The Royal Marsden and the ICR. Valerie J. Lewington consults for Bayer Healthcare Pharmaceuticals. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 16, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 5, 2015.
- Accepted for publication June 23, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- ISIT-QA: In Silico Imaging Trial to Evaluate a Low-Count Quantitative SPECT Method Across Multiple Scanner-Collimator Configurations for 223Ra-Based Radiopharmaceutical Therapies
- Beyond Average: {alpha}-Particle Distribution and Dose Heterogeneity in Bone Metastatic Prostate Cancer
- Dose-Dependent Growth Delay of Breast Cancer Xenografts in the Bone Marrow of Mice Treated with 223Ra: The Role of Bystander Effects and Their Potential for Therapy
- Cellular and Genetic Determinants of the Sensitivity of Cancer to {alpha}-Particle Irradiation
- First Whole-Body Three-Dimensional Tomographic Imaging of Alpha Particle Emitting Radium-223
- Prostate-Specific Membrane Antigen-Targeted Radiohalogenated PET and Therapeutic Agents for Prostate Cancer
- Bone-Targeted Imaging and Radionuclide Therapy in Prostate Cancer