


Abstract
111In-DOTA-exendin-4 SPECT/CT has been shown to be highly efficient in the detection of insulinomas. We aimed at determining whether novel PET/CT imaging with [Nle14,Lys40(Ahx-DOTA-68Ga)NH2]exendin-4 (68Ga-DOTA-exendin-4) is feasible and sensitive in detecting benign insulinomas. Methods: 68Ga-DOTA-exendin-4 PET/CT and 111In-DOTA-exendin-4 SPECT/CT were performed in a randomized cross-over order on 5 patients with endogenous hyperinsulinemic hypoglycemia. The gold standard for comparison was the histologic diagnosis after surgery. Results: In 4 patients histologic diagnosis confirmed a benign insulinoma, whereas one patient refused surgery despite a positive 68Ga-DOTA-exendin-4 PET/CT scan. In 4 of 5 patients, previously performed conventional imaging (CT or MR imaging) was not able to localize the insulinoma. 68Ga-DOTA-exendin-4 PET/CT correctly identified the insulinoma in 4 of 4 patients, whereas 111In-DOTA-exendin-4 SPECT/CT correctly identified the insulinoma in only 2 of 4 patients. Conclusion: These preliminary data suggest that the use of 68Ga-DOTA-exendin-4 PET/CT in detecting hidden insulinomas is feasible.
The most common cause of endogenous hyperinsulinemic hypoglycemia in adults is an insulinoma. Endogenous hyperinsulinemic hypoglycemia is biochemically diagnosed by a prolonged supervised fasting test in an inpatient setting (1). Approximately 5%–10% of insulinomas are multiple, mainly in the context of multiple endocrine neoplasia type 1, less than 10% are malignant, and most are benign single insulinomas (1). The only curative treatment of an insulinoma is its surgical removal. Therefore, exact preoperative localization of the insulinoma is critical to planning the surgical intervention (1). MR imaging, CT, or endoscopic ultrasound is normally used to localize insulinomas (1). However, the small size of the tumors (often <1 cm) limits the sensitivity of these methods (1). Sensitivity can be increased by including methods such as angiography with selective arterial calcium stimulation and hepatic venous sampling. However, this procedure is invasive, with a concomitant risk of complications. The sensitivity of somatostatin receptor scintigraphy and SPECT/CT is usually low (33%–50%) and inconsistent for 18F-DOPA PET (90% in a prospective study and 20% in a retrospective study) (2).
It has been shown that targeting the glucagonlike peptide-1 receptors (GLP-1R) using the specific ligand [Lys40(Ahx-DOTA-111In)NH2]exendin-4, [Lys40(Ahx-DTPA-111In)NH2]exendin-4, or [Lys40(Ahx-HYNIC-99mTc/EDDA)NH2]exendin-4 is a very sensitive (≥95% sensitivity), noninvasive method to localize benign insulinomas with SPECT (2–4). In comparison to SPECT, PET has a higher spatial resolution and sensitivity and accurately quantifies tracer uptake (5). Recently, it has been shown that 68Ga-DO3A-VS-Cys40-exendin-4 PET/CT can detect malignant insulinomas (6).
The aim of our study was, first, to determine whether the use of [Nle14,Lys40(Ahx-DOTA-68Ga)NH2]exendin-4 (68Ga-DOTA-exendin-4) PET/CT in the detection of benign insulinomas is feasible and, second, to compare its detection rate with that of [Nle14,Lys40(Ahx-DOTA-111In)NH2]exendin-4 (111In-DOTA-exendin-4) SPECT/CT in the same patients.
MATERIALS AND METHODS
Patients
Five consecutive patients were screened and accepted for our prospective pilot study. The patients were referred from 4 tertiary care centers in Switzerland. All patients fulfilled the following inclusion criteria: biochemically proven endogenous hyperinsulinemic hypoglycemia with neuroglycopenic symptoms, negative results on sulfonylurea screening (exclusion of hypoglycemia factitia), contrast-enhanced 3-T MR imaging performed no more than 2 mo previously, and age above 18 y. Patients with evidence of malignant insulinoma on conventional imaging were excluded, as well as pregnant women, patients with allergies to exendin-4, and patients with renal insufficiency (blood creatinine concentrations > 140 μmol/L).
The institutional review board approved this study, and all subjects gave written informed consent.
Procedures
111In-DOTA-exendin-4 SPECT/CT and 68Ga-DOTA-exendin-4 PET/CT were performed within 24–73 h in randomized crossover order. Synthesis and labeling of 68Ga-DOTA-exendin-4 and 111In-DOTA-exendin-4 have been described elsewhere (7).
Total-body planar images and SPECT/CT of the abdomen were performed 4 and 72 h after intravenous injection of 79.2 ± 9.3 MBq (range, 66–90 MBq, 10.5–14.4 μg) of 111In-DOTA-exendin-4. The SPECT/CT scanner (Symbia Intevo; Siemens Healthcare) was equipped with a medium-energy, parallel-hole collimator (window setting, 172 and 247 keV; width, 15%; rotation, 2 × 180°; matrix, 256 × 256; projections, 60; acquisition time per projection, 24 s). All patients underwent unenhanced low-dose CT (130 kVp, 40 mA) for attenuation correction and to provide an anatomic reference.
PET/CT was performed on a PET/16-detector CT scanner (Discovery ST; GE Healthcare). One bed position of the upper abdomen was acquired during 8 min, 2.5 h after intravenous injection of 79.8 ± 3.9 MBq (range, 76–97 MBq, 12.0–15.3 μg) of 68Ga-DOTA-exendin-4. All patients underwent unenhanced low-dose CT for attenuation correction and to provide an anatomic reference (120 kVp, 30–100 mAs). Blood samples were taken 2, 5, 15, 30, 60, 120, and 180 min after injection of 68Ga-DOTA-exendin-4 and 111In-DOTA-exendin-4 to measure glucose levels and blood clearance. An additional blood sample was taken 300 min after injection of 111In-DOTA-exendin-4. All conventional scans were independently interpreted by experienced radiologists at the referral centers. GLP-1R SPECT/CT and PET/CT scans were independently assessed by 2 board-certified nuclear medicine physicians. Both interpreters were masked to other imaging results and the patient’s clinical history. In cases of discordant findings, a consensus was reached between the 2 interpreters. Tumor-to-background ratios were measured for 111In-DOTA-exendin-4 (counts) and 68Ga-DOTA-exendin-4 (maximal standardized uptake values).
Histologic diagnosis was regarded as the standard for comparison. The pathologists were masked to the results of other diagnostic tests but were aware of the patient’s clinical history. Finally, GLP-1R expression was evaluated in vitro by GLP-1R autoradiography as previously described (8).
RESULTS
The clinical characteristics are summarized in Table 1. In all 5 patients, the fasting plasma glucose level was measured. Symptoms of neuroglycopenia in association with low plasma glucose levels (mean, 2.1 mmol/L; range, 1.6–2.6 mmol/L) and inadequately increased insulin (mean, 12.1 mU/L; range, 3.9–21.9 mU/L) and C-peptide (mean, 0.714 nmol/L; range, 0.5–0.98 nmol/L) levels were documented in all patients after 12–52 h of fasting.
Clinical Characteristics
The labeling yield of 111In- and 68Ga-DOTA-exendin-4 was more than 95%, and the radiochemical purity was at least 95% for 111In-DOTA-exendin-4 and at least 93% for 68Ga-DOTA-exendin-4, at a specific activity of 30 MBq/nmol.
Blood sampling of 111In-DOTA-exendin-4 revealed a biexponential blood clearance with half-times of 16 ± 2 min and 110 ± 19 min. 68Ga-DOTA-exendin-4 also revealed a biexponential blood clearance, with half-times of 14 ± 3 min and 41 ± 4 min. Both compounds showed a plasma clearance of about 50% in the α phase (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org).
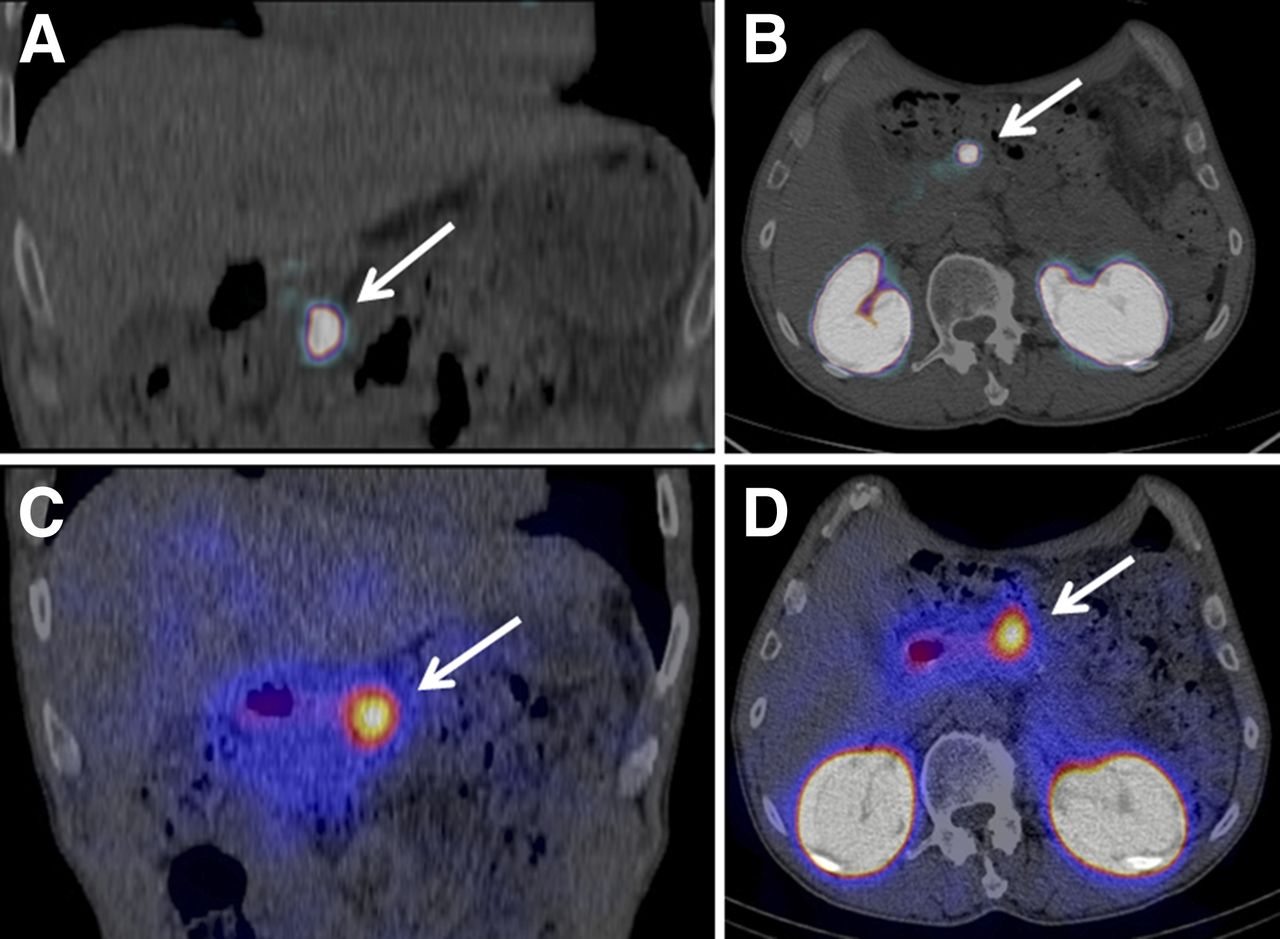
The imaging results are summarized in Table 2. In patient 4, focal uptake of 111In-DOTA-exendin-4 and 68Ga-DOTA-exendin-4 was highly suggestive of an insulinoma (Fig. 1); however, the patient has refused surgery so far.
Preoperative Imaging and Operative Procedures
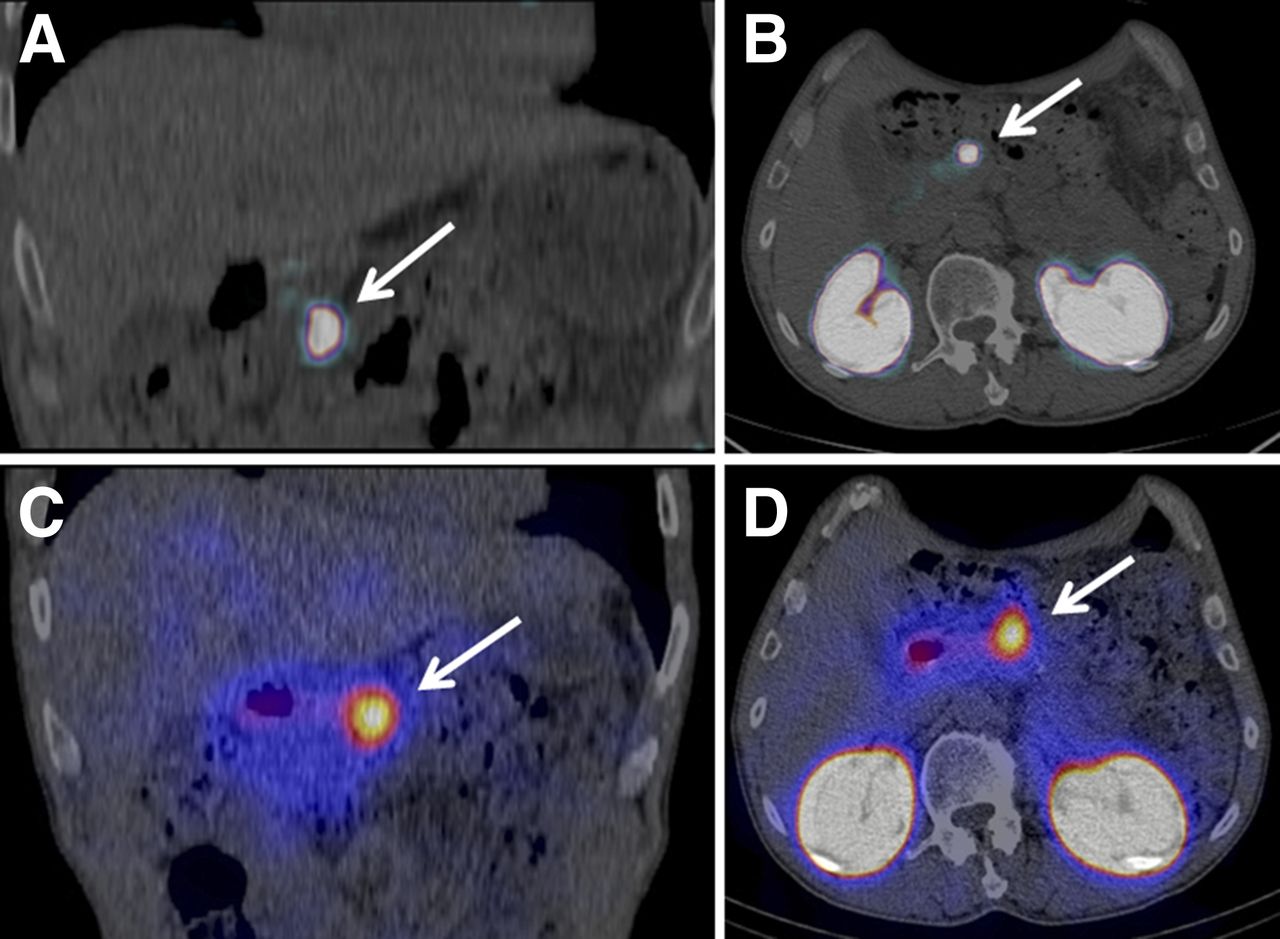
(A and B) Coronal (A) and transaxial (B) PET/CT images from patient 4 obtained 2.5 h after injection of 80 MBq of 68Ga-DOTA-exendin-4. (C and D) Coronal (C) and transaxial (D) SPECT/CT images of same patient 72 h after injection of 90 MBq of 111In-DOTA-exendin-4. Focal uptake of 111In-DOTA-exendin-4 and 68Ga-DOTA-exendin-4 is seen in pancreatic body (arrows); patient has refused surgery so far.
All patients received an infusion of exogenous glucose (1,000 mL, 10%) for 5 h starting just before injection of the radiotracer. This step prevented the occurrence of any severe hypoglycemic episodes. Two patients experienced nausea—and 2 patients nausea and vomiting—after injection of 111In-DOTA-exendin-4. One patient experienced nausea after injection of 68Ga-DOTA-exendin-4. No other adverse effects were observed.
In all 4 patients who underwent surgery, histologic examination confirmed the diagnosis of a benign insulin-producing tumor (Table 2) and symptoms of hypoglycemia resolved immediately after surgery.
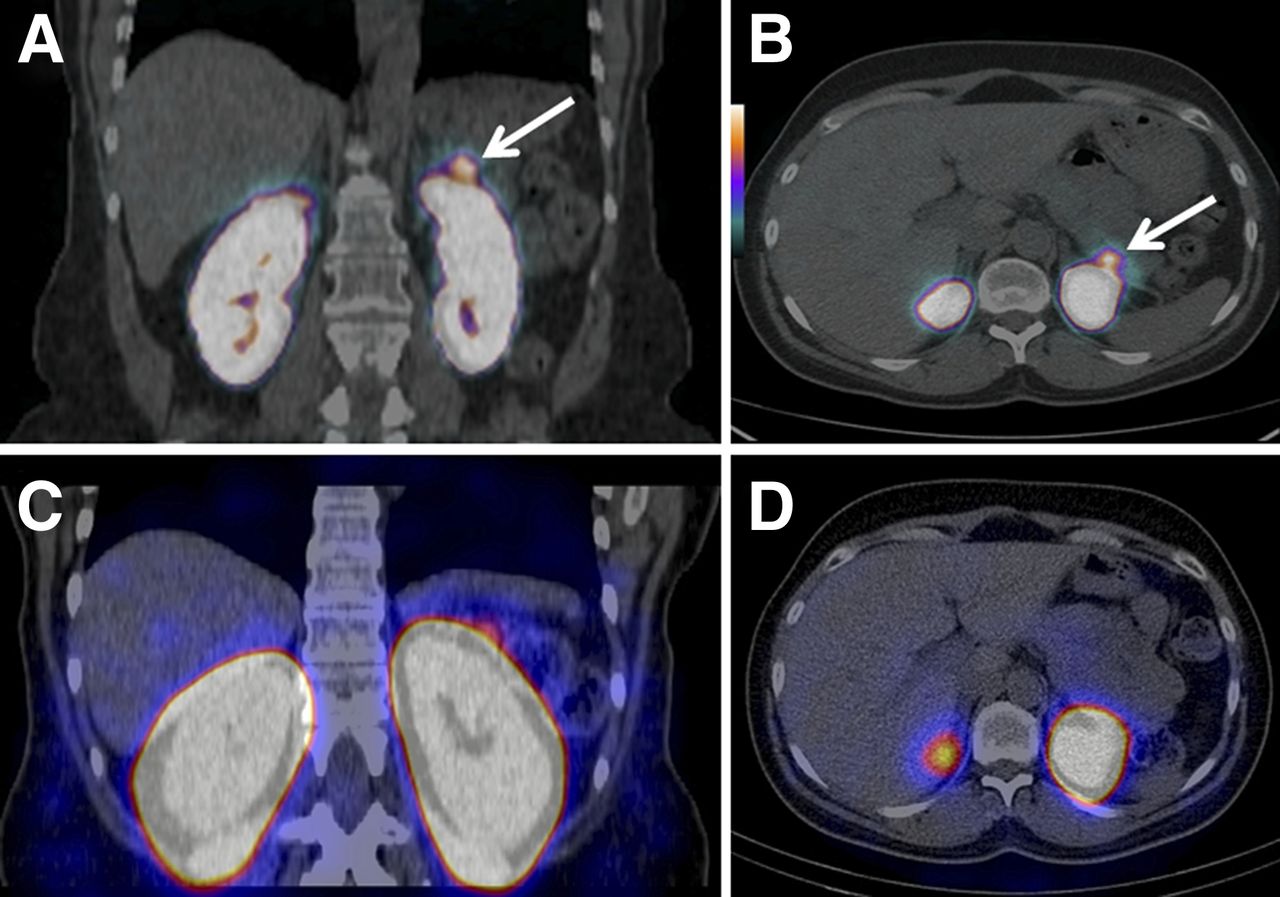
Histopathologic diagnosis was made at the local institution. In patient 5, imaging and additional in vitro GLP-1R autoradiography was performed (Figs. 2 and 3).

(A and B) Coronal (A) and transaxial (B) PET/CT images from patient 5 obtained 2.5 h after injection of 76 MBq of 68Ga-DOTA-exendin-4. (C and D) Coronal (C) and transaxial (D) SPECT/CT images of same patient 72 h after injection of 66 MBq of 111In-DOTA-exendin-4. Arrows show focal 68Ga-DOTA-exendin-4 uptake in distal pancreatic tail consistent with surgically removed insulinoma. SPECT/CT did not show the insulinoma.

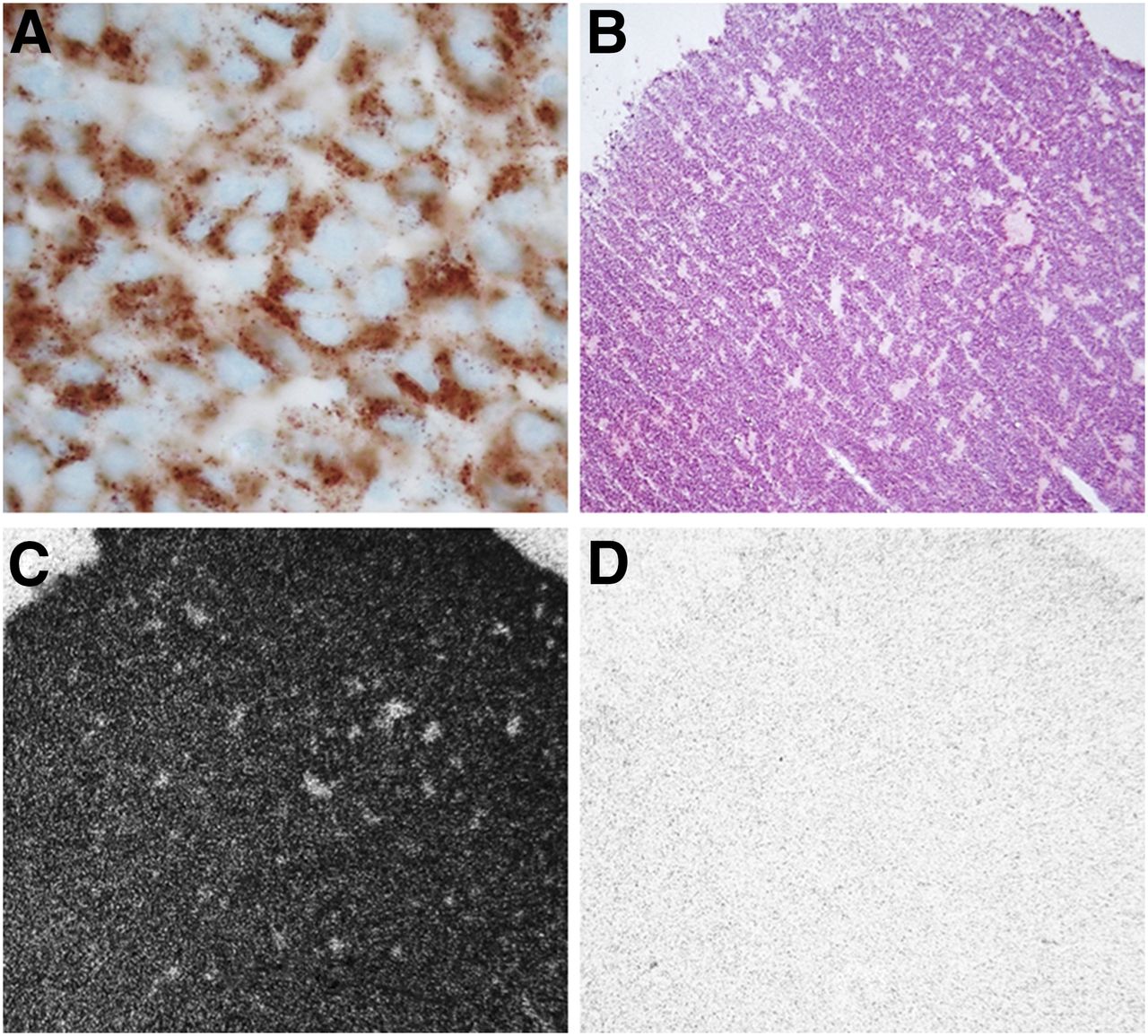
Hormone and receptor evaluation of resected insulinoma in patient 5. (A) Immunohistochemistry for insulin showing strongly labeled tumor cells. (B) Hematoxylin- and eosin-stained tumor tissue. (C) In vitro autoradiography revealing high GLP-1R density (mean, 5,766 dpm/mg of tissue). (D) Autoradiogram showing nonspecific binding of 125I-GLP-1 (7–36) amide in presence of 100 nM GLP-1 (7–36) amide.
DISCUSSION
This report provides the proof of principle that 68Ga-DOTA-exendin-4 PET/CT is feasible and sensitive in the preoperative detection of hidden insulinomas in patients. In all 4 of the patients who underwent surgery, 68Ga-DOTA-exendin-4 PET/CT had already detected the insulinoma by 2.5 h after injection. GLP-1R imaging changed the clinical management of 3 of the 4 patients, whereas in the first patient only 68Ga-DOTA-exendin-4 PET/CT correctly localized the small insulinoma, which was crucial for planning surgery. 68Ga-DOTA-exendin-4 PET/CT revealed higher tumor-to-background ratios (2.5 h after injection) than 111In-DOTA-exendin-4 SPECT/CT (4 and 72 h after injection) because of an advantageous partial-volume effect in PET (9) and faster blood clearance of 68Ga-DOTA-exendin-4 than of 111In-DOTA-exendin-4. Furthermore, PET has a higher spatial resolution than SPECT (5). This is relevant for the detection of insulinomas near the highly active kidneys. The better spatial resolution of PET together with the higher tumor-to-background ratio of 68Ga-DOTA-exendin-4 PET/CT brought about a higher insulinoma detection rate than was obtained with 111In-DOTA-exendin-4 SPECT/CT.
Late 111In-DOTA-exendin-4 SPECT scans (72 h after injection) showed a slightly higher tumor-to-background ratio than early SPECT scans. This finding is consistent with our previously published work (2) in which we suggested late scans 3–7 d after injection in patients with negative findings on early scans. However, late scans may increase the risk of false-positive results because of the physiologic expression of GLP-1R in pancreatic islets or acini and the Brunner gland of the duodenum (8).
The shorter imaging procedure, higher tumor-to-background ratio, better spatial resolution (5), and lower radiation burden of 68Ga-DOTA-exendin-4 PET/CT (7) favor this novel method over 111In-DOTA-exendin-4 SPECT/CT. Furthermore, absolute quantification of tumor and background uptake, which might be useful to improve interobserver agreement and specificity, is better evaluated with PET/CT than with SPECT/CT. GLP-1R PET/CT is expected to have a high clinical impact on the management of patients with endogenous hyperinsulinemic hypoglycemia. Previous experience (2) suggests that insulinomas in the context of multiple endocrine neoplasia type 1 express GLP-1R. It is therefore likely that GLP-1R PET/CT will be a valuable tool to distinguish between insulin-secreting lesions and gastrin-secreting or nonsecreting pancreatic lesions in this genetic syndrome, thereby determining the surgical strategy. Whether GLP-1R PET/CT will be useful in diagnosing other conditions of endogenous hyperinsulinemic hypoglycemia, such as β-cell hyperplasia or hypertrophy (nesidioblastosis), in adults and children remains to be determined.
This study had limitations. First, conventional imaging could not be standardized because of differences in local availability. However, MR imaging was performed on all patients. Second, conventional imaging had a tendency to underperform compared with what has been reported in the published literature (1,10). This discrepancy might be explained by the fact that most patients were referred after having undergone conventional imaging with negative results and were therefore part of a negative selection. Finally, this study included only 5 patients. However, it was intended to be a pilot study. Because of the promising results, a larger study evaluating GLP-1R PET/CT has been started.
CONCLUSION
This study proved that 68Ga-DOTA-exendin-4 PET/CT is a feasible and sensitive tool for the detection of insulinomas. The higher spatial resolution, the possibility of quantification, and the lower radiation burden favor 68Ga-DOTA-exendin-4 PET/CT over 111In-DOTA-exendin-4 SPECT/CT.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported in part by the Swiss National Science Foundation (grant 320030_152938/1) and the Desirée and Niels Yde’s Foundation (grant 389-12). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the respective doctors for referring the patients, as well as the University of Basel Hospital staff for excellent technical assistance.
Footnotes
↵* Contributed equally to this work.
Published online May 21, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 23, 2015.
- Accepted for publication May 15, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improved Localization of Insulinomas Using 68Ga-NODAGA-Exendin-4 PET/CT
- 68Ga-NODAGA-Exendin-4 PET/CT Improves the Detection of Focal Congenital Hyperinsulinism
- Glucagon-like Peptide-1 Receptor as Emerging Target: Will It Make It to the Clinic?
- Optoacoustic Imaging of Glucagon-like Peptide-1 Receptor with a Near-Infrared Exendin-4 Analog
- Optoacoustic imaging of GLP-1 Receptor with a near-infrared exendin-4 analog
- PET-Based Human Dosimetry of 68Ga-NODAGA-Exendin-4, a Tracer for {beta}-Cell Imaging
- The future: surgical advances in MEN1 therapeutic approaches and management strategies
- Molecular imaging in the investigation of hypoglycaemic syndromes and their management
- Approaches to Improve the Pharmacokinetics of Radiolabeled Glucagon-Like Peptide-1 Receptor Ligands Using Antagonistic Tracers
- Glucagon-Like Peptide-1 Receptor PET/CT with 68Ga-NOTA-Exendin-4 for Detecting Localized Insulinoma: A Prospective Cohort Study
- Radiopeptides for Imaging and Therapy: A Radiant Future