


Abstract
The objective of this study was to evaluate the response rate and survival of hepatocellular carcinoma portal vein thrombosis (PVT) patients treated with 90Y-loaded glass microspheres using a personalized dosimetry and intensification concept. Methods: The microspheres were administered to 41 hepatocellular carcinoma PVT patients (main = 12; lobar/segmental = 29). 99mTc-macroaggregated albumin SPECT/CT quantitative analysis was used to calculate the tumor dose (TD), healthy injected liver dose (HILD), and injected liver dose (ILD). Response was evaluated at 3 mo using the criteria of the European Association for the Study of the Liver, with CT follow-up lasting until disease progression or death. Survival was assessed using the Kaplan–Meier method. Results: The mean injected activity was 3.1 ± 1.5 GBq, and mean ILD was 143 ± 49 Gy. When a TD threshold of 205 Gy was applied, 99mTc-macroaggregated albumin SPECT/CT achieved a 100% sensitivity and 90% overall accuracy (0 false-negatives; 4 false-positives) in response prediction. On the basis of TD and HILD values, 37% of patients received an intensification of the treatment (increased injected activity with the aim of achieving a TD ≥ 205 Gy and HILD < 120 Gy, applying an ILD > 150 Gy). This intensification resulted in a high response rate (85%) without increased liver toxicity of grade 3 or higher (6% vs. 12% in the patients who did not receive treatment intensification; not statistically significant). For the total 41 patients, median overall survival (OS) was 18 mo (95% confidence interval, 11–25 mo). For patients with a TD of less than 205 Gy, median OS was 4.3 mo (3.7–5 mo), versus 18.2 mo (8.5–28.7 mo) for those with a TD of 205 Gy or more (P = 0.005). Median OS was 20.9 mo for patients with a TD of 205 Gy or more and good PVT targeting (n = 36). OS was 12 mo (3 mo to ∞) for patients with main PVT, versus 21.5 mo (12–28.7 mo) for those with segmental or lobar PVT (not statistically significant). For the 5 patients with complete portal vein revascularization who underwent lobar hepatectomy, median OS was not reached yet exceeded 24.5 mo and was significantly higher than that of other patients (P = 0.0493). Conclusion: Using a 99mTc-macroaggregated albumin SPECT/CT personalized dosimetry and intensification concept with 90Y-loaded glass microspheres induced prolonged OS for PVT patients as compared with the standard of care (sorafenib), without increasing liver toxicity. Prospective randomized studies are therefore warranted.
Hepatocellular carcinoma is one of the most common cancers in the world, with approximately 500,000 new cases per year (1). The prognosis is particularly poor in portal vein thrombosis (PVT) cases, with a reported spontaneous survival of 5.1 mo in Western counties (2) and 4.2 mo in Asia (3). Therapeutic care for PVT patients is difficult, because PVT is a contraindication for surgery and chemoembolization. Radioembolization using 131I-Lipiodol (Guerbet) is the first therapeutic option that has proven effective in significantly increasing overall survival (OS) in a randomized study (4). The efficacy of sorafenib has also been validated in 2 positive randomized studies (2,3). However, even with the administration of sorafenib, the OS for this patient population is poor, remaining below 8.1 mo (4).
Several nonrandomized studies applying radioembolization using 90Y-loaded microspheres have reported promising results, with OS ranging from 10 to 13 mo in PVT patients using the standard dosimetric approach (5–9). In a technique combining 90Y-loaded glass microspheres and the standard dosimetric approach, the objective is to administer 120 ± 20 Gy to the treated liver, regardless of the tumoral dosimetry. Using macroaggregated albumin (MAA)–based dosimetry, a dose–response relationship was clearly identified (10,11), and we found that it was necessary to reach a 205-Gy tumor dose (TD) threshold to achieve a response (11). We have also recently described the lobar intensification concept in a cohort of unselected patients (12).
This paper reports our results using a personalized dosimetric approach of 90Y-loaded glass microsphere injections in PVT patients, with treatment intensification when required.
MATERIALS AND METHODS
This was a retrospective cohort study comprising 41 consecutive PVT patients treated using a personalized dosimetric evaluation between October 2008 and September 2012. This study was an extension of our previously published cohort of PVT patients (12). Written informed consent was obtained from each patient, and the use of selective internal radiation therapy was approved by the Ethics Committee of our university hospital. The indications governing the use of selective internal radiation therapy were defined during a hepatocellular carcinoma multidisciplinary staff meeting. Selective internal radiation therapy was used as first-line treatment for 66% of patients and for recurrences in the remaining 34%. Patients were considered unsuitable for chemoembolization if they had PVT involvement. No patient presented with extrahepatic spread. The patient and tumor characteristics are presented in Table 1.
Demographic and Baseline Characteristics of Patients (n = 41)
Microspheres were administered according to current standard guidelines. After diagnostic angiography, liver perfusion scanning was conducted, and then 185 MBq of 99mTc-MAA were injected into the hepatic artery. Planar acquisitions were performed for lung shunt evaluation. SPECT/CT acquisitions were conducted with the following parameters: window, 140 ± 7.5 keV; 32 projections; 180°; matrix, 128 × 128; and 30 s/projection (Symbia T2 gantry; Siemens). Findings were reconstructed using an iterative method consisting of ordered-subset expectation maximization, 5 iterations, and 8 subsets, with attenuation correction using a low-dose CT attenuation map, and scatter correction applying the Jaszczak method (dual-energy-window scatter correction, with a scatter window of 120 ± 7.5 keV). No correction for volume effect was performed because of the large lesion sizes. The images were then visualized with or without CT scan fusion.
As previously described, volumetric analysis software (Syngo workstation; Siemens) was used for quantitative tumoral and nontumoral liver tissue evaluation (11,12). This software enables the semiautomatic generation of the volume of interest in the injected liver and tumor by means of an isocontour method. For each volume of interest, the threshold value was adjusted to achieve good matching between the isocontours of the 99mTc-MAA distribution and the liver and tumor boundaries on fusion images. These volumes of interest were then used to measure the 99mTc-MAA volume of distribution in the injected liver and tumor, as well as the total activity contained therein.
Rather than absolute quantification of 99mTc-MAA in Bq/mL for each volume of interest, relative quantification was performed (percentage of detected counts in each volume of interest). The volume and activity values in the injected healthy liver were calculated by subtraction.
The doses in the selected volumes of interest (i.e., tumor, injected liver, and healthy injected liver) were calculated using the classic MIRD formula: where DVOI = mean dose in the volume of interest, AVOI = total activity in the volume of interest, and WVOI = weight of the volume of interest, with W being a volume of 1.03 L.
where DVOI = mean dose in the volume of interest, AVOI = total activity in the volume of interest, and WVOI = weight of the volume of interest, with W being a volume of 1.03 L.
The injected activity was calculated using the following personalized dosimetric endpoints: if possible, attain a TD of 205 Gy or more, with a healthy injected liver dose (HILD) of less than 120 Gy and a lung dose of less than 30 or 50 Gy for cumulative treatments.
Treatment intensification was defined as delivery of an injected liver dose (ILD) of at least 150 Gy (12). For treatment intensification, the established endpoint was to achieve a TD of 205 Gy or more. Treatment intensification was not intended to reach 120 Gy for the HILD. Conserving HILD below 120 Gy was only a matter of safety. No intensification was performed if required to reach an HILD of at least 120 Gy to attain the TD threshold of 205.
After 8–15 d, glass microspheres (TheraSphere; BTG International) were injected using a lobar approach typically on the following Wednesday, 3 d after calibration, during the first treatment week. In cases of bilateral disease, 2 lobar treatments were administered separately, with a 6- to 8-wk interval between treatments.
The response of treated lesions was assessed using the criteria of the European Association for the Study of the Liver (13). Morphologic responses using the Response Evaluation Criteria in Solid Tumors and α-fetoprotein responses for patients with an α-fetoprotein level of 200 kIU/L or more were also provided. Triphasic CT was performed 3 mo after treatment and then every 3 mo until disease progression or death. Toxicity was scored by applying the common terminology criteria for adverse events (version 4). Only permanent and clinically relevant liver toxicity of grade 3 or higher and manifesting within 6 mo of radioembolization was considered a limiting factor. The imputability of the suspected toxicity was defined according to guidelines laid down by the International Conference on Harmonization (ICH E2B [R3]), attributing toxicity to disease progression for patients with both liver toxicity and evidence of widely progressive disease.
Statistics
Quantitative values were expressed as mean ± SD and were compared between responding and nonresponding patients using a distribution-free Wilcoxon–Mann–Whitney comparison test. Discontinuous data were compared by means of the χ2 test (Fisher exact test). This test was used in conjunction with univariate analysis to identify parameters associated with tumor response, progression-free survival (PFS), OS, and liver toxicity. Significant data from univariate analysis were then subjected to multivariate analysis using logistic regression testing. Survival rates were estimated using the Kaplan–Meier method and compared on the basis of log-rank testing. Survival rates were not censored for hepatectomies. SAS software was used for statistical analysis, with a significance threshold set at a P value of 0.05 or less.
RESULTS
Of the total 41 treated patients, 15 (37%) received treatment intensification and 26 (63%) a standard dose (ILD = 120 ± 20 Gy, not exceeding 150 Gy). In 2 standard-dose cases, treatment intensification was warranted yet impossible because of the HILD. The lung dose was not found to constitute a limit on intensification.
For the entire patient cohort, the mean injected activity was 3.1 ± 1.5 GBq, and mean ILD was 143 ± 49 Gy.
For the treatment-intensification patients, the mean injected activity increase was 58% ± 39%, resulting in a mean ILD of 187 ± 49 Gy and a mean HILD of 85% ± 25% (Table 2).
Treatment-Intensification Patients (n = 15), Baseline Characteristics, Percentage of Intensification, Dosimetry, and Response
Of the treatment-intensification patients, 47% received the intensified treatment because of a predicted TD—when using the standard dosimetric approach (120 Gy to the treated lobe)—that should have been below 205 Gy; 40% because of a predicted TD between 205 and 250 Gy; and 13% despite a provisional TD greater than 250 Gy.
The response rate of treated lesions according to the criteria of the European Association for the Study of the Liver was 85%, with 5 patients showing a complete response, 30 a partial response, and 6 stable disease. The response rate was 81% for patients who received intensification and 88% for those who did not (not statistically significant), with a rate of 91% observed for those with lesions measuring at least 10 cm (n = 12). Five patients exhibiting good response and complete portal vein revascularization, including one with main PVT (Fig. 1), underwent wide hepatectomy. Complete resection (R0) was achieved for all patients, although residual tumoral areas were revealed on microscopic examination in all patient tumors and in the portal veins of two. At the time of evaluation, 2 patients had died of disease progression and the remaining 3 were still alive with recurrence.
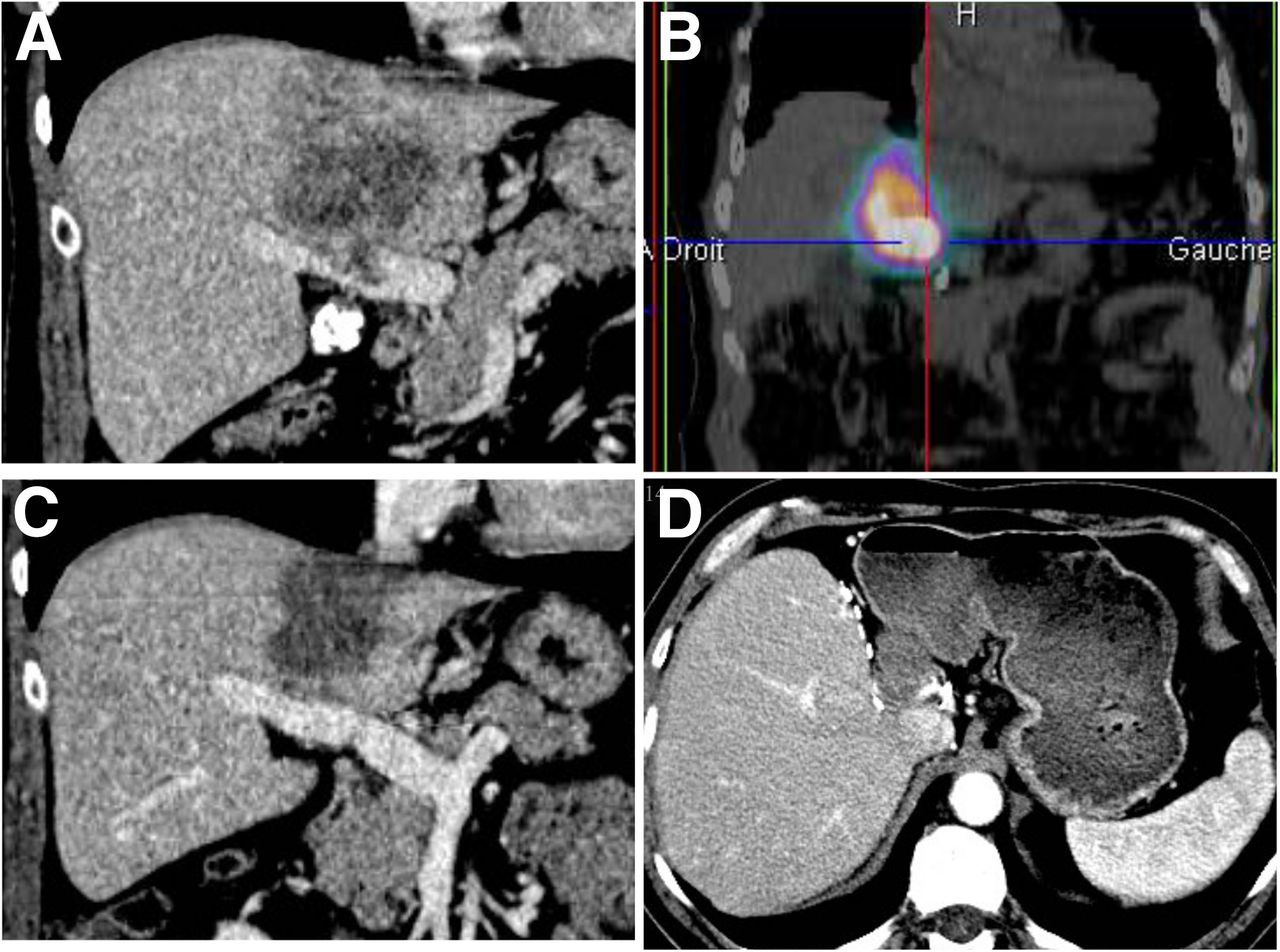
A 62-y-old patient with large hepatocellular carcinoma and main PVT with major response and prolonged OS after revascularization of portal vein. (A) Initial CT slice, showing infiltrative 9.6-cm hepatocellular carcinoma with main PVT. (B) 99mTc-MAA SPECT/CT with high uptake in tumor and main PVT. Using standard approach, only 0.56 GBq of 90Y-loaded glass microspheres should have been used to achieve ILD of 120 Gy (TD should have been only 162 Gy and HILD 37 Gy). Treatment was then intensified to twice the standard activity (1.16 GBq; ILD was 211 Gy, TD 285 Gy, and HILD 65 Gy). (C) CT slices 6 wk after injection: partial response of tumor (according to criteria of European Association for Study of Liver) and main portal vein revascularization. Patient subsequently underwent left hepatectomy (with complete tumoral resection). PFS was 15 mo, with lung recurrence only. (D) Patient was still alive at 36.2 mo, with still only lung recurrence and no liver recurrence.
Three patients with treated-lesion response showed progression at 3 mo in areas outside the treated liver, 1 with contralateral progression and 2 with distant progression.
Using univariate analysis, only 2 factors were associated with response of the treated lesions according to the criteria of the European Association for the Study of the Liver: a TD of 205 Gy or more (P = 0.0183) and tumor-to-nontumor ratio (P = 0.0028), with a mean of 7.8 for responders and only 2.8 for nonresponders. None of these parameters continued to prove significant when evaluated on multivariate analysis (Supplemental Table 1, available at http://jnm.snmjournals.org).
The response of treated lesions according to the Response Evaluation Criteria in Solid Tumors was available for 40 patients and unavailable for 1 patient, who exhibited a diffuse poorly delineated hepatocellular carcinoma. The response rate was only 42%, with 15 partial responses and 35 cases of stable disease.
An evaluation of α-fetoprotein response was available for 19 of the 20 patients with an α-fetoprotein level of more than 200 kIU/L. The response rate was 78.9%, with 15 partial responses, 1 case of stable disease, and 3 cases of progressive disease (contralateral liver, n = 1; distant metastases, n = 2).
Four cases of clinically relevant and permanent liver toxicity of grade 3 or higher were encountered (liver decompensation with abundant ascites), 1 in the intensified group (6%) and 3 in the conventional-dose group (12%). The difference was nonsignificant. Decompensation began within 6 wk, worsening until inducing death in all 4 patients. Each had a Child–Pugh score of A5 at baseline, transaminases lower than 5-fold normal value, and normal bilirubin values, with the exception of 1 patient with a value of 34 μmol/mL. All 4 patients with liver toxicity exhibited poor 99mTc-MAA targeting of the PVT (3 main, 1 branch). PVT targeting was the only tested parameter that was associated with liver toxicity on univariate analysis (P < 0.0001). Other nonsignificant factors tested were α-fetoprotein level, treatment line (first-line vs. ≥second-line), bilirubin level (< or ≥34 μmol/mL), alanine aminotransferase level (< or ≥5N), Child–Pugh score (A5 or A6/B7), tumor involvement (< or ≥50%), hepatic reserve (percentage of nonirradiated liver, < or ≥30%), HILD, and a combination of HILD (≥40, 60, 80, 100, and 120 Gy) and hepatic reserve less than 30%.
For all 41 patients, the median PFS and OS were 9 mo (95% confidence interval [CI], 6–11 mo) and 18 mo (95% CI, 11–24.5 mo), respectively. Median PFS and OS have been presented in relation to several parameters in Table 3.
Factors Associated with PFS and OS (with Univariate Analysis)
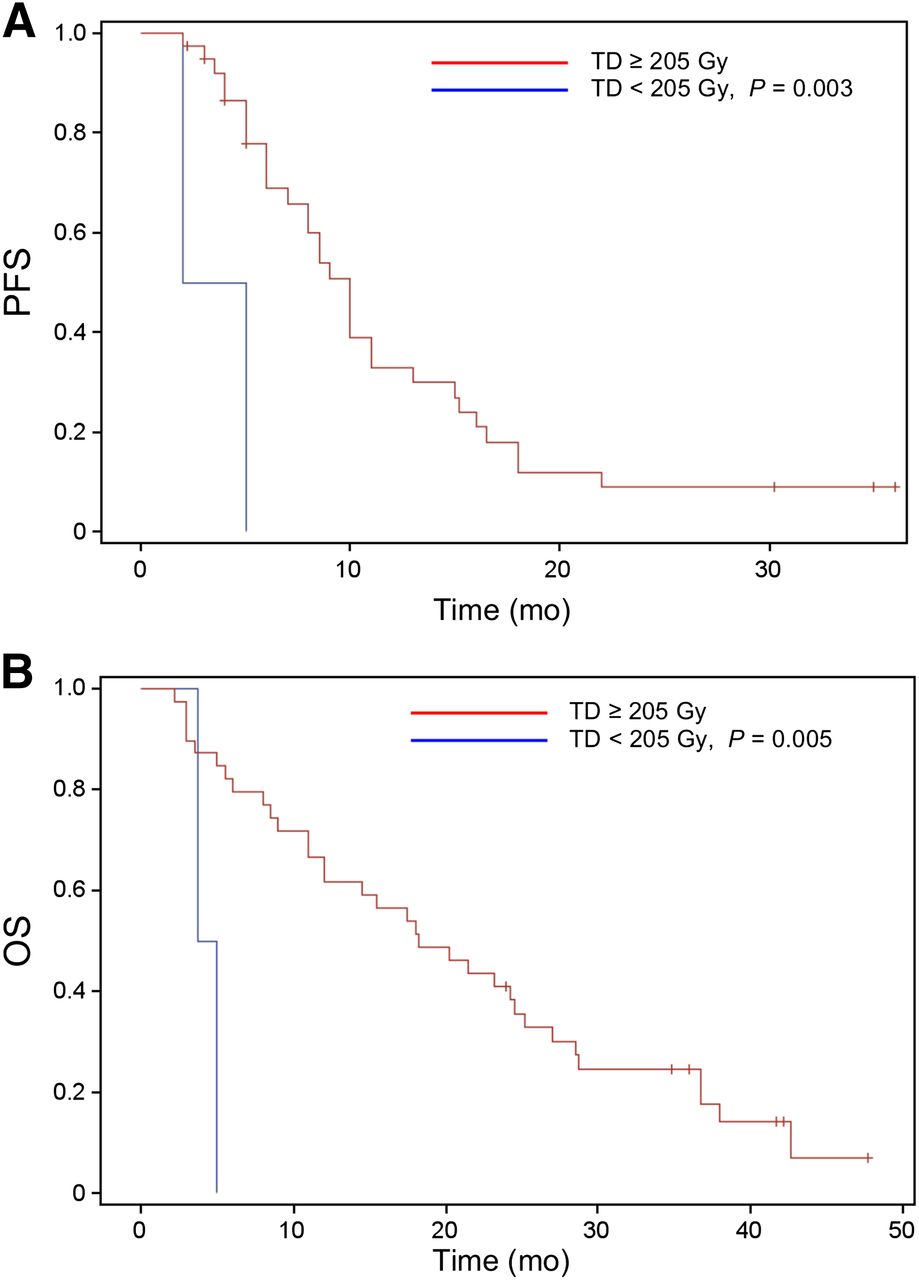
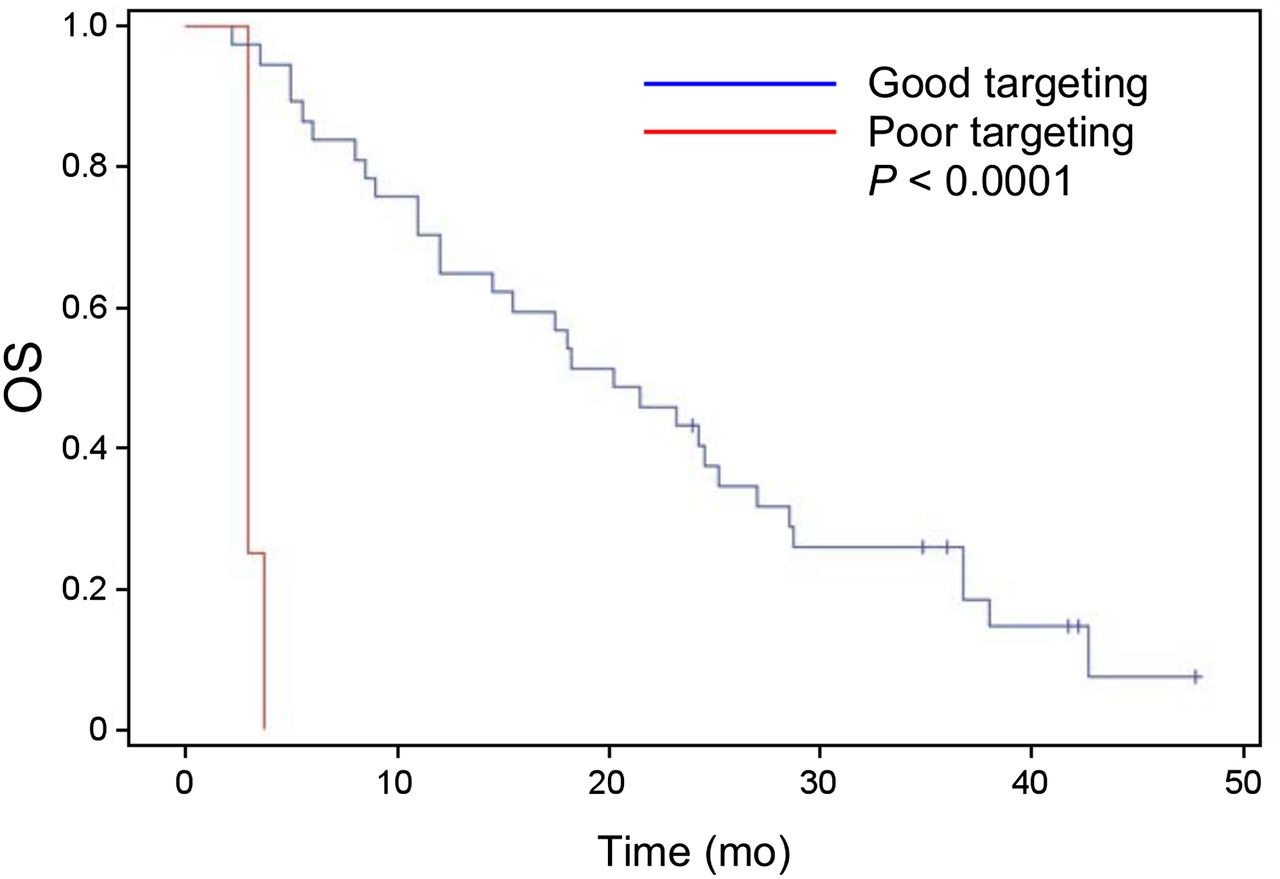
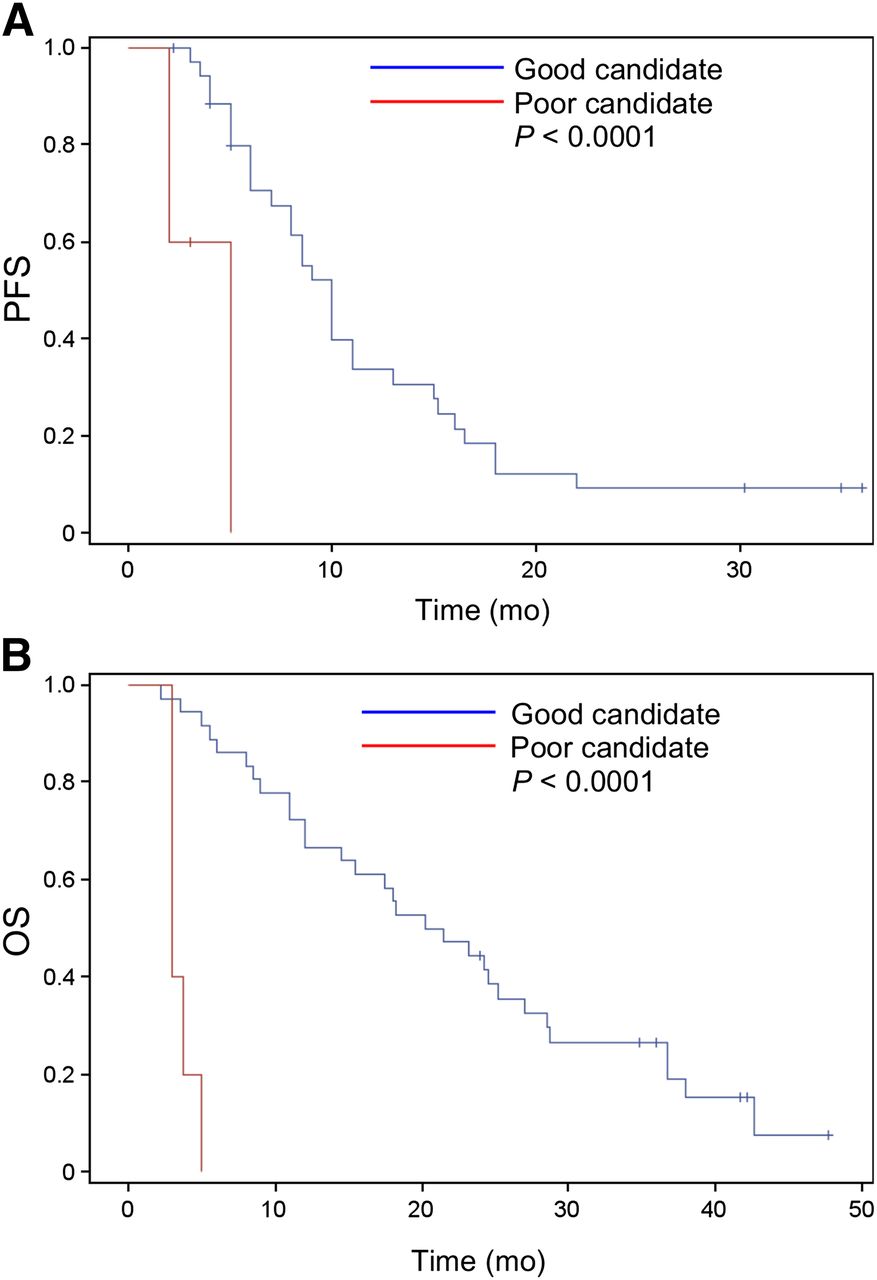
PFS was found to significantly correlate with TD, α-fetoprotein, Eastern Cooperative Oncology Group status, and good or poor candidate status, with the last defined as patients with a TD of 205 Gy or more and good PVT targeting or a TD of less than 205 Gy and poor PVT targeting, respectively. A highly significant correlation was found between OS and TD (< versus ≥205 Gy, P = 0.005, Fig. 2) and PVT targeting (good vs. poor, P < 0.0001, Fig. 3), as well as with good or poor candidate status (P < 0.0001, Fig. 4). A significant correlation was found between OS and Child–Pugh status (A5 vs. A6, and B7) (P = 0.015). OS was significantly higher for patients who underwent lobar hepatectomy than for those who did not, not reached (yet exceeding 24.5 mo) versus 15 mo, respectively (P = 0.0493, Fig. 5). Finally, OS did not statistically differ between main or branch/segmental PVT.

Kaplan–Meyer estimates of PFS (A) and OS (B) stratified by TD.

Kaplan–Meyer estimates of OS stratified by PVT targeting (good, n = 37; poor, n = 4).
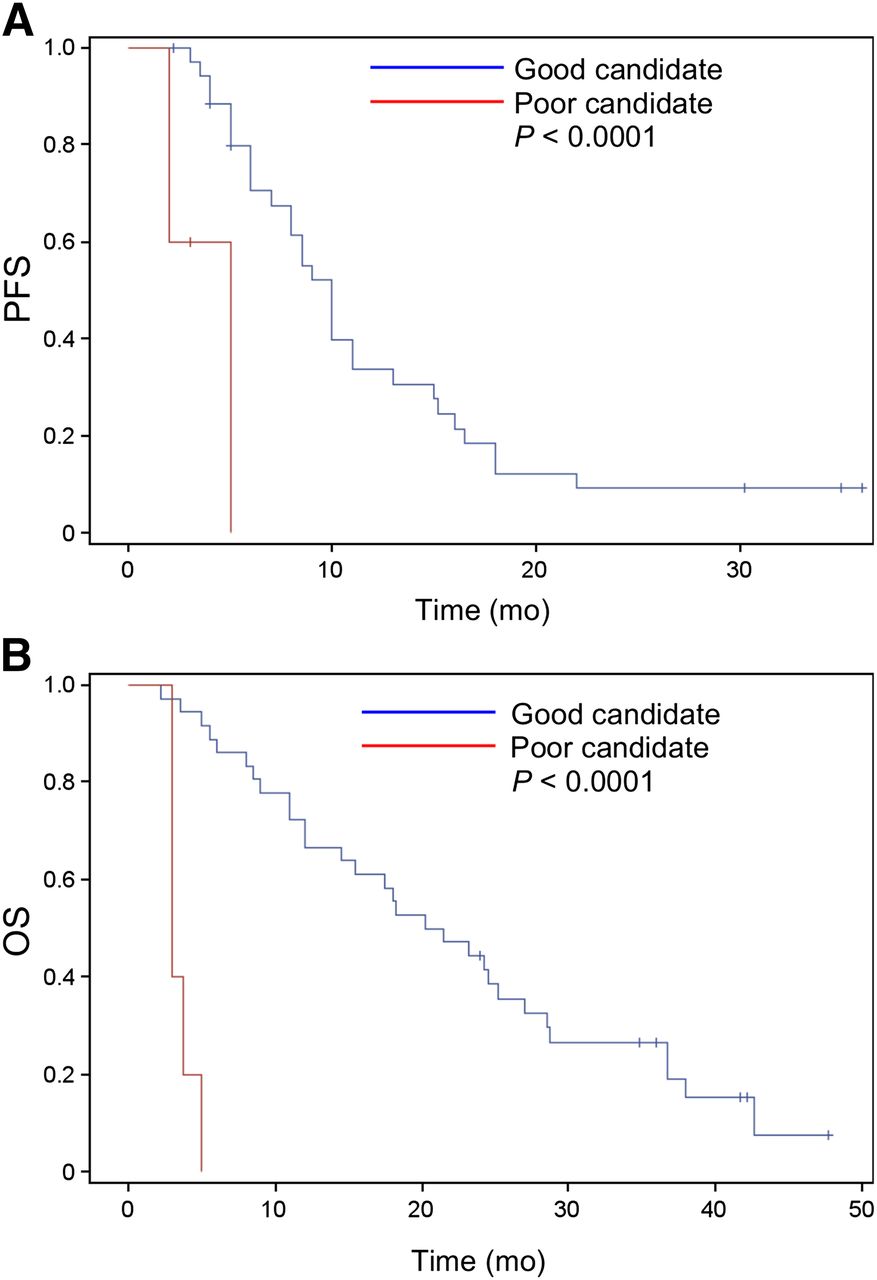
Kaplan–Meyer estimates of PFS (A) and OS (B) for poor (n = 5) or good (n = 36) candidates for radioembolization.
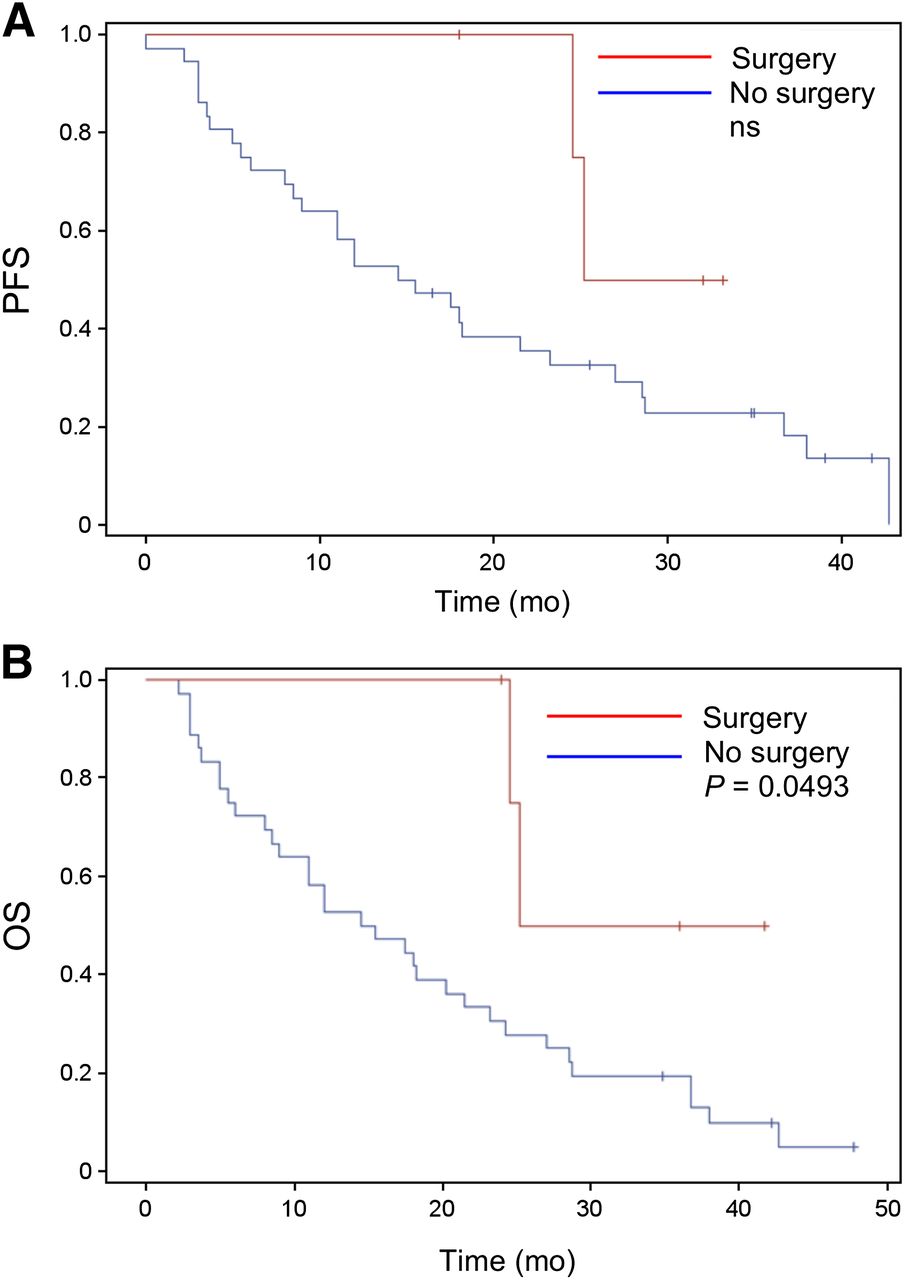
Kaplan–Meyer estimates of PFS (A) and OS (B) stratified by surgery.
DISCUSSION
The radio-induced tumoricidal effect has been found to respond to the determinist rule, with a minimum absorbed TD necessary to induce response (tumoral threshold dose).
To date, 2 independent teams have described this dose–response relationship in the context of hepatocellular carcinoma with a clear tumoral threshold dose identification, based on 99mTc-MAA scintigraphy, while using 90Y-loaded glass microspheres (10–12). By applying a biologically effective dose and a voxel approach, Chiesa et al. were the first to describe a dose–response relationship, with a tumoral threshold dose of 257 Gy (10). Using a simple MIRD approach and mean dose evaluation, we also described a tumoral threshold dose of 205 Gy, with sensitivity and accuracy in the prediction of response of 100% and 91%, respectively (11). TD has been described as the only predictive parameter of response on multivariate analysis (12).
More recently, posttherapeutic dosimetry has also identified a clear dose–response relationship (14) in hepatocellular carcinoma patients treated with 90Y-loaded glass microspheres, thus confirming the significant relevance of TD.
99mTc-MAA SPECT/CT–based dosimetry is, however, the only technique currently available that can be performed before microsphere injection, thus allowing for modification of treatment schedule, such as a personalized dosimetric approach with intensification in cases of low TD. We recently described this approach, comprising personalized dosimetry and intensification at the lobar level, with interesting results (79% response rate) in an unselected cohort of hepatocellular carcinoma patients (12). Using this approach, we found no evident correlation between tumor size and response (12). This finding is highly relevant, as tumor size has been recognized as a critical parameter related to response using radioembolization with no personalized dosimetric approach. Previous studies have reported significant decreases in response rate as tumor size increased (7,15). With the application of standard radioembolization, the complete histologic response rate was 89% for lesions smaller than 3 cm and only 33% for lesions larger than 5 cm (15). In another study, the morphologic response rate was 82% for lesions smaller than 5 cm, 17.6% for those between 5 and 10 cm, and only 2% for those larger than 10 cm (7). This point underlines the fact that intensification should be considered for large lesions. Riaz et al. have also previously described an intensification approach at a segmental level called radiation segmentectomy, producing good results (81% response rate; no clinical toxicity) and thus underlining the usefulness of the intensification concept (16,17). Recent results by means of radiation segmentectomy have demonstrated that the rate of complete histologic response was significantly higher for segments receiving a mean dose of 190 Gy or more (i.e., 66.6% for a segment dose ≥ 190 Gy, compared with only 25% for a segment dose < 190 Gy; P = 0.03) (17). TDs were not provided in that study, thus rendering any direct comparison with our threshold TD of 205 Gy impossible. Nevertheless, the study brings to light new evidence of the dose–response relationship observed with radioembolization. It also demonstrates that intensification at a segmental level for small lesions (median size, 2.6 cm) can be performed in an uncomplicated manner (not requiring evaluation of the TD), producing good clinical results (safety and response rate of 86%), with the objective of delivering a threshold dose of 190 Gy to the segment. Interestingly, the mean ILD of our intensified patients was in the same range, namely 187 Gy.
As PVT patients often present with large lesions, and because of the existence of PVT itself, lobar intensification seemed particularly worth investigating in this selected patient cohort. In this study, intensification was applied in 37% of cases. For intensification, our primary endpoint was to achieve a TD of at least 205 Gy, namely the threshold TD that had already been identified (11,12). We had previously observed (12) that the response rate was higher for patients with a TD of more than 275 Gy, in comparison with patients with a TD of 205–275 Gy. Intensification was therefore also performed for some patients with a predicted TD of more than 205 Gy (as predicted using the standard dosimetric approach), with a little over 50% of intensified patients thus concerned. We might wonder if an interesting endpoint of intensification could be reaching the maximal tolerated dose to the healthy injected liver. One difficulty with this hypothesis is the fact that this maximal tolerated dose is not well defined with radioembolization, especially for cirrhotic patients, and we currently do not know up to which level we can intensify treatment. For these reasons, we conservatively decided to not use, as an endpoint, reaching of any potential maximal tolerated dose.
Nevertheless, using this concept of intensification, we obtained a high response rate (85%) in this cohort of PVT patients with large lesions (mean tumor size, 8.5 ± 3.1 cm). Once again, we observed that TD clearly affected the response rate, as previously described (10–12). Achieving high response rates is a crucial goal that has been associated with extended OS (7,18), especially in PVT patients, with responders exhibiting a 3-y survival rate of 25%, compared with only 4.4% for nonresponders (P = 0.02) (7). In line with previous findings (11,12), we saw no evident correlation between response and size, and we observed a high response rate (91%) for patients with lesions measuring 10 cm or more. This finding demonstrates that, with a controlled TD (using a personalized dosimetric approach and intensification), we were able to restore, at least partially, the prognosis of patients with large lesions. An additional interesting finding was that PFS and OS also strongly correlated with TD, with a median OS of only 4.3 mo (95% CI, 3.7–5 mo) for a TD of less than 205 Gy, compared with 18.2 mo (95% CI, 8.5–28.7 mo) for a TD of 205 Gy or more (P = 0.005).
The other parameter that strongly correlated with OS in our study was PVT targeting. The 4 patients who underwent no 99mTc-MAA PVT targeting exhibited severe acute liver toxicity leading to death. One explanation is that radioembolization induces transient portal hypertension (19), which can be poorly tolerated by PVT patients who present with poor liver function and no accurate treatment of PVT because of the absence of targeting. The median OS was only 3 mo (95% CI, 3–3.7 mo) for patients with poor PVT targeting, compared with 20.2 mo (95% CI, 12–25.1 mo) for those with good PVT targeting (P < 0.0001). Interestingly, we found that PVT location (main vs. branch/segmental) was not statistically related to OS. This finding is also of significant interest since patients with main PVT are often considered poor candidates for radioembolization or the procedure may be considered contraindicated in these cases. In reality, the key parameter for PVT is 99mTc-MAA targeting and not PVT location. Thus, irrespective of PVT location, radioembolization should be considered and PVT targeting evaluated. Only poor PVT targeting should be considered a contraindication.
In this study, using intensification did not increase liver toxicity. The rate of severe and permanent hepatic toxicity was no higher in intensified patients (6%) than in those treated with the standard approach (12%). The only parameter found to strongly correlate with liver toxicity was the presence of main or branch PVT without 99mTc-MAA targeting. No patient exhibited a combination of small hepatic reserve (<30%) with a HILD of more than 120 Gy, which represented a previously identified liver toxicity factor (12). It is for this reason that 2 patients did not receive intensification, given that the process would have induced this at-risk situation.
In this group of patients treated with a personalized dosimetric approach and intensification when necessary, the global median OS was 18 mo, regardless of TD or PVT targeting. Such a prolonged OS in nonselected PVT patients has never previously been described, whether using radioembolization with a standard dosimetric approach or sorafenib. Previous studies have, in fact, reported a median OS of between 6.4 and 13 mo for PVT patients using glass or resin microspheres (6–10), which contrasts with values of only 6.5–8.1 mo with sorafenib (4,9).
Child–Pugh A and lobar PVT patients appeared good candidates for radioembolization in our study, with a median OS of 23.3 mo (95% CI, 8–23.7 mo). A relatively long median OS ranging between 15.7 and 17 mo has also been described in this type of patient subgroup in other studies (5,7,20), thus emphasizing the particular interest of radioembolization in this context.
The median OS was 20.9 mo for good radioembolization candidates identified before therapy, namely patients with both a TD higher than 205 Gy and good PVT targeting.
Lastly, OS was not attained for patients who underwent surgery, though it did exceed 24.5 mo and was significantly longer in these patients than in those who did not undergo surgery (15 mo, P = 0.0493), underlining the potential interest in surgery for PVT patients exhibiting a good response to radioembolization.
The results of our study were observed with glass microspheres on day 3, after calibration, applying a specific activity of approximately 1,250 Bq/sphere. A recent simulation (21) has demonstrated that the specific activity of microspheres is hugely influential from a radiologic point of view, with lower radiobiologic effects observed with high specific activity because of the more heterogeneous distribution of radiation. Lewandowski et al. (22) proposed using glass microspheres on week 2, typically 8 d after calibration, with a lower specific activity of approximately 393 Bq/sphere. This technique has been shown to provide good clinical results, with a high response rate (57%) and a low hepatic toxicity profile (2% of grade 3/4 bilirubin toxicity). This approach also provides a good opportunity to optimize glass microsphere radioembolization. The use of glass microspheres with an extended shelf-life, combined with a personalized dosimetric approach, could be a promising method for further improving therapeutic effectiveness. New tumoral threshold dose values and maximal HILD values will, however, have to be defined for the use of glass microspheres with a specific activity of 393 Bq/sphere.
To our knowledge, only a single retrospective nonrandomized study has to date sought to compare sorafenib and 90Y-loaded resin microsphere radioembolization (9). No statistical difference in OS was identified between the therapeutic options (8.6 mo for sorafenib vs. 6.4 mo for resin microsphere radioembolization, P = 0.879). Nevertheless, this study’s findings should be interpreted with caution, given the major bias against radioembolization that was present (9). The body-surface-area method was used for activity calculation, despite the fact that the partition method is now the technique preferred by several experts (23,24). Moreover, some patients were treated with radioembolization despite presenting with inappropriately high lung shunting, leading to death, and no personalized dosimetric approach used.
The main drawback of this study was its retrospective and uncontrolled nature. Despite the valuable data it has provided regarding the potential use of radioembolization in PVT patients, as in other trials, further randomized studies are still warranted.
CONCLUSION
Radioembolization using a 99mTc-MAA SPECT/CT personalized dosimetry and intensification concept with 90Y-loaded glass microspheres offers a fully customized oncologic therapeutic option. This option appears to be of particular interest in PVT patients, as it induces prolonged OS without increasing liver toxicity. TD and PVT targeting are the most relevant parameters to control to achieve good clinical results, even in main-PVT cases. Surgery was performed on 12.2 % of the patients, achieving significantly higher OS. Prospective randomized studies are therefore now warranted to clearly define the application of this new personalized therapeutic approach.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Etienne Garin is a consultant for BTG and has received lecture fees from Bayer. Jean-Luc Raoul is a consultant for Bayer. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Feb. 12, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 4, 2014.
- Accepted for publication December 4, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-Term Overall Survival After Selective Internal Radiation Therapy for Locally Advanced Hepatocellular Carcinomas: Updated Analysis of DOSISPHERE-01 Trial
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Lung Shunt Reduction for Yttrium-90 Radioembolization: Chemoembolization Versus Radioembolization
- Yttrium-90 Radioembolization for Hepatocellular Carcinoma: Virtual Tumor Absorbed Dose as a Predictor of Complete Response
- First-Line Selective Internal Radiation Therapy in Patients with Uveal Melanoma Metastatic to the Liver
- 90Y Radioembolization for Locally Advanced Hepatocellular Carcinoma with Portal Vein Thrombosis: Long-Term Outcomes in a 185-Patient Cohort
- Intraarterial Hepatic SPECT/CT Imaging Using 99mTc-Macroaggregated Albumin in Preparation for Radioembolization
- 90Y Hepatic Radioembolization: An Update on Current Practice and Recent Developments