


Abstract
This was a study to compare the diagnostic efficacies of endoscopic ultrasonography (EUS), CT, PET/MR imaging, and PET/CT for the preoperative local and regional staging of esophageal cancer, with postoperative pathologic stage used as the reference standard. Methods: During 1 y, 19 patients with resectable esophageal cancer were enrolled and underwent preoperative EUS, CT, PET/CT, and PET/MR imaging. A chest radiologist and nuclear medicine physician retrospectively reviewed the images and assigned tumor and lymph node stages according to the seventh version of the TNM system and the American Joint Committee on Cancer staging system. Four patients who were treated nonsurgically were excluded from data analysis. The efficacies of EUS, CT, PET/CT, and PET/MR imaging were compared. Results: Primary tumors were correctly staged in 13 (86.7%), 10 (66.7%), and 5 (33.3%) patients at EUS, PET/MR imaging, and CT, respectively (P value ranging from 0.021 to 0.375). The accuracy of determining T1 lesions was 86.7%, 80.0%, and 46.7% for EUS, PET/MR imaging, and CT, respectively. For distinguishing T3 lesions, the accuracy was 93.3% for EUS and 86.7% for both PET/MR imaging and CT. For lymph node staging, the accuracy was 83.3%, 75.0%, 66.7%, and 50.0% for PET/MR imaging, EUS, PET/CT, and CT, respectively. In addition, area-under-the-curve values were 0.800, 0.700, 0.629, and 0.543 for PET/MR imaging, EUS, PET/CT, and CT, respectively. Conclusion: PET/MR imaging demonstrated acceptable accuracy for T staging compared with EUS and, although not statistically significant, even higher accuracy than EUS and PET/CT for prediction of N staging. With adjustments in protocols, PET/MR imaging may provide an important role in preoperative esophageal cancer staging in the future.
Accurate staging of esophageal cancer is critical for decisions on patient treatment. Current practice guidelines for the staging of esophageal cancer include CT of the chest and abdomen, endoscopic ultrasonography (EUS), and PET/CT (1). EUS is a relatively accurate modality for evaluating primary tumor depth compared with CT, which cannot identify the histologic layers of the esophageal wall; thus, the role of CT is usually limited to exclusion of T4 cancers (2,3).
Considering nodal metastasis, CT scans, which depend on size criteria, have relatively poor diagnostic performance, as enlarged lymph nodes may be reactive and normal-sized lymph nodes may be positive for metastasis (4,5). Currently, a combination of EUS with or without fine-needle aspiration and PET/CT is widely accepted for assessment of nodal metastasis (1). However, certain lymph nodes that are not immediately adjacent to the esophagus could be dismissed, and the EUS probes, which are typically larger than standard endoscopic probes, are not feasible if the lumen has been narrowed by a large tumor or stricture. PET/CT supports the role of EUS and CT because the maximum standardized uptake value helps identify patients with T1 cancers and pathologic lymph nodes, but the diagnostic accuracy still remains unsatisfactory (5–7).
The recently available hybrid modality PET/MR imaging allows combination of both metabolic and anatomic information about the cancer (8–10). PET/MR imaging is a rapidly evolving modality whose full potential has yet to be discovered and whose diagnostic utility in esophageal cancer has yet to be addressed in the literature. Therefore, the purpose of our study was to compare the diagnostic efficacies of EUS, CT, PET/CT, and PET/MR imaging for the preoperative local and regional staging of esophageal cancer, with postoperative pathologic stage used as the reference standard.
MATERIALS AND METHODS
Our institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
Patient Enrollment
From January 2012 to August 2013, 19 patients newly diagnosed with esophageal cancer were prospectively enrolled in this study. Esophageal cancer was diagnosed by pathologic confirmation, and none of the patients had a history of previous malignancy. All were eligible for surgery and underwent a preoperative staging protocol that included EUS, contrast-enhanced chest CT, and PET/CT. All had an impression of malignancy from previous endoscopy and biopsy results performed at outside hospitals and had been referred to our hospital, a tertiary referral hospital with a comprehensive cancer center. After distant metastasis had been excluded by contrast-enhanced CT and PET/CT, the patients underwent EUS for locoregional staging. In addition, PET/MR imaging was performed. EUS and all imaging took place within 2 wk before surgery.
Image Acquisition
Chest CT was performed using a 64-detector scanner (Discovery 750HD CT; GE Healthcare) with the following parameters: 0.625-mm detector collimation, 120 kVp, 100–250 mA, and 2-mm reconstruction interval. Contrast material (100 mL) was injected at a rate of 2 mL/s, and scanning was performed from the supraclavicular area to the adrenal glands. Images were directly displayed on the monitors of a PACS (M-view; Infinitt).
18F-FDG PET/CT was performed using a combined PET/CT scanner (Gemini; Philips) consisting of a dedicated germanium oxyorthosilicate detector, a full-ring PET scanner, and a dual-slice helical CT scanner. Images were obtained from the skull base to the proximal thighs 60 min after intravenous administration of a 3.7 MBq/kg dose of 18F-FDG. Low-dose CT (30 mAs, 120 kVp) without contrast material was performed, and PET data were reconstructed iteratively with attenuation correction and reoriented in axial, sagittal, and coronal slices. Meanwhile, 18F-FDG PET/MR images were obtained with a sequential-acquisition PET/MR system (Ingenuity TF; Philips Healthcare), which combines a time-of-flight PET scanner and 3-T MR imaging, similar to the standard PET/CT workflow. PET images were acquired first, followed by diagnostic MR scans. PET scans from the top of the head to the thighs were obtained 60 min after intravenous injection of a 3.7 MBq/kg dose of 18F-FDG, with a dedicated MR protocol for MR-based attenuation correction (11,12). PET images were reconstructed using 3-dimensional time-of-flight ordered-subsets expectation maximization incorporating an MR-based attenuation map with 3 segments: air, lung, and soft tissue (11–13). Diagnostic MR imaging was performed from the lower neck to the mid-kidney level and consisted of axial and sagittal breath-hold T2-weighted images, with a slice thickness of 5 mm and an axial THRIVE (T1 high-resolution isotropic volume excitation) unenhanced sequence of 2-mm thickness. Contrast agent was not applied. The average acquisition time for PET/MR was 40 min. PET data were reconstructed with attenuation correction, and fusion was performed for the T1-weighted images in axial, sagittal, and coronal slices. Both PET/CT and PET/MR images were displayed on a workstation (Extended Brilliance Workstation; Philips).
EUS examination was performed with a radial echoendoscope (GF-UM2000 or UM-DP20–25R; Olympus) at frequencies of 7.5, 12, or 20 MHz. All patients allowed passage of the echoendoscope through the esophagus, stomach, and duodenum.
Image Interpretation
Two chest radiologists and 2 nuclear medicine physicians retrospectively reviewed the images and, in consensus, assigned tumor and lymph node stages according to the seventh version of the TNM system and the American Joint Committee on Cancer staging system. Tumor staging was based on depth through the esophageal wall and involvement of periesophageal fat or surrounding organs. Unenhanced PET/CT scans preclude information about esophageal wall layers and therefore were excluded from T-staging analyses.
In cases of nodal staging, all 4 imaging modalities—EUS, CT, PET/CT, and PET/MR imaging—were included for analyses. For CT scans, lymph nodes were evaluated for size and necrosis: a short-axis diameter of more than 10 mm was defined as abnormal, and the presence of necrosis within a lymph node was classified as abnormal, irrespective of its size. When lymph nodes contained laminated or nodular calcification, they were regarded as benign. A region of interest was drawn manually on axial images that had uptake higher than the physiologic background level to obtain the maximum standardized uptake value, and a value of more than 2.5 on PET/CT images determined nodal metastasis. For PET/MR scans, lymph nodes with a maximum standardized uptake value of more than 2.5 or with eccentric cortical thickening or obliteration of the fatty hilum were considered abnormal, regardless of their size.
Standard Reference and Image Correlation
Esophagectomy and gastric pull-up with total 2-field lymph node dissection was performed on all patients by an experienced thoracic surgeon. Esophagogastrostomy was done in the chest (Ivor Lewis operation) or neck (McKeown operation) according to the location of esophageal cancer. The results of T and N staging were compared with those of pathologic staging. For the detection of lymph node metastasis, imaging findings and pathologic results were correlated on a per-nodal-station basis.
Statistical Analyses
Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated for T and N staging using standard definitions. We also conducted separate analyses for T1, T2, and T3 cancer. Differences in accuracy between modalities were determined using the McNemar test. In addition, receiver-operating-characteristic curve analyses were assessed between modalities for N staging. For statistical analysis, SPSS for Windows (Microsoft) software (version 18.0; SPSS) and MedCalc (version 12.7.5; MedCalc) were used, and a P value of less than 0.05 indicated statistical significance.
RESULTS
Clinical Features
All patients were eligible for surgery at preoperative staging, but 4 patients who did not undergo a final operation were excluded from data analysis: 3 underwent concurrent chemoradiation treatment because of comorbid conditions, and 1 elderly patient refused surgical resection. Among the final study group of 15 patients who underwent surgery, all were men and their mean age was 68.1 ± 7 y. Most tumors were in the middle (n = 8, 53.3%) or lower (n = 4, 26.7%) esophagus. All patients had squamous cell carcinoma, with moderately differentiated tumors being the predominant histologic type (n = 10, 66.7%) (Table 1). Figure 1 shows a representative case of esophageal cancer.
Patient Characteristics
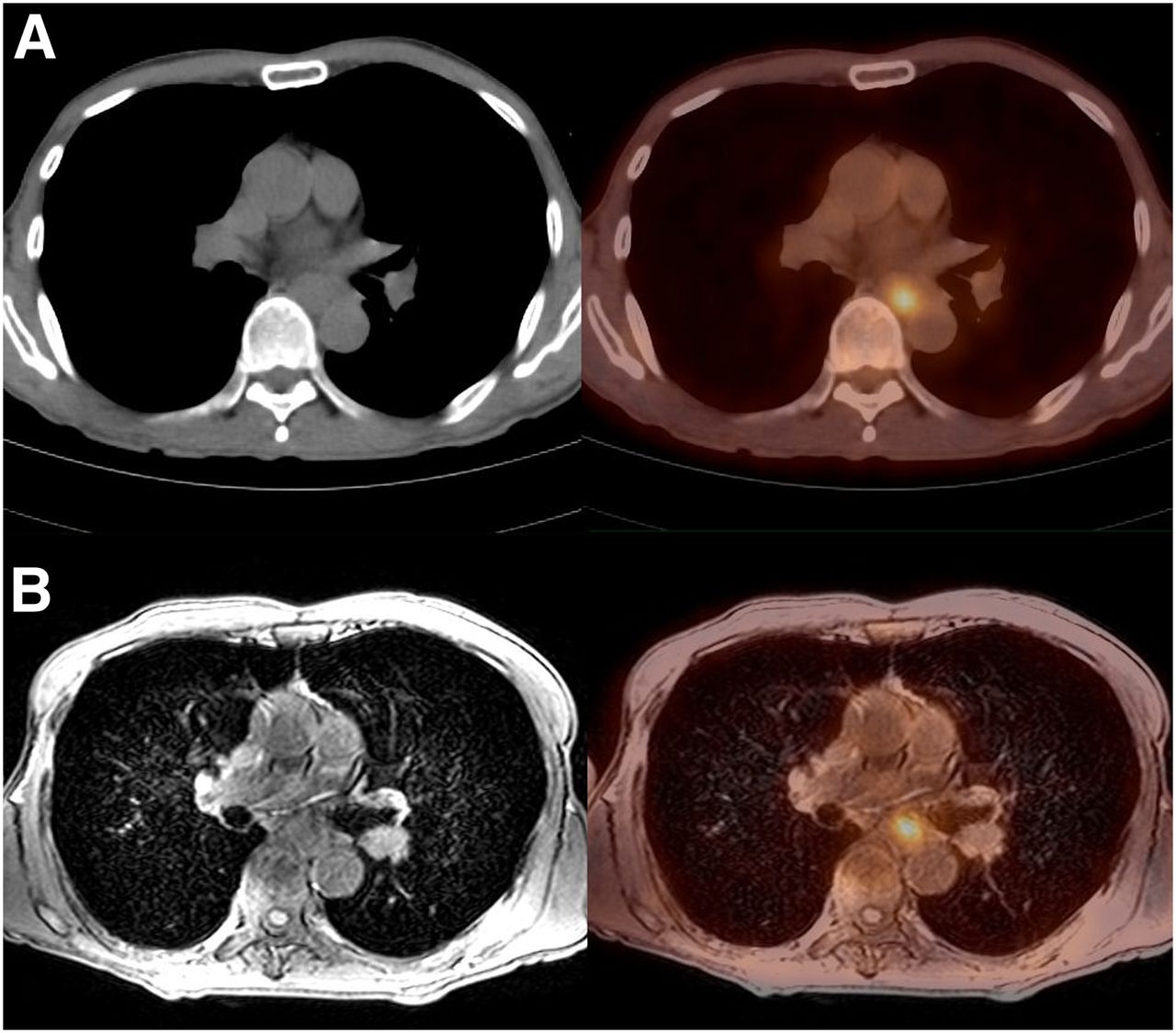
18F-FDG PET/CT (A) and PET/MR (B) images of representative case of esophageal cancer (patient 10, 63-y-old man). On PET/MR image, T stage was interpreted as T3. Pathologic diagnosis was squamous cell carcinoma, and pathologic stage was pT3N1M0 and IIIA.
Seven patients (46.7%) underwent the Ivor-Lewis operation, and the others underwent the Ivor-Lewis hybrid operation (n = 2, 13.3%), the 3-hole operation (n = 2, 13.3%), the 3-hole hybrid operation (n = 2, 13.3%), transhiatal esophagectomy (n = 1, 6.7%), or esophagocolojejunostomy (n = 1, 6.7%). All patients underwent total 2-field lymph node dissection.
T Staging
A comparison of T and N staging at PET/MR imaging, EUS, CT, and PET/CT with pathologic standards for all 15 patients is presented in Table 2.
Comparison of T and N Staging
As verified by pathologic standards, there was T1 cancer in 9 patients, T2 cancer in 2 patients, and T3 cancer in 4 patients (Table 3). The primary tumor was correctly staged in 13 (86.7%), 10 (66.7%), and 5 (33.3%) patients at EUS, PET/MR imaging, and CT, respectively. Although only the difference in accuracy between EUS and CT (P = 0.021) was statistically significant, the difference between PET/MR imaging and CT (P = 0.063) closely approached significance. The difference between EUS and PET/MR imaging did not (P = 0.375) (Table 4).
Detection of Primary Tumor: Comparison with Pathology
Diagnostic Accuracy for Primary Tumor Staging
For EUS, PET/MR imaging, and CT, accuracy was 86.7%, 80.0%, and 46.7%, respectively, for distinguishing T1 lesions; 86.7%, 73.3%, and 53.3%, respectively, for distinguishing T2 lesions; and 93.3%, 86.7%, and 86.7%, respectively, for distinguishing T3 lesions (Table 4).
N Staging
During correlation between per-nodal-station imaging findings and pathologic results, 3 patients were further excluded (Table 2). They had imaging findings of lymph node metastases at the 2R or 4R nodal stations, but these stations had not undergone dissection during the Ivor-Lewis operation. In other words, pathologic reference standards were not available for some suggestive lymph nodes in the 3 patients, who were therefore excluded from N-staging data analyses.
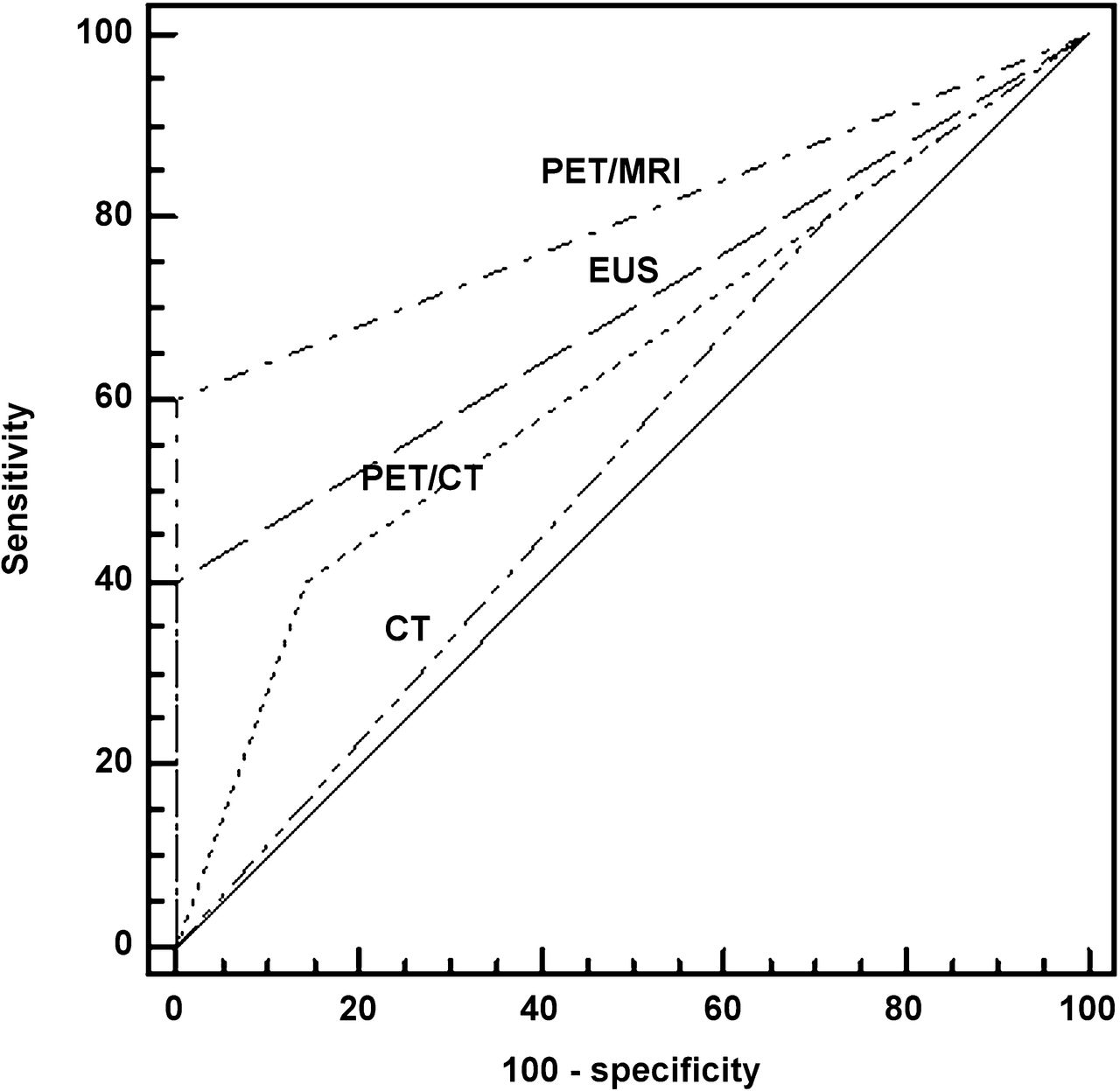
Of the 12 patients who had pathologic reference standards for 106 nodal stations, 7 patients had stage N0 and 5 patients had stage N1. Nodal metastasis was correctly staged in 10 (83.3%), 9 (75.0%), 8 (66.7%), and 6 (50.0%) patients at PET/MR imaging, EUS, PET/CT, and CT, respectively (P > 0.99 for all) (Table 5). The results of receiver-operating-characteristic curve analysis for efficacy in diagnosing nodal metastasis demonstrated area-under-the-curve values of 0.800, 0.700, 0.629, and 0.543 for PET/MR imaging, EUS, PET/CT, and CT, respectively (Fig. 2). Although the area-under-the-curve value of PET/MR imaging was higher than those of EUS, PET/CT, and CT, there were no statistical differences among the 4 modalities (P = 0.476, 0.656, 0.218, 0.761, 0.593, and 0.163 for CT vs. EUS, CT vs. PET/CT, CT vs. PET/MR imaging, EUS vs. PET/CT, EUS vs. PET/MR imaging, and PET/CT vs. PET/MR imaging, respectively).
Detection of Nodal Metastasis: Comparison with Pathology
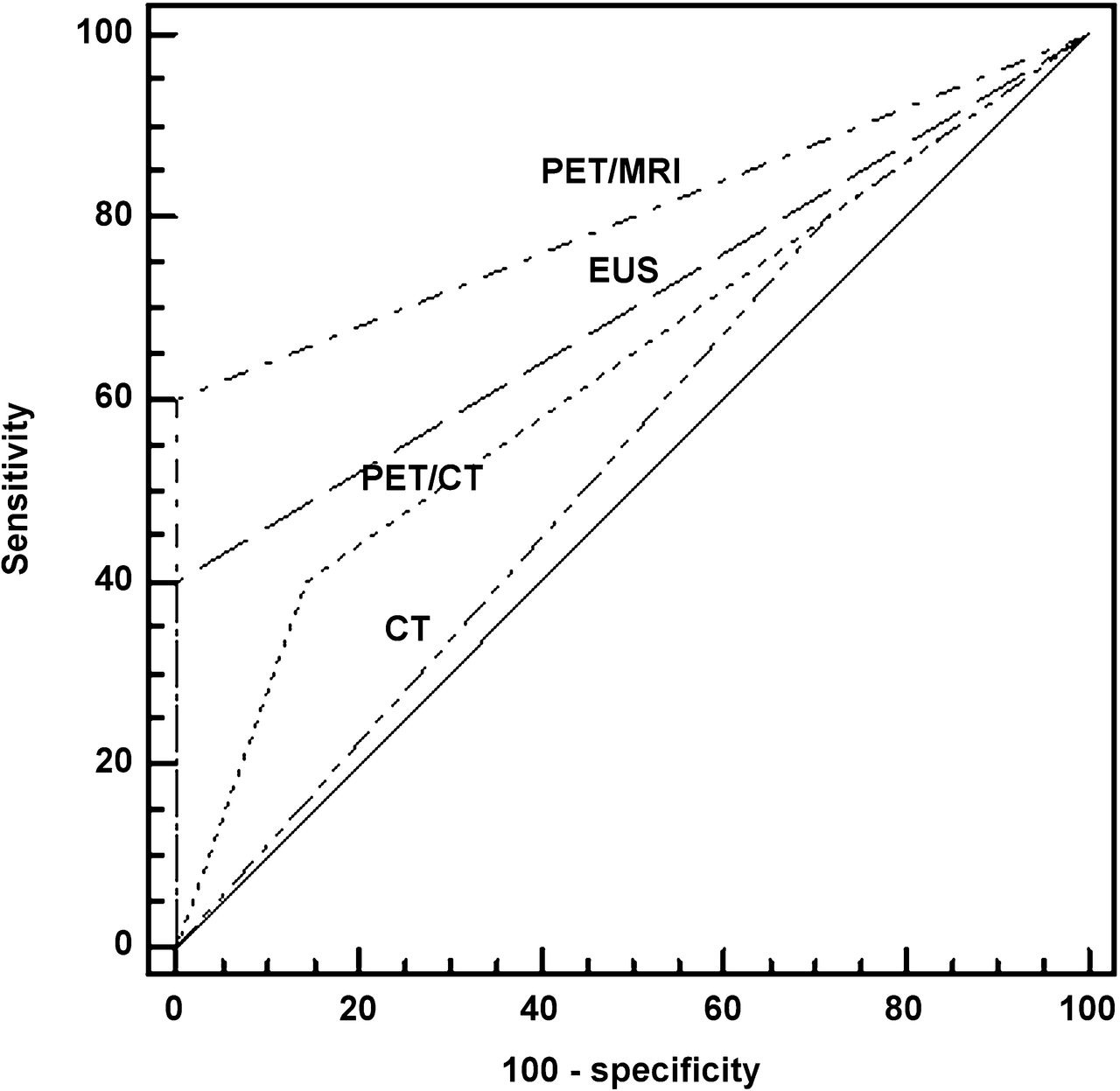
Receiver-operating-characteristic curve analysis of nodal metastasis detection by all methods on per-patient basis. Area-under-curve values are 0.8, 0.7, 0.629, and 0.543 for PET/MR imaging, EUS, PET/CT, and CT, respectively.
DISCUSSION
Our results showed that for T staging, EUS demonstrated the overall highest accuracy, followed by PET/MR imaging and CT (P values of 0.021 and 0.063 for EUS vs. CT and for PET/MR imaging vs. CT, respectively), which is analogous to the present guideline that EUS is the modality of choice. In addition, whereas EUS maintained high accuracy for all stages, CT and PET/MR imaging showed a tendency toward more accurate staging of higher-stage lesions than of lower-stage lesions, thus indicating limited diagnostic accuracy for superficial lesions compared with EUS. Meanwhile, PET/MR imaging showed better diagnostic efficacy than CT. Earlier studies showed disappointing results for the role of conventional MR imaging compared with CT in esophageal cancer staging (14,15). However, because of technical advancements such as faster scanning, respiratory and cardiac gating, and use of surface coils, the diagnostic efficacy of MR imaging for T staging has improved considerably (16,17). In the present study, although still inferior to EUS, PET/MR imaging was shown to be feasible for the identification of esophageal wall layers, whereas such use was limited for CT and impossible for PET/CT. Therefore, we cautiously suggest that PET/MR imaging may overcome the inherent limitation of CT and PET/CT, namely failure to depict esophageal wall layers.
Accurate N staging is essential, as it is a known prognostic factor associated with overall survival (18,19). Optimal N staging of esophageal cancer requires a multimodality approach, and currently, EUS, CT, and PET/CT are known to be an effective combination (4,20–23). In this study, PET/MR imaging demonstrated the highest diagnostic performance for N staging, followed by EUS, PET/CT, and CT (area-under-the-curve values of 0.8, 0.7, 0.629, and 0.543 for PET/MR imaging, EUS, PET/CT, and CT, respectively). MR imaging offers the advantages of excellent soft-tissue contrast and lack of exposure to ionizing radiation. For various reasons, soft-tissue masses usually demonstrate high signal intensity on T2-weighted MR images, and several previous studies have reported malignant lymph nodes to have higher signal intensity than benign lymph nodes on T2- or contrast-enhanced T1-weighted MR images (24–26). Evaluation of signal intensity and morphologic features such as internal necrosis was feasible on the MR images of PET/MR scans. In other words, PET/MR imaging provides both anatomic visualization and quantitative measurement of physiologic processes of the malignancy. Thus, we believe that the advantages of PET/MR imaging yielded favorable outcomes for N staging compared with other modalities.
The novelty of our study is that it was a comparison of 4 modalities: EUS, CT, PET/CT, and PET/MR imaging. To date, we are aware of no reported studies involving PET/MR imaging of esophageal cancers and only a few studies describing the role of conventional MR imaging, which currently is usually not part of the standardized imaging protocol in most institutes (27,28). We hope that our initial experience may provide some baseline data to be validated in future studies.
Our study had several limitations. First, the fact that it included few patients could have weakened the statistical power, and although we prospectively enrolled consecutive patients who were diagnosed with esophageal cancer, our study included only male patients with squamous cell carcinoma. Second, our imaging system does not acquire PET and MR data at the same time, and there is a potential for misregistration due to patient motion and respiration. Third, with no baseline data available for imaging of esophageal cancer with PET/MR, the PET/MR imaging protocol we used was somewhat suboptimal. For conventional MR imaging, various protocols and methods have been validated and used worldwide. However, no certain protocol has been confirmed for PET/MR imaging of esophageal cancers. Specifically, we did not use contrast agents and techniques such as cardiac or respiratory gating, which might have increased the conspicuity of lesions. Fourth, we did not analyze the diagnostic efficacy of M staging. Whole-body MR imaging has been reported to have advantages over PET/CT in lung cancers, especially for detecting brain and hepatic metastasis (29). Therefore, PET/MR imaging may also aid in detecting metastatic lesions that are dismissed at PET/CT. However, in the present study, we focused on locoregional staging of surgically resectable esophageal cancers. Finally, because of the limited availability of PET/MR imaging equipment and the cost involved, only a few institutes can perform this study currently. Despite these limitations of our study, we think that PET/MR imaging is an effective modality with substantial potential in the preoperative staging of esophageal cancer (Fig. 3). Therefore, the efficacy of PET/MR imaging should be verified in additional research consisting of larger series of patients and further adjustment of the imaging protocols.
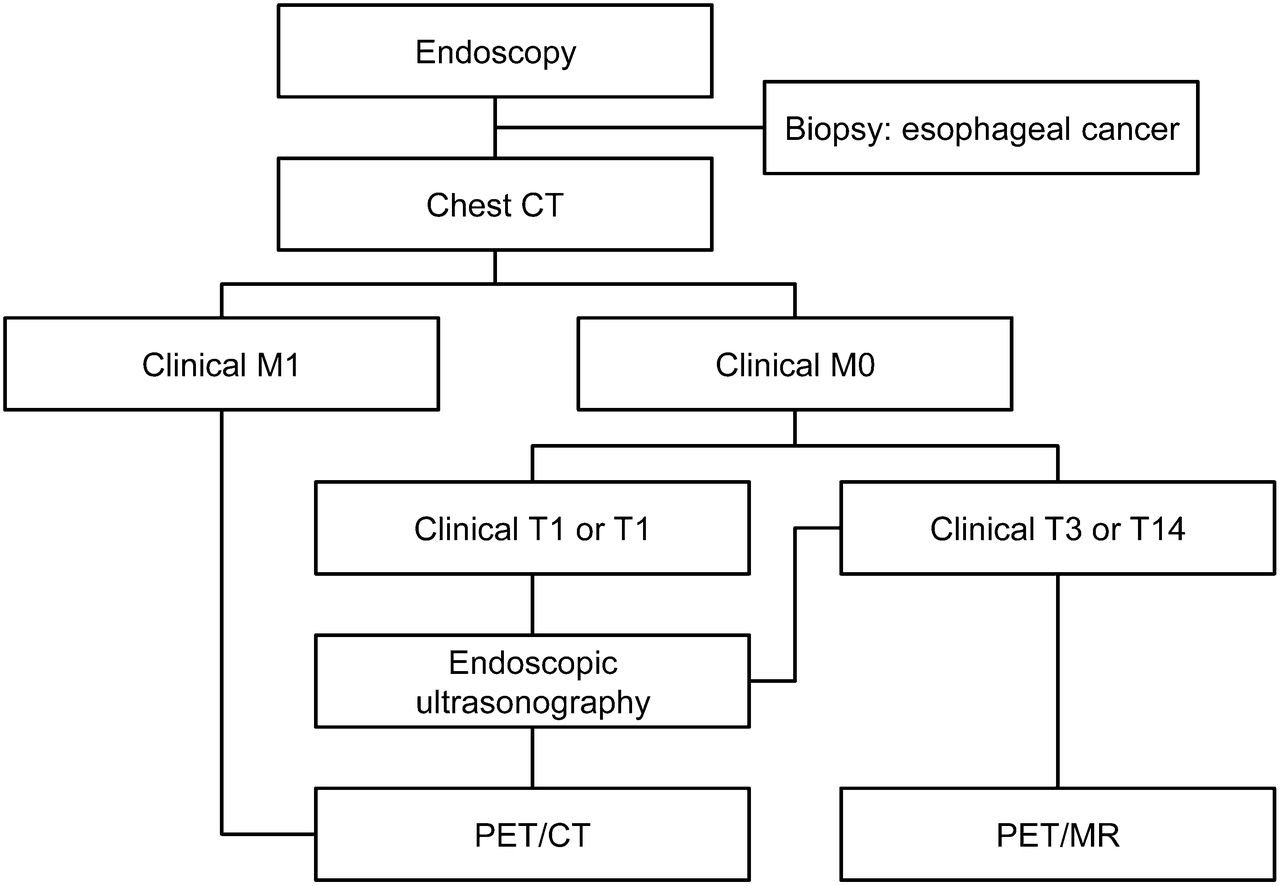
Possible diagnostic flow for esophageal cancer.
CONCLUSION
In the current study, PET/MR imaging demonstrated T-staging accuracy comparable to that of EUS, and although not statistically significant, even higher accuracy than EUS and PET/CT for prediction of N staging. Therefore, our results suggest that with protocol adjustments, PET/MR imaging may be used clinically for the preoperative staging of esophageal cancer in the future.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The current study was supported by grant 2012-26 from the Biomedical Research Institute of Pusan National University Hospital. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online May 27, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 10, 2014.
- Accepted for publication March 31, 2014.





{kind=link}
{kind=link}
{kind=link}