


Abstract
Metastatic disease to bone is commonly seen in the advanced stages of many cancers. The cardinal symptom, pain, is often the cause of significant morbidity and reduced quality of life. Treatment of bone pain includes nonsteroidal analgesics and opiates; however, long-term use of these drugs is commonly associated with significant side effects, and tolerance is common. External-beam radiation therapy is effective mainly in localized disease sites. Bone-targeting radiopharmaceuticals are beneficial in the management of patients with multiple metastatic lesions. This article focuses on the 3 most commonly used agents: the Food and Drug Administration–approved 89Sr-chloride, 153Sm-ethylenediaminetetramethylene phosphonic acid (EDTMP), and 223Ra-dichloride. We will discuss the physical characteristics, clinical data, dosage, and administration of these agents, including optimal patient selection and toxicity associated with their use. These radioactive agents have proven efficacy in the treatment of painful osseous metastases from prostate cancer and breast cancer. Significant recent advances include use of these agents in combination with chemotherapy and the use of the α emitter 223Ra-dichloride in prostate cancer, primarily to improve survival and skeletal related events. The review is presented in 2 parts. The first will discuss the characteristics and clinical use of 223Ra-dichloride, and the second will discuss the β emitters 89Sr and 153Sm-EDTMP.
Several cancers, most commonly breast and prostate, present with bone metastases. In advanced stages, these are frequently associated with adverse clinical sequelae including pain, fractures, and hypercalcemia. These cause significant morbidity and affect performance status and quality of life. The effect of bone metastasis is related to altered signals and balance between osteoclastic and osteoblastic activity. In a normal bone, there is continuous remodeling that maintains optimal mechanical and metabolic functions performed by the osteoclasts and osteoblasts, which resorb and replace bone, respectively (1). Parathyroid hormone, local osteoclast-activating cytokines, and growth factors are some of the systemic processes contributing (2). Metastatic disease leads to secretion of tumor-derived factors that result in increased osteolytic activity and increased bone resorption. Tumor microenvironment and interactions with transient and stromal cells in the bone microenvironment, and molecules such as endothelin-1, are also suggested factors involved in bone metastasis. Growth factors released from the bone matrix further stimulate the tumor cells to grow and secrete additional cytokines. Overall, there is increased risk of skeletal related events, such as osteopenia and fractures, spinal cord compression, and bone marrow dysfunction, and the release of calcium from the bone matrix may cause hypercalcemia of malignancy. Recently, it has been recognized that a critical role in regulating osteoclast activity leading to bone destruction associated with cancer metastasis is played by signaling of receptor activator of nuclear factor κB ligand, inhibitors of which have been developed for management of bone metastasis and skeletal related complications (3). The bone affected by metastatic disease undergoes resorption and loss due to increased osteoclastic activity along with osteoblastic activity that is a compensatory reparative process. Many agents are used in bone metastasis that inhibit osteoclastic activity. Radionuclide therapy is based on incorporation of radiopharmaceuticals in the bone matrix through interaction with the matrix in the newly forming bone.
Management of bone pain includes analgesic therapy, external-beam radiation therapy, surgical intervention, and the use of systemic bone-seeking radiopharmaceuticals. Bone pain is controlled with analgesic medications in a 3-step approach. Nonsteroidal antiinflammatory drugs (NSAIDs), including aspirin, ibuprofen, and naproxen, are used initially for mild to moderate pain. If the pain persists or increases, treatment progresses to the second step, weak opioids such as codeine or hydrocodone, and then to the third step, higher doses or more potent opioids such as morphine, hydromorphone, or fentanyl. The World Health Organization has published guidelines for pain management (4,5). Narcotics form the next level of treatment, given with increasing potency for more painful disease, but are associated with side effects including constipation, limitations in mental and physical status, and addiction. The pain management guidelines of the National Comprehensive Cancer Network (6) recommend an initial comprehensive assessment of pain, including severity, pathophysiology, presence of cancer pain syndromes, and any skeletal related events. Recommendations include initiation of analgesic NSAIDs such as acetaminophen. Pain associated with inflammation is treated with NSAIDs and corticosteroids. For pain without an oncologic emergency, NSAIDs are given first, with the dose being increased if pain persists or increases on treatment. Bisphosphonates, chemotherapy, and endocrine therapy may be used to prevent bone resorption and target the bone metastasis, respectively. Localized radiotherapy or systemic radionuclide treatment may be added as needed for cases of local pain or generalized diffuse disease pain, respectively. Continuous pain is treated with regular doses of pain medication, and small doses of opioids may additionally be given for breakthrough pain. Opioids are rotated or changed when pain persists or increases (6). Lethargy and constipation are particularly common symptoms that are associated with opiate use. Prolonged use leads to tolerance, and progressively increased dosing is required. Radiation therapy and surgery are commonly used for the treatment of localized bone metastases (7). The use of antiresorptive agents such as bisphosphonates and targeting of the pathway of receptor activator of nuclear factor κB with denosumab are commonly used for reducing pain and skeletal related events (8). Bone-seeking radiopharmaceuticals are preferred for widespread symptomatic bone metastasis (9,10).
Although several radiopharmaceuticals with different physical properties have been used for treatment of metastatic bone disease, our review will focus on more commonly used β-emitting isotopes, namely 89Sr-chloride (Metastron; GE Healthcare), 153Sm-ethylenediaminetetramethylene phosphonic acid (EDTMP) (lexidronam/Quadramet; Dow Chemical Co.), and the α-emitting radioisotope 223Ra-dichloride (Xofigo [previously known as Alphradin]; Bayer HealthCare), the 3 radiopharmaceuticals currently approved and available in the United States.
223RA-DICHLORIDE
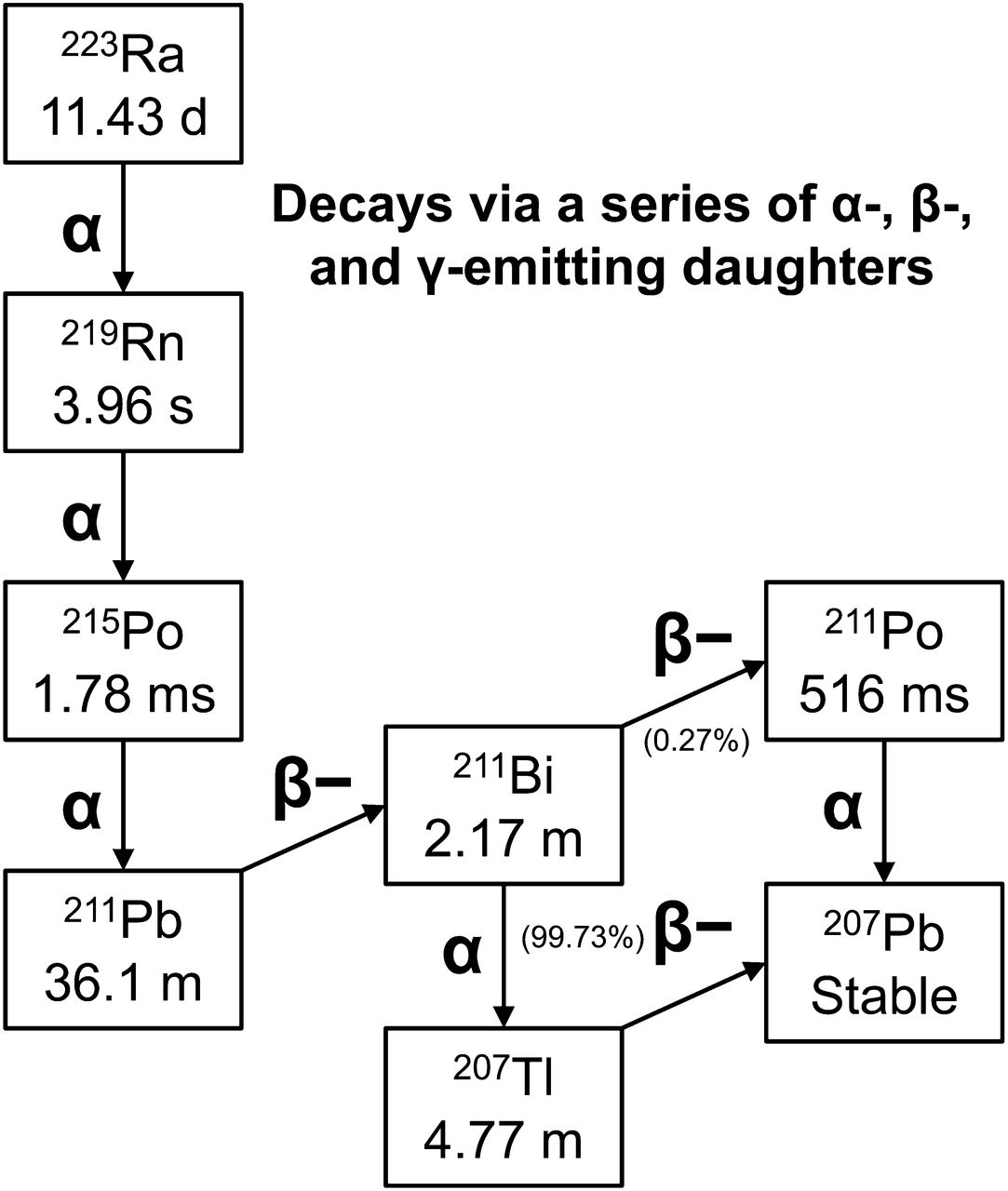
223Ra-dichloride is a novel, bone-seeking calcium mimetic α emitter, accumulating in areas of increased bone turnover, that is being developed to target metastatic bone disease (11–17). The physical characteristics of 223Ra are shown in Table 1. Among its advantages are its availability from a long-lived 227Ac/227Th generator (18) and a physical half-life of 11.4 d, which allows for easy shipping to end users because of the long time between manufacturing and expiration. 223Ra has a complex decay scheme in which 4 α particles are generated during each decay, resulting in high energy deposition (28.2 MeV), with 95% of the energy from the α emissions (Fig. 1). The high linear energy transfer of α radiation results in a greater biologic effectiveness than β radiation, as well as generation of double-strand DNA breaks, and gives rise to cytotoxicity that is independent of dose rate, cell cycle growth phase, and oxygen concentration (19). The range of the α particles (<100 μm) is much smaller than the 0.7-cm path length of 89Sr and the 0.33-cm path length of 153Sm; as a result, less hematologic toxicity for a given bone surface dose would be expected from α emitters than from β emitters (20). It is estimated that as few as 1–20 α tracks crossing the nucleus will result in cell death (19). 223Ra, similar to other alkaline earth elements such as calcium, is absorbed into bone matrix at sites of active mineralization (21).
Physical Properties of Bone-Seeking Radiopharmaceutical 223Ra

Decay scheme for 223Ra.
Preclinical studies have shown selective concentration in bone, compared with 89Sr, with no significant redistribution of the daughter radionuclides (16). Lack of significant redistribution of the daughter radionuclides has also been shown in patients (22). Use of 223Ra also resulted in an increased symptom-free survival in mice (17), thus laying the foundation for clinical translation.
Clinical experience with 223Ra is more recent and overall less extensive than experience with 89Sr and 153Sm-EDTMP. The data are more focused on prostate cancer metastasis (Table 2) (11,13,14,23,24). The results of the ALSYMPCA (Alpharadin in Symptomatic Prostate Cancer) study, a phase III 223Ra multinational trial on patients with prostate cancer, showed survival benefit in those receiving 223Ra, resulting in priority review for approval by the Food and Drug Administration and full approval granted in May 2013 (24,25). The trade name of 223Ra dichloride, Xofigo, is being copromoted by Bayer HealthCare and Algeta US, LLC. A request for approval by the European Medicines Agency is pending at the time of writing.
Clinical Studies with 223Ra
PHARMACOKINETICS AND BIODISTRIBUTION
Analysis of the pharmacokinetics of 223Ra (13,22) showed rapid clearance from the blood, with less than 1% remaining at 24 h. Imaging of γ rays from 223Ra and its daughters, although feasible, is of poor quality but does allow for understanding the biodistribution and establishing targeting of lesions (Fig. 2) (13,22,26). Elimination is mainly through the gastrointestinal tract, and early excretion is seen in the small bowel, presumably transluminally, with the median being 52% activity in the bowel at 24 h (22). Urinary excretion is minimal (typically <5%), in contrast to 153Sm-EDTMP (22).
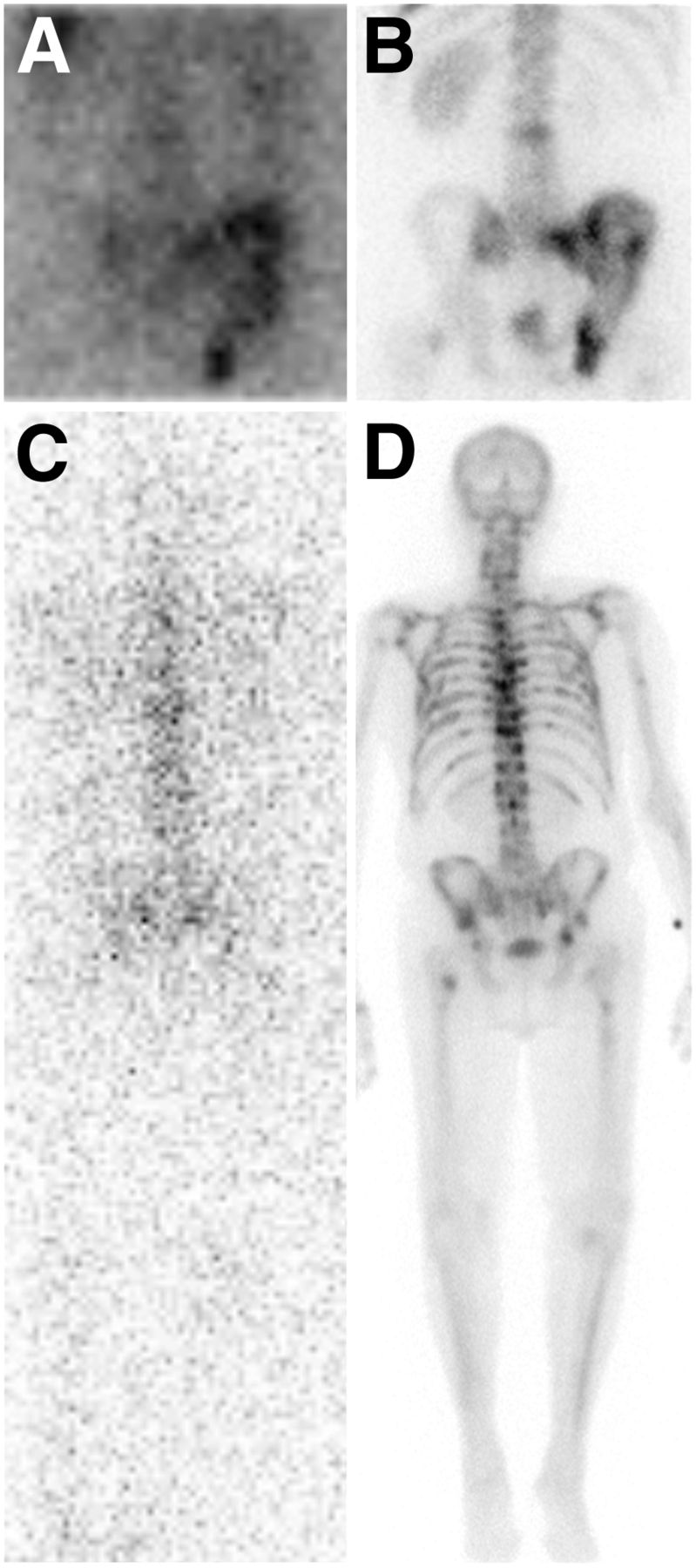
Imaging with 223Ra. (A and B) Posterior spot image (A) of 223Ra at 6 d (200 kBq/kg [240 μCi]) shows prominent uptake in right iliac bone, right ischium, and sacrum corresponding to lesions seen on bone scan image (B). (C and D) Whole-body 223Ra posterior image (C) shows heterogeneous uptake in spine corresponding to multiple lesions seen on bone scan (D).
CLINICAL STUDIES WITH 223RA (TABLE 2)
Administration of 223Ra is based on body weight, similar to 153Sm-EDTMP. However, because of the higher relative biologic effectiveness of α emitters than β emitters, the activity required is much smaller. An initial phase I study using single escalating doses ranging from 46 to 250 kBq/kg showed favorable biologic effects, good tolerance at all levels, and no dose-limiting toxicity even at the highest administered dose (13). Other phase II trials were conducted using either a single injection of no more than 200 kBq/kg or cumulative activity of up to 240 kBq/kg administered in split doses, with low toxicity and clinical benefit. Later studies focused on administering fractionated activity. A larger multicenter phase III trial was done with a 223Ra dose of 50 kBq/kg given as repeated injections for 6 doses (24). In the United States, a small phase I trial evaluated activity of 50, 100, and 200 kBq/kg as a single injection without an effort to reach a maximal tolerated dose because of the favorable biologic effect of lower repeated activity (22).
In contrast to development of several other bone-targeting radionuclides that have focused on relief of pain as endpoints, several of the clinical trials with 223Ra have focused on survival, biochemical response, skeletal related events, and quality-of-life outcomes as endpoints. Furthermore, most of the phase II trials are randomized, placebo-controlled trials limited to castration-resistant metastatic prostate cancer.
Decrease in Bone Markers
There is a suggestion that bone alkaline phosphatase (ALP) is a predictive marker for tumor response in patients with castration-resistant prostate cancer (27), and a significant decrease in ALP is seen with 223Ra. A randomized study performed by Nilsson et al. evaluated 64 castration-resistant prostate cancer patients with painful bone disease requiring external-beam radiation therapy followed by randomization to external-beam radiation either alone (n = 31) or along with 223Ra at 50 kBq/kg every 4 wk × 4 (n = 33). At 4 wk after treatment, a median decrease of 65.6% in ALP levels was seen in the 223Ra group, versus a 9.3% rise in those treated with external-beam radiation alone (14). Similar results for ALP decrease were noted in other studies (13,22). In patients treated with a 25, 50, or 80 kBq/kg dose of 223Ra repeated 3 times, a drop of at least 50% in bone ALP was seen in 16%, 67%, and 66%, respectively (24). When patients were treated with only a single dose of 223Ra, a significant drop in ALP was seen only at the 100 kBq/kg dose level (24).
Markers of bone turnover such as CTX-1 (carboxy-terminal crosslinking telopeptide of type I collagen) and procollagen I N-terminal propeptide also show a significant decrease in patients treated with 223Ra (14). A significant decrease in prostate-specific antigen (PSA) levels occurs after 223Ra treatment, versus placebo (23.8% PSA decease vs. 44.9% increase, respectively). A longer median time to PSA progression is also seen: 26 wk versus 8 wk for 223Ra versus the control group (14). A dose response was seen; for treatment at 25, 50, or 80 kBq/kg, a drop of at least 50% in PSA was seen in no patients (0%), 2 patients (6%), and 5 patients (13%), respectively, whereas a drop of at least 50% in bone ALP levels was seen in 16%, 67%, and 66% for the respective dose levels (24).
Effect on Skeletal Related Events
223Ra effectively decreases the onset of the first skeletal related events. In a group of 64 patients receiving external-beam radiation plus 50 kBq/kg × 4 doses of 223Ra or external-beam radiation and placebo (14,23), the median time for the first skeletal related event was 14 wk versus 11 wk, respectively. In the ALSYMPCA trial, on 921 patients, a significant delay in skeletal related event onset was seen: median, 14.9 mo, versus 11.3 mo for the control group (25).
Survival Benefit
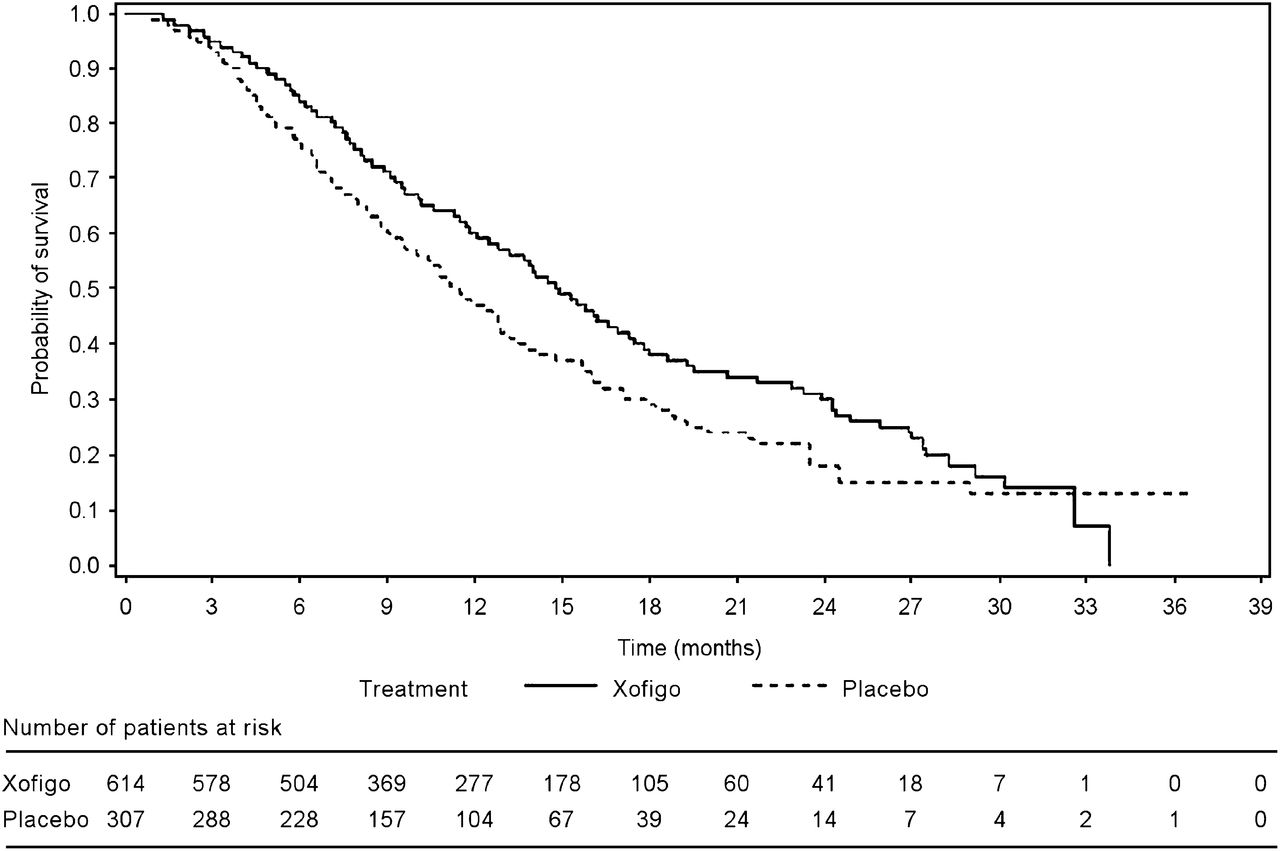
In contrast to other radiopharmaceutical agents, 223Ra therapy has demonstrated significant improvement in survival as a single agent. Among patients with bone pain receiving external-beam radiation alone or external-beam radiation plus 223Ra, 15 patients assigned to the 223Ra group were alive at 18 mo of follow-up, compared with 8 in the group receiving external-beam radiation alone (14). The median overall survival was, at 18 mo, 65.3 wk for 223Ra versus 46.4 wk for external-beam radiation only and, at 24 mo, 65.3 wk versus 46.4 wk, respectively (hazard ratio of 0.47 in favor of the 223Ra arm). Furthermore, at 2 y 30% of the 223Ra group were alive, compared with 13% for placebo. Those who received all 4 injections had longer overall survival than those receiving fewer injections (23). Overall survival in the phase III ALSYMPCA trial was 14.9 mo for men treated with 223Ra and 11.3 mo for those receiving placebo (Fig. 3). An overall survival benefit with 223Ra was seen in all subgroups of men, regardless of their extent of disease and whether they had previously received docetaxel or current treatment with bisphosphonates (25).

Survival curve, phase III study. (Adapted from (29).)
Effect on Pain
223Ra is effective in pain relief. In an initial study, pain relief was seen at all dose levels ranging from 46 to 250 kBq/kg given as a single dose. Pain relief occurred in 52%, 60%, and 56% of patients at 1, 4, and 8 wk, respectively. There was no definite dose–response relationship. Similar results were noted in a randomized double-blind controlled trial focused on patients experiencing pain from castration-resistant prostate cancer. Patients received a single 5, 25, 50, or 100 kBq/kg dose of 223Ra. At 8 wk, 40% of those treated with the 5 kBq/kg dose had pain relief, versus 71% of those treated with the 100 kBq/kg dose, with complete or very good pain response seen in 30% versus 51%. A significant number of patients had a decrease in pain medication at 8 wk. The mean pain relief duration was 44 d for higher doses (50 and 100 kBq/kg), versus 28 d for the 5 kBq/kg dose and 35 d for the 25 kBq dose (P > 0.05) (24).
DOSIMETRY AND TOXICITY
There is less bone marrow toxicity with 223Ra than with β emitters. Dosimetry estimates using standard approaches have been compared with cell level dosimetry using a model for the expected localization of 223Ra relative to marrow cavity. Hobbs et al. estimated the percentage of cells that receive a potentially toxic absorbed dose (2 or 4 Gy). On the basis of the model, it is estimated that the majority of the radiation dose is deposited near the trabecular elements, substantially decreasing the risk of marrow toxicity at higher doses (20). Using an International Commission on Radiological Protection biokinetic model for alkaline earth elements, Lassman et al. estimated the absorbed dose to organs from 223Ra. The largest estimated doses were 3.8 × 10−6 Gy/Bq to bone endosteum and 3.7 × 10−7 Gy/Bq to bone marrow (28). The organ-based dosimetry from patient studies and using the MIRD method and OLINDA software are provided in the Xofigo product information (29), and the major organ doses are summarized in Table 3.
Dosimetry for 223Ra-Dichloride (30)
Hematologic Toxicity
Compared with β emitters, 223Ra has the theoretic advantage of sparing much of the marrow irradiation given the short-range emissions (15,20,28). Although the activity of administered 223Ra has ranged from single injections of 5 kBq/kg to 250 kBq/kg and maximum fractionated activity of up to 300 kBq/kg (12,24), a maximum tolerated dose has not been reached. 223Ra is well tolerated, with a small incidence of adverse events.
223Ra myelotoxicity is infrequent, typically with no grade 4 toxicities and infrequent grade 3 toxicities (using National Cancer Institute common toxicity criteria) (13,14). Of 33 patients receiving 50 kBq/kg × 4 doses of 223Ra, none developed grade 4 myelotoxicity and only 1 had grade 3 leukopenia, neutropenia, and anemia, seen in the first 2–4 wk (13,14) and with no cumulative myelotoxicity. Hematopoietic toxicity is dose-related (11). The hematopoietic toxicity or myelosuppression is reversible, with the nadir occurring 2–4 wk after treatment (13). Generally, recovery occurs by 24 wk; those with anemia at baseline may take longer (24).
Nonhematologic Toxicity
Nonhematologic toxicities are generally more common than hematologic toxicity and are mild to moderate in intensity. The most common side effects are diarrhea, fatigue, nausea, vomiting, and bone pain (13,14,24), some of which are dose-related. These side effects are easy to manage; treatment is symptomatic and supportive. In one study, there was no difference in the incidence of these toxicities in the 223Ra versus control patients for most symptoms except for a higher incidence of constipation in 223Ra-treated patients (12/33) versus controls (2/31) (14).
In a larger trial on 600 patients treated with 223Ra, toxicities were mild. The most frequent reported side effects, occurring in more than 10% of patients, were nausea, diarrhea, vomiting, and peripheral edema; interestingly, constipation was not mentioned. Hematopoietic grade 3 or 4 leukopenia and thrombocytopenia occurred in less than 3% of the 223Ra-treated group and less than 1% of the placebo group (29).
COMBINED THERAPY
The landscape in prostate cancer treatment has changed significantly in the last few years, with various new therapies having become available, including cabazitaxel, abiraterone, and enzalutamide. Although this progress has increased the armamentarium available for metastatic prostate cancer, it creates challenges in determining the sequencing of treatment and provides opportunities and challenges for combined therapy with 223Ra. Several studies combining 89Sr-chloride and 153Sm-EDTMP with chemotherapy and other reagents have been reported (30–38); these will be detailed more thoroughly in part 2 of this article. On the basis of the observed benefits of combining 153Sm EDTMP with docetaxel and the expected greater marrow-sparing effect of 223Ra, interest in combination therapy has arisen. Although there is a phase I/II trial comparing the effect of 223Ra in conjunction with docetaxel to docetaxel alone (ClinicalTrials.gov identifier NCT01106352), no definite data are yet available.
LATE TOXICITY
Long-term follow-up of patients receiving 223Ra is limited given the time from the initial clinical studies (2005) and the relatively short survival of patients treated with advanced prostate or breast cancer. A 24-mo follow-up showed 57% mortality, with similar proportions per group treated at various dose levels; however, this mortality was attributable to progression of disease. No myelodysplastic syndrome, acute myelogenous leukemia, or aplastic anemia occurred (24). Of 10 patients who were alive at 2 y after 4 injections of 50 kBq/kg, none developed acute myelogenous leukemia, myelodysplastic syndrome, or aplastic anemia. A case of bladder cancer and a case of pancreatic cancer seen in follow-up patients were not related to 223Ra (23).
DOSAGE, ADMINISTRATION, AND PATIENT INSTRUCTIONS
The approved dose for 223Ra is 50 kBq/kg given as 6 doses. The indications, contraindications, and dose calculation details are given in Tables 4 and 5. The dose is administered intravenously with precautions to ensure proper placement in the vein by a repeated check for blood return. A 3-way stopcock is recommended to enable easy infusion and backflush so that residual can be minimized.
Indications, Contraindications, and Prerequisites for 223Ra-Dichloride
Dosage and Administration of 223Ra-Dichloride
Radiation safety precautions are standard, and there is less concern about exposure to the public because of the limited γ emission of 223Ra. Mean dose rates measured from a typical administered activity to patients are given in Table 6 (39). Those administering the doses should take standard precautions during the injections. Follow-up includes serial complete blood counts for any decrease in levels and follow-up until recovery from nadir counts. Patients should report any evidence of bleeding or infection to the treating physician. Because of the possibility of nausea and diarrhea, attention should be paid to maintaining good hydration. Soiled clothing or bodily fluids should be handled using gloves, and universal precautions are sufficient to protect from radiation contamination. Soiled clothing should be laundered separately to eliminate direct transfer. Even though no data are available on the potential effect on sperm and reproduction, a 6-mo period of contraception use is recommended.
Mean Dose Rates* for Injected Activity of 223Ra-Dichloride (39)
SUMMARY OF 223RA
223Ra is a safe and effective treatment for bone metastasis in castration-resistant prostate cancer. 223Ra is helpful not only in pain control but, more importantly, in decreasing skeletal related events and increasing survival. Additional clinical data will be available in the coming years as 223Ra is utilized more extensively in clinical practice. Future possibilities include exploring the use of 223Ra as first-choice treatment in patients with symptomatic bone disease and use in the adjuvant setting of minimal metastatic disease. Use of 223Ra in combination with chemotherapy is being studied. Its role in the treatment of bone metastasis from other cancers has yet to be defined.
Footnotes
Published online Jan. 16, 2014.
Learning Objectives: On successful completion of this activity, participants should be able to (1) define the advantages and disadvantages of the use of α-emitting radionuclide 223Ra-dichloride in the treatment of painful metastatic osseous metastasis; (2) recognize the indications and contraindications and define the prerequisites for administration of 223Ra-dichloride; and (3) apply and integrate the treatment of osseous metastasis with 223Ra-dichloride in routine clinical practice.
Financial Disclosure: Dr. Carrasquillo is a consultant/advisor for Bayer and Algeta. Dr. Larson is on the advisory board of ImaginAb, Molecular Imaging, and Perceptive Informatics; is a scientific advisor for Millennium and Progenics Pharmaceuticals, Inc., is a board member and the Chief Medical Officer of Claymore Technologies LLC; and has other ownership interest in Clinical Silica Technologies. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, participants can access this activity through the SNMMI Web site (http://www.snmmi.org/ce_online) through February 2017.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 21, 2013.
- Accepted for publication September 3, 2013.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Development of sodium fluoride PET response criteria for solid tumours (NAFCIST) in a clinical trial of radium-223 in osteosarcoma: from RECIST to PERCIST to NAFCIST
- Molecular radiotheragnostics in prostate cancer
- Radium-223: Insight and Perspectives in Bone-metastatic Castration-resistant Prostate Cancer