


Abstract
18F-FDG PET has already proved its usefulness in the follow-up of patients with alveolar echinococcosis (AE) and has been proposed as a surrogate marker for therapeutic decisions on structured treatment interruption by benzimidazoles. However, standard PET acquisition (1 h after 18F-FDG injection) lacks sensitivity, and the parasite may stay viable even if 18F-FDG perilesional uptake has disappeared. The aim of our study was to evaluate the usefulness of delayed 18F-FDG PET in the management of AE patients. Methods: During a 6-y period, 120 PET scans using 18F-FDG were obtained for 70 AE patients treated by benzimidazoles, without selection. All patients underwent whole-body imaging on a PET/CT device 1 h after 18F-FDG injection (4 MBq/kg), as well as an acquisition focused on the liver 3 h after the injection. We also analyzed the results of serologic tests. Results: Of the 57 scans considered negative at the standard acquisition, 13 (22.8%) became clearly positive at the delayed acquisition, and 6 (10.5%) became indeterminate at the delayed acquisition. Furthermore, 20 of 22 scans interpreted as indeterminate at the standard acquisition were considered positive because of clear perilesional 18F-FDG uptake at the delayed acquisition. Thus, delayed acquisition changed the interpretation in 32.5% of cases. Moreover, of 44 patients treated by benzimidazoles and followed for more than 2 y by regular 18F-FDG PET scans and specific AE serology, 11 (25%) presented pathologic 18F-FDG uptake at the delayed acquisition but not at the standard one. In these patients, the treatment was continued despite negative results on standard 18F-FDG PET and negative serologic findings. On the other hand, in 7 patients with negative delayed 18F-FDG PET and negative serology, the treatment was safely interrupted with no evidence of disease recurrence during 8–37 mo (mean, 23 mo). Conclusion: Our study clearly demonstrated that delayed 18F-FDG PET greatly facilitated the differentiation between active and inactive liver lesions in AE patients. Also, our results strongly suggested that the combination of delayed 18F-FDG PET and specific serology would prevent most of the recurrences observed after premature interruption of the treatment based only on standard 18F-FDG PET.
Alveolar echinococcosis (AE) is a rare and chronic parasitic disease caused by the intrahepatic development of the larval form (metacestode) of Echinococcus multilocularis. Human AE is observed only in the northern hemisphere. The main endemic regions are western-central Europe, western China, eastern Russia, and North America (Alaska and northern Canada), but it has also been reported in Turkey, central Asia, Japan (Hokkaido Island), and northern India (1,2). Eastern France, southern Germany, and Switzerland are the most affected areas in Europe, but E. multilocularis is now present in all European countries except Spain, Portugal, and the United Kingdom. Between 1982 and 2009, 417 cases of AE were recorded in France (3).
The metacestode initially develops almost exclusively in the liver, and the larvae can then spread to other organs by infiltration or metastatic dissemination. Primary extrahepatic locations of AE are rare (1). Despite its parasitic nature, AE behaves like a slow-growing liver cancer and the lesions, constituted by the metacestode and an infiltrating granulomatous and fibrous immune response, are responsible for the destruction of hepatic tissue and the obstruction of bile ducts and vessels, causing severe and often lethal complications (4). According to the World Health Organization (WHO) Informal Working Group on Echinococcosis (IWGE) expert consensus (5), complete surgical resection of the parasitic lesion should be the first treatment choice, as it gives the best prospect for a complete cure. However, because of the long clinical latency and the consequent late stage at which many cases are diagnosed, curative resection can be performed in only about 30%–40% of patients (6). Benzimidazole treatment using mebendazole or, more frequently now, albendazole has led to a major improvement in patient survival during the last 30 y (5). This treatment is mandatory in all patients and should be given for at least 2 y after radical surgery. Because it only prevents parasitic growth instead of killing the parasite, lifelong treatment is necessary in inoperable patients and in those receiving a liver transplant.
Conventional imaging modalities, such as ultrasound, CT or MR imaging, are not useful for follow-up because neither the reduction of lesion size nor the presence or increase of calcifications within the lesions is a reliable predictive factor for parasitic activity (7,8). Thus, surrogate markers of parasitic involution that can predict the absence of recurrence after treatment interruption are needed.
The main 2 tools that have been proposed for this purpose are E. multilocularis–specific serology and 18F-FDG PET (5). A negative specific serology in patients who had a positive serology before treatment initiation is statistically associated with clinical improvement and relative stability of the lesions but, on an individual basis, cannot assess absence of E. multilocularis viability (9). 18F-FDG PET with whole-body acquisition 1 h after radiopharmaceutical intravenous injection has been proposed as a functional surrogate marker (7,8,10,11); however, attempts at treatment interruption according to complete loss of perilesional 18F-FDG uptake have often been followed by reevolution of the lesions (12). This pattern strongly suggests that the parasite was still viable and that 18F-FDG uptake might have been underestimated and misinterpreted. Improving 18F-FDG PET sensitivity in AE patients would allow clinicians to better predict the outcome of treatment interruption and to prevent dangerous recurrence. It is why, given the analogy between malignant tumors and AE, experience in the field of cancer inspired us to undertake a prospective study of the usefulness of delayed acquisition of 18F-FDG PET images in AE patients. Koyama et al. showed that delayed 18F-FDG PET image acquisition (2 h after 18F-FDG injection), also called dual-time-point imaging, improved detection of malignant hepatic lesions (13). Lin et al. demonstrated that tumor-to-background ratio in the liver was even higher at a 3-h acquisition than at a 2-h acquisition (14), and further studies confirmed that an improvement of tumor-to-background ratio with better visualization of liver tumors could be obtained by delayed 18F-FDG PET (15–18).
The aim of our study was to assess, in a large population of AE patients followed at the same center, whether delayed 18F-FDG PET might be useful in the detection of 18F-FDG uptake in AE lesions. The correlation between 18F-FDG uptake and Em2+ serology, which is based on the Em18 antigen present in viable lesions, was also studied to determine whether combining both parameters could be of use in predicting lesion activity and possible recurrence after benzimidazole interruption.
MATERIALS AND METHODS
Patients
We included in the study, without selection, all 70 patients with AE (Table 1) who were followed up prospectively in our hospital between March 1, 2004, and December 31, 2010, and were treated orally by mebendazole or albendazole according to the WHO IWGE expert consensus (5).
Patient Characteristics
The diagnosis of AE was assessed according to WHO IWGE recommendations; 25 were considered as confirmed cases, 41 as probable cases, and 4 as possible cases (because of serology positive with only a single specific test). Partial liver resections were performed on 18 patients, and 5 patients underwent liver transplantation.
The study protocol was approved by the Ethics Committee of our institution (Comité de Protection des Personnes), and all patients signed a written informed consent.
Imaging
During the follow-up, all patients underwent 1–4 whole-body 18F-FDG PET scans (Biograph; Siemens/CTI). The patients fasted for at least 6 h before 18F-FDG injection. The imaging protocol consisted of a standard whole-body spiral CT acquisition without intravenous injection of a contrast agent, immediately followed by a standard whole-body PET acquisition (7–9 bed positions, 3 min each) 1 h after intravenous injection of 18F-FDG (4 MBq/kg), and completed by a delayed acquisition (2 bed positions for the hepatic region, 3 min each) 3 h after the 18F-FDG injection. PET images were reconstructed using an iterative 3-dimensional ordered-subsets expectation maximization reconstruction algorithm, and all images were evaluated independently by 2 experienced nuclear medicine physicians. The scan was considered negative when no area of enhanced metabolic activity was found, positive if at least 1 focus of enhancement (hot spot) appeared, and indeterminate when the perilesional metabolic activity was difficult to differentiate from the hepatic physiologic uptake.
Biologic and Serologic Tests
The patients regularly had blood count and liver function tests, according to the international recommendations (5). Serologic tests for diagnostic and therapeutic evaluation were also performed for all patients. All patients underwent serologic follow-up using Em2-plus-ELISA (Bordier Affinity Products; cutoff index, 0.8), which contains purified Em2 antigen localized in the laminated layer and recombinant EmII/3-10 antigen localized in the tegument of the protoscolex and the germinal layer and considered to be a relevant marker of disease activity (19–21).
Follow-up
Therapeutic efficiency was evaluated by clinical and ultrasound examinations, liver tests, blood counts, and serology every 6 mo. 18F-FDG PET was performed every 6–12 mo, depending on the severity of the disease.
Moreover, according to WHO IWGE expert consensus (5), all patients underwent a separate ultrasound examination as a routine imaging technique, as well as multiphase CT or MR imaging, as a part of combined follow-up (22,23) when other tests suggested that disease- or treatment-related complications were present. However, as stated by the WHO IWGE expert consensus, the results of CT or MR imaging were not taken into consideration when decisions on treatment interruption were being made (5).
RESULTS
Comparison Between Standard and Delayed 18F-FDG PET Acquisitions
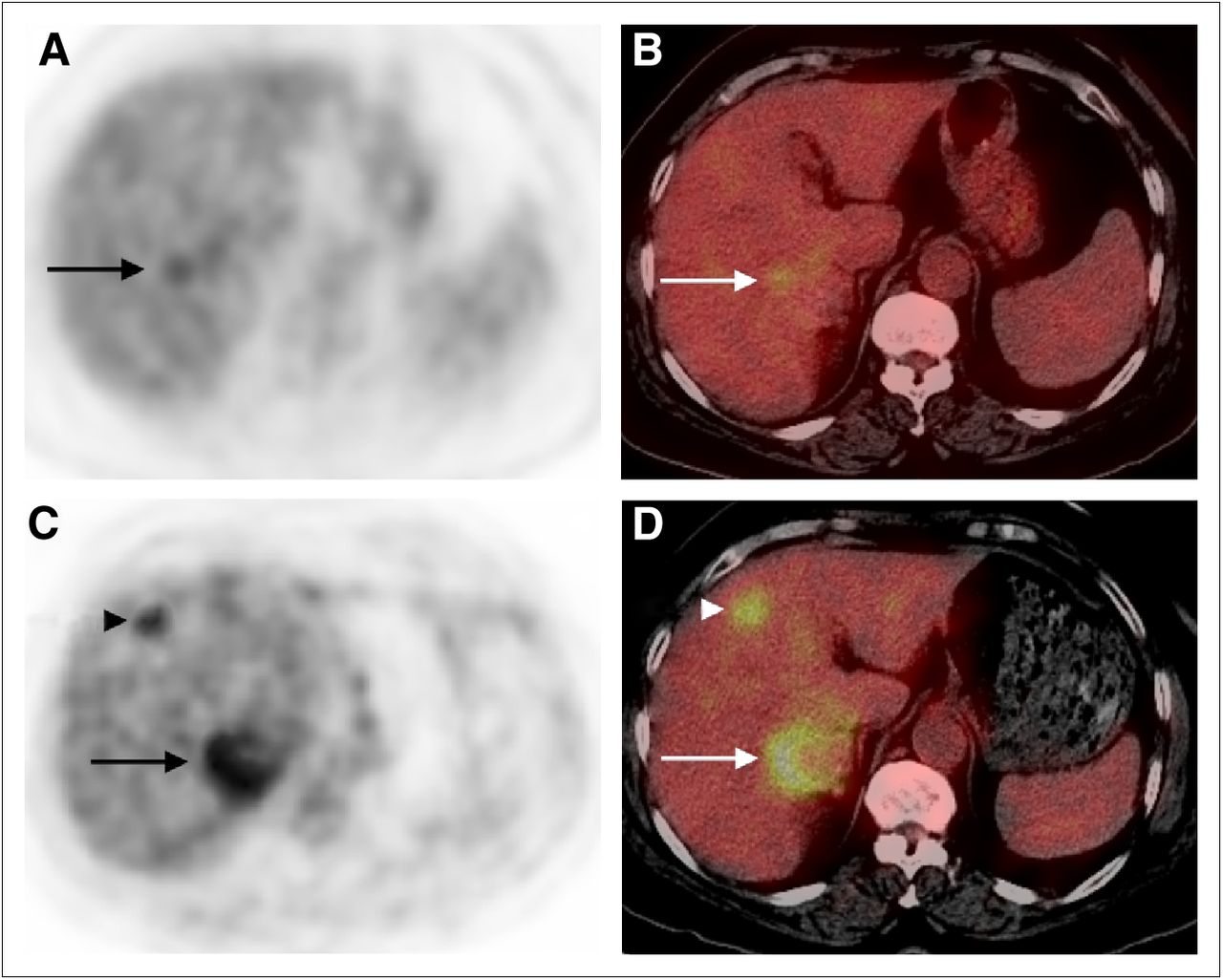
We performed 120 dual-time-point 18F-FDG PET scans on 70 patients (Table 2). There was no discordance between the 2 image acquisitions for the 41 scans that were positive at the standard acquisition. In 20 of 22 scans described as indeterminate at the standard acquisition, we observed clear 18F-FDG uptake at the delayed acquisition, allowing us to identify these scans as unequivocally positive (Fig. 1). In the remaining 57 scans that were negative at the standard acquisition, the interpretation of PET images changed to positive in 13 patients (22.8%) at the delayed acquisition and to indeterminate in 6 patients (10.5%). Furthermore, no image considered positive or indeterminate at the standard acquisition was negative at the delayed acquisition.
Comparison of Standard and Delayed 18F-FDG PET Results in 70 Patients (120 Scans)

Indeterminate vs. positive results. Moderate, diffuse 18F-FDG uptake (arrows) around hepatic lesion of segment VII at standard acquisition (A [PET] and B [PET/CT]) becomes clear at delayed acquisition (C [PET] and D [PET/CT]); another lesion in segment V is visualized at delayed acquisition only (arrowheads).
Finally, the interpretation of 39 scans (32.5%) changed after the delayed acquisition. Thus, clear assessment of the metabolic activity of the lesions was made possible by the delayed acquisition on 112 of 120 scans.
Therapeutic Decision Based on 18F-FDG PET and Serology
These results, which showed that delayed 18F-FDG PET acquisition improved the sensitivity of detection of perilesional metabolic activity, led us to evaluate whether this technical refinement could facilitate therapeutic decisions. We performed a strict follow-up of the AE patients, including clinical examinations, serology, and 18F-FDG PET, with the aim of interrupting benzimidazole treatment in those patients with no 18F-FDG uptake in the lesions. Patients with a short-term follow-up (<2 y) were excluded from this part of the study because benzimidazole interruption could not be envisaged so prematurely. Thus, we evaluated the impact of standard and delayed 18F-FDG PET, alone or combined with specific serology, on the therapeutic decision in 44 of the 70 AE patients.
Table 3 summarizes the comparison between serology and 18F-FDG PET in this group of patients. Fifteen patients had positive results for both serology and standard 18F-FDG PET, and this number increased to 21 when delayed acquisition was considered. In this way, delayed acquisition increased the number of results that were doubly true-positive and for which treatment interruption was thus contraindicated. Also the number of doubly true-negative results was improved by delayed 18F-FDG PET because we observed 12 patients with negative serology after standard PET (Fig. 2) versus 7 patients after delayed acquisition, thus further reducing the number of patients who could be subjected to treatment interruption.
18F-FDG PET and Serologic Results in 44 Patients Potentially Eligible for Treatment Interruption Because of More Than 2 Years of Follow-up

Role of 18F-FDG PET in therapeutic decision. Huge AE lesion of hepatic dome with perilesional 18F-FDG uptake is seen on PET (A) and calcifications on initial PT/CT (B). Five years later, despite negative serology and negative findings on standard PET (C), treatment was continued because of positive findings on delayed PET (D).
So, theoretically, the decision to interrupt treatment would have been made for a far higher number of patients if only the standard 18F-FDG PET had been considered. The inclusion of delayed acquisition reduced this number from 26 to 15 patients; the inclusion of negative serology further reduced this number to 7 (Table 3).
Among these 7 patients, the serology was totally negative in 5 patients. In 2 patients, the serology was borderline-positive, but since it had remained stable for 26 and 11 mo in the absence of perilesional 18F-FDG uptake on delayed 18F-FDG PET, benzimidazole was stopped nevertheless and the patients were followed up more closely; one of these patients wanted to become pregnant, in which case benzimidazole drugs need to be discontinued as they are teratogenic (5). All 7 patients, including the patients with borderline serology, had an uneventful favorable outcome after treatment interruption (mean duration of follow-up, 23 mo; range, 8–37 mo); there was no evidence of disease recurrence, and no positive 18F-FDG PET findings (either at the standard or the delayed acquisition) were observed during the follow-up.
If the serology was strongly positive, the decision on treatment interruption was never made by clinicians on the basis of negative serology alone or on the basis of negative 18F-FDG PET alone, whatever the acquisition time.
DISCUSSION
Benzimidazoles are the only established medical therapy for human AE. Although the efficacy of these drugs in AE is well established, they often induce significant and sometimes severe side-effects, and the cost in terms of public health and quality of life is high (24). Thus, a major goal for the clinicians in charge of AE patients receiving long-term benzimidazole treatment is to select patients in whom treatment might be safely interrupted.
Aborted forms of AE, which may occur spontaneously (25,26), have also been observed after years of medical treatment (27). Thus, although benzimidazoles are largely considered to be parasitostatic, such reports suggest that in some cases they may be parasitocidal and that their administration might be safely stopped after several years of treatment in selected cases (27,28). Nevertheless, selecting such cases, that is, asserting the abortive evolution of AE under treatment and, even more, predicting this issue, is currently impossible using the imaging techniques that are otherwise recognized to give reliable information for diagnosis of the disease or of its complications. Histopathologic examination, which would be the gold standard, cannot be done as by definition these patients are inoperable; percutaneous biopsy would be only partial and thus misleading and unethical as well.
Previous studies have demonstrated the value of standard 18F-FDG PET in the follow-up of patients with AE, and this imaging procedure is currently considered the best surrogate marker of parasite viability. It has especially been proposed for the detection of patients in whom the parasite had become inactive and in whom treatment interruption could be programmed (7,8,10–12,22,23).
To our knowledge, our study was the first to systematically analyze the use of delayed 18F-FDG PET in AE patients; it also included the largest population ever studied with 18F-FDG PET. As observed in liver cancer, better AE lesion detection on delayed 18F-FDG PET images was due to both reduction of liver background activity and perilesionally increased 18F-FDG uptake (14–18). However, in AE, the nature of cells involved in 18F-FDG uptake is still unknown. The parasitic tissue (germinal layer) is surrounded by an acellular laminated layer that is in direct contact with cells of the immune response—macrophages, lymphocytes, eosinophils, and other effector cells such as fibroblasts and myofibroblasts—all of which together constitute the periparasitic granuloma (29). The perilesional location of 18F-FDG uptake, as well as negative findings at the early acquisition time despite the presence of viable parasite, suggests that the periparasitic immune infiltrate is responsible for the increased uptake of 18F-FDG in AE. Unlike most of the usual inflammatory or infectious diseases that have been studied using 18F-FDG PET (30,31), AE lesions do not include any polymorphonuclear neutrophils, thus perhaps explaining why delayed acquisition reinforced the PET images rather than decreasing the signal on dual-time-point imaging. A rather unusual metabolism of the periparasitic immune cells that are maintained in a chronic status of tolerance might also explain an increase in 18F-FDG uptake with time (32). Specific studies are currently being performed to better understand this apparently paradoxic phenomenon.
Nevertheless, whatever the precise mechanism of 18F-FDG uptake in this parasitic disease, the clinical relevance of 18F-FDG PET finds more support in the demonstration of a better sensitivity of delayed PET. In our study, the use of delayed image acquisition prevented 11 patients from erroneously undergoing an interruption of benzimidazole therapy that was initially indicated by the standard 18F-FDG PET results.
In fact, ethical issues were raised and the search for appropriate surrogate markers of parasite viability was reactivated after the rather disappointing results of the structured treatment interruption based on standard 18F-FDG PET (specific serology was not considered in these studies); in the group of 15 patients with negative 18F-FDG PET, 18-mo treatment interruption provoked clinical recurrence in 2 patients and reactivation of perilesional 18F-FDG uptake in 6 patients (12). Because the WHO IWGE raised some caution at its expert consensus international meeting in 2007 (5), no more treatment interruptions were performed on patients with negative findings on the standard 18F-FDG PET acquisition and positive findings on the delayed 18F-FDG PET acquisition. In June 2007 at our center (just before the introduction of delayed acquisition in routine), clinicians decided to stop albendazole treatment in one patient who also had fully negative serology after more than 10 y of treatment; this decision was based on a negative result on the standard 18F-FDG PET. The treatment interruption was followed by a reincrease in specific Em2+ serology, confirmed by a reincrease in specific anti-Em18 serology. The disease course of this patient has been published elsewhere (21). One year after the treatment interruption, 18F-FDG PET showed clear 18F-FDG uptake at the delayed acquisition, and albendazole treatment was resumed in this patient.
Thus, neither Em2+ serology nor 18F-FDG PET can be considered a gold standard technique to determine parasite viability. In the 7 patients with negative delayed 18F-FDG PET and negative serology, our observations of a favorable outcome and permanent 18F-FDG PET negativity after an 8- to 37-mo period without any treatment confirmed that combined follow-up is necessary to improve the sensitivity of both techniques and to make a safer decision on treatment interruption. Indeed, in a recent evaluation of the outcome of patients with liver transplantation for AE who had residual or recurrent lesions, the results of delayed 18F-FDG PET and the noncommercialized Em18 ELISA, but also the easily available Em2+ ELISA, were well correlated and the 20-y follow-up suggested that the combination of these surrogate markers could provide the best indication for treatment interruption (21).
Because one of the main issues concerning nonoperable AE patients is the selection of patients in whom the treatment can be stopped without recurrence, negative predictive value is clinically more important than positive predictive value. Our study showed that both parameters were improved by using delayed 18F-FDG PET and serology.
CONCLUSION
Our study demonstrated the value of delayed 18F-FDG PET in the follow-up of AE patients. Because of the possibility of parasite reactivation in AE, delayed 18F-FDG PET acquisition (3 h after the injection) should be performed to confirm a negative result in a standard acquisition. Indeed, delayed 18F-FDG PET improves the sensitivity of this technique.
Combined follow-up with delayed 18F-FDG PET and serology is a reliable method for discriminating between active and inactive AE lesions and may be useful in selecting patients in whom benzimidazole is parasitocidal. In such patients, the treatment can safely be discontinued. This approach could markedly improve cost-effectiveness and quality of life in at least some selected AE patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 9, 2013
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 13, 2012.
- Accepted for publication September 26, 2012.





{kind=link}
{kind=link}