


Abstract
Tumor hypoxia is well known to be radiation resistant. 18F-fluoromisonidazole (18F-FMISO) PET has been used for noninvasive evaluation of hypoxia. Quantitative evaluation of 18F-FMISO uptake is thus expected to play an important role in the planning of dose escalation radiotherapy. However, the reproducibility of 18F-FMISO uptake has remained unclarified. We therefore investigated the reproducibility of tumor hypoxia by using quantitative analysis of 18F-FMISO uptake. Methods: Eleven patients with untreated head and neck cancer underwent 2 18F-FMISO PET/CT scans (18F-FMISO1 and 18F-FMISO2) with a 48-h interval prospectively. All images were acquired at 4 h after 18F-FMISO injection for 10 min. The maximum standardized uptake (SUVmax), tumor-to-blood ratio (TBR), and tumor-to-muscle ratio (TMR) of 18F-FMISO uptake were statistically compared between the 2 18F-FMISO scans by use of intraclass correlation coefficients (ICCs). The hypoxic volume was calculated as the area with a TBR of greater than or equal to 1.5 or the area with a TMR of greater than or equal to 1.25 to assess differences in hypoxic volume between the 2 18F-FMISO scans. The distances from the maximum uptake locations of the 18F-FMISO1 images to those of the 18F-FMISO2 images were measured to evaluate the locations of 18F-FMISO uptake. Results: The SUVmax (mean ± SD) for 18F-FMISO1 and 18F-FMISO2 was 3.16 ± 1.29 and 3.02 ± 1.12, respectively, with the difference between the 2 scans being 7.0% ± 4.6%. The TBRs for 18F-FMISO1 and 18F-FMISO2 were 2.98 ± 0.83 and 2.97 ± 0.64, respectively, with a difference of 9.9% ± 3.3%. The TMRs for 18F-FMISO1 and 18F-FMISO2 were 2.25 ± 0.71 and 2.19 ± 0.67, respectively, with a difference of 7.1% ± 5.3%. The ICCs for SUVmax, TBR, and TMR were 0.959, 0.913, and 0.965, respectively. The difference in hypoxic volume based on TBR was 1.8 ± 1.8 mL, and the difference in hypoxic volume based on TMR was 0.9 ± 1.3 mL, with ICCs of 0.986 and 0.996, respectively. The maximum uptake locations of the 18F-FMISO1 images were different from those of the 18F-FMISO2 images and were within the full width at half maximum of the PET/CT scanner, except in 1 case. Conclusion: The values for 18F-FMISO PET uptake and hypoxic volume in head and neck tumors between the 2 18F-FMISO scans were highly reproducible. Such high reproducibility of tumor hypoxia is promising for accurate radiation planning.
It has been well established that hypoxic regions of tumors are radiation resistant and that head and neck cancers with substantial areas of hypoxia are associated with a poor prognosis (1,2). 18F-fluoromisonidazole (18F-FMISO) PET has been used for noninvasive evaluation of hypoxia, and 18F-FMISO uptake is related to patient prognosis (3–6). Quantitative evaluation of 18F-FMISO uptake is expected to play an important role in the planning of dose escalation radiotherapy (7–9). However, the reproducibility of 18F-FMISO uptake has remained unclarified. A single report has indicated a low reproducibility of 18F-FMISO uptake (10). In that report, the hypoxic volume was calculated on the basis of the tumor-to-blood ratio (TBR). However, there has been no report evaluating the stability of radioactivity in the blood pool. On the other hand, another report has shown a correlation between the values obtained from a tumor-to-muscle ratio (TMR) evaluation of 18F-FMISO PET and pO2 polarography (11), indicating that TMR is a suitable marker of tumor hypoxia.
We postulated that high-resolution, high-contrast 18F-FMISO images collected by use of a state-of-the art PET camera might provide a high reproducibility of tumor hypoxia. Therefore, the aim of this study was to investigate the reproducibility of 18F-FMISO uptake by use of quantitative analysis, including TBR and TMR.
MATERIALS AND METHODS
Patients
Patients with untreated head and neck cancer were prospectively enrolled in this study. Signed informed consent was obtained in all cases, and this study was approved by the Institutional Review Board of Hokkaido University. Twelve patients were recruited between June 2010 and March 2012 at Hokkaido University Hospital. Technical problems prevented adequate collection of the 18F-FMISO scan in 1 patient. Therefore, 18F-FMISO images were analyzed for 11 patients, including 4 patients with nasopharyngeal cancer, 1 with oropharyngeal cancer, 2 with hypopharyngeal cancer, 2 with laryngeal cancer, 1 with maxillary sinus cancer, and 1 with ethmoid sinus cancer (Table 1).
Characteristics of Patients*
18F-FMISO PET
Patients underwent 2 18F-FMISO PET/CT scans (18F-FMISO1 and 18F-FMISO2) with a 48-h interval. All images were acquired at 4 h after injection of 18F-FMISO for 10 min in the 3-dimensional mode with a PET/CT scanner (TruePoint Biograph with TrueV Option; Siemens Japan). Compared with the scanner without the true V option (axial field of view, 16.2 cm), the TruePoint Biograph with the TrueV Option had an extended axial field of view (21.6 cm), sensitivity that was 1.82 times higher, and a comparable scatter fraction (32% of the National Electrical Manufacturers Association standard NU 2-2007) (12). The images were reconstructed with the iterative TrueX reconstruction method, which included partial-volume correction (13). The full width at half maximum after reconstruction was 8 mm, and the slice thickness was 3 mm. Venous blood sampling was performed immediately after scanning.
Image Analysis
18F-FMISO PET images were analyzed quantitatively, including assessment of the maximum standardized uptake value (SUVmax), TBR, and TMR. The SUVmax was calculated as the activity concentration/(injected dose/body weight). The TBR was derived as the maximum concentration of the tumor divided by the concentration of blood collected from venous blood sampling. For calculation of the TMR, a region of interest was placed over the primary lesion and posterior cervical muscle. The TMR was then defined as the tumor uptake divided by the uptake of the posterior cervical muscle. The hypoxic volume was also calculated to evaluate the reproducibility of hypoxia clinically. Although a threshold for the definition of hypoxia has not been formally established, a TBR of greater than or equal to 1.5 was defined as hypoxia for the calculation of hypoxic volume based on TBR (HV-TBR) in this study; the threshold for hypoxic volume based on TMR (HV-TMR) was set at 1.25.
CT images from the first and second PET/CT scans were coregistered by maximization of mutual information on a Windows XP (Microsoft) workstation, and 18F-FMISO PET images were coregistered with the same parameters (14). The distances from the maximum uptake locations of the 18F-FMISO1 images to those of the 18F-FMISO2 images were measured to evaluate the locations of 18F-FMISO uptake.
Statistical Analyses
For statistical analyses of the reproducibility of 18F-FMISO uptake and hypoxic volume, the intraclass correlation coefficients (ICCs) were calculated for SUVmax, TBR, TMR, HV-TBR, and HV-TMR. In addition, SDs in the paired data were statistically compared between TBR and TMR and between HV-TBR and HV-TMR (15). Bland–Altman analysis was used for evaluation of the differences in these parameters (16). Because tumors expand in an exponential fashion, log10-scale analyses were added for HV-TBR and HV-TMR. We also calculated Pearson correlation coefficients for all patients from scatterplots of 18F-FMISO1 versus 18F-FMISO2. Plots were extracted from 3-dimensional regions of interest that covered all of the hypoxic area in the tumor. P values of less than 0.05 were considered to indicate statistical significance. Statistical analyses were performed with JMP version 10 software (SAS Institute Inc.).
RESULTS
The 11 patients ranged in age from 44 to 78 y (mean ± SD, 62.0 ± 11.9). The injected dose of 18F-FMISO was 414 ± 26 MBq, and the time interval between injection and the start of the scan was 262 ± 21 min. Because 1 patient had a problem with blood sampling, blood data for this patient were excluded from analysis (Table 1). There were no statistically significant differences in the injected dose, time interval, SUVmax, TBR, or TMR between 18F-FMISO1 and 18F-FMISO2 (Table 2).
Parameters of 2 18F-FMISO PET Studies and Distances Between 18F-FMISO1 and 18F-FMISO2 Maximum Uptake Locations
The SUVmax (mean ± SD) for 18F-FMISO1 and 18F-FMISO2 was 2.08 ± 1.18, with a range of 1.21–5.01 (Table 2). The difference in SUVmax between the 2 18F-FMISO studies was 7.0% ± 4.6% (range, 1.2%–11.7%). The TBR (mean ± SD) was 2.98 ± 0.72 (range, 1.76–4.71), and the difference in TBR between the 2 18F-FMISO studies was 9.9% ± 3.3% (range, 3.4%–14.5%). The TMR (mean ± SD) was 2.23 ± 0.67 (range, 1.22–3.82), and the difference in TMR between the 2 18F-FMISO studies was 7.1% ± 5.3% (range, 0.4%–15.3%). The ICCs for SUVmax, TBR, and TMR were 0.959, 0.913, and 0.965, respectively (Fig. 1). The SD for the difference in TMR was significantly smaller than that for the difference in TBR (P = 0.04).
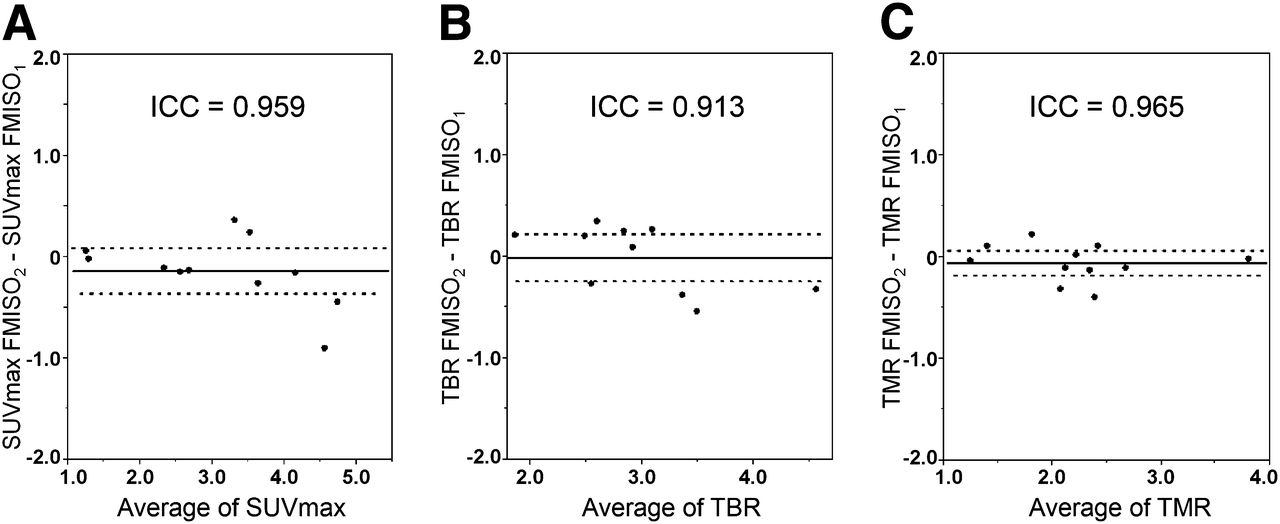
Bland–Altman plots of SUVmax (A), TBR (B), and TMR (C) of 18F-FMISO1 and 18F-FMISO2. Lines show combined mean and 95% confidence interval. SD of difference for TMR was significantly smaller than that for TBR (P = 0.04).
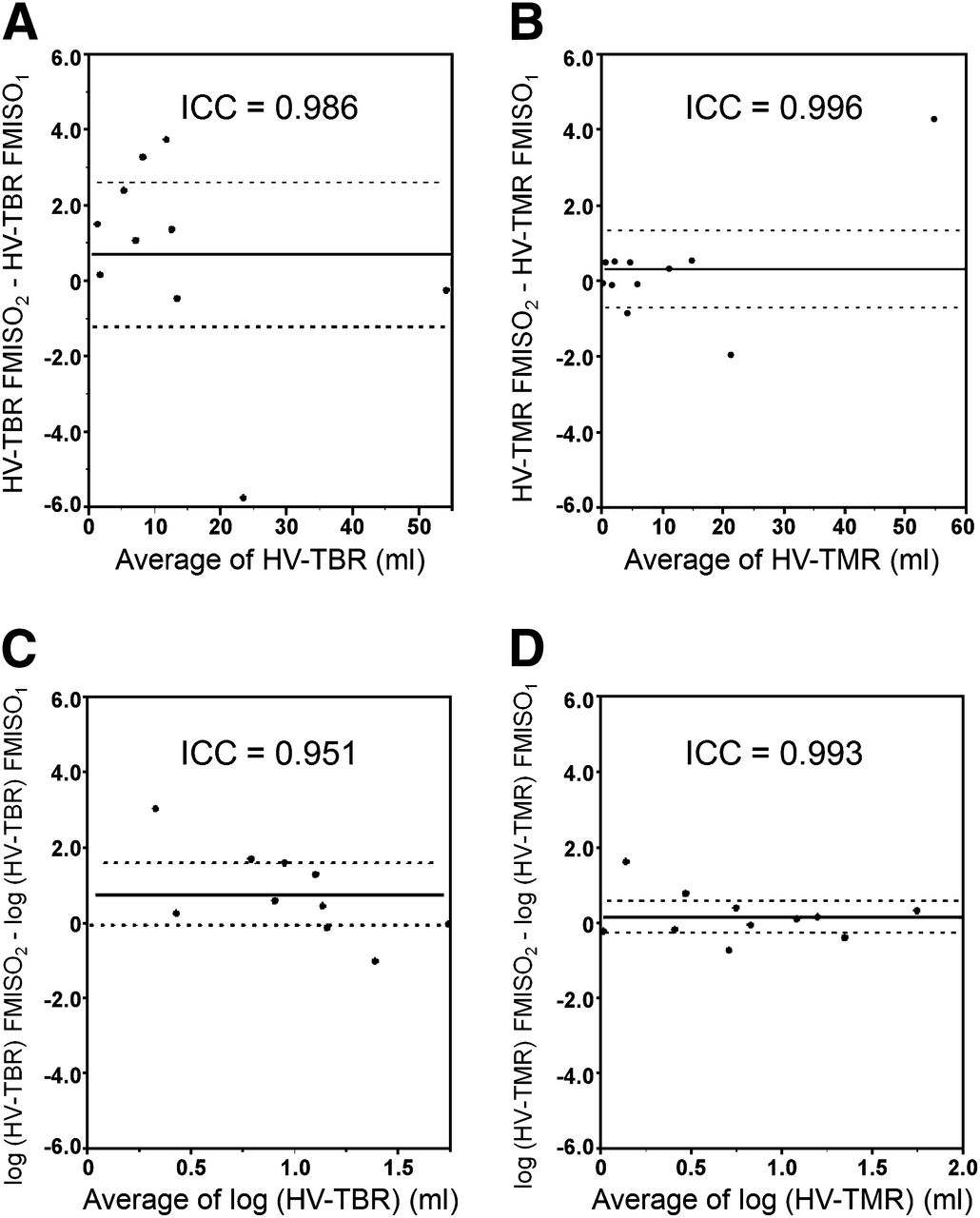
HV-TBR ranged from 0.5 mL to 54.3 mL. The difference between 18F-FMISO1 and 18F-FMISO2 was 1.8 ± 1.8 mL. HV-TMR ranged from 0.0 mL to 56.8 mL, and the difference was 0.9 ± 1.3 mL. The ICCs for HV-TBR, HV-TMR, log HV-TBR, and log HV-TMR were 0.986, 0.996, 0.951, and 0.993, respectively (Fig. 2). The SD for the difference in log HV-TMR was also significantly smaller than that for the difference in log HV-TBR (P = 0.03).
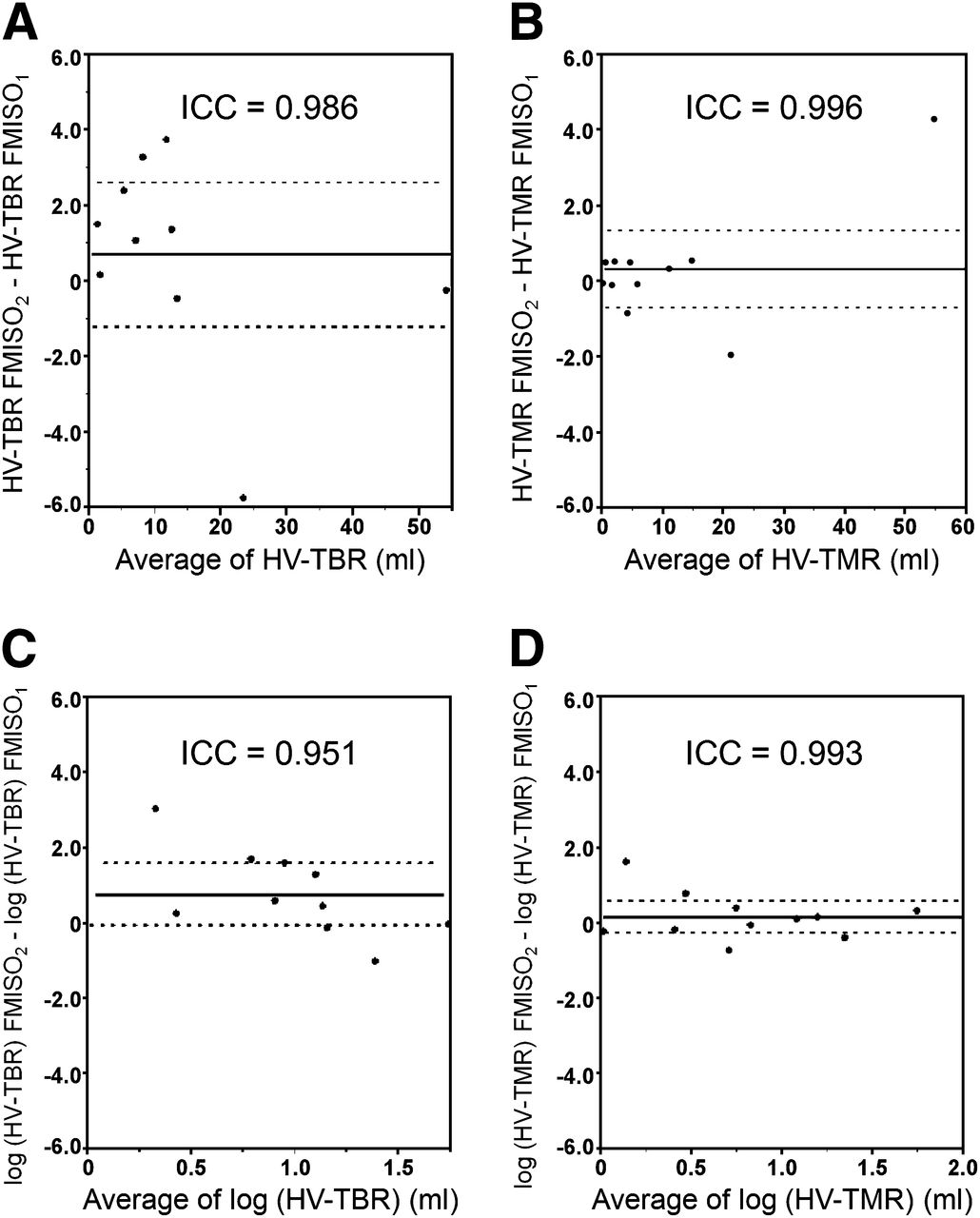
Bland–Altman plots of HV-TBR (A), HV-TMR (B), log HV-TBR (C), and log HV-TMR (D). Lines show combined mean and 95% confidence interval. SD of difference for log HV-TMR was significantly smaller than that for log HV-TBR (P = 0.03).
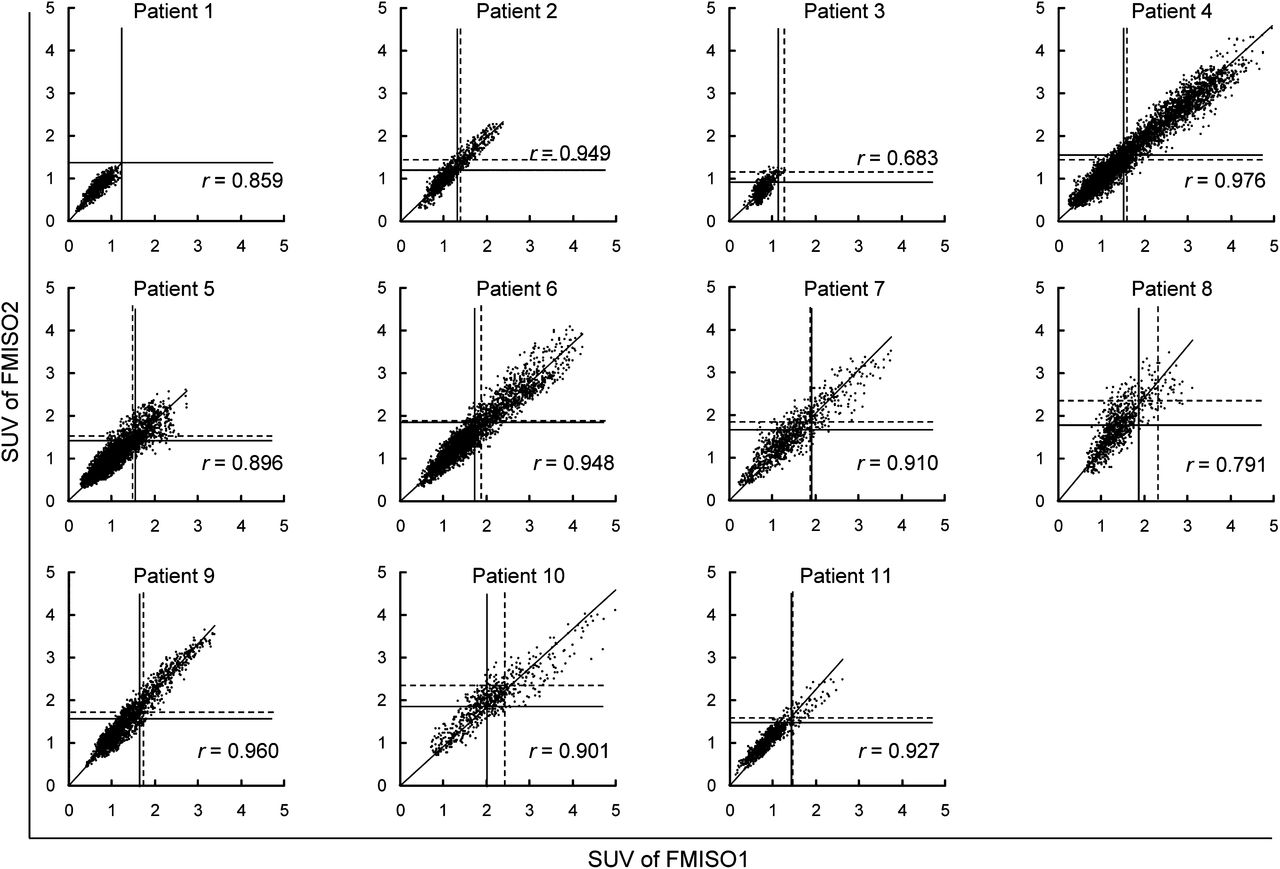
Figure 3 shows scatterplots of 18F-FMISO1 versus 18F-FMISO2 for all patients. The straight line represents a TBR of 1.5, and the dotted line represents a TMR of 1.25. Of the 11 patients, 7 had ICCs of greater than 0.9.

Scatterplots of tumor voxel SUV of 18F-FMISO1 vs. tumor voxel SUV of 18F-FMSO2 for each patient. Solid lines indicate TBR of 1.5, and broken lines indicate TMR of 1.25.
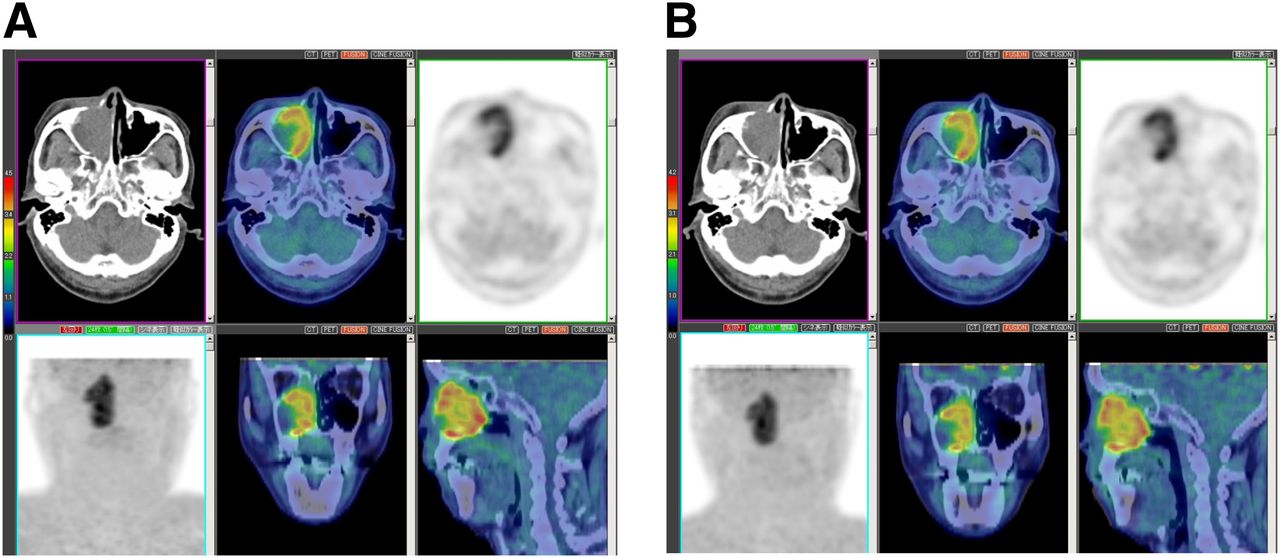
The distance between the maximum uptake location of 18F-FMISO1 and that of 18F-FMISO2 was 4.3 ± 3.0 mm. This distance was smaller than the full width at half maximum of the PET/CT scanner (8 mm), except in 1 case. In that 1 case, the 11.8-mm distance had 2 peaks with similar 18F-FMISO uptake values, and the maximum uptake of 18F-FMISO1 was located at a peak different from that of 18F-FMISO2. The locations of the 2 peaks were different—that is, 2.3 and 3.3 mm—and both were within the full width at half maximum of the PET/CT scanner (Fig. 4).

18F-FMISO imaging of patient 9, who had hypopharyngeal cancer. Distance between maximum uptake on 18F-FMISO1 image (A) and that on 18F-FMISO2 image (B) was 11.8 mm. On 18F-FMISO1 image, maximum uptake was observed at SUVmax of 3.40 (white arrow). On 18F-FMISO2 image, maximum uptake was observed at another peak (SUVmax, 3.64) (black arrow). Locations of peaks (white arrow and black arrow) were different—that is, 2.3 and 3.3 mm, respectively.
Another representative case (maxillary sinus cancer) is shown in Figure 5. The values for SUVmax (4.95 vs. 4.91), TBR (4.71 vs. 4.39), TMR (3.82 vs. 3.80), HV-TBR (54.3 vs. 54.1 mL), and HV-TMR (52.5 vs. 56.8 mL) were similar. The distance between the maximum uptake of 18F-FMISO1 and that of 18F-FMISO2 was 4.3 mm.
18F-FMISO imaging of patient 4, who had maxillary sinus cancer. Uptake of 18F-FMISO on 18F-FMISO1 image (A) was similar to that on 18F-FMISO2 image (B). Distance between maximum uptake on 18F-FMISO1 image and that on 18F-FMISO2 image was 4.3 mm (smaller than full width at half maximum of PET scanner). Values for SUVmax (4.95 vs. 4.91), TBR (4.71 vs. 4.39), TMR (3.82 vs. 3.80), HV-TBR (54.3 vs. 54.1 mL), and HV-TMR (52.5 vs. 56.8 mL) were similar.
DISCUSSION
To our knowledge, this is the first report to demonstrate a high reproducibility of 18F-FMISO uptake through the use of major methods of 18F-FMISO analysis, such as SUVmax, TBR, TMR, HV-TBR, HV-TMR, and the location of maximum 18F-FMISO uptake. Validation of the reproducibility of 18F-FMISO uptake is critically important for clinical applications, because various factors, including acute hypoxia, might cause changes in the hypoxic area between the 18F-FMISO study and the actual radiation planning. Such high reproducibility of tumor hypoxia is promising for accurate radiation planning.
Our results for the reproducibility of tumor hypoxia evaluated by 18F-FMISO uptake were different from those obtained by Nehmeh et al. (10). There are several possible reasons for the discrepancy. First, the time interval from 18F-FMISO injection to scanning in the study of Nehmeh et al. (10) was short and variable among patients (117–195 min). The images with short time intervals included 18F-FMISO accumulation in the blood pool (17,18). We considered 18F-FMISO imaging at 4 h after injection to be more suitable than imaging in less than 3 h, as used in several other studies (3–5,7–11), for the following reasons. Because blood clearance of 18F-FMISO is rather slow, residual blood pool activity at 1–3 h remains relatively high. Such high blood pool activity might cause poor reproducibility of the tumor-to-blood pool activity ratio and decrease image quality. However, high-quality 18F-FMISO images were obtained even at 4 h after 18F-FMISO administration, as shown in Figures 4 and 5. Therefore, a high reproducibility of several hypoxic parameters was observed on 18F-FMISO images obtained at 4 h after injection. Unfortunately, we did not compare the reproducibilities of 18F-FMISO images at 2 and 4 h after tracer administration with the same PET camera. Such a comparison would be the next step in confirming the value of 18F-FMISO imaging at 4 h.
Second, PET was performed in the 2-dimensional mode with a short scanning time (8 min) in the study of Nehmeh et al. (10). In the present study, 18F-FMISO images were obtained for 10 min with 3-dimensional acquisition on a PET/CT system with high spatial resolution and high sensitivity (19,20). In addition, those images were reconstructed with the iterative TrueX reconstruction method, which included partial-volume correction. Therefore, we obtained images with high contrast and low statistical noise as well as stable 18F-FMISO uptake.
The hypoxic area in a tumor has been reported to include chronic hypoxia and acute hypoxia (1,21). Acute hypoxia can change every few hours or days. Therefore, acute hypoxia could have changed the distribution of 18F-FMISO uptake between the 2 18F-FMISO studies. In the present investigation, no case showed major changes in SUVmax, TBR, TMR, HV-TBR, and HV-TMR. Our results did not indicate an effect of acute hypoxia on 18F-FMISO studies with a 48-h interval. Mönnich et al. (22) reported that acute hypoxia did not influence the reproducibility of PET imaging in simulations. Our results are consistent with their report.
Dose escalation for a hypoxic tumor is an important consideration for improving the effect of radiotherapy (23–25). The definition of hypoxic volume is essential for choosing the target for dose escalation. The high reproducibility of tumor hypoxia evaluated by 18F-FMISO uptake offers hope for defining the hypoxic area. In the present study, the hypoxic area was defined as the area with a TBR of greater than or equal to 1.5 or a TMR of greater than or equal to 1.25. The threshold for TBR has been not established, so different thresholds (from 1.2 to 1.4) have been used in various reports (5,10,26–28). The threshold for TBR (1.5) in the present study was higher than those in previous studies. The reason was that the time interval (4 h) between 18F-FMISO injection and scanning in the present study was longer than those in previous studies (from 2 to 3 h) and resulted in higher lesion contrast and less background activity. The threshold for TMR (1.25) was determined as the upper limit of the 95% confidence interval for normal muscle uptake in 11 people without carcinoma. These thresholds are not widely used.
Another study is needed to determine a more appropriate threshold for applying 18F-FMISO PET to clinical dose escalation in patients. For clinical practice, immobilization of a patient’s head and neck is important. We immobilized them by using a dedicated device for the PET/CT scanner. When possible, 18F-FMISO PET with immobilization devices, such as radiation treatment masks, would be helpful for the delineation of dose painting in dose escalation radiotherapy.
Our results indicated that TMR analysis yielded better reproduction of tumor hypoxia than TBR analysis. TMR analysis is a unique quantitative method that has been shown to be correlated with pO2 polarography (11). TBR analysis typically has been used for quantification of 18F-FMISO uptake and definition of the hypoxic area. However, this method requires blood sampling, which is invasive for patients and can introduce technical mistakes. In contrast, TMR analysis is a noninvasive, simple quantitative method. Our results indicate that TMR analysis is a potential alternative for TBR analysis. However, TMR analysis has some limitations related to the uptake of 18F-FMISO in the posterior muscles of the neck, which is seen in most people. Therefore, the accuracy of TMR analysis should be investigated in another study.
The present study has several limitations. The major limitation is that the number of patients was small. Although our data were limited in this regard, it was important to promptly report the high reproducibility of 18F-FMISO uptake to advance 18F-FMISO investigations. Another study with a larger number of patients may establish not only reproducibility but also a definition of the hypoxic area. Second, the hypoxic volume in the present study was smaller than that in a previous study (10) because our study included early-stage cases (stage I). Although our data could not provide enough evidence of reproducibility over a large hypoxic area, we were able to demonstrate high reproducibility even in small hypoxic lesions. Third, the present study did not include women. We believe that this factor is incidental because many head and neck cancers (e.g., nasopharyngeal, oropharyngeal, and laryngeal cancers) occur mostly in men. Additionally, we did not compare the reproducibilities of 18F-FMISO images at 2 and 4 h after tracer administration or 2-dimensional and 3-dimensional acquisitions with the same PET camera.
CONCLUSION
The reproducibility of quantitative evaluation of tumor hypoxia by18F-FMISO PET was high. Such high reproducibility in terms of hypoxic location and area is promising for the accurate delineation of dose painting in dose escalation radiotherapy with 18F-FMISO PET.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank radiologic technologists Hidehiko Omote, Yamato Munakata, Kazumi Kawanabe, and Junya Katahata for their excellent technical assistance and PET scanning. We also thank Ken-ichi Nishijima and Norifumi Abo for synthesis of 18F-FMISO and Shuichi Takinami for performance of 18F-FMISO PET.
Footnotes
Published online Jan. 15, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 17, 2012.
- Accepted for publication September 18, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Development of 18F-Fluoromisonidazole Hypoxia PET/CT Diagnostic Interpretation Criteria and Validation of Interreader Reliability, Reproducibility, and Performance
- PET/CT in the Evaluation of Hypoxia for Radiotherapy Planning in Head and Neck Tumors: Systematic Literature Review
- Mitochondrial Inhibitor Atovaquone Increases Tumor Oxygenation and Inhibits Hypoxic Gene Expression in Patients with Non-Small Cell Lung Cancer
- Tumor Hypoxia Detected by 18F-fluoromisonidazole Positron Emission Tomography (FMISO PET) as a Prognostic Indicator of Radiotherapy (RT)
- 18F-Fluoromisonidazole Kinetic Modeling for Characterization of Tumor Perfusion and Hypoxia in Response to Antiangiogenic Therapy
- Multiparametric Imaging of Tumor Hypoxia and Perfusion with 18F-Fluoromisonidazole Dynamic PET in Head and Neck Cancer
- In Vivo Quantification of Hypoxic and Metabolic Status of NSCLC Tumors Using [18F]HX4 and [18F]FDG-PET/CT Imaging
- 18F-Fluoromisonidazole PET Uptake Is Correlated with Hypoxia-Inducible Factor-1{alpha} Expression in Oral Squamous Cell Carcinoma