


Abstract
The presence of estrogen receptor (ER) in breast cancer is a prognostic indicator for both disease-free and overall survival. 16α-18F-fluoro-17β-estradiol (18F-FES) with PET is a noninvasive test for evaluation of ER expression and has been used for predicting response to endocrine therapy in patients with ER-positive metastatic breast cancer. The purpose of this study was to correlate 18F-FES PET and ER expression in patients with primary, operable breast cancer. Methods: Forty-eight patients were prospectively enrolled in an institutional review board–approved protocol and signed an informed consent form. All patients had undergone 18F-FES PET preoperatively. Clinical characteristics, tumor characteristics, and treatment outcomes were recorded. Immunohistochemical analysis for ER and progesterone receptor (PgR) percentage expression (46 surgical, 2 core biopsy specimens) was performed. 18F-FES PET standardized uptake value (SUV) of the breast lesion was correlated with percentage immunohistochemistry ER and PgR expression. 18F-FES PET SUV was quantified, with a value of 1.5 or more considered positive, and ER and PgR was quantified, with 1% or more considered positive. Formalin-fixed paraffin-embedded tissue was available for 44 patients (42 surgical, 2 core biopsy specimens). We used a microarray platform, and estrogen-related gene expression data (ESR1, ESR2, and PGR) were compared with 18F-FES PET SUV (Spearman rank correlation). Tumor size, ductal histology, grade, HER2-neu overexpression, PgR expression, estradiol level, body mass index (BMI), and lean BMI were compared with 18F-FES PET uptake using univariate and multivariate analysis. Results: Forty-eight patients completed our protocol, and 2 patients did not undergo surgery because bone metastases were identified preoperatively on 18F-FES PET. Eighty-three percent of our patients were stage I or II, with a median tumor size of 1.9 cm. Forty-one patients underwent a sentinel node biopsy. Twenty-one patients had nodal involvement. 18F-FES PET identified 5 patients with axillary nodal uptake (median SUV, 3.0; range, 1.7–6.9). These 5 patients had ER-positive breast cancer, and all had more than 4 positive nodes at the time of axillary node dissection. 18F-FES PET SUV was associated with immunohistochemistry ER expression. The sensitivity and specificity of the 18F-FES PET for the breast lesion were 0.85 and 0.75, respectively. Estrogen and progesterone gene expression (ESR1, ESR2, and PGR) was not associated with 18F-FES PET SUV (Spearman rank correlation). We found a significant correlation between 18F-FES PET SUV and tumor size (P = 0.0015) but not with ductal histology, grade, HER2-neu overexpression, PgR, estradiol, BMI, or lean BMI (logistic regression). ER expression (P < 0.001) and tumor size (P < 0.0001) were significant on multivariate regression analysis. Conclusion: 18F-FES PET SUV correlated with ER immunohistochemistry expression but not gene expression in our patients with early breast cancer. We found that size of primary tumor was significantly associated with 18F-FES PET SUV. 18F-FES PET is highly predictive for metastatic disease and helped in the identification of patients with metastatic disease in a preoperative setting.
The presence of estrogen receptor (ER) in breast cancer is an important prognostic indicator for both disease-free survival and overall mortality in breast cancer. The presence of ER or progesterone receptor (PgR) is required for the use of endocrine therapy, making it one of the most important predictive factors in breast cancer management (1).
Currently, the ER status of a breast tumor is assessed through an immunohistochemistry assay performed on thin sections of tumor tissue (2). However, this method has high and consistent rates of intralaboratory and interlaboratory variability, which in turn makes it difficult to determine the true rates of ER tumor expression. Also, there is intrinsic heterogeneity of receptor content within the same lesion, as well as variations in receptor status among the primary and metastatic sites (3,4). Immunohistochemistry is the method currently used for making clinical therapy decisions at most centers. However, the presence of the ER receptor in a tumor is not predictive of a functional ER. This is evident in that not all patients with ER-positive breast cancers respond to endocrine therapy (5).
16α-18F-fluoro-17β-estradiol (18F-FES) PET is a noninvasive test that can simultaneously measure the in vivo delivery and binding of estrogens, and thus ER expression, at multiple sites (6). Multiple studies have validated 18F-FES PET uptake as a predictor of response to endocrine therapy in patients with locally advanced or metastatic breast cancer (7–11).
The purpose of this study was to correlate 18F-FES PET and ER expression in patients with primary, operable breast cancer.
MATERIALS AND METHODS
This 18F-FES study was performed under the authority of title 21 of Code of Federal Regulations part 361.1 and was approved by the Memorial Sloan-Kettering Cancer Center Radioactive Drug Research Committee and institutional review board.
Eligible patients were enrolled during the preoperative surgical consultation and gave informed, written consent. Eligibility criteria included women with intact, histologically confirmed invasive breast cancer at least 1 cm in size. Ineligibility criteria included a prior breast cancer diagnosis, known active infection, autoimmune or inflammatory disease, prior radiation therapy to the affected breast, chemotherapy (including neoadjuvant chemotherapy), and prior endocrine therapy.
Serum estradiol levels were measured at the time of preoperative testing or within 30 d before surgery. Estradiol measurements were performed by our clinical laboratory using the RIA Coat-a-Count test (Siemens Healthcare Diagnostics).
Immunostaining for ER and PgR was performed on one 5-μm–thick tissue section processed from a formalin-fixed, paraffin-embedded tumor tissue block (46 surgical and 2 core biopsy specimens) with 6F11 monoclonal antibody for ER and IE2 antibody for PgR using the Benchmark automated system (Ventana).
Immunohistochemistry ER and PgR expression was the percentage of tumor cells with positively staining nuclei as reported by one of the authors in our study, who also procured the tumor tissue for both immunohistochemistry analysis and microarray analysis.
The commercially available Illumina DASL expression microarray platform (Cancer Panel TMv1; Illumina), which is optimized for gene expression analysis from formalin-fixed, paraffin-embedded tissue, was used for this study. This platform contains 502 cancer-related genes with unique probe groups for 3 different sites per gene and uses DASL technology. We selected the estrogen-related genes (ESR1, ESR2, and PGR) for our analysis. Formalin-fixed, paraffin-embedded tissue was available for 44 patients (42 surgical and 2 core biopsy specimens) for the microarray analysis. Clinical characteristics, tumor characteristics, and treatment outcomes were recorded.
18F-FES PET
The synthesis of 18F-FES was based on previously reported methods (12,13). The 18F-FES precursor and chemical standard were purchased from ABX Advanced Biochemical Compounds GmbH. All drug preparations were checked before release for appearance, radiochemical identity, pH, radiochemical purity, chemical purity, and pyrogenicity, and were shown to conform to the set acceptance criteria before human administration. Postrelease sterility testing was performed and was shown to conform to the set acceptance criteria in all cases. All patients received an injection of 185–296 MBq (5–8 mCi) of 18F-FES. The exact time of injection and net dose were recorded. Scans consisted of a whole-body PET/CT examination (3 min per bed position) from the lower neck to the pelvis at 30 min after injection to obtain general information on the biodistribution. This scan was followed by a single 15-min spot view (or in some patients, 2 fields of view) of the chest that included the area of the primary tumor so as to obtain more counts and thereby increase the limits of detectability for the smaller lesions. The total time from injection to completion of imaging was about 90 min. All patients were imaged on a Discovery LS or DSTE PET/CT scanner (GE Healthcare).
All patients underwent 18F-FES PET preoperatively. The images were evaluated prospectively by the study’s 2 nuclear medicine physicians, who were masked to the results of imaging modalities, such as breast MR imaging and mammography, but not to CT, which was used for coregistration. Grading of the results as positive or negative was based on visualization of foci of uptake suggestive of active tumor involvement. A scan was determined to be positive if focal uptake was seen in an area in at least 2 planes and was not at a site of physiologic uptake. Findings were also considered positive if uptake in an area of nonphysiologic accumulation had a standardized uptake value (SUV) of 1.5 or greater. All such sites of abnormal activity in the breast, axillae, mediastinum, or other distant organs, such as the lung, liver, or bones, or in other sites, were noted.
Images were analyzed in 3 ways: a semiquantitative analysis was performed by placing the regions of interest in areas of abnormality and determining SUV normalized to body weight; the tumor-to-nontumor ratio was determined for each site by placing volumetric regions of interest on the tumor using the anatomic CT dataset; and identical regions of interest were drawn in a background area (contralateral breast or other normal soft tissue). The ratio of tumor radioactivity to background radioactivity was recorded.
Statistical Analysis
Paired t test comparison of ER and 18F-FES PET SUV was performed with cutoffs for positivity defined as at least 1% for ER and at least 1.5 SUV for 18F-FES PET. Gene ER and PgR expression and 18F-FES PET SUV were compared with Spearman rank correlation. The relationships between serum estradiol levels, tumor size, histology, grade, PgR expression, body mass index (BMI), lean BMI, and continuous 18F-FES PET SUV were explored using linear regression or ANOVA as appropriate. Multivariate analysis of tumor size, ER percentage, and ductal histology with 18F-FES PET SUV was performed.
RESULTS
Forty-eight patients completed our protocol, and 2 patients did not undergo surgery because bone metastases were identified preoperatively on 18F-FES PET.
Table 1 demonstrates the clinical and pathologic characteristics of our study group. The median age of the patients was 50 y, and most patients (29 [60%]) were premenopausal. The median estradiol level was 25 pg/mL, and only 7 patients reported using hormone replacement therapy at the time of estradiol level measurement. The median BMI was 25 kg/m2, and the median lean BMI was 21 kg/m2. Most patients were stage I or II (40 [83%]), with a median tumor size of 1.9 cm. Forty-four patients (92%) had invasive ductal histology (ductal and mixed ductal/lobular).
Patient Characteristics
Twenty-three patients (50%) had undergone mastectomy, and 23 patients, breast-conserving surgery. Forty-one of 46 patients (89%) had undergone sentinel node biopsy with a combination of blue dye and 99mTc-sulfur colloid on the day of or day before surgery or with blue dye alone on the day of surgery. Six patients had received a 99mTc-sulfur colloid injection on the same day as the 18F-FES injection and had undergone lymphoscintigraphy before receiving the 18F-FES injection.
Twenty-one of 46 patients (46%) had nodal involvement. 18F-FES PET uptake in the axilla was identified in 5 patients (median SUV, 3.0; range, 1.7–6.9). All 5 of these patients had ER-positive breast cancer and more than 4 positive nodes at the completion of axillary node dissection. The mean number of positive lymph nodes was 22 (range, 7–39), with the largest node measuring an average of 2.2 cm (range, 1.2–4.2 cm). There were 16 patients with no 18F-FES PET uptake in the axilla: 6 had immunohistochemistry-only cells, 5 had 1 positive node, and the remaining 5 had 2 positive nodes (3 patients) or 3 positive nodes (2 patients), with the largest node measuring an average of 1.5 cm (range, 0.8–4.5).
18F-FES uptake was identified in 4 bone lesions; 3 patients had undergone fine-needle aspiration biopsy, which confirmed metastasis, and 2 were identified preoperatively and did not have surgery; 1 patient was identified at follow-up. An additional patient had an 18F-FES SUV of 6.6 in a rib lesion, and biopsy revealed fibrous dysplasia. Three of the 4 bone metastases had been assessed for ER and PgR immunohistochemistry expression, with ER immunohistochemistry values of 5%, 90%, and 90% and PgR immunohistochemistry values of 0%, 90%, and 50%, respectively.
Most patients were treated with adjuvant chemotherapy (85%) or endocrine therapy (81%) (Table 2). Oncotype DX (Genomic Health) test results were available in 10 patients, with a median score of 19 (range, 6–46). Seven patients had a distant recurrence; 2 of these had concomitant local recurrence, and 1 patient died of disease (median follow-up, 3.7 y; range, 0.1–5.9 y). The Kaplan–Meier survival curve is shown in Figure 1. The 3-y disease-free interval was 0.88 (95% confidence interval, 0.73–0.95).
Adjuvant Treatment
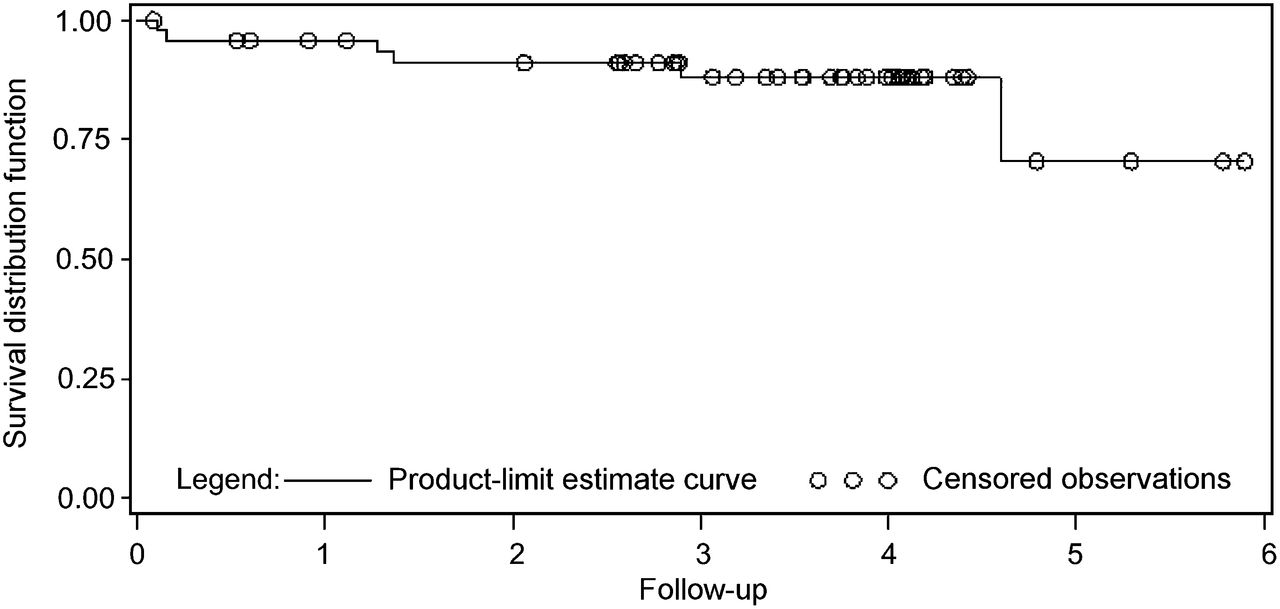
Kaplan–Meier survival analysis for study cohort. Median follow-up was 3.7 y (range, 0.1–5.9 y), with 3-y median disease-free survival of 0.88 (95% confidence interval, 0.73–0.95).
The sensitivity of the 18F-FES PET SUV as compared with immunohistochemistry ER expression was 0.85, and specificity was 0.75. The positive predictive value was 0.94, and the negative predictive value was 0.50 (Table 3). The receiver-operating-characteristic curve for ER expression is shown in Figure 2, with an area under the receiver operating curve of 0.85 (95% confidence interval, 0.71–0.96). The Spearman rank correlation coefficient of several gene expression values (ESR1, 0.01; ESR2, −0.04; and PgR, −0.23) and 18F-FES PET SUV did not show a significant association. We also compared the microarray gene expression and immunohistochemistry ER expression; the Spearman rank correlation was 0.16 and not statistically significant (P = 0.30).
Comparison of Immunohistochemistry ER Expression and 18F-FES PET SUV
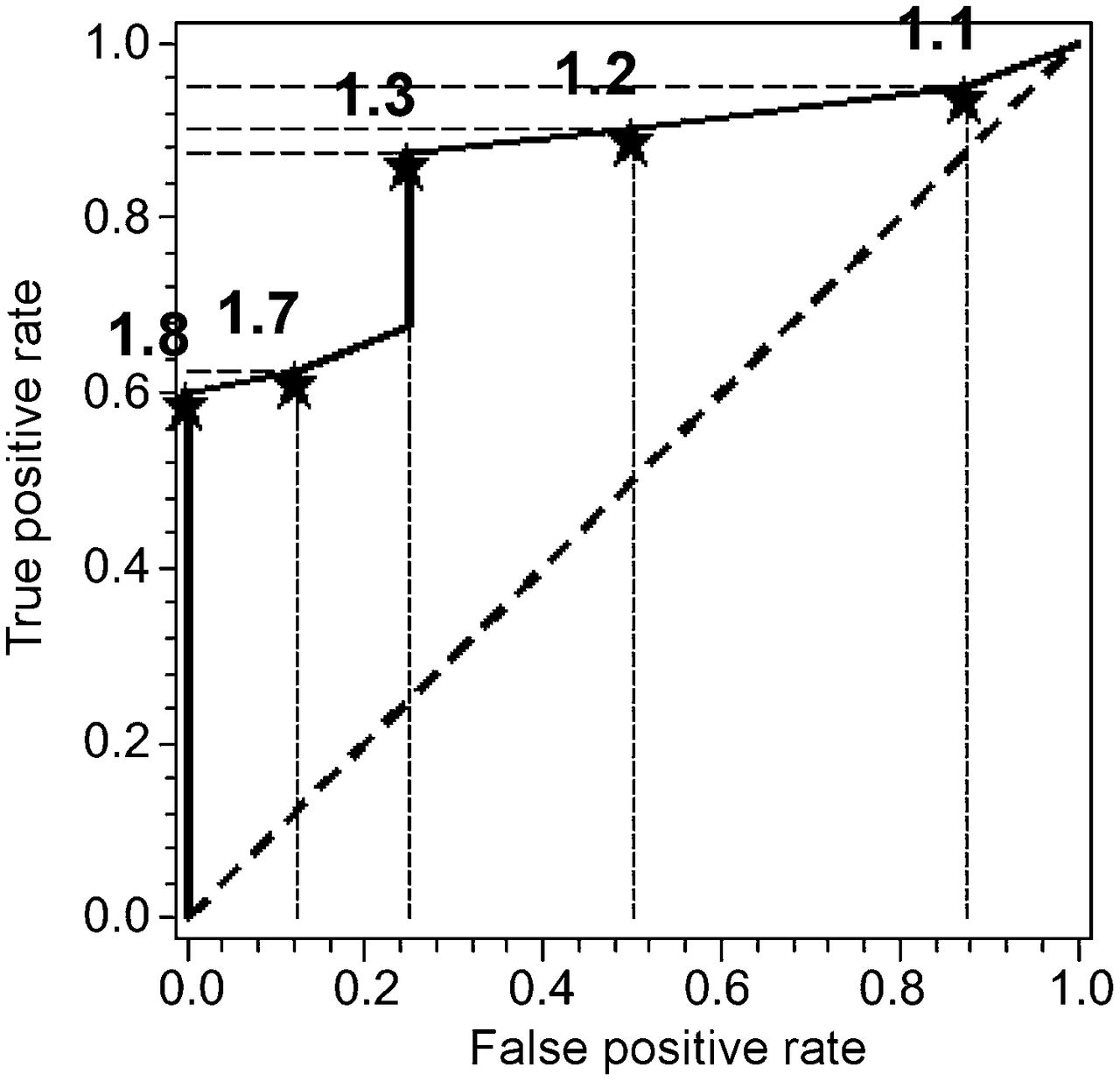
Receiver-operating-characteristic curve for ER expression vs. 18F-FES PET SUV (n = 48; stars with associated number identify 18F-FES PET SUV at that point on receiver-operating-characteristic curve).
On univariate analysis, we found a significant correlation between 18F-FES PET SUV and tumor size (P = 0.0015) but not HER2-neu overexpression (P = 0.58), estradiol (P = 0.60), PgR expression (P = 0.44), BMI (P = 0.15), lean BMI (P = 0.14), tumor type (P = 0.60), histologic grade (P = 0.29), or nuclear grade (P = 0.67). On multivariate regression analysis, tumor size (P < 0.0001) and immunohistochemistry ER expression (P < 0.001) were significant.
We had 6 patients who had immunohistochemistry tumor expression of at least 1% (median, 90%; range, 5%–95%) and an 18F-FES PET SUV of less than 1.5. Four of these 6 patients had stage I disease, and thus it is likely the breast lesions were too small to be visualized on 18F-FES PET. The median tumor size of these 6 patients was 1.2 cm (range, 0.9–2.0 cm).
Figure 3 shows an 18F-FES scan with intense uptake in the left breast lesion corresponding to an ER-positive breast cancer. Five patients in our study underwent additional 18F-FDG PET at the time of the 18F-FES PET. Figure 4 shows the 18F-FDG and 18F-FES scans of a patient with ER-negative cancer. Figure 5 shows an 18F-FES scan of a patient with locally advanced, ER-positive breast cancer with multiple sites of disease in the breast and regional lymph node metastases.

ER-positive left breast cancer. Axial 18F-FES image (A) shows intense uptake (arrow) in left breast lesion, corresponding to 2.3-cm lesion seen on CT (C) and confirmed by 18F-FES PET/CT image (B). Tumor was ER-positive, with SUV of 3.5.

ER-negative right breast cancer. Intense uptake (arrow) is seen in right breast lesion on 18F-FDG PET/CT scan (A), corresponding to lesion seen on CT (B); no uptake is seen on 18F-FES PET/CT scan (C).
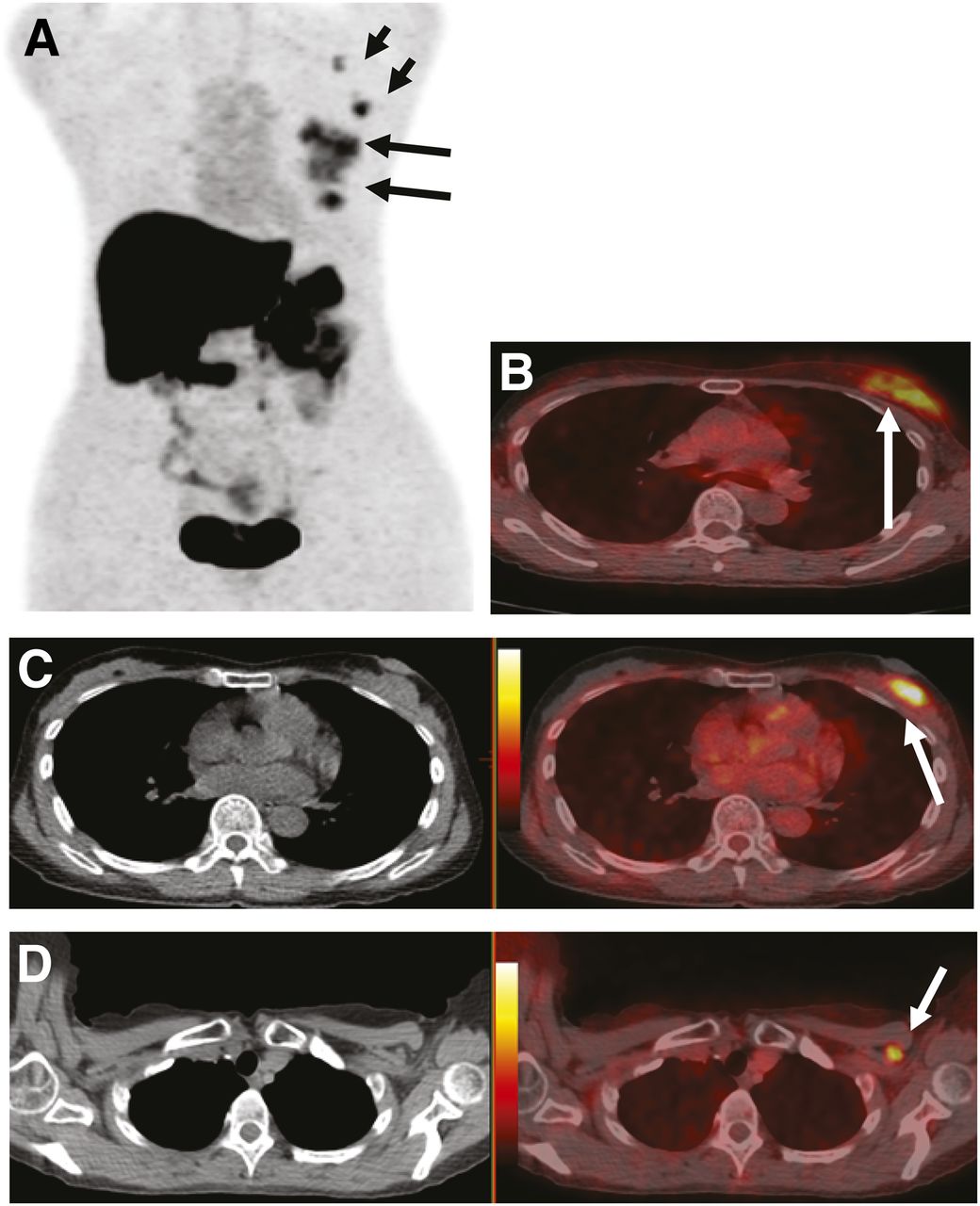
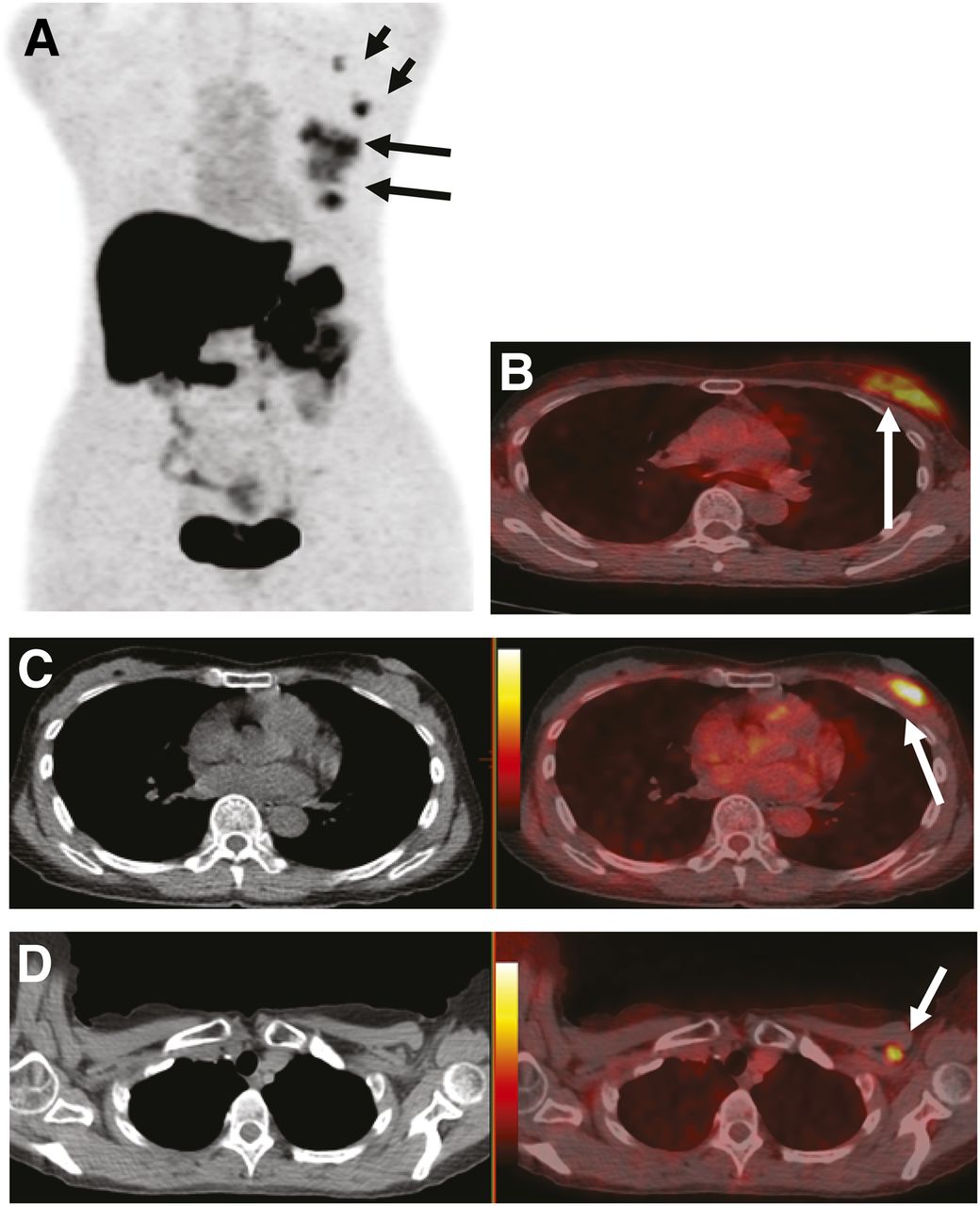
Locally advanced ER-positive breast cancer. (A) On maximum-intensity-projection 18F-FES image, intense uptake is seen in large left breast mass (long arrows). Smaller mass is also seen inferiorly (short arrows). (B) 18F-FES PET/CT image shows uptake with SUV of 5.7 in large breast mass (arrow). (C and D) Smaller inferior mass (arrow) is also seen on 18F-FES PET/CT (C), as is uptake in small subpectoral node and axillary node (D). Corresponding CT scans are shown on left.
DISCUSSION
Studies have previously validated 18F-FES PET uptake as a measure of ER expression in breast cancer (6,14). Mintun et al. demonstrated a high correlation between in vitro tumor ER concentrations measured using the radioligand method and 18F-FES uptake in the primary lesion (6,8). Peterson et al. compared ER expression measured by in vitro immunohistochemistry with 18F-FES uptake and noted a high correlation with 18F-FES uptake and ER expression in the primary lesion (14). Dehdashti et al. (9) found a correlation of 88% between in vitro ER assays and 18F-FES PET SUV.
Most of the studies to date include patients with locally advanced or metastatic breast cancer. Our study correlates ER expression in tumor tissue with 18F-FES uptake in patients with early-stage operable breast cancer. We found a correlation with immunohistochemistry ER expression but not with gene expression. There was a significant association with 18F-FES uptake and size of primary tumor, likely accounting for the lower sensitivity we saw in our study group as compared with prior published work (8,14).
Peterson et al. (11) examined potential factors that would influence 18F-FES PET uptake and found an association with BMI but not lean BMI. In that study, an association with sex hormone–binding globulin but not estradiol was noted. In our study, we explored the relationship between factors such as estradiol levels, BMI, and lean BMI and did not find an association. Like Mintun et al. (6), we also did not find an association with PgR expression. Additionally, we evaluated grade, histology, and HER2-neu overexpression and did not find any association.
18F-FES PET has also been shown to measure ER expression in multiple sites of disease. Studies have demonstrated 18F-FES uptake in axillary nodes and distant sites of disease (6,8).
Similarly, in our study population, we found that 18F-FES PET detected disease in distant sites (bone) and in axillary lymph nodes. In the axilla, small-volume disease was not identified with 18F-FES uptake. All 5 patients with uptake in the axilla had more than 4 nodes involved with disease, suggesting that a larger burden of disease was necessary for 18F-FES PET uptake to be demonstrated in the axilla.
The heterogeneity of the ER expression of multiple sites of disease was demonstrated in a study by Kumar et al. (15) that compared 18F-FDG PET and 18F-FES PET and showed multiple sites of 18F-FDG activity without corresponding 18F-FES uptake (15). Mortimer et al. (10) found that in a study of 21 patients with ER-positive breast cancer, 5 demonstrated no 18F-FES uptake, thus showing that 18F-FES PET can reveal the functional status of the ER that is not accessible through in vitro ER measurement. Similarly, Linden et al. (16) found that 6 of 47 patients with ER-expressing breast cancer had one or more sites of metastatic disease that did not have 18F-FES uptake.
Our study had 6 patients with strongly ER-expressing primary tumors that did not show significant 18F-FES uptake. Four of the 6 patients had stage I disease, and small tumor size likely contributed to this discordant finding. Overall, the correlation between ER expression and 18F-FES PET in our study was not as strong as previously reported in other studies, and we found no association with ER gene expression. Given the discrepancy in association between 18F-FES PET SUV and immunohistochemistry ER expression versus ER gene expression, it is possible that significant tumor heterogeneity for ER expression is present even in this group of patients with untreated, early breast cancers.
One of the most important potential applications of this technology appears to be in predicting response to endocrine therapy. Several studies have validated the use of 18F-FES PET in predicting response. Mortimer et al. (17) showed that the level of 18F-FES uptake predicted response to tamoxifen in locally advanced and metastatic breast cancer. Linden et al. (16) showed the ability of 18F-FES PET to predict response to endocrine therapy with aromatase inhibitors. Dehdashti et al. (9) showed that metabolic flare assessed through 18F-FES and 18F-FDG SUV can be predictive of response to endocrine therapy with aromatase inhibitor and fulvestrant. Linden et al. (7) recently reported on a study of serial 18F-FES PET in patients with metastatic breast cancer comparing aromatase inhibitor, tamoxifen, or fulvestrant and noted that tumor 18F-FES uptake decreased more with ER-blocking therapies than with estrogen-depleting therapies. All these studies support the use of 18F-FES PET in accurately predicting response to endocrine therapy.
Our study group predominantly comprised early-stage patients who received additional adjuvant therapies. Most received endocrine therapy (81%) or chemotherapy (85%) and had excellent disease-free survival. We did not find an association with 18F-FES PET SUV and outcome, but this analysis was limited, as few events occurred in our study population at this time. With further follow-up, it will be interesting to correlate the 18F-FES PET SUV and outcomes in our study group.
CONCLUSION
Our study supported the existing data on the role of 18F-FES PET in characterizing ER expression. In the perioperative setting, 18F-FES PET reliably identified additional sites of disease. However, our study highlighted the effects of tumor size and disease burden in imaging with 18F-FES PET and possible limitations on its role in the primary operative, early breast cancer setting.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Funding for this study was provided by U.S. Department of Defense grant BC030997 (principal investigator, Mary L. Gemignani). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Eva Burnazi, Shangde Cai, Howard Sheh, and Calvin Lom of the MSKCC Cyclotron-Radiochemistry Core (NIH Center grant P30-CA08748) for the production of 18F-FES.
Footnotes
Published online Aug. 22, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 31, 2012.
- Accepted for publication April 23, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Breast Cancer: Evaluating Tumor Estrogen Receptor Status with Molecular Imaging to Increase Response to Therapy and Improve Patient Outcomes
- 18F-FES PET/CT Influences the Staging and Management of Patients with Newly Diagnosed Estrogen Receptor-Positive Breast Cancer: A Retrospective Comparative Study with 18F-FDG PET/CT
- Improved Estrogen Receptor Assessment by PET Using the Novel Radiotracer 18F-4FMFES in Estrogen Receptor-Positive Breast Cancer Patients: An Ongoing Phase II Clinical Trial
- 18F-Fluoroestradiol PET/CT Measurement of Estrogen Receptor Suppression during a Phase I Trial of the Novel Estrogen Receptor-Targeted Therapeutic GDC-0810: Using an Imaging Biomarker to Guide Drug Dosage in Subsequent Trials
- Functional Estrogen Receptor Imaging Before Neoadjuvant Therapy for Primary Breast Cancer
- A Randomized Feasibility Study of 18F-Fluoroestradiol PET to Predict Pathologic Response to Neoadjuvant Therapy in Estrogen Receptor-Rich Postmenopausal Breast Cancer
- Estrogen Receptor Binding (18F-FES PET) and Glycolytic Activity (18F-FDG PET) Predict Progression-Free Survival on Endocrine Therapy in Patients with ER+ Breast Cancer
- 18F-Fluoroestradiol PET: Current Status and Potential Future Clinical Applications
- Translation of New Molecular Imaging Approaches to the Clinical Setting: Bridging the Gap to Implementation