


Abstract
The clinical performance of the Duke Endocarditis Service criteria to establish the diagnosis of infectious endocarditis (IE) can be improved through functional imaging procedures such as radiolabeled leukocytes (99mTc-hexamethylpropyleneamine oxime [HMPAO]–labeled white blood cells [WBC]). Methods: We assessed the value of 99mTc-HMPAO-WBC scintigraphy including SPECT/CT acquisitions in a series of 131 consecutive patients with suspected IE. Patients with permanent cardiac devices were excluded. 99mTc-HMPAO-WBC scintigraphy results were correlated with transthoracic or transesophageal echocardiography, blood cultures, and the Duke criteria. Results: Scintigraphy was true-positive in 46 of 51 and false-negative in 5 of 51 cases (90% sensitivity, 94% negative predictive value, and 100% specificity and positive predictive value). No false-positive results were found, even in patients with early IE evaluated within the first 2 mo from the surgical procedure. In 24 of 51 patients with IE, we also found extracardiac uptake, indicating septic embolism in 21 of 24. Despite the fact that septic embolism was found in 11 of 18 cases of Duke-definite IE, most of the added value from the 99mTc-HMPAO-WBC scan for decision making was seen in patients in whom the Duke criteria yielded possible IE. The scan was particularly valuable in patients with negative or difficult-to-interpret echocardiographic findings because it correctly classified 11 of 88 of these patients as having IE. Furthermore, 3 patients were falsely positive at echocardiography but correctly negative at 99mTc-HMPAO-WBC scintigraphy: these patients had marantic vegetations. Conclusion: Our results demonstrate the ability of 99mTc-HMPAO-WBC scintigraphy to reduce the rate of misdiagnosed cases of IE when combined with standard diagnostic tests in several situations: when clinical suspicion is high but echocardiographic findings are inconclusive; when there is a need for differential diagnosis between septic and sterile vegetations detected at echocardiography; when echocardiographic, laboratory, and clinical data are contradictory; and when valve involvement (especially of a prosthetic valve) needs to be excluded during febrile episodes, sepsis, or postsurgical infections.
The incidence of infectious endocarditis (IE) is approximately 2–4 cases per 100,000 persons per year (1). At present, 25%–50% of the cases occur in patients older than 60 y (2).
The diagnosis of IE, first suspected on clinical ground, is further supported by detection of a vegetation at either transthoracic or transesophageal echocardiography (TTE or TEE, respectively) or a finding of positive blood cultures (3). In most institutions, the final diagnosis is established using the Duke Endocarditis Service criteria (4), which also entail echocardiographic findings. Overall sensitivity is about 80% (5). However, in some instances, blood cultures or echocardiography is inconclusive, thus leading to a high proportion of unconfirmed cases of suspected IE. Indeed, up to 24% of the patients with pathologically proven endocarditis were misclassified as having possible IE based on the Duke criteria alone (5).
Attempts have been made at improving the diagnostic performance of these criteria, and modifications that consider several additional clinical and microbiologic parameters have been proposed (6). The so-called modified Duke criteria are now recommended for diagnostic classification (7). Traditional diagnostic criteria may also be integrated with information derived from radionuclide imaging, given the ability to localize the functional hallmark of infection: increased radiolabeled leukocyte recruitment. It is possible to detect and precisely localize throughout the body all sites of infection represented by areas of radiopharmaceutical uptake using 3-dimensional reconstruction of hybrid SPECT/CT or PET/CT images. In association with echocardiography, this imaging technique can be used to confirm or rule out IE in equivocal or difficult-to-explore situations (i.e., marantic vegetations, artifacts caused by a mechanical prosthesis). Furthermore, scintigraphy can also reveal the presence of extracardiac infection sites as the consequence of septic embolism originated from IE (8).
In this study, we assessed the added value of SPECT/CT with 99mTc-hexamethylpropyleneamine oxime (HMPAO)–labeled autologous white blood cells (WBC) in the characterization of patients with suspected or established IE, as defined according to the Duke criteria.
MATERIALS AND METHODS
Patient Population
Between October 2005 and December 2010, 185 consecutive patients were referred for scintigraphy with 99mTc-HMPAO-WBC for suspected IE. Fifty-four of these patients were excluded from the present analysis because they had permanent cardiac devices, a condition that might introduce confounding factors linked to the different mechanism of infection (9). Therefore, the population for the present work included the remaining 131 patients (45 women and 86 men; mean age ± SD, 62.8 ± 16.6 y) in whom IE was suspected or established as definite according to the Duke criteria; in the latter case, scintigraphy was performed to exclude septic embolism. All patients had undergone clinical examination and blood tests (including WBC counts, C-reactive protein level, erythrocyte sedimentation rate, and acute-phase protein level), electrophoresis, urinalysis, and echocardiography (either TTE, TEE, or both). Three sets of blood cultures including at least 1 aerobic and 1 anaerobic from a peripheral vein were obtained for all patients (10). The main clinical features and risk factors of the patients are summarized in Table 1.
Patient Characteristics (n = 131)
Final diagnosis of IE or exclusion of this condition and identification of an alternative cause of disease was defined on the basis of the final microbiologic (n = 20) or clinical diagnosis (n = 31), with clinical follow-up of 12 mo for all patients. On the basis of these combined parameters, IE was confirmed in 51 of the 131 patients, that is, in 24 of 28, 25 of 55, and 2 of 48 of the cases in which IE had been classified as definite, possible, or rejected, respectively, according to the Duke criteria.
For the 51 patients who were eventually diagnosed as having IE, infection involved more frequently the aortic valve and affected almost equally the native valves, either biologic or mechanical prosthetic implants (Table 2). For the 35 patients with prosthetic valves, early IE (<2 mo from valve replacement) was present in 9, semilate IE (between 2 and 12 mo) in 11, and late-onset IE in 15 (Table 2).
Type of Valve, Site of IE, Type of Infection, and Time of Infection Onset
Staphylococcus species were the microorganisms more frequently responsible for the infection (n = 24/51), followed by Enterococcus species (n = 11/51), Streptococcus species (n = 10/51), and Pseudomonas aeruginosa (n = 4/51). Haemophilus and Candida were found in 2 of 51 patients each.
Radiolabeling of Autologous Leukocytes and Image Acquisition Protocol
Autologous radiolabeled WBC were prepared according to guidelines for the labeling of leukocytes with 99mTc-HMPAO from the European Association of Nuclear Medicine (11,12). Radiolabeling efficiency was always between 70% and 85%, and viability of the radiolabeled leukocytes was always tested by the trypan blue exclusion test before reinfusion.
Whole-body and spot planar images were obtained after 30 min (early) and then at 4–6 and 20–24 h (delayed images) after reinfusion of 370–555 MBq of 99mTc-HMPAO-WBC. SPECT/CT of the chest was performed for all patients at 6 h and repeated at 24 h in the case of negative findings or doubtful imaging results at 6 h. Images were acquired using a dual-head, variable-angle SPECT/CT γ-camera (Hawkeye; GE Healthcare). The low-dose CT transmission scan was acquired for 16 s over 220° for each transaxial slice. The full field of view consisting of 40 slices was completed in 10 min. The transmission data were reconstructed using filtered backprojection to produce cross-sectional images. The resolution of the CT scan was 2.2 mm, and localization images were produced with a 4.5-mm pixel size, similar to the nuclear medicine emission images. The CT scans were reconstructed into a 256 × 256 matrix. The SPECT component of the same field of view was acquired using a 128 × 128 matrix, 360° rotation, 6° angle step, and acquisition time of 40- to 60-s per frame at 6 and 24 h. Both attenuation-corrected CT and noncorrected SPECT images were evaluated in the coronal, transaxial, and sagittal planes and in tridimensional maximum-intensity-projection cine mode. Matching pairs of radiographic transmission and radionuclide emission images were fused using the Xeleris workstation with Volumetrix software (GE Healthcare), and hybrid images of overlying transmission and emission data were generated.
Interpretation Criteria
Two experienced nuclear physicians aware of the patients’ clinical history and of the results of prior conventional imaging tests reviewed independently the planar scans and the SPECT/CT images with regard to the presence and location of any focus of abnormal radioactivity accumulation indicating infection. Preliminary analysis of the SPECT/CT images included visual inspection to exclude misregistration between the SPECT and the CT components.
The scintigraphic studies were classified as negative when no sites of abnormal uptake were observed on SPECT/CT images or positive for infection when at least 1 focus of abnormal uptake characterized by a time-dependent increase in radioactivity from early planar to delayed images was observed (13). This time-dependent pattern of uptake is especially relevant for the cardiac region, considering that physiologic accumulation of radiolabeled leukocytes in the bone marrow (as in the sternum, overlying the heart) early after reinfusion can interfere with interpretation of the planar images. When present, focal uptake indicating infection was further classified as pertaining to the heart or to extracardiac sites.
The contribution of SPECT/CT was considered, with special attention to the possibility of anatomically localizing the exact site of infection, particularly for the heart region. In fact, neither planar nor stand-alone SPECT allows cardiac foci of radiolabeled leukocyte uptake to be localized to the endocardium.
Data Analysis
The results of 99mTc-HMPAO-WBC scintigraphy were correlated with those of TTE, TEE, blood culture, and the Duke criteria. The ability to detect or exclude the presence of IE was defined using the final microbiologic or clinical diagnosis. Furthermore, in patients with known IE the ability to identify septic emboli and metastatic sites of infection was considered, in order to assess the potential of 99mTc-HMPAO-WBC scintigraphy to define disease burden.
The ability of stand-alone SPECT to localize infectious foci within the heart was not compared with that of SPECT/CT, because the low resolution of stand-alone SPECT cannot distinguish features as close to one another as the mitral and aortic valves (the most frequent sites of IE), which are less than 1 cm apart.
Statistical Analysis
All values are expressed as median and range, as customary for nonparametric data.
RESULTS
By adopting the interpretation criteria of this study for the scintigraphic detection of infection, it was possible to classify all the scans as either frankly positive or frankly negative, without any equivocal result at scintigraphy. With these criteria, 99mTc-HMPAO-WBC scintigraphy was negative in 34 of 131 patients for either cardiac or extracardiac sites of focal uptake indicating infection, without any discordant results between planar and SPECT/CT acquisitions. At least 1 area of focal radiolabeled leukocyte uptake was detected in 97 of 131 patients included in this study. In the 51 patients with a final diagnosis of IE, the uptake was limited to the heart only (n = 23; Figs. 1–3), to both the heart and the extracardiac sites (n = 23), or to extracardiac sites only (1 patient with septic embolism in the spleen, which was therefore considered a false-negative finding of IE).
99mTc-HMPAO-WBC scintigraphic images for patient with aortic endocarditis. Maximum-intensity-projection image (A) demonstrates focal increase of radiolabeled WBC in heart region. Transaxial SPECT/CT images (B) show that such focal uptake is localized at mechanical prosthesis of aortic valve (CT [left], fused SPECT/CT [center], and SPECT [right]).

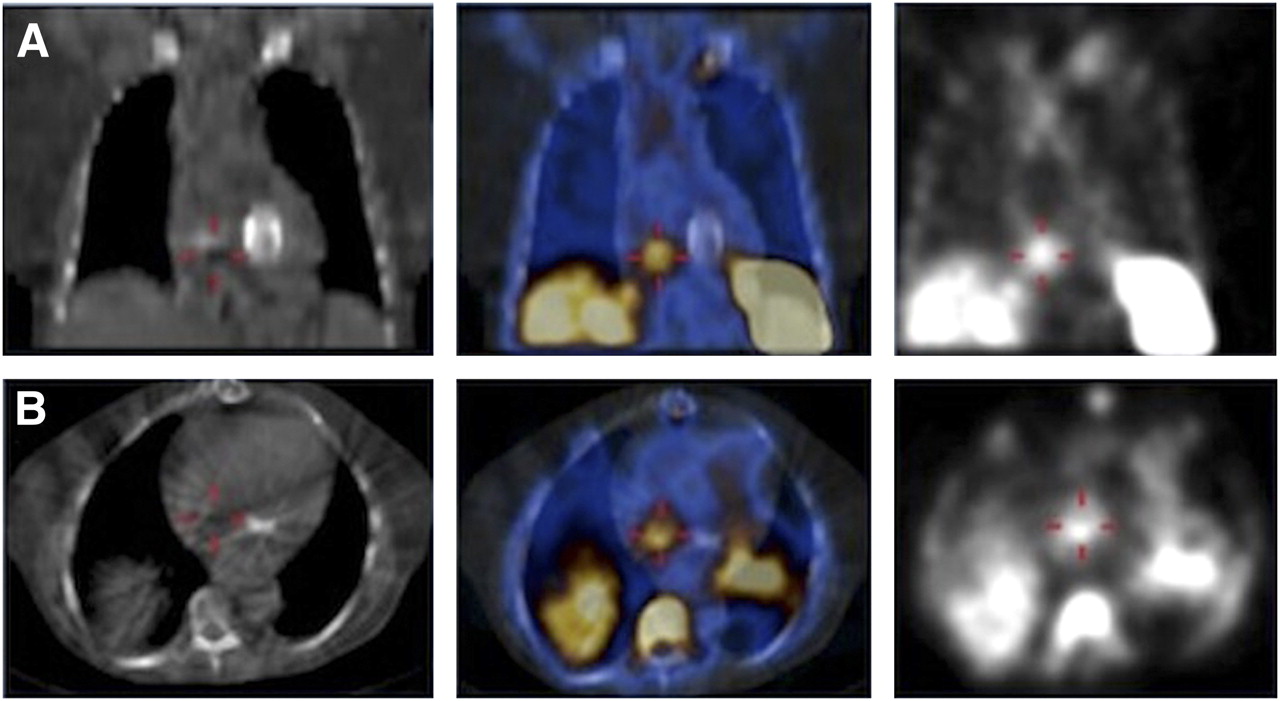
99mTc-HMPAO-WBC SPECT/CT images for patient with positive blood cultures and fever that arose a few months after substitution of mitral valve with mechanical prosthesis (coronal views [top], transaxial views [bottom]; CT [left], fused SPECT/CT [center], and SPECT [right]). SPECT images demonstrate clear focus of uptake in right heart, identified as endocarditis of native tricuspid valve by superimposed SPECT/CT images. Endocarditis of mechanical prosthesis, expected site of infection before 99mTc-HMPAO-WBC was performed, was therefore excluded.

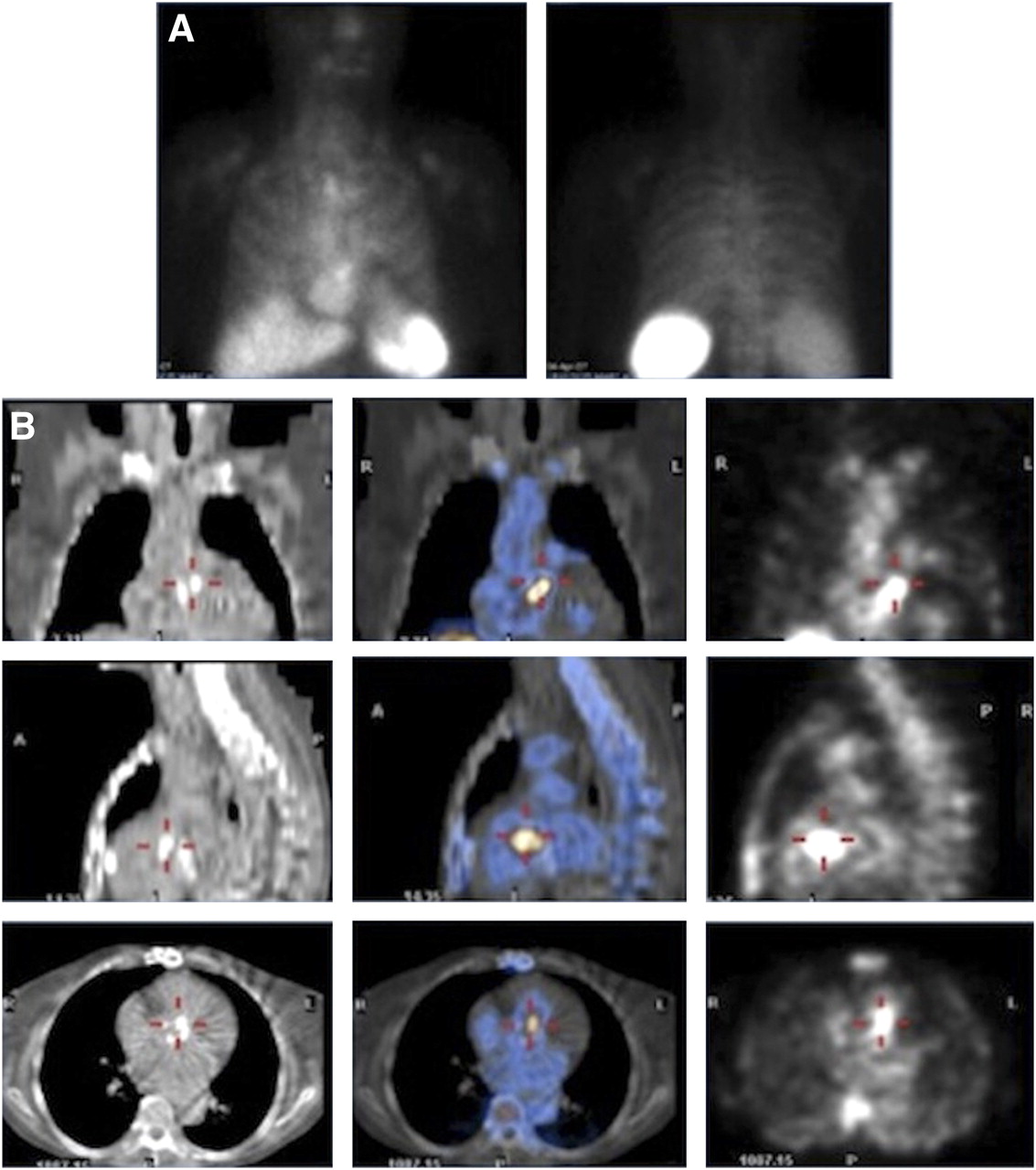
99mTc-HMPAO-WBC scintigraphy demonstrating value of SPECT/CT for precisely localizing site of infection. (A) Planar anterior (left) and posterior (right) views, where focal uptake of radiolabeled WBC mimics sternal osteomyelitis. (B) Coronal, sagittal, and transaxial CT (left); fused SPECT/CT (middle); and SPECT (right). Tomographic images correctly localize uptake of 99mTc-HMPAO-WBC at mitral valve prosthesis.
99mTc-HMPAO-WBC SPECT/CT was therefore true-positive in 46 of 51 and false-negative in 5 of 51 cases. The 5 false-negative findings for IE using 99mTc-HMPAO-WBC scintigraphy occurred in patients with small valve vegetations (<6 mm) and in the presence of infection from Enterococcus (n = 4) or Candida (n = 1); all such patients were receiving high-dose antimicrobial therapy at the time of scintigraphy. There were no false-positive scans for infection of the cardiac valves.
Although both planar and stand-alone SPECT images were sufficiently accurate to detect the presence of infection involving the heart in most patients (there were in fact only 4 false-negative planar scans, in which the accumulation of radiolabeled leukocytes was hidden by the sternum or ribs), only after coregistration with CT was it possible to precisely discriminate the localization of 99mTc-HMPAO-WBC uptake (i.e., especially mitral vs. aortic valves, given their proximity; metal devices; or surgical stitches or clips) from any noncardiac site of infection in the mediastinal space. Of the total of 89 sites of increased 99mTc-HMPAO-WBC uptake in the chest, fused SPECT/CT images demonstrated heart valve localization in 44 cases, compared with noncardiac-valve localizations due to infection of the aortic graft (n = 11), sternum osteomyelitis (n = 13), mediastinitis (n = 3), and lung infection (n = 17). For areas with focal 99mTc-HMPAO-WBC uptake outside the thorax, the major impact of the SPECT/CT findings was observed for imaging sites of central nervous system infection and head-and-neck lesions and for discriminating between bone infection and soft-tissue infection. In particular, the exact sites of 99mTc-HMPAO-WBC accumulation were diagnosed as the central nervous system; the nasal and maxillary sinuses (infections; in 3 and 5 cases, respectively); the spleen (embolism; n = 4); and bone, soft tissues, or joints (prosthetic joint infections) (22 cases overall, involving the spine in 10 cases).
Septic embolism was detected in 41% of patients (Fig. 4). Three cases interpreted as septic embolism at 99mTc-HMPAO-WBC scintigraphy were instead false-positive because of active vasculitis of the aortic arch, an isolated vertebral metastasis from prostate cancer, and an osteoporotic vertebral crush. There were 8 scans false-negative for extracardiac infection due to kidney (n = 3) or cerebral septic embolism (n = 5) (all detected by CT or MRI).

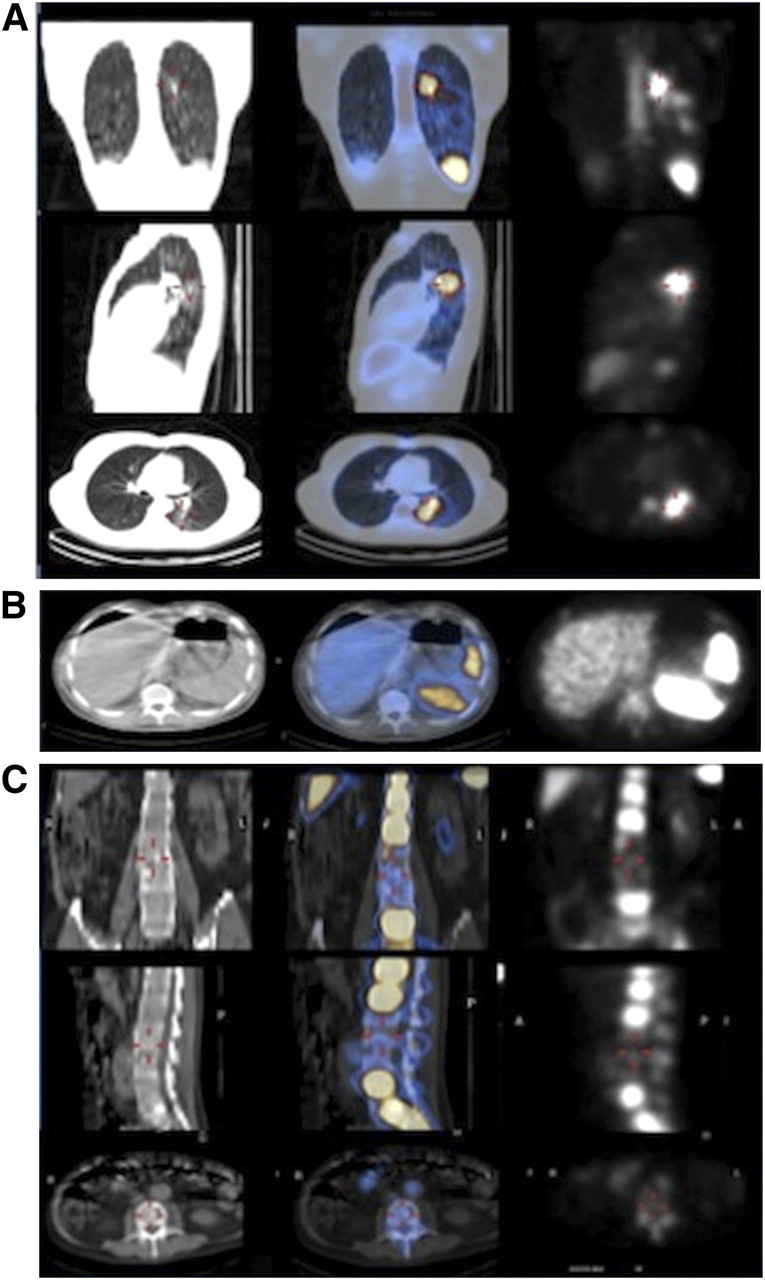
Examples of septic embolism at different sites as detected by 99mTc-HMPAO-WBC SPECT/CT. (A) Patient with septic embolism in left lung (coronal, sagittal, and transaxial CT [left]; fused SPECT/CT [middle]; and SPECT [right]). (B) Patient with septic embolism in spleen, where infection shows as photopenic area in splenic parenchyma (transaxial CT [left], fused SPECT/CT [center], and SPECT [right]). (C) Patient with septic embolism in spine (coronal, sagittal, and transaxial CT [left]; fused SPECT/CT [middle]; and SPECT [right]). Similarly, as in case of spleen, infection shows as photopenic area, which in this patient involves 2 vertebral bodies.
Table 3 correlates the SPECT/CT results and the Duke classification in the 51 patients with a final diagnosis of IE. Most of the added value from the 99mTc-HMPAO-WBC scan for decision making was seen in patients for whom the Duke criteria yielded possible IE.
Results of 99mTc-HMPAO-WBC Scintigraphy in the 51 Patients with Final Diagnosis of IE, Stratified According to Duke Criteria
Table 4 shows the correlation between echocardiographic and 99mTc-HMPAO-WBC scintigraphic findings. The scan was particularly valuable in patients with negative or difficult-to-interpret echocardiographic findings due to several circumstances, such as mechanical valve implants or the presence of huge calcifications (in a diabetic patient undergoing dialysis). Furthermore, 3 patients were falsely positive using echocardiography but correctly negative with 99mTc-HMPAO-WBC scintigraphy: these patients had marantic vegetations.
Results of 99mTc-HMPAO-WBC Scintigraphy in the 51 Patients with Final Diagnosis of IE, Stratified According to Echocardiography
Table 5 correlates the results of 99mTc-HMPAO-WBC scintigraphy and blood cultures. The most striking result was a positive scan observed in patients with a negative blood culture; such a high false-negative fraction of blood culture results could be linked to high-dose antibiotic therapy.
Results of 99mTc-HMPAO-WBC Scintigraphy in the 51 Patients with Final Diagnosis of IE, Stratified According to Blood Culture
Table 6 shows the results of all the diagnostic procedures in patients without IE. Of the 50 of 80 patients without IE who exhibited a positive 99mTc-HMPAO-WBC scintigraphy finding (only at extracardiac sites), 48 were correctly classified on scanning as having either osteomyelitis (n = 22), peripheral vascular graft infection (n = 12), lung infection (n = 7), mediastinitis (n = 5), or cholecystitis (n = 2). In the other 2 patients, focal uptake of the radiolabeled leukocytes in the spine was falsely positive for infection because of a vertebral crush caused by osteoporosis in one case and by metastasis from a melanoma with an unknown primary site in the other case.
Results of All Diagnostic Procedures in the 80 Patients Without IE
DISCUSSION
The diagnosis of IE is becoming progressively more challenging because of a variety of factors. These include the indiscriminate use of antimicrobial agents in some clinical settings, the increased proportion of individuals with predisposing or underlying conditions (i.e., frail and elderly, immunosuppressed persons), and the increasing number of interventional cardiovascular procedures and placement of valve prostheses, intravascular devices, or cardiac devices. Mortality from IE remains high when this condition is undiagnosed and, therefore, not adequately treated (14). Early diagnosis and prompt institution of appropriate antibiotic therapy reduce septic embolism and mortality (15); therefore, the identification of patients at highest risk of death may offer the opportunity to change the course of the disease and improve prognosis.
Because of the ability to detect endocardial vegetations (16), abscesses (17), and intracardiac complications (i.e., valve perforation and chordal rupture) (18), echocardiography is the indirect method of choice for investigating patients for whom IE is clinically suspected (19,20). Furthermore, some echocardiographic features such as vegetation size (higher risk for lesions > 10 mm in diameter and for vegetations that are growing), number (multiple), and features (mobile but pedunculated, noncalcified, prolapsing) (20) may also be used to predict the potential embolic burden of IE. However, the presence of prosthetic valves consistently decreases the sensitivity and specificity of echocardiography, to about 20% for TTE and around 90% (in the hands of an experienced operator) for TEE (8). In approximately 15% of the patients, echocardiography can be false-positive (because thickened valves, nodules, or valvular calcifications are misinterpreted as vegetations) (4), whereas a similar proportion can be false-negative (4). Thus, echocardiographic findings alone cannot always definitely confirm or exclude the clinical suspicion of IE. Because echocardiography represents the backbone of the Duke criteria, this suboptimal diagnostic accuracy translates into a relatively high proportion of cases classified as possible IE; however, about 24% of such cases are eventually diagnosed as definite IE (5).
Additional potentially misleading factors in the Duke classification include some well-known pitfalls in blood cultures (antimicrobial treatment, subacute right-sided and mural endocarditis (21), fungi, slow-growing and difficult-to-identify organisms) (22) and ambiguous symptoms without any of the classic stigmata of valvular infection.
A functional imaging modality such as radionuclide imaging, capable of characterizing specific features of the endocardial vegetations, may contribute to solving clinical dilemmas in such conditions. In our experience, when the results of 99mTc-HMPAO-WBC scintigraphy were associated with either positive echocardiography or a positive blood culture, no cases of IE went undiagnosed. In particular, the radiolabeled leukocyte scan facilitated the diagnosis of IE in challenging situations for echocardiography, as in the presence of a mechanical prosthetic valve, anuloplasty rings, calcifications, or nonbacterial thrombotic vegetations. Furthermore, 99mTc-HMPAO-WBC scintigraphy allowed the exclusion of valve infection in patients with concomitant risk factors, nondiagnostic echocardiographic findings, and positive blood cultures (37% of the cases in our series) or the identification of other focal infections different from IE (as occurred in 38% of the overall 131 patients). 99mTc-HMPAO-WBC scintigraphy can therefore be considered as the second-line test of choice in patients with prosthetic valves or devices, fever, positive blood cultures, and equivocal TTE/TEE findings.
This study confirms that 99mTc-HMPAO-WBC scintigraphy is a crucial imaging modality also for localizing sites of infection in patients with symptoms, signs, and laboratory findings of sepsis (increased erythrocyte sedimentation rate, C-reactive protein level, and WBC count) (12) and either a positive or a negative blood culture. In these patients, generally neither TEE nor TTE is used for screening purposes (4), and therefore, the heart region should always be carefully evaluated when one is analyzing the 99mTc-HMPAO-WBC scan.
The possibility of acquiring whole-body images and additional planar and SPECT/CT spot images constitutes an invaluable aid for detecting septic embolism and metastatic sites of infection, as observed in our patient population. In particular, septic embolism was detected even in the absence of the typical echocardiographic predictors of systemic embolism (8,20).
These results refer only to patients with IE arising on native and prosthetic valves, because we intentionally excluded patients with device-related infection. In fact, we consider application of the same diagnostic algorithm to this different clinical entity impossible.
Specific methodology-related issues must be properly addressed to ensure adequate scintigraphic acquisitions. Images should be acquired in time-mode, compensating for isotope decay at each time point. In the case of equivocal findings for 6-h SPECT/CT of the thorax, acquisition of images should be repeated at 24 h. Images should be analyzed using the same scale frame to easily identify any focal area of activity that increases over time or shows a change in shape from early to late images. Both attenuation-corrected and noncorrected CT images should be always inspected side by side, to minimize metal-related artifacts. The quantitative analysis of target-to-background ratios was not necessary in these patients. SPECT/CT is mandatory to correctly interpret and localize the site and extent of radiolabeled leukocyte uptake indicating infection (23) and to discriminate involvement of the heart valve or prosthesis from uptake around the prosthesis. Furthermore, in cases with positive scintigraphy findings in the cardiac region, SPECT/CT can discriminate endocardial infections from all other possible causes of postsurgical fever (i.e., mediastinitis, osteomyelitis of the sternum or ribs, wound infections).
There were no false-positive findings, even in patients with early IE evaluated within the first 2 mo from the surgical procedure, suggesting that adequate acquisition protocol and interpretation criteria can optimize the specificity of the scan even in this clinical setting. On the other hand, the false-negative findings observed in the presence of IE sustained by Candida or Enterococcus species may be explained by the ability of these microorganisms (and others such as Staphylococcus epidermidis) to form a biofilm resulting in resistance to antimicrobial treatment and escape from the host defense mechanisms (24). Additionally, altered neutrophil recruitment at the primary site of IE by Enterococcus faecalis extracellular proteases constitutes a further mechanism of innate immune response impairment (25). Such mechanisms might reduce the sensitivity of scintigraphy with radiolabeled leukocytes in patients with IE. However, in our experience the reduced sensitivity of 99mTc-HMPAO-WBC scintigraphy was counterbalanced by the association with echocardiography.
Both false-negative and false-positive findings were also observed regarding distant septic embolism. In particular, the typical 99mTc-HMPAO-WBC scintigraphic pattern of spleen embolism and spondylodiskitis represented by a cold spot (26) may also be present in other benign or malignant conditions. Thus, despite being highly suggestive for septic embolism, such a finding in patients with IE should be confirmed with additional diagnostic imaging such as MRI. Finally, it is reasonable to assume that the availability of new-generation SPECT/CT scanners with a more advanced CT component will further increase diagnostic accuracy, particularly when the central nervous system and bone are evaluated. Alternatively, PET/CT may be proposed to improve spatial resolution. In this regard, preliminary data have demonstrated significant uptake of 18F-FDG both in infected endocardial vegetations and at metastatic sites of infection (27–30). However, 18F-FDG uptake is observed in a variety of benign and malignant conditions such as inflammation or tumors (31), thus reducing its specificity. Moreover, special caution should be used in the interpretation of 18F-FDG uptake in the cardiac region, because of the high number of possible causes other than IE for a positive finding: recent thrombi (32), soft atherosclerotic plaques (33), vasculitis (34), primary and metastatic cardiac tumors (35,36), or simply a postsurgical inflammatory reaction (37). In clinical routine, focal areas of 18F-FDG uptake at the heart in the absence of IE are quite commonly observed (Paola A. Erba, unpublished data, 2011; Fig. 5). The possibility of efficient radiolabeling of autologous leukocytes with positron-emitting radionuclides can be expected to change the whole scenario of PET for patients with suspected IE. In this regard, intense 18F-FDG-WBC uptake at the valve site has been described for the only patient with IE as yet reported (38). Unfortunately, the physical half-life of 18F is too short to encompass the whole kinetics of leukocyte migration into sites of infection, thus creating a major limitation for the use of this method in this clinical setting.

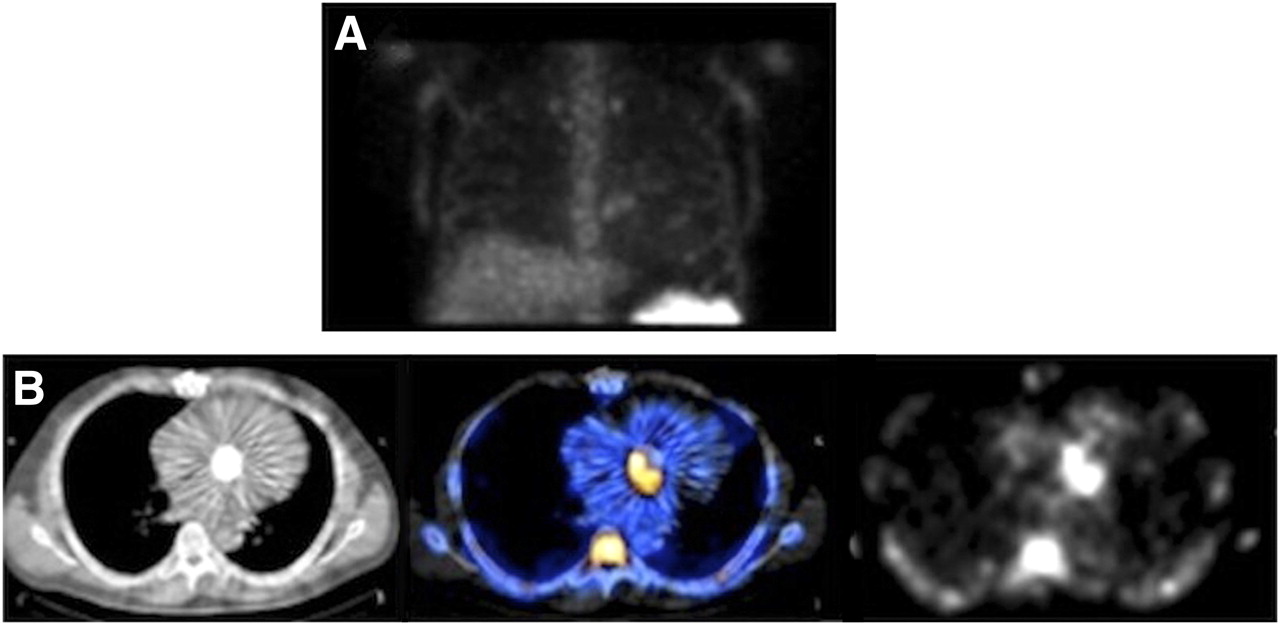
False-positive 18F-FDG PET/CT result in patient with fever. Area of increased 18F-FDG uptake suspected of being endocarditis at mitral valve mechanical prosthesis (A; fused transaxial PET/CT [left] and PET alone [right]) turned out to be negative with 99mTc-HMPAO-WBC SPECT/CT (B; fused transaxial SPECT/CT [left] and SPECT [right]). Clinical follow-up confirmed absence of infection. (C) CT transaxial image.
CONCLUSION
Our experience supports the use of scintigraphy with 99mTc-HMPAO-WBC in patients with high clinical suspicion of IE, to confirm the diagnosis in doubtful circumstances or to detect sites of septic embolism. The rate of misdiagnosed IE can be reduced with 99mTc-HMPAO-WBC in patients with a high clinical suspicion but inconclusive echocardiographic findings; for the differential diagnosis between septic and sterile vegetations detected at echocardiography; when echocardiographic, laboratory, and clinical data are contradictory; and to exclude valve involvement (especially of a prosthetic valve) during febrile episodes, sepsis, or postsurgical infections.
SPECT/CT is necessary to demonstrate and localize 99mTc-HMPAO-WBC at native or prosthetic valves, thus confirming the diagnosis of IE. Furthermore, whole-body images followed by additional planar and SPECT/CT spot images allow the detection of distant sites of septic embolism and thus constitute an invaluable aid. Negative results in the presence of a typical echocardiographic pattern for IE should be carefully evaluated, because false-negative findings due to limited spatial resolution or non–leukocyte-recruiting microorganisms can be encountered.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 11, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 2, 2012.
- Accepted for publication March 21, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Infection Imaging: Focus on New Tracers?
- Radiolabeled-White Blood Cell Imaging in Cardiac Device-Related Infective Endocarditis: Worth All the Effort?
- The Prognostic Value of 99mTc-HMPAO-Labeled Leucocyte SPECT/CT in Cardiac Device-Related Infective Endocarditis
- Infective endocarditis complicating transcatheter aortic valve implantation
- Methicillin-Resistant Staphylococcus aureus Prosthetic Valve Endocarditis: Pathophysiology, Epidemiology, Clinical Presentation, Diagnosis, and Management
- Approach to Diagnosis of Cardiovascular Implantable-Electronic-Device Infection
- Targeting Cardiovascular Implant Infection: Multimodality and Molecular Imaging
- Clinical Trial Principles and Endpoint Definitions for Paravalvular Leaks in Surgical Prosthesis: An Expert Statement
- 18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography in Cardiac Implantable Electronic Devices Infection: Ready for Routine Care!
- 18F-Fluorodeoxyglucose Imaging of Inflammation: Ready to Represent a Standard in Diagnosing Endocarditis?
- Challenges in Infective Endocarditis
- Diagnostic Accuracy of 18F-FDG PET/CT in Infective Endocarditis and Implantable Cardiac Electronic Device Infection: A Cross-Sectional Study
- Improving the Diagnosis of Infective Endocarditis in Prosthetic Valves and Intracardiac Devices With 18F-Fluordeoxyglucose Positron Emission Tomography/Computed Tomography Angiography: Initial Results at an Infective Endocarditis Referral Center
- Respective Performance of 18F-FDG PET and Radiolabeled Leukocyte Scintigraphy for the Diagnosis of Prosthetic Valve Endocarditis
- Radiolabeled WBC Scintigraphy in the Diagnostic Workup of Patients With Suspected Device-Related Infections
- Positron Emission Tomography/Computed Tomography for Diagnosis of Prosthetic Valve Endocarditis: Increased Valvular 18F-Fluorodeoxyglucose Uptake as a Novel Major Criterion
- The Use of 18F-FDG-PET/CT in the Diagnostic Workup of CIED Infections: Another Perspective