


Abstract
Our goal in this study was to elucidate the mechanisms by which methotrexate radiosensitizes HER2-positive human breast cancer cells to the Auger electron emitter 111In-trastuzumab modified with nuclear-localization sequence peptides (111In-NLS-trastuzumab) and to compare these mechanisms with the potential sensitizing effects of paclitaxel and doxorubicin when combined with this radiopharmaceutical. Methods: Experiments were performed in MDA-MB-231 human breast cancer cells, their HER2-transfected subclones (231-H2N), and 2 trastuzumab-resistant variants (trastuzumab-resistant-1 and -2 [TrR1 and TrR2]). Effects of coexposure of these cells to 111In-NLS-trastuzumab and low-dose, radiosensitizing methotrexate, paclitaxel, or doxorubicin were assessed by clonogenic cell-survival assay. Quantification of residual DNA damage was measured by the γH2AX-immunofluorescence assay, and cell cycle distribution was measured by fluorescence-activated cell sorting analysis. The radiation-enhancement ratio was calculated as the ratio of the surviving fraction (SF) of cells treated with 111In-NLS-trastuzumab alone to that of cells treated concurrently with 111In-NLS-trastuzumab and methotrexate, paclitaxel, or doxorubicin. Results: A reduction in the SF in HER2-positive 231-H2N (55.7% ± 1.3%) and TrR1 (62.6% ± 6.5%) cells was demonstrated after exposure to 111In-NLS-trastuzumab (∼0.2 MBq/μg, 100 nmol/L) but not in MDA-MB-231 or TrR2 cells expressing low levels of HER2 (SF > 90%, P > 0.05). Coadministration of methotrexate, paclitaxel, or doxorubicin enhanced the cytotoxicity of 111In-NLS-trastuzumab toward 231-H2N and TrR1 cells but not toward MDA-MB-231 or TrR2 cells. The radiation-enhancement ratios for methotrexate, paclitaxel, and doxorubicin for 231-H2N or TrR1 cells were 2.0–2.2, 1.6–1.8, and 2.7–2.8, respectively. Methotrexate or doxorubicin combined with 111In-NLS-trastuzumab, compared to treatment with 111In-NLS-trastuzumab alone, significantly increased residual γH2AX foci in 231-H2N and TrR1 cells but not in MDA-MB-231 or TrR2 cells or in any cell line treated concurrently with paclitaxel and 111In-NLS-trastuzumab. Cells exposed to low-dose methotrexate accumulated in the G1/S phase of the cell cycle, whereas low-dose paclitaxel or doxorubicin caused cells to arrest in the G2/M phase. Conclusion: Low-dose methotrexate, paclitaxel, or doxorubicin potently sensitized HER2-overexpressing human breast cancer cells, with and without acquired trastuzumab-resistance, to the Auger electron emissions from 111In-NLS-trastuzumab through cell cycle distribution changes and in part through the inhibitory effects of these agents on DNA damage repair.
Despite the success of radioimmunotherapy for advanced lymphohematopoietic malignancies, the treatment of patients with solid tumors such as breast cancer has been limited because of the small amounts of antibody that can be targeted to tumors. Also of concern in treatment are the irradiation and killing of normal cells (e.g., bone marrow stem cells) by the moderate-energy and long-range (2–10 mm) β-particles emitted by 131I and 90Y, which have been commonly conjugated to radiotherapeutic agents (1,2). Therefore, considerable attention has been given to the combination of radioimmunotherapy with drugs that are known radiosensitizers and that can amplify the lethal effects of ionizing radiation on cancer cells while having minimal or no toxicity on tissues at the low concentrations used (3).
This strategy may be especially relevant for patients whose tumors display amplification of the HER2 receptor tyrosine kinase. HER2 overexpression occurs in 25%−30% of breast cancers (4), has been correlated with resistance to hormonal therapy (5–7) and chemotherapy (8), and is directly associated with poor long-term survival (4). Trastuzumab (Herceptin; Hoffmann-La Roche) is a humanized anti-HER2 monoclonal antibody approved for immunotherapy of HER2-amplified breast cancer (4). However, only 50% of patients with tumors exhibiting moderate to high (2+ to 3+) immunohistochemistry scores or having greater than 3 copies of the HER2 gene by fluorescence in situ hybridization are predicted to respond to trastuzumab when given in combination with chemotherapy (9,10). Moreover, the short duration of response to trastuzumab (9–12 mo) and the rapid development of drug resistance limit the effectiveness of trastuzumab treatment in this patient population (11,12). In an attempt to enhance its antineoplastic activity, our group has been studying Auger electron radioimmunotherapy of HER2-amplified breast cancer using 111In-trastuzumab modified with 13 mer peptides (CGYGPKKKRKVGG) harboring the nuclear-localization sequence (NLS) of SV-40 large T antigen, which promotes its nuclear importation after HER2-mediated internalization into breast cancer cells (13). Auger electrons are highly damaging to DNA when they decay near the cell nucleus, making them exquisitely selective and highly potent for killing targeted single cancer cells (14). Indeed, we recently reported that 111In-NLS-trastuzumab, compared with nonradiolabeled trastuzumab (Herceptin), could slow the growth of HER2-positive breast cancer xenografts in mice, with minimal harm to normal tissues, and prolong survival (15). In in vitro studies, we further found that 111In-NLS-trastuzumab was able to kill breast cancer cells that are resistant to trastuzumab and that the potency of the radiopharmaceutical could be enhanced by coexposing these cells to low, noncytotoxic concentrations of methotrexate (16).
Understanding the mechanisms resulting in tumor cell radiosensitization caused by the interaction of chemotherapeutic drugs and Auger electron radiotherapeutics would be useful in the development of rational clinical protocols that combine these agents. The first objective of this study, therefore, was to elucidate the mechanisms that underlie methotrexate radiosensitization of HER2-positive breast cancer cells to 111In-NLS-trastuzumab. Methotrexate is an antifolate drug that inhibits purine de novo synthesis. This antifolate activity of methotrexate is hypothesized to impede DNA synthesis and repair and amplify the lethal effects of the Auger electron emissions from 111In-NLS-trastuzumab (17,18). Therefore, we examined the effects of low-dose methotrexate on cell cycle progression using fluorescence-activated cell sorting and measured DNA damage by the γH2AX fluorescence assay in breast cancer cells exposed to the combination of methotrexate and 111In-NLS-trastuzumab. Other chemotherapeutic agents, such as paclitaxel and doxorubicin, are commonly administered to breast cancer patients in combination with trastuzumab and are also known radiosensitizers (4). Therefore, we also sought to determine whether paclitaxel and doxorubicin would radiosensitize HER2-postive breast cancer cells to 111In-NLS-trastuzumab. The radiosensitizing effects of these agents, when combined with 111In-NLS-trastuzumab, were evaluated and compared with those caused by methotrexate.
MATERIALS AND METHODS
Cell Culture
MDA-MB-231 human breast cancer cells were obtained from the American Type Culture Collection, and the 231-H2N and trastuzumab-resistant 1 and 2 (TrR1 and TrR2) cell lines were kindly provided by Dr. Robert S. Kerbel (Sunnybrook Health Sciences Centre). The 231-H2N cell line was derived from MDA-MB-231 cells that were transfected to stably overexpress c-erbB-2 (HER2), whereas TrR1 and TrR2 cells were isolated from 231-H2N tumors in athymic mice with acquired trastuzumab resistance (19). 231-H2N and TrR1 cells express high levels of HER2 (5.0–6.0 × 105 receptors per cell), which is approximately 10-fold greater than MDA-MB-231 and TrR2 cells, which express 0.4–0.6 × 105 HER2 receptors per cell (16). All cell lines were cultured in Dulbecco's minimal essential medium (Ontario Cancer Institute) supplemented with 10% fetal bovine serum (Sigma-Aldrich) containing 100 U of penicillin per milliliter and 100 μg of streptomycin per milliliter at 37°C in an atmosphere of 5% CO2.
Trastuzumab and Radiosensitizers
Trastuzumab was reconstituted according to the package insert. Methotrexate and doxorubicin were prepared by dissolving 1 mg of the drug (Sigma-Aldrich) in 1 mL of alkalinized (pH 11.0) or neutral (pH 7.0) distilled, deionized water, respectively. The methotrexate stock solution was adjusted to pH 7.0 before use. Paclitaxel (Sigma-Aldrich) was prepared by dissolving 1 mg of the drug in 100 mL of dimethyl sulfoxide. Stock solutions were diluted in culture medium to the desired final concentration. The final concentration of dimethyl sulfoxide in the culture medium was 0.1% (v/v) or less.
111In-Trastuzumab Modified with NLS-Peptides
Trastuzumab (Herceptin) was modified with synthetic 13 mer NLS-peptides (CGYGPKKKRKVGG) and labeled with 111InCl3 (MDS-Nordion) using diethylenetriaminepentaacetic acid (DTPA) (Sigma-Aldrich) to a specific activity of 201 ± 6 MBq/mg (13). Briefly, trastuzumab (500 μg, 10 mg/mL) was reacted with a 10-fold molar excess of DTPA dianhydride for 1 h at room temperature before reaction with a 15-fold molar excess of sulfo-succinimidyl-4-(N-maleimidomethyl)cyclohexane-1-carboxylate (SMCC) (2–5 mmol/L). Maleimide-derivatized DTPA-trastuzumab was concentrated to 2–5 mg/mL and reacted overnight at 4°C with a 60-fold molar excess of NLS-peptides (5–10 mmol/L diluted in phosphate-buffered saline [PBS], pH 7.0). DTPA-trastuzumab modified with NLS-peptides (NLS-DTPA-trastuzumab) was purified on a Sephadex-G50 minicolumn (GE Healthcare) eluted with PBS, pH 7.5. Under these conditions, 3–4 NLS-peptides were conjugated to trastuzumab at an SMCC:IgG:NLS-peptide molar ratio of 15:1:60 (13).
NLS-conjugated trastuzumab or unmodified DTPA-trastuzumab was radiolabeled by incubation of 37–111 MBq of monoclonal antibodies with 111InCl3 (MDS-Nordion) for 60 min at room temperature. 111In-labeled monoclonal antibodies were purified on a Sephadex-G50 minicolumn and buffer-exchanged to PBS, pH 7.5, using a Microcon YM-50 ultrafiltration device (Amicon; Millipore). The radiochemical purity was routinely greater than 97% as determined by instant thin-layer chromatography–silica gel (Pall Corp.) developed in 100 mM sodium citrate, pH 5.0. All radioactivity measurements were made using an automatic γ-counter (Wallac Wizard-1480; Perkin Elmer).
Clonogenic Assays
Approximately 2 × 106 breast cancer cells were incubated with 111In-NLS-trastuzumab (100 nmol/L) alone or concurrently with an inhibitory concentration of 10% (IC10) of methotrexate, paclitaxel, or doxorubicin in 1 mL of culture medium in microtubes for 24 h at 37°C. The 24-h time point was chosen because nuclear accumulation of 111In-NLS-trastuzumab increases for up to 24 h in HER2-overexpressing breast cancer cells (13). Controls consisted of cells treated with PBS (pH 7.5) or cells treated with escalating doses of methotrexate, paclitaxel, or doxorubicin (the concentrations of the tested chemotherapeutic drugs ranged from 0.01 to 100 μmol/L). For treatments including methotrexate, cells were serum-starved by lowering the serum concentration from 10% to 1% to reduce the concentrations of thymidine, 5-methyl tetrahydrofolate, and purine ribonucleosides that counteract the effects of methotrexate (20). After treatment, the cells were centrifuged at 1,000g for 5 min and washed twice with normal culture medium containing 10% serum. Sufficient cells were then plated in triplicate in 12-well plates and cultured in normal medium at 37°C. After 10–14 d, the dishes were stained with methylene blue, and colonies of 50 cells or more were counted. The surviving fraction (SF) was calculated by dividing the number of colonies formed for treated cells by the number for untreated cells. Survival curves were derived for cells treated with methotrexate, paclitaxel, or doxorubicin by plotting the SF values versus the log molar concentration of agent used. The inhibitory concentrations of 50% (IC50) and IC10 were estimated with Origin 6.0 (Microcal Software Inc.) using the dose-response equation y = A1 + [(A2 − A1)/(1 + 10(log EC50 − x) × p], where p is the slope (set to −1), and A1 and A2 are the amplitudes of the baseline and maximum response, respectively. The radiation-enhancement ratio (RER) was determined by dividing the SF of cells treated with 111In-NLS-trastuzumab alone by that of cells treated concurrently with 111In-NLS-trastuzumab and methotrexate, paclitaxel, or doxorubicin. An RER greater than 1 indicated radiosensitization (16,21).
Cell Cycle Analysis
Cells were plated into 100-mm tissue culture plates (Sarstedt Inc.) at a density of 1 × 106 cells per plate and cultured overnight. Control cells and cells treated with methotrexate, paclitaxel, or doxorubicin were incubated in 10 mL of medium in 100-mm cell culture dishes for 24 h at 37°C. Treated and control cells were then suspended in 300 μL of PBS and fixed with 700 μL of 100% ice-cold ethanol for 1 h. The cells were then washed, resuspended with 10 mg of RNase (Invitrogen) per milliliter, and stained with propidium iodide (25 mg/mL; Sigma-Aldrich) in 100 μL of PBS, pH 7.5, for 1 h at 37°C. The DNA content was analyzed with a flow cytometer (BD FACSCalibur), and the distribution of cells in the different phases of the cell cycle was determined.
Measurement of DNA Damage
The ability of 111In-NLS-trastuzumab alone or combined with methotrexate, paclitaxel, or doxorubicin to cause DNA double-strand breaks (DSBs) in breast cancer cells was evaluated using the γH2AX-assay, which detects phosphorylation of histone-H2AX at serine-139 (γH2AX) at sites of DSBs as discrete nuclear foci using γH2AX-specific antibodies (22). Control cells were treated with methotrexate, paclitaxel, doxorubicin, or unlabeled trastuzumab alone or the combination of unlabeled trastuzumab and methotrexate, paclitaxel, or doxorubicin. Cells were cultured overnight in 1 mL of medium containing 111In-NLS-trastuzumab (100 nmol/L) alone or combined with methotrexate, paclitaxel, or doxorubicin. Exactly 24 h after the incubation period, cells were fixed with 2% paraformaldehyde containing 0.5% Triton X-100 in PBS, pH 8.2, for 15 min. After three 10-min washes with PBS, pH 7.5, containing 0.5% bovine serum albumin and 0.2% polysorbate-20, the cells were permeabilized for 15 min with PBS, pH 8.2, containing 0.5% Nonidet P-40 (Sigma-Aldrich) and blocked for 1 h in 2% bovine serum albumin and 1% donkey serum. The slides were then incubated with antiphospho-γH2AX (1:800; Upstate Biotechnology) in 3% bovine serum albumin overnight at 4°C and then with AlexaFluor-488 antimouse IgG (Molecular Probes) for 45 min at room temperature. All slides were mounted with Vectashield medium containing 4,6-diamidino-2-phenylindole (DAPI) (Vector Laboratories) and kept at 4°C overnight. Images were taken with an inverted LSM510 confocal microscope (Carl Zeiss) at the Advanced Optical Microscopy Facility (Princess Margaret Hospital). Excitation was at 364 nm or 488 nm for visualization of DAPI or AlexaFluor-488, using 385- to 470-nm and 505- to 550-nm emission filters, respectively. For imaging of γH2AX, 10–15 z-stack images at approximately 1-μm intervals were acquired throughout the entire cell nucleus, merged using LSM-Viewer software (version, 3.5.0.376; Zeiss), and stored as .tiff files. The number of γH2AX-foci present in each cell was counted manually using ImageJ software (version, 1.36b; National Institutes of Health) as described previously (23).
Statistical Methods
Data are presented as mean ± SEM. Statistical comparisons were made using the Student t test. P < 0.05 was considered significant.
RESULTS
Effect of Methotrexate, Paclitaxel, and Doxorubicin on Survival of Breast Cancer Cells
MDA-MB-231, 231-H2N, TrR1, and TrR2 human breast cancer cells were incubated with increasing concentrations of methotrexate, paclitaxel, and doxorubicin for 24 h to determine a low, relatively noncytotoxic concentration of drug that resulted in survival of 90% or more cells (i.e., IC10) by clonogenic assay. There was a strong dose-dependent decrease in colony formation of the different breast cancer cells treated with increasing amounts of chemotherapeutic agent. Table 1 shows the IC50 and IC10 values of each agent for each cell line; IC10 values ranged between 0.01 and 12 mmol/L, 0.02 and 0.14 mmol/L, and 0.02 and 0.19 mmol/L for methotrexate, paclitaxel, and doxorubicin, respectively. These IC10 doses were chosen to evaluate the radiosensitizing effect of combined treatment of low-dose chemotherapy with 111In-NLS-trastuzumab.
IC10 and IC50 Values for Methotrexate, Paclitaxel, and Doxorubicin on MDA-MB-231, 231-H2N, TrR1, and TrR2 Human Breast Cancer Cells
Effect of 111In-NLS-Trastuzumab Combined with Low-Dose Methotrexate, Paclitaxel, or Doxorubicin on Clonogenic Survival
The SF of the 4 cell lines treated for 24 h with 111In-NLS-trastuzumab (100 nmol/L) alone or combined with the IC10 concentrations for methotrexate, paclitaxel, and doxorubicin was measured in clonogenic assays. Compared with no 111In-NLS-trastuzumab exposure, exposure to 111In-NLS-trastuzumab significantly decreased the SF for 231-H2N and TrR1 cells (55.6% ± 1.3% and 74.1% ± 5.4%, respectively) that express intermediate to high levels of HER2 but not for MDA-MB-231 or TrR2 cells (97.9% ± 7.2% and 89.5% ± 3.8%, respectively) that express low levels of HER2 (16) (Fig. 1). The effect of a 24-h treatment with 111In-NLS-trastuzumab combined with low-dose methotrexate, paclitaxel, or doxorubicin (i.e., the IC10 dose of drug) on the SF of cells was then measured. The combined treatment, compared with 111In-NLS-trastuzumab alone, caused an even greater reduction in the SF of 231-H2N and TrR1 cells, with doxorubicin causing the greatest decrease in the SF in both cell lines (Fig. 1). In contrast, the combined treatment, compared with treatment with 111In-NLS-trastuzumab alone, had little effect on the SF of MDA-MB-231 and TrR2 cells. The RERs for low-dose chemotherapy combined with 111In-NLS-trastuzumab are shown in Table 2. The greatest RERs were observed for 231-H2N and TrR1 cells when 111In-NLS-trastuzumab was combined with doxorubicin (RER, 2.7–2.8), followed by cotreatment with methotrexate (RER, 2.0–2.2) and paclitaxel (RER, 1.6–1.8).
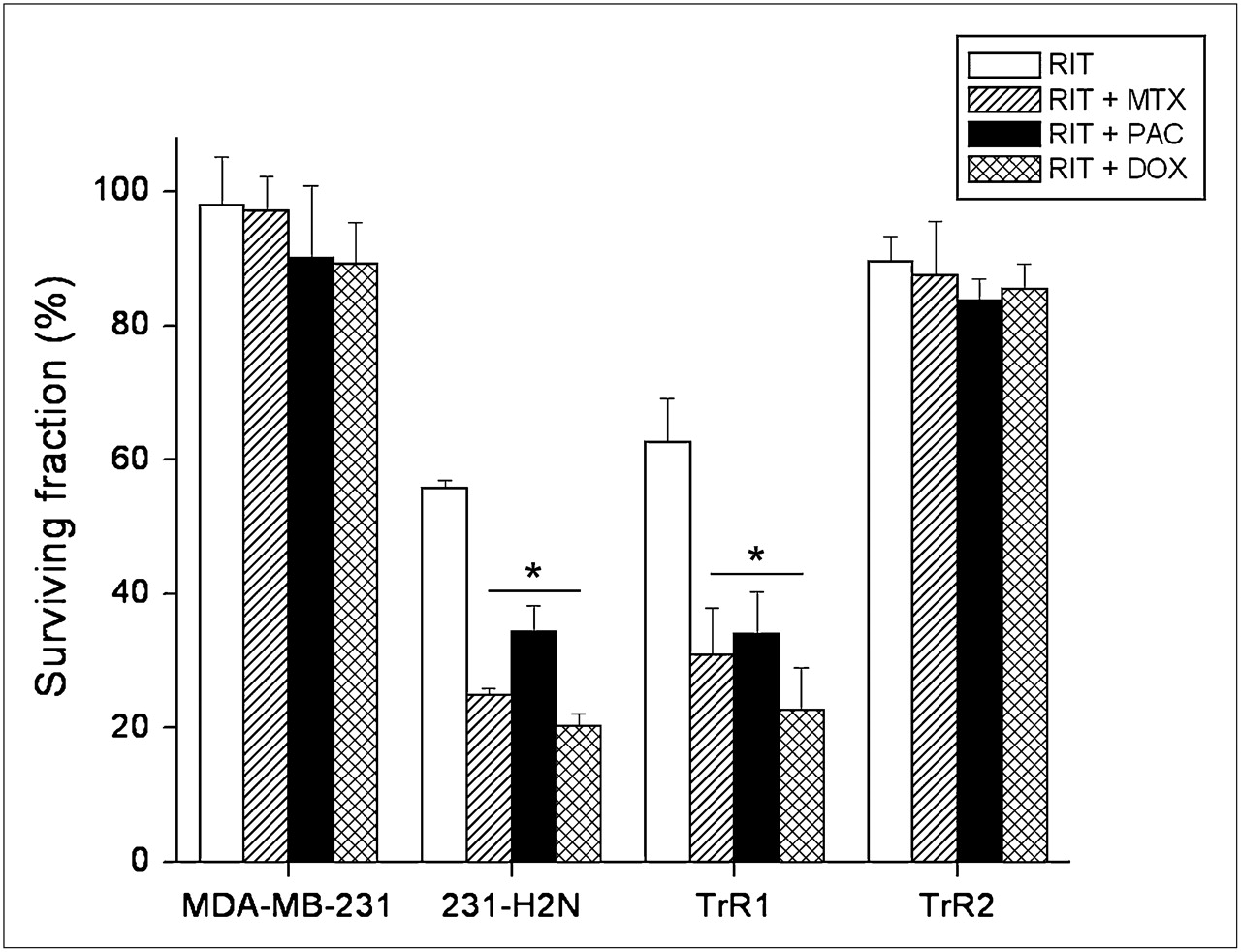
SFs of MDA-MB-231, 231-H2N, TrR1, and TrR2 human breast cancer cells after treatment with 111In-NLS-trastuzumab alone (radioimmunotherapy [RIT]) (∼0.2 MBq/μg, 100 nmol/L) or 111In-NLS-trastuzumab combined with IC10 concentrations of methotrexate (MTX) (RIT + MTX ), paclitaxel (PAC) (RIT + PAC), or doxorubicin (DOX) (RIT + DOX). IC10 values of each drug for each cell line are shown in Table 1. *P < 0.05, compared with RIT.
Radiation Enhancement Ratio (RER) for Methotrexate, Paclitaxel, and Doxorubicin on Human Breast Cancer Cells When Combined with 111In-NLS-Trastuzumab
DNA Damage Induced by 111In-NLS-Trastuzumab Combined with Methotrexate, Paclitaxel, or Doxorubicin
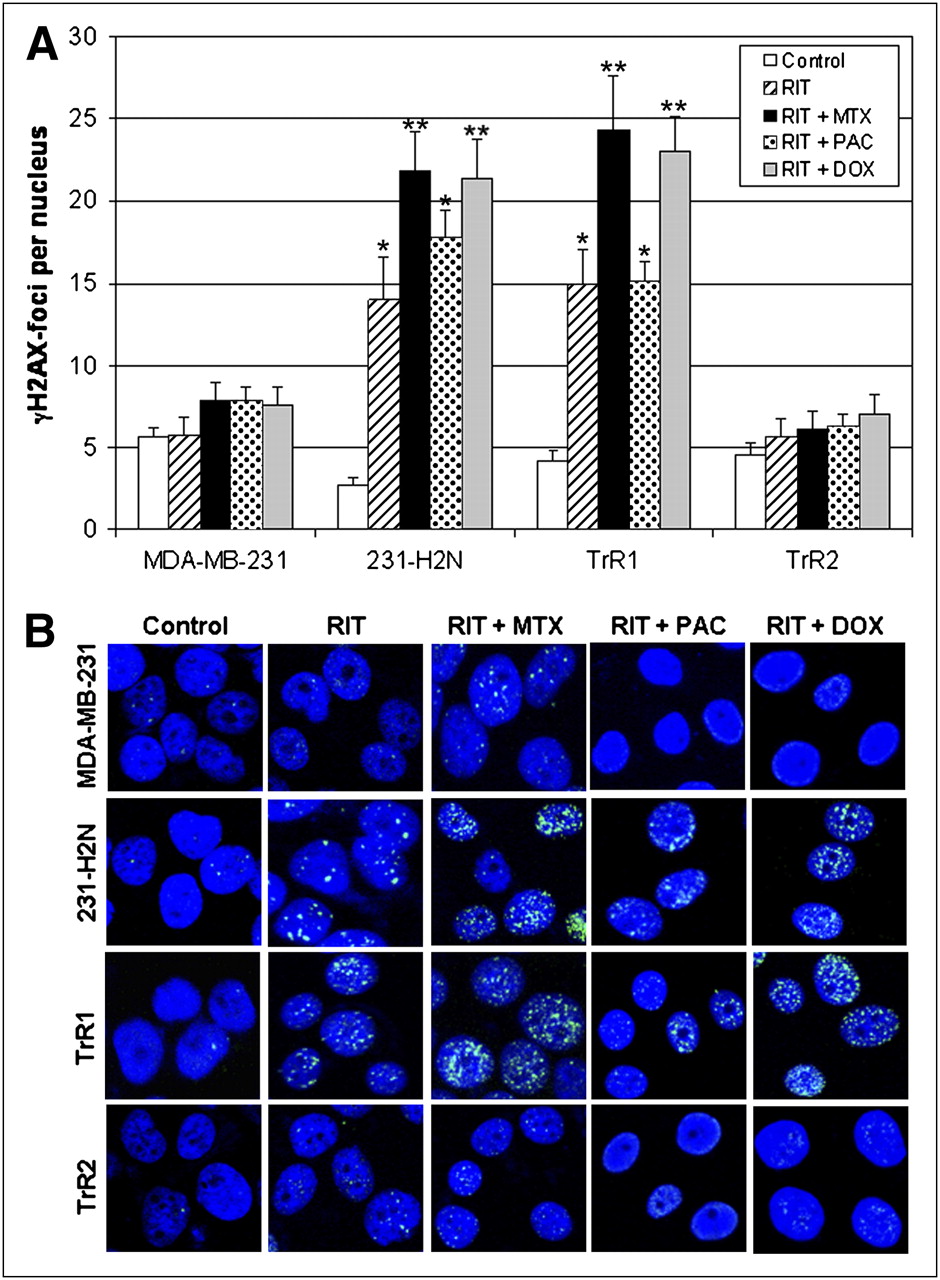
A 4- to 5-fold increase in the number of residual γH2AX-foci 24 h after incubation with 111In-NLS-trastuzumab (100 nmol/L), compared with after no incubation, was observed in 231-H2N (14.0 ± 2.6 foci/nucleus vs. 2.7 ± 0.5 foci/nucleus, P < 0.05) and TrR1 cells (15.0 ± 2.1 foci/nucleus vs. 4.1 ± 0.7 foci/nucleus, P < 0.05) (Fig. 2). In contrast, treatment with 111In-NLS-trastuzumab did not significantly increase the formation of residual γH2AX-foci in MDA-MB-231 or TrR2 cells (5.7 ± 1.1 foci/nucleus and 5.6 ± 1.1 foci/nucleus, respectively), compared with 231-H2N or TrR1 cells, likely because of the 10-fold lower expression of HER2. 231-H2N and TrR1 cells exposed to a low dose of methotrexate or doxorubicin in combination with 111In-NLS-trastuzumab, compared with cells exposed to either agent alone, showed a higher number of γH2AX-foci (231-H2N: 21.8 ± 2.4 foci/nucleus and 21.4 ± 2.4 foci/nucleus, respectively; TrR1: 24.3 ± 3.3 and 23.0 ± 2.2, respectively) (P < 0.05). However, the combination of low-dose paclitaxel and 111In-NLS-trastuzumab, compared with treatment with 111In-NLS-trastuzumab alone, did not significantly increase the number of residual γH2AX-foci in these cells (231-H2N: 17.8 ± 1.6 foci/nucleus; TrR1: 15.1 ± 1.1 foci/nucleus, P > 0.05). There was a modest increase in the formation of γH2AX-foci in MDA-MB-231 and TrR2 cells exposed to 111In-NLS-trastuzumab and chemotherapy, compared with cells exposed to only 1 of these agents, but this increase did not reach the level of statistical significance. Compared with control untreated cells, cells treated with an equivalent dose of methotrexate, paclitaxel, doxorubicin, or unlabeled trastuzumab alone, or the combination of unlabeled trastuzumab and methotrexate, paclitaxel, or doxorubicin, did not show significantly higher γH2AX foci/nucleus (data not shown).

(A) Residual γH2AX-foci in MDA-MB-231, 231-H2N, TrR1, and TrR2 human breast cancer cells 24 h after exposure to 111In-NLS-trastuzumab alone (radioimmunotherapy [RIT]) (100 nmol/L) or 111In-NLS-trastuzumab combined with IC10 concentrations of methotrexate (MTX) (RIT + MTX), paclitaxel (PAC) (RIT + PAC), or doxorubicin (DOX) (RIT + DOX). Number of γH2AX-foci per nucleus is shown as mean ± SEM, and at least 30 nuclei were assessed for γH2AX-foci for each treatment. (B) Induction of γH2AX-foci (green) 24 h after exposure to 111In-NLS-trastuzumab alone or concurrently with MTX, PAC, or DOX. Nuclear DNA was stained with DAPI (blue). *P < 0.05, compared with control, or **P < 0.05, compared with 111In-NLS-trastuzumab.
Cell Cycle Arrest by Methotrexate, Paclitaxel, and Doxorubicin
As shown in Supplemental Figure 1 (supplemental materials are available online only at http://jnm.snmjournals.org), low-dose methotrexate, paclitaxel, and doxorubicin caused a major redistribution of cells in the cell cycle. All cell lines, except for TrR2 cells, were arrested in the G1/S phase when incubated for 24 h with low-dose methotrexate. This arrest was accompanied by a significant decrease in the percentage of cells in the G2/M phase. In contrast, 24-h incubation with low-dose paclitaxel and doxorubicin caused all 4 cell lines to arrest in the G2/M phase of the cell cycle, accompanied by a significant decrease of cells in the G1/S phase.
DISCUSSION
Considerable attention has been given to combining radioimmunotherapy with chemotherapeutic agents that are known radiosensitizers or have other potential additive or synergistic properties (24). The chemotherapeutic agent is usually given at a reduced dose or modified schedule, primarily to enhance the radiosensitivity of cancer cells and improve the efficacy of radioimmunotherapy without increased cytotoxicity. Previously, we examined this approach using low, noncytotoxic concentrations of methotrexate to radiosensitize HER2-postive breast cancer cells to the high-linear-energy–transfer Auger electron radiation emitted by 111In-NLS-trastuzumab (16). The IC50 for 111In-NLS-trastuzumab against 231-H2N and TrR1 human breast cancer cells treated concurrently with low-dose methotrexate was 5-fold lower than that for cells treated with radiopharmaceutical alone (28 nmol/L and 14 nmol/L vs. 140 nmol/L and 70 nmol/L, respectively). These findings suggested that radiosensitizing chemotherapy combined with targeted Auger electron radiotherapy can enhance cytotoxicity, but the mechanism underlying this radiosensitization remained unknown. Therefore, we sought in the current study to determine the causes mediating methotrexate radiosensitization and to explore the potential sensitizing effects of paclitaxel and doxorubicin because these agents are commonly administered in combination with trastuzumab (i.e., Herceptin) to patients with HER2-positive breast cancer (4). The results presented here confirm the ability of methotrexate to selectively radiosensitize HER2-overexpressing breast cancer cells (i.e., 231-H2N and TrR1) to 111In-NLS-trastuzumab and further demonstrate that the cytotoxicity of this radiopharmaceutical can be enhanced by the coexposure of these cells to low, noncytotoxic concentrations of paclitaxel or doxorubicin. The radiosensitizing effects were shown to be mediated through cell cycle distribution changes and in part through the inhibitory effects of these agents on DNA repair, as evidenced by the increase in γH2AX foci in the cells.
The main intracellular target of methotrexate is dihydrofolate reductase, an enzyme that participates in reduced folate metabolism (18). Methotrexate is thought to radiosensitize cells through its effect on the depletion of reduced folates required for the production of purine deoxyribonucleotides and thymidylate necessary for DNA synthesis and repair (18,25). Indeed, the low, noncytotoxic concentration of methotrexate that was determined in clonogenic assays to radiosensitize 231-H2N and TrR1 breast cancer cells to 111In-NLS-trastuzumab was found to cause these cells to accumulate in the G1/S phase of the cell cycle, possibly through the depletion of intracellular purine nucleotide pools (Supplemental Fig. 1). Although we did not attempt to assess the distinction between cells in the G1 and early S phases of the cell cycle, a more accurate estimate may be obtained by measuring the DNA content of bromodeoxyuridine-labeled S-phase cells using dual-parameter flow cytometry (26). Nevertheless, the extent of DNA damage (γH2AX-foci) in these cells at 24 h after exposure to 111In-NLS-trastuzumab was enhanced by coexposure to methotrexate (Fig. 2), suggesting that nucleotide depletion by methotrexate can indirectly affect the repair of DNA damage in cells exposed to Auger electron radiation. Alternatively, chemotherapeutic radiosensitizers may produce their effect mainly by direct action on DNA (17). Doxorubicin, for example, forms complexes with DNA by intercalation between base pairs, interfering with DNA polymerase and topoisomerase II activity, and inhibits enzyme repair of radiation-induced DNA DSBs (27). Indeed, the addition of low-concentration doxorubicin to 111In-NLS-trastuzumab, compared with cells treated with either of these agents alone, induced more DNA damage and increased the killing of 231-H2N and TrR1 cells. This result is in agreement with the observations by Supiot et al. (21), who demonstrated synergy between doxorubicin and α-particle radioimmunotherapy on induction of DNA damage and cell death in RPMI8226 myeloma cells. The powerful arrest of 231-H2N and TrR1 cells in the radiosensitive G2/M phase of the cell cycle induced by doxorubicin (Supplemental Fig. 1) may also account for the observed increase in DNA damage and reduction in the SF of these cells after coexposure with 111In-NLS-trastuzumab.
Paclitaxel also caused 231-H2N and TrR1 cells to arrest in the radiosensitive G2/M phase of the cell cycle (Supplemental Fig. 1) (28). However, the level of paclitaxel radiosensitization, combined with 111In-NLS-trastuzumab, was moderately lower than with combinations of the radiopharmaceutical with methotrexate or doxorubicin. For example, the RER for the addition of paclitaxel to 111In-NLS-trastuzumab for 231-H2N and TrR1 cells was 1.6−1.8, versus 2.0–2.2 and 2.7–2.8 for combinations with methotrexate and doxorubicin, respectively (Table 2). The lower level of radiosensitization caused by paclitaxel also correlated with fewer residual γH2AX-foci in 231-H2N and TrR1 cells after cotreatment with 111In-NLS-trastuzumab (Fig. 2). This correlation is consistent with the fact that paclitaxel does not promote DNA damage but instead binds to and promotes the polymerization of tubulin, which interferes with normal microtubule breakdown (29). Moreover, paclitaxel has been shown to trigger apoptosis, possibly by inducing the phosphorylation and inactivation of the antiapoptotic factors Bcl-2 and Bcl-xL (30). It is possible that paclitaxel-mediated radiosensitization of HER2-positive breast cancer cells results from mechanisms unrelated to DNA DSB induction. Other DNA-incorporated, Auger electron–emitting radiopharmaceuticals, such as 5-[125I]iodo-2′-deoxyuridine, have been shown to promote apoptosis through a caspase-3–mediated process (31). Thus, chemotherapeutic agents that amplify the apoptotic response in HER2-positive breast cancer cells exposed to Auger electron radiation may also be effective in causing radiosensitization.
Future studies examining low-dose chemotherapy radiosensitization and 111In-NLS-trastuzumab in vivo will need to assess the dose-limiting toxicities on normal tissues associated with this combined treatment. Indeed, one limitation of this regimen is that the radiosensitization effect might not be exclusive to tumor cells, particularly when the radiopharmaceutical is administered at high doses. However, minimal toxicity toward MDA-MB-231 and TrR2 cells expressing low levels of HER2 was observed from this combination, suggesting that radiosensitization may be specific for cells overexpressing HER2 (i.e., HER2-amplified breast cancer cells). Moreover, the feasibility of combining radiosensitizing chemotherapy with radioimmunotherapy has been demonstrated previously in preclinical and clinical studies (32). For example, DeNardo et al. (33) examined the effect of combining paclitaxel with radioimmunotherapy using 90Y-chimeric anti-L6 antibody (90Y-ChL6) in mice bearing HBT-3477 human breast cancer xenografts. Paclitaxel administered 6 or 24 h after radioimmunotherapy did not substantially increase normal-tissue toxicity but resulted in cures or complete responses in all (46/46) treated mice, whereas only 21% (6/29) of animals were cured when paclitaxel was given before 90Y-ChL6 (33). Thus, the optimal combination and scheduling of low-dose chemotherapy and 111In-NLS-trastuzumab needs to be determined because the radiosensitizing effect may be highly dependent on the timing of administration of the chemotherapeutic drug relative to radioimmunotherapy. One approach may be to administer the radiotherapeutic agent, wait for 72 h for optimal tumor uptake and elimination from normal tissues (13), and then administer these low-molecular-weight radiosensitizers, which are expected to equilibrate rapidly between the plasma and the tissues (including tumor), thereby providing concurrently high concentrations of radioactivity and radiosensitizers.
The trastuzumab-resistant TrR1 cells (19) were efficiently killed by 111In-NLS-trastuzumab, and the toxicity was enhanced by coexposure to radiosensitizing concentrations of methotrexate, paclitaxel, or doxorubicin (Fig. 1). Combination therapy with low-dose chemotherapy and 111In-NLS-trastuzumab may, therefore, offer a route to overcoming the challenges associated with trastuzumab resistance. Indeed, only about half of patients with HER2-overexpressing metastases respond to trastuzumab when combined with paclitaxel or doxorubicin, and in almost all initially responding patients, resistance to trastuzumab develops within a year (11,12). There have been few studies that have examined the combination of radiotherapeutics that emit high-linear-energy transfer radiation, such as Auger electron–emitting 111In-NLS-trastuzumab and radiosensitizers (34). Achieving such a synergistic interaction by combining radiosensitizing chemotherapy and 111In-NLS-trastuzumab, compared with either of these therapies alone, could dramatically improve the response.
CONCLUSION
Methotrexate, paclitaxel, and doxorubicin radiosensitize trastuzumab-sensitive and trastuzumab-resistant human breast cancer cell lines overexpressing HER2 to 111In-NLS-trastuzumab, and the combination of radiosensitizing chemotherapy and targeted Auger electron radiotherapy with this radiopharmaceutical, compared with either of these agents alone, is more cytotoxic to these cells. The radiosensitizing effects of these agents were shown to be mediated through changes in cell cycle distribution and partly through inhibition of DNA repair (methotrexate and doxorubicin) after exposure to 111In-NLS-trastuzumab. These results are promising for the development of novel regimens for radioimmunotherapy of HER2-amplified breast cancer incorporating low-dose, radiosensitizing chemotherapy.
Acknowledgments
This research was supported by grants 016456 and 019513 from the Canadian Breast Cancer Research Alliance, funds from the Canadian Cancer Society, and a predoctoral fellowship from the Canadian Breast Cancer Foundation (Ontario Chapter).
Footnotes
-
↵* Contributed equally to this work.
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 23, 2009.
- Accepted for publication November 24, 2009.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multi-omics analysis of endothelial cells reveals the metabolic diversity that underlies endothelial cell functions
- Cancer Tissue Classification, Associated Therapeutic Implications and PDT as an Alternative
- Experimental Radionuclide Therapy of HER2-Expressing Xenografts Using Two-Step Targeting Nuclisome Particles
- Changes in Lognormal Shape Parameter Guide Design of Patient-Specific Radiochemotherapy Cocktails