


Abstract
Although studies have shown that 18F-FDG PET, when used to assess the response of malignant lymphoma after treatment, has a strong ability to predict relapse, its diagnostic accuracy in clinical practice remains unclear. The aim of this study was to systematically review the diagnostic accuracy of 18F-FDG PET in detecting residual disease at the completion of first-line therapy of Hodgkin's disease (HD) and aggressive non-Hodgkin's lymphoma (NHL). Methods: We searched relevant articles from 1966 to July 2006 using MEDLINE, EMBASE, SCOPUS, Biological Abstracts, bibliographies, review articles, and textbooks without language restriction. One assessor (for non–English-language studies) or 2 assessors (for English-language studies) independently reviewed each article to abstract relevant study characteristics and results. Relevant individual patient data or subgroup data were provided by the investigators if they were unavailable from the publications. We estimated summary receiver operating characteristic curves and confidence regions for summary sensitivity and specificity. Results: Nineteen studies consisting of 474 HD and 254 aggressive NHL patients were included. These studies had heterogeneity and suboptimal methodologic quality and reporting. Reported ranges for the sensitivity and specificity of 18F-FDG PET in predicting disease relapse were 0.50–1.00 and 0.67–1.00, respectively, for HD and 0.33–0.77 and 0.82–1.00, respectively, for NHL. These estimates were similar when conventional imaging tests showed a residual mass. For HD studies, the summary receiver operating characteristic curves were similar irrespective of whether a residual mass was detected by conventional tests. Factors explaining the variability of diagnostic estimates were not identified. Conclusion: Although currently available evidence is still limited, 18F-FDG PET seems to have good diagnostic accuracy for assessing residual HD at the completion of first-line treatment. Clinical data on this use of 18F-FDG PET for aggressive NHL are more limited. Prospective studies with a more rigorous research design, conduct, and reporting would more reliably reveal the clinical diagnostic accuracy of this imaging modality.
Persistence of a mass after completion of first-line therapy is a common problem in assessing the response of both Hodgkin's disease (HD) and non-Hodgkin's lymphoma (NHL) (1,2). Based on the likelihood of residual disease, clinicians need to proceed to further therapeutic interventions such as applying radiotherapy to the residual mass or salvage chemotherapy with or without high-dose chemotherapy followed by stem cell transplantation. Therefore, more accurate diagnostic tests to distinguish a posttherapy disease mass from fibrosis or scar tissue are needed to reduce the likelihood of unnecessary and potentially toxic therapy (3).
18F-FDG PET is a promising functional imaging test for patients with malignant lymphoma and other malignancies and has gained wide use during the last decade (4). Its routine use has been recommended to assess the posttherapy response of HD, especially if CT reveals a residual mass (3). Others have also recommended its use for the same purpose on the basis of its high negative predictive value for HD and high positive predictive value for NHL (5). A recent survey of physicians caring for lymphoma patients found that intended management plans were often changed on the basis of 18F-FDG PET results (6).
Recently, a systematic review explored the diagnostic accuracy of 18F-FDG PET for this purpose and assessed the quality of the included studies (7). Similar to studies of diagnostic tests in other medical fields, this review revealed several methodologic problems affecting both the internal and the external validity of the published studies. The authors, however, estimated summary diagnostic accuracy without considering the effect of major methodologic variability on diagnostic tests underlying the original studies. For example, some of the studies included a mix of NHL histologies consisting of indolent, aggressive, and highly aggressive lymphomas, and others included a mix of patients consisting of those who received first-line therapy and those who received salvage therapy. The diagnostic accuracy estimates reported from these studies have limited external validity and cannot be directly applied to specific clinical scenarios; each distinct histologic subtype has its unique clinical profiles, such as treatment strategies, responses, and prognoses. Also, the review did not consider the different ways that the primary studies presented results (e.g., individual patient vs. each lymphoma lesion, all involved sites vs. only bulky disease, or single vs. multiple inclusions of a patient).
This study was an updated systematic review of the diagnostic accuracy of 18F-FDG PET in assessing the response of HD and aggressive NHL after first-line therapy, with special emphasis on the methodologic issues discussed above.
MATERIALS AND METHODS
Study Identification
We searched MEDLINE and EMBASE from January 1966 through July 2006 without language restriction. The detailed search strategy can be found in Supplemental Table 1 (supplemental materials are available online only at http://jnm.snmjournals.org). This search was augmented by SCOPUS and Biological Abstracts. We also manually reviewed the reference lists of eligible studies, review articles, and textbooks.
Study Selection
Two of us reviewed the pertinent studies to determine eligibility. We included prospective or retrospective studies evaluating posttherapy response assessment by 18F-FDG PET exclusively for patients with HD or aggressive NHL followed by clinical follow-up, with or without pathologic confirmation as a reference standard. We included studies that evaluated at least 10 patients. We considered aggressive NHL to be mantle cell lymphoma; follicular center lymphoma, grade III; diffuse large B-cell lymphoma (DLBCL); primary mediastinal large B-cell lymphoma; peripheral T-cell lymphoma, unspecified; angioimmunoblastic T-cell lymphoma; angiocentric lymphoma; and anaplastic large cell lymphoma, T- and null-cell type by the Revised European–American Classification of Lymphoid Neoplasms (REAL)/World Health Organization classification, or corresponding subcategories for the International Working Formulation classification, the Kiel classification, or the Rappaport classification (8). We included studies of only those patients who completed first-line chemotherapy, radiotherapy, or combined-modality therapy and underwent conventional imaging tests such as CT, ultrasonography, or MRI for posttreatment restaging just before or after undergoing PET. We focused our analysis on studies that reported individual patients as the unit of analysis irrespective of the number of relapses or of the sites of relapse or residual disease, because this is the most appropriate perspective for clinical decision making. We excluded abstracts, editorials, comments, letters, review articles, and case reports. We excluded studies enrolling patients with HIV-associated or posttransplant lymphoproliferative disorders.
Many studies did not meet all the rigorous inclusion criteria but did partially include a relevant patient population. For these studies, we contacted the authors by mail or email to ask for individual patient data or subgroup data relevant to our inclusion criteria. When there was no response within 3 wk, another correspondence was sent. When there was no response to the third communication attempt, we considered the request rejected.
Data Abstraction
Two independent, board-certified hematologists abstracted relevant data for English-language articles. For non–English-language articles, data were extracted by a single reviewer working with a physician native speaker of the relevant language. We used an abstraction form consisting of items recommended in the Standards for Reporting of Diagnostic Accuracy (9). One nuclear medicine specialist evaluated the technical specifications and quality of the PET procedure by using recommended guidelines (10). The reviewers knew in which journals the studies had been published. Based on the enrollment of participants before PET, we categorized studies into 2 groups: “posttherapy evaluation,” or studies that included patients irrespective of restaging results on conventional imaging tests, and “residual mass evaluation,” or studies that evaluated only patients for whom visible residual mass lesions were shown on conventional imaging tests. In the posttherapy evaluation, we also abstracted the data on the subgroup of patients who had a residual mass shown on imaging. If the relevant data were unavailable from the published literature, we contacted the authors of the paper to request the subgroup data. Inconsistencies between reviewers were either clarified by the paper authors or resolved by consensus.
Assessment of Study Quality and Applicability
To evaluate the quality and applicability of the studies included in this review, we used an established quality rating system for diagnostic studies (11) and a recently proposed quality evaluation tool (12). In the established system, we examined 6 aspects of study quality: quality and application of the reference standard, independence of test interpretation, description of patient characteristics, cohort assembly, and sample size. We then rated each study as “a” (the highest quality), “b,” “c,” or “d” (the lowest quality) according to the predefined score. The recently proposed quality evaluation tool, which was designed exclusively for studies of diagnostic accuracy, comprehensively explores both methodologic quality and reporting. The tool consists of 14 items addressing patient spectrum, reference standard, disease progression bias, partial and differential verification bias, test review bias, clinical review bias, incorporation bias, test execution of both index test and reference standard, study withdrawals, and indeterminate test results.
Data Synthesis and Statistical Analysis
For each study, we constructed a 2 × 2 contingency table consisting of true-positive, false-positive, false-negative, and true-negative, where all patients were categorized as being PET-positive or -negative and as being positive or negative for disease according to the results determined through 18F-FDG PET and the reference standard, respectively. We defined as disease-positive a patient who had biopsy-confirmed residual disease or whose disease had relapsed during clinical follow-up. We did not independently combine the sensitivity and specificity of the included studies because this approach does not take into account the interdependence of these 2 test parameters. We instead estimated summary receiver operating characteristic (ROC) curves and elliptic 95% confidence regions of summary sensitivity and specificity by the hierarchical summary ROC method (13). This model is a more sophisticated approach than the conventional linear regression model to compute summary diagnostic measures taking account of variations both within a study and between studies. We fitted the model by using maximum-likelihood estimation implemented in the NLMIXED procedure of SAS/STAT (version 8; SAS Institute) (14). Then, we depicted the summery ROC curves and confidence regions for summary sensitivity and specificity by using Stata (version 8.2.; Stata Corp.) (15). Also, we estimated the area under the curve and the Q* statistic, the point on the curve where sensitivity equals specificity, as global measures for the summary ROC curves. We explored heterogeneity between studies by visual assessment of ROC plots for the following predetermined items: study design (prospective vs. retrospective), rates of patients with residual mass as found on conventional imaging tests, relapse rates, follow-up period, timing of PET scan after completion of therapy, and publication year. We also performed post hoc subgroup analyses for the items used for the technical specifications of PET and quality assessment.
RESULTS
Study Characteristics
We included 19 studies: 9 studies (16–24) that met all eligibility criteria and 10 studies (25–34) with relevant published data or with unpublished data obtained by contacting the authors of the paper (Table 1). The detailed process by which articles were selected can be found in the Supplemental Appendix and in Supplemental Figure 1. Because one group of researchers reported a “residual therapy evaluation” for HD and aggressive NHL and a “posttherapy evaluation” exclusively for aggressive NHL—and included in both groups the data on some participants (23,29)—we separately extracted the relevant data. Another group of researchers published an updated “posttherapy evaluation” for HD, with some participants overlapping from the previous report (27,31). We contacted the principal investigator and obtained updated combined results. For 5 studies that reported both HD and aggressive NHL (25–28,30), the contacted investigators provided unpublished subgroup data for each category. As a result, we finally had for further evaluation 15 studies consisting of 474 patients with HD and 8 studies consisting of 254 patients with aggressive NHL (Table 2).
Studies Included in the Systematic Review
Patient Characteristics for Studies Included in the Systematic Review
Most studies were retrospective (Table 1). Four studies exclusively evaluated patients for whom a posttherapy visual residual mass was found on conventional imaging tests (25,29,32,34). Generally, patients underwent PET 1–3 mo after completing therapy, but some underwent PET at less than 1 mo. Most studies included both adult and adolescent patients, but 3 studies also included pediatric patients (16,21,24).
For HD studies, nodular sclerosis was the leading histologic subcategory and either ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) or MOPP (nitrogen mustard, vincristine, procarbazine, prednisone) plus ABVD or ABV (doxorubicin, bleomycin, vincristine) with or without radiotherapy was the most widely reported first-line treatment (Table 2). In posttherapy evaluations, 35%–72% of patients were found to have a residual mass on conventional imaging (Supplemental Table 2). Relapse rates were similar for both posttherapy evaluations and residual mass evaluations, ranging from 4% to 55% and 0% to 50%, respectively.
For aggressive NHL studies, DLBCL was the leading histologic subcategory, and the most widely adopted first-line therapy was CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) or comparable doxorubicin-containing regimens with or without radiotherapy (Table 2). In posttherapy evaluations, 26%–56% of patients were found to have a residual mass on conventional imaging (Supplemental Table 2). Relapse rates were 33%–60% for posttherapy evaluations and 33%–67% for residual mass evaluations.
Concerning imaging techniques and technologies, although their reporting was limited, the included studies generally followed the guidelines of the Society of Nuclear Medicine for performing 18F-FDG PET (Supplemental Table 3). Only a single study used PET/CT (30). Most studies adopted qualitative diagnostic criteria: foci of elevated 18F-FDG uptake unexplained by physiologic uptake. Two studies (32,34) also adopted quantitative diagnostic criteria: standardized uptake values (the ratio of 18F-FDG uptake in tumor sites to that in normal sites). Only 2 studies clearly reported that all the included participants underwent pretherapy PET (17,23). Generally, experienced nuclear medicine physicians interpreted the results.
Sensitivity, Specificity, and Summary ROC Curves
HD studies reported widely ranging sensitivities and specificities for 18F-FDG PET. For posttherapy evaluations, sensitivity ranged from 0.50 to 1.00 and specificity ranged from 0.67 to 1.00 (Supplemental Table 2; Fig. 1). For residual mass evaluations, reported estimates had a similarly wide range: 0.43–1.00 for sensitivity and 0.67–1.00 for specificity. The summary ROC curves and confidence regions for summary sensitivity and specificity for posttherapy evaluations and residual mass evaluations were similar (Fig. 2): The area under the curve for the summary ROC curve was 0.94 for posttherapy evaluations and 0.93 for residual mass evaluations, and the Q* statistic was 0.88 for posttherapy evaluations and 0.86 for residual mass evaluations.
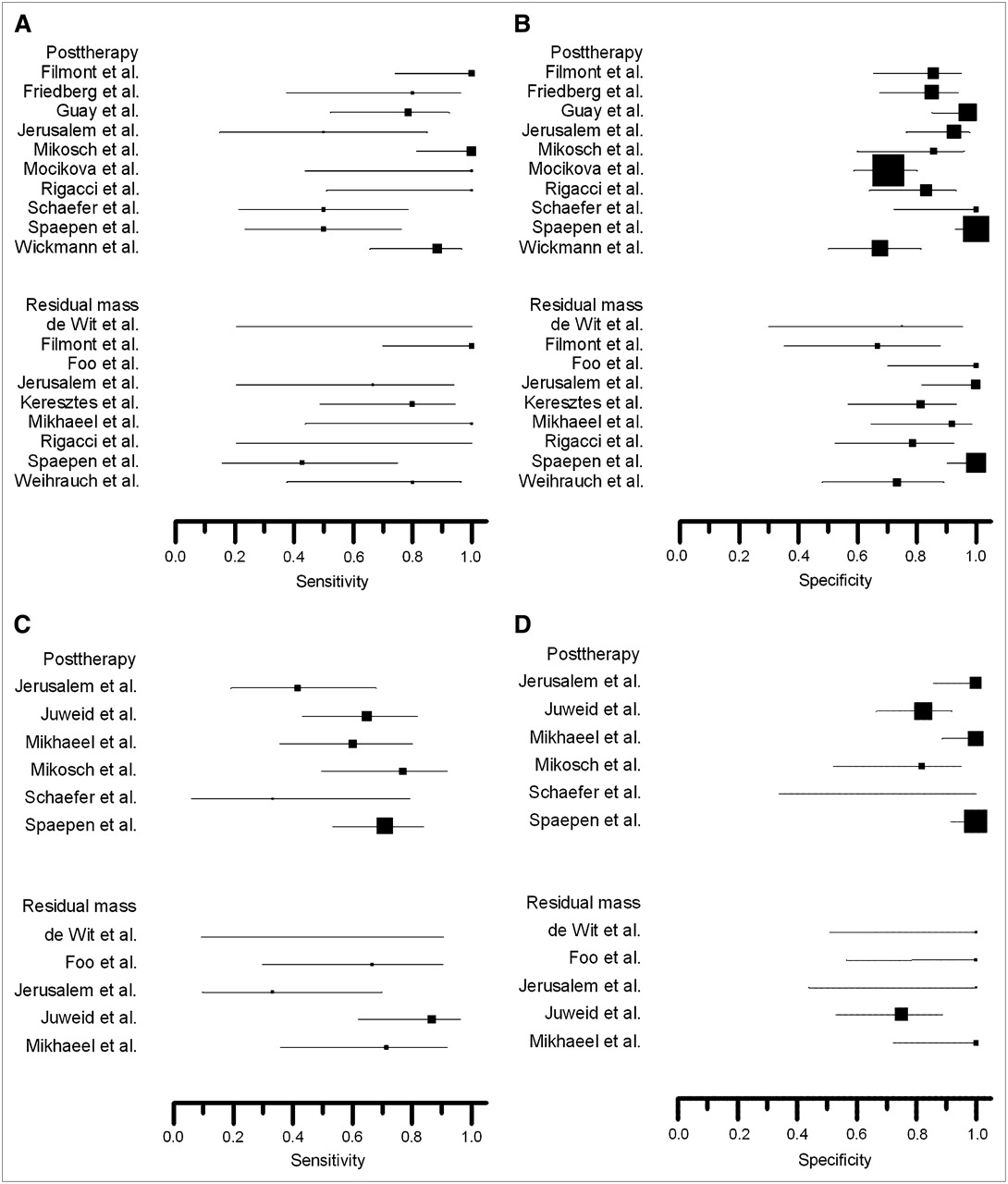
Sensitivity and specificity for HD (A and B) and aggressive NHL (C and D). Size of square plotting symbol is proportional to sample size (for sensitivity, number of patients who relapsed; for specificity, number of patients in remission) for each study. Horizontal lines are 95% confidence intervals. One study (Foo et al.) is omitted for sensitivity for HD because there were no cases of relapse.
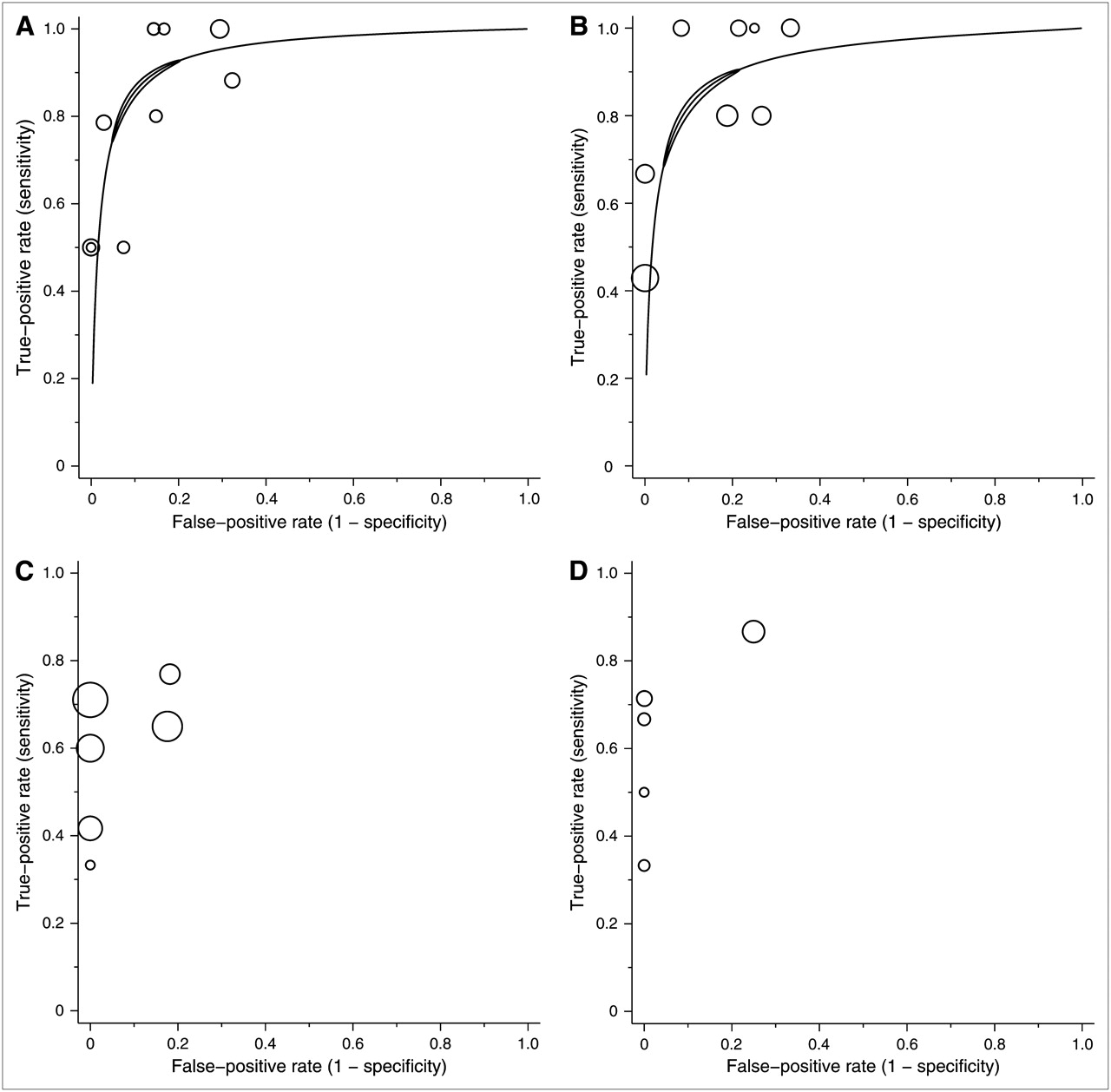
ROC plotting and summary ROC curve of 18F-FDG PET for HD and aggressive NHL. Individual study estimates of sensitivity and 1 − specificity are shown for posttherapy evaluation and residual mass evaluation of HD (A and B) and aggressive NHL (C and D). Size of each circle is proportional to sample size for each study (all study participants). Solid crescent boundary represents 95% confidence region for summary sensitivity and specificity.
Studies of aggressive NHL also reported a widely ranging sensitivity but a narrower high specificity. For posttherapy evaluations, sensitivity ranged from 0.33 to 0.77 and specificity ranged from 0.82 to 1.00 (Supplemental Table 2; Fig. 1). For residual mass evaluations, sensitivity ranged from 0.33 to 0.87 and specificity ranged from 0.75 to 1.00. We did not perform the metaanalysis because there were too few data points to reliably estimate the summary ROC curves and confidence regions for summary sensitivity and specificity.
Investigating Heterogeneity
We did not identify any clinical or 18F-FDG PET test characteristics, or any items that assessed the quality and applicability of each study, to explain the heterogeneity of sensitivity and specificity (data not shown).
Quality Assessment of Published Studies
Overall, the quality and reporting of the included studies were limited (Supplemental Table 4), suggesting that they are subject to bias and variation limiting the internal and external validities, respectively, of the test results. The detailed results of the quality assessment can be found in the Supplemental Appendix.
DISCUSSION
This systematic review showed that the reported sensitivities and specificities of 18F-FDG PET to assess residual disease for patients with HD who completed first-line chemo- or chemoradiotherapy had large between-study heterogeneity. In addition, the summary ROC curves and confidence regions for sensitivity and specificity showed similar and good overall diagnostic accuracy irrespective of the presence of a visible residual mass on conventional imaging modalities such as CT or MRI. For aggressive NHL, although our review showed a relatively stable high specificity and variable sensitivity, there were too few studies to calculate a reliable overall diagnostic accuracy.
Many potential factors may explain the heterogeneity. For test characteristics, differences in the type of PET scanner, in the timing of PET after the completion of therapy, in positive test criteria, and in the clinical experience of the interpreters are relevant. For patient characteristics, several differences should be considered: in the type of histology, especially for aggressive NHL (e.g., DLBCL vs. other aggressive NHLs); in therapeutic strategy (e.g., chemotherapy vs. combined-modality therapy); in the presence or absence of a visible residual mass on conventional imaging tests; and in relapse risk groups, such as the international prognostic score for advanced-stage HD (36) or the international prognostic index for aggressive NHL (8). For study characteristics, differences such as method of patient selection (e.g., prospective vs. retrospective), type and application of a reference standard, and patient follow-up have been reported to affect the variability of sensitivity and specificity (9,37). Because the available data were limited, we could not identify specific factors that explain the heterogeneity, which should be further addressed in future studies. Although the reported positive PET criteria appeared almost identical in all HD studies, the large crescent shape of the confidence regions implies a negative correlation between sensitivity and specificity across the included studies, suggesting that a variation in threshold may partially explain the between-study heterogeneity.
Our study had several important limitations. Because we selected only those studies for which pertinent data were available, several important investigations (some of which were included in the previous metaanalysis) may have been excluded. Also, because most data were derived from retrospective studies with poor-quality design and reporting, our conclusions are subject to the bias and variations in the original studies (37). In addition, our review included only a single study in which patients with DLBCL received rituximab in addition to CHOP (22). Because the combination of rituximab with CHOP is a current standard therapy (38), our results may be less applicable to clinical practice. Further, we included only a single study (30) that used a relatively new and promising additional technique—PET/CT—that may overcome the current technical limitations of PET (39).
In the recently revised consensus recommendations, 18F-FDG PET has become an important component of posttherapy response assessments in clinical trials for HD and DLBCL (40). Although the currently available data have limitations, our systematic review would probably support the clinical relevance of the response criteria for high-risk HD; incomplete response defined by positive PET findings would have an excellent ability to predict relapse irrespective of whether a residual tumor mass is found on conventional imaging. For favorable-risk HD, patients labeled as incomplete responders after first-line therapy should still have a moderate possibility of long-term remission. Thus, clinical investigators adopting the recommendations into therapeutic efficacy trials would need to decide how to manage patients in this category before implementing the trials. For DLBCL and other aggressive NHLs, our results based on the limited clinical evidence would not suffice to support the criteria, and further research is necessary to validate them.
Our review shows that currently available data do not suffice to answer the phase 3 question of diagnostic accuracy studies: What is the diagnostic accuracy of 18F-FDG PET for posttherapy response assessment of malignant lymphoma? (41). Reliable clinical evidence is especially limited for aggressive NHL. Further investigation should include prospective diagnostic accuracy studies (phase 3) of PET or PET/CT that adopt a more rigorous research methodology. We propose that, ideally, diagnostic accuracy studies should accompany prospective clinical trials to answer efficacy questions. Data on additional therapy, such as involved-field radiotherapy or high-dose chemotherapy with autotransplantation, for posttherapy PET-positive patients are limited. Before the routine clinical implementation of a treatment strategy based on posttherapy PET findings, randomized studies should assess the impact on patients' clinical outcomes, if appropriate (phase 4) (41). Also, determination of the cost-effectiveness of treatment strategies adopting PET is necessary to allow a better understanding of the role of posttherapy PET.
CONCLUSION
The currently available data show that 18F-FDG PET has good overall accuracy in detecting residual disease in patients with HD who have completed first-line therapy. The current literature has methodologic weaknesses that may overestimate accuracy. Because data from original studies are limited, our review could not find robust evidence to answer the question of whether clinicians should routinely use PET to assess the posttherapeutic response, suggesting that they should be cautious about making clinical decisions based solely on a PET result.
Acknowledgments
We thank Maike de Wit, MD, Jerusalem Guy, MD, Malik Juweid, MD, Katalin Keresztes, MD, Peter Mikosch, MD, Heidy Mocikov, MD, Robert Pichler, MD, Niklaus Schaefer, MD, and Martin Weihrauch, MD, for providing the data on their original work; Yinghua Li, MD, and Leo Kawaguchi, MD, for assistance in translating Chinese- and German-language publications; Jonathan Deeks, PhD, Kengo Ito, MD, and Kazuo Kubota, MD, for helpful comments; Petra Macaskill, PhD, for providing statistical programs; and Bruce Cheson, MD, and Joseph Lau, MD, for reviewing the manuscript. Part of this work was supported by Grant-in-Aid 15-2 for Cancer Research from the Ministry of Health, Labor, and Welfare of Japan, by the Japanese Society of Nuclear Medicine, and by Nihon Medi-Physics Corporation Limited.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 15, 2007.
- Accepted for publication August 18, 2007.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Fact Sheet About Interim and End-of-Treatment 18F-FDG PET/CT in Lymphoma
- Response Assessment Criteria and Their Applications in Lymphoma: Part 2
- End-Therapy Positron Emission Tomography for Treatment Response Assessment in Follicular Lymphoma: A Systematic Review and Meta-analysis
- 18F-FDG PET Is an Independent Outcome Predictor in Primary Central Nervous System Lymphoma
- Interim FDG-PET in Hodgkin lymphoma: a compass for a safe navigation in clinical trials?
- How does PET/CT help in selecting therapy for patients with Hodgkin lymphoma?
- Positron emission tomography/computed tomography surveillance in patients with lymphoma: a fox hunt?
- Role of Routine Imaging in Lymphoma
- 18F-FDG PET/CT for Early Response Assessment in Diffuse Large B-Cell Lymphoma: Poor Predictive Value of International Harmonization Project Interpretation
- Volume-of-Interest Assessment of Oncologic Response Using 18F-FDG PET/CT: A Phantom Study
- Metabolic Imaging Allows Early Prediction of Response to Vandetanib
- Fluorine-18-Fluorodeoxyglucose Positron Emission Tomography in Response Assessment Before High-Dose Chemotherapy for Lymphoma: A Systematic Review and Meta-Analysis
- Fluorine-18-Fluorodeoxyglucose Positron Emission Tomography for Interim Response Assessment of Advanced-Stage Hodgkin's Lymphoma and Diffuse Large B-Cell Lymphoma: A Systematic Review
- Prognostic Value of Interim 18F-FDG PET in Patients with Diffuse Large B-Cell Lymphoma: SUV-Based Assessment at 4 Cycles of Chemotherapy
- Primary Mediastinal B-Cell Lymphoma