


Abstract
Dynamic PET studies with a 68Ga-bombesin analog, DOTA-PEG2-[d-Tyr6, β-Ala11,Thi13,Nle14] BN(6-14) amide (68Ga-BZH3; DOTA is 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid, and PEG is ethylene glycol [2-aminoethyl-carboxymethyl ether]), were performed on patients with gastrointestinal stromal tumors (GIST) to investigate the impact of complementary receptor scintigraphy on diagnosis and the potential of a radionuclide treatment. Furthermore, dynamic 18F-FDG studies were performed on the same patients. Methods: This study comprised 17 patients with GIST. All patients were scheduled for therapy with imatinib because of unresectable primary or recurrent GIST or because of metastatic disease. Dynamic PET scans using 68Ga-BZH3 and 18F-FDG were obtained on 2 consecutive days. Multivariate analysis was used to evaluate the kinetic data. Standardized uptake values (SUVs) were calculated, and a compartmental model (2-tissue) and noncompartmental model were used for data evaluation of both tracers. Results: Fourteen of 17 patients (25/30 lesions) were positive for uptake on 18F-FDG imaging, whereas 68Ga-BZH3 demonstrated an enhanced accumulation in 7 of 17 patients (8/30 lesions). Thirteen lesions were confirmed by histologic examination, and the remaining 17 were confirmed by follow-up. One recurrent tumor in the stomach could not be delineated on 18F-FDG imaging but showed enhanced 68Ga-BZH3 uptake. The median SUV for 68Ga-BZH3 was 3.3, in comparison with 7.9 for 18F-FDG. Best-subset analysis demonstrated that the global SUV (55–60 min after injection) for 18F-FDG was primarily dependent on k3, followed by k1. Multivariate analysis did not show a significant correlation between the kinetic parameters (k1–k4, fractional blood volume, and SUV) for 18F-FDG and bombesin. Conclusion: 68Ga-BZH3 may be helpful for diagnostic reasons in a subgroup of patients with GIST, as in the case of negative 18F-FDG findings and suspicion of viable tumor tissue. The meaning of the enhanced 68Ga-BZH3 uptake is open at the moment.
Gastrointestinal stromal tumors (GIST) are tumors that occur in the wall of the bowel and are thought to be derived from the cells of Cajal, which drive peristalsis in the intestine. Most GIST show a gain-of-function mutation in the cKIT proto-oncogene resulting in ligand-independent activation of the cKIT receptor tyrosine kinase (1). PET with 18F-FDG is frequently used for oncologic applications to assess tissue viability. Especially in patients with GIST, 18F-FDG is being used for staging and therapy monitoring. Not all patients respond to imatinib mesylate, and many of those who initially respond may later become resistant. Therefore, new therapeutic approaches are needed. One idea is to study the expression of different receptors to guide therapy in that direction. It has recently been shown that somatostatin receptors can be quite well imaged using a new radiolabeled compound, 68Ga-DOTA-d-Phe1-Tyr3-octreotide (DOTATOC). In patients with neuroendocrine tumors, DOTATOC has successfully been used both for diagnostic purposes, labeled with 68Ga, and for therapy, labeled with 90Y (2). Reubi et al. reported in a recent paper that GIST expressed bombesin subtype 2 receptors, better known as gastrin-releasing peptide receptors, using in vitro receptor autoradiography (3). The authors reported that not only primary GIST but also metastases and even tumor samples from patients who did not respond to imatinib were receptor-positive. On the basis of these data, in patients with GIST we used for the first time 68Ga-bombesin, in terms of a pan-bombesin analog, the peptide DOTA-PEG2-[d-Tyr6,β-Ala11,Thi13,Nle14] BN(6-14) amide (BZH3; DOTA is 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid, and PEG is ethylene glycol [2-aminoethyl-carboxymethyl ether]).
Because of the increased spatial resolution of PET and its ability to quantify biodistribution, the pan-bombesin analog BZH3 was labeled with the positron emitter 68Ga, which has a half-life of 68.3 min for the positron emission (4). BZH3 binds to at least 3 receptor subtypes: bombesin receptor subtypes 1 (also known as neuromedin B), 2, and 3. The aim of this study was to investigate the impact of complementary receptor scintigraphy on diagnosis and the potential of a radionuclide treatment. Furthermore, bombesin kinetics were compared with 18F-FDG kinetics. We compared the bombesin kinetic data derived from a 60-min full dynamic acquisition with those obtained from the dynamic 18F-FDG data. For quantitative analysis of both tracers, a 2-tissue-compartment model and a noncompartment model based on the fractal dimension were used. In particular, we evaluated different kinetic parameters such as k1–k4 and VB, which reflects the fraction of blood within the evaluated volume, and compared them with global tracer uptake (SUV) to find which parameter has the greatest impact.
MATERIALS AND METHODS
68Ga for PET was obtained from a 68Ge/68Ga generator, which consists of a column containing a phenolic ion exchanger (manufactured in-house) loaded with 68Ge and coupled in series with a small-sized anion-exchanger column (AG 1 × 8 Cl− ion-exchange resin, 200–400 mesh; Bio-Rad) to concentrate 68Ga during elution. This generator provides 68Ga with an average yield of 60% for more than 1.5 y. 68Ga-BZH3 was prepared according to the method described by Schuhmacher et al. (4).
For 18F-FDG studies, all patients fasted for at least 4 h before undergoing PET. Blood glucose levels were measured immediately before PET began and were within normal levels (<130 mg/dL). 18F-FDG was prepared according to the method described by Toorongian et al. (5).
The study included 17 patients with histologically proven GIST. Two of the patients had primary GIST without previous treatment and were scheduled for preoperative imatinib therapy because of unresectable tumors. The remaining 15 patients were previously treated with surgery and were scheduled for imatinib therapy because of suggestive metastatic lesions on CT or MRI. Five of these patients received imatinib before undergoing PET. All 17 patients were scheduled for imatinib therapy and underwent an 18F-FDG PET study for staging and a bombesin PET study for assessment of bombesin receptor expression. Dynamic PET studies were performed for 60 min after the intravenous application of 300–370 MBq of 18F-FDG and 150–210 MBq of 68Ga-BZH3 (3 nmol) using a 28-frame protocol (10 frames of 30 s, 5 frames of 60 s, 5 frames of 120 s, and 8 frames of 300 s) on 2 consecutive days. A dedicated PET system (ECAT EXACT HR+; Siemens) with an axial field of view of 15.3 cm, operated with septa extended (2-dimensional mode), was used for patient studies. The system allows the simultaneous acquisition of 63 transaxial slices with a theoretic slice thickness of 2.4 mm. Before application of the radionuclide, transmission scans for a total of 10 min were obtained for attenuation correction of the acquired emission tomographic images. All PET images were corrected for attenuation, and an image matrix of 256 × 256 pixels was used for iterative image reconstruction. Conversion of reconstructed images to SUV images was based on the following formula (6): standardized uptake value (SUV) = tissue concentration (Bq/g)/(injected dose [Bq]/body weight [g]). The SUV 55–60 min after injection was used for the analysis of both tracers.
Dynamic PET data were evaluated using the software package PMOD (provided courtesy of PMOD Technologies Ltd.) (7,8). Areas with enhanced tracer uptake on transaxial, coronal, and sagittal images were evaluated visually. Time–activity curves were created using volumes of interest. A volume of interest consists of several regions of interest over the target area. Irregular regions of interest were drawn manually. To compensate for possible patient motion during the acquisition, the original regions of interest were visually repositioned but not redrawn. A detailed quantitative evaluation of tracer kinetics requires the use of compartmental modeling. A 2-tissue-compartment model was used to evaluate the dynamic studies. This methodology is standard, particularly for the quantification of dynamic 18F-FDG studies (9,10).
One problem in patient studies is accurate measurement of the input function, which theoretically requires arterial blood sampling. However, the input function can be retrieved from the image data with good accuracy (11). For the input function, the mean value of the volume-of-interest data obtained from a large artery, such as the descending aorta, was used. The constants k1–k4 were calculated using a 2-compartment model implemented in the PMOD software taking into account VB in a volume of interest as an additional variable. Details about the applied compartmental model have been described by Burger and Buck (7). The model parameters were accepted when k1–k4 was less than 1 and VB exceeded 0. The unit for the rate constants k1–k4 was 1/min.
Concerning the 68Ga-BZH3 kinetics, again the 2-tissue-compartment model was applied to the data. In the case of 68Ga-BZH3, k1 is associated with receptor binding, k2 with displacement from the receptor, k3 with cellular internalization, and k4 with externalization. For 18F-FDG, k1 is associated with influx of the tracer, k2 with efflux, k3 with phosphorylation, and k4 with dephosphorylation. VB, which is associated with the volume of blood exchanging with tissue, was calculated as a separate parameter.
Besides the compartmental analysis, a noncompartmental model based on the fractal dimension was used. The fractal dimension is a parameter of heterogeneity and was calculated for the time–activity data of each individual volume of interest. The values for fractal dimension vary from 0 to 2, showing the deterministic or chaotic distribution of tracer activity. We used a subdivision of 7 × 7 and a maximal SUV of 20 for the calculation of fractal dimension (12).
The data were statistically evaluated using JMP IN software (version 5.1; SAS Institute GmbH) on a notebook computer (MacBook Pro, 2.16 GHz, 2 GB of random-access memory; Apple) running with the Mac OS X operating system (Apple). The statistical evaluation used descriptive statistics, box plots, and linear regression analysis. The parameters for measuring linear fit were determined by the least-squares method.
Each patient gave written informed consent to participate in the study and to have their medical records released. The study was performed with the approval of the institutional review board.
RESULTS
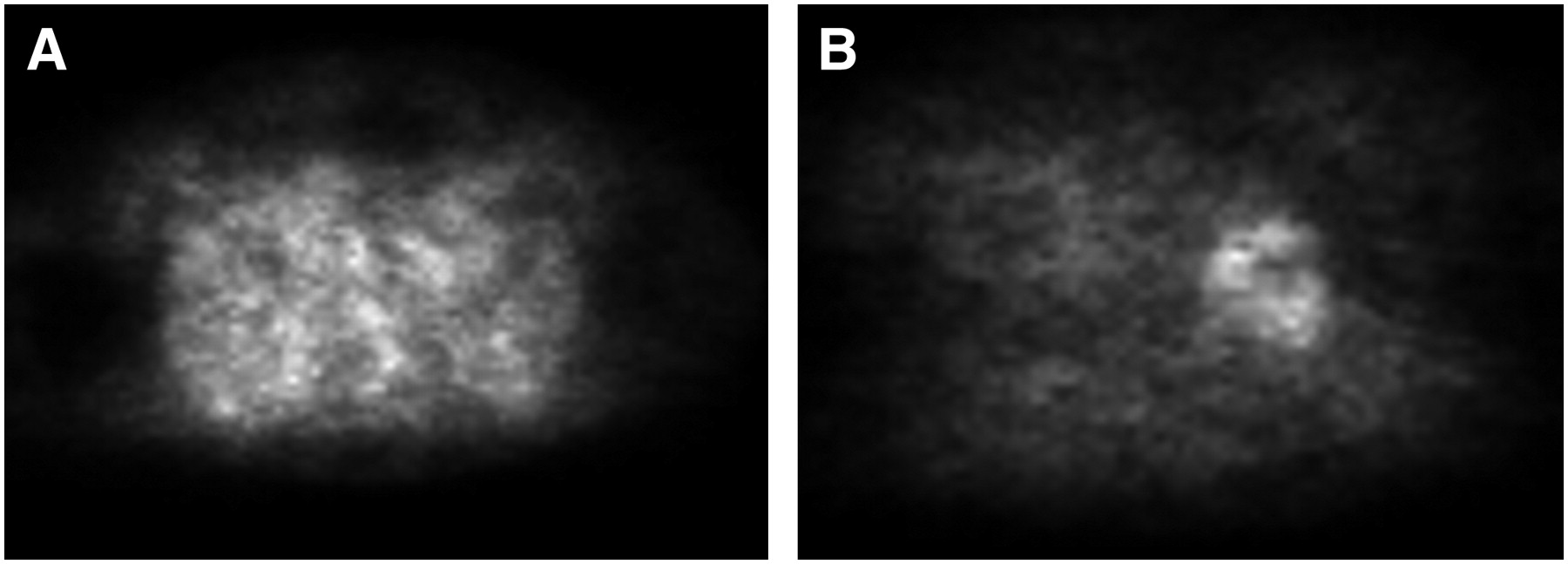
The evaluation comprised 17 patients with 30 lesions, including 2 primary lesions (stomach and rectum), 3 recurrent lesions (stomach), and 25 metastatic lesions (12 liver metastases, 10 gut lesions, 2 pelvic lesions, and 1 soft-tissue metastasis in the upper leg). All study patients were scheduled for therapy with imatinib because of unresectable primary or recurrent GIST or because of metastatic disease. Of the 30 evaluated lesions, 13 were confirmed by histologic evaluation and 17 by clinical follow-up. Fourteen of 17 patients (25/30 lesions) showed increased 18F-FDG uptake in the primary or recurrent tumor or in the metastases. Two hypermetabolic areas were falsely classified as tumors on the basis of the 18F-FDG findings. These 2 findings were in the gastroesophageal junction (average SUV, 2.8) and in the colon ascendens (average SUV, 3.5). The lack of correlative pathologic findings on CT and MRI and on clinical follow-up confirmed that these 18F-FDG findings were not due to malignancy. Four lesions in 2 patients who received imatinib therapy were true-negative on the basis of clinical follow-up data. A lesion in a patient with recurrent, histologically confirmed GIST of the stomach could not be delineated on the 18F-FDG scan (false-negative). Comparison with the histologic data revealed a low proliferative activity, with a Ki-67 of less than 10%, in this patient. However, this recurrent tumor showed enhanced 68Ga-BZH3 uptake (Fig. 1).
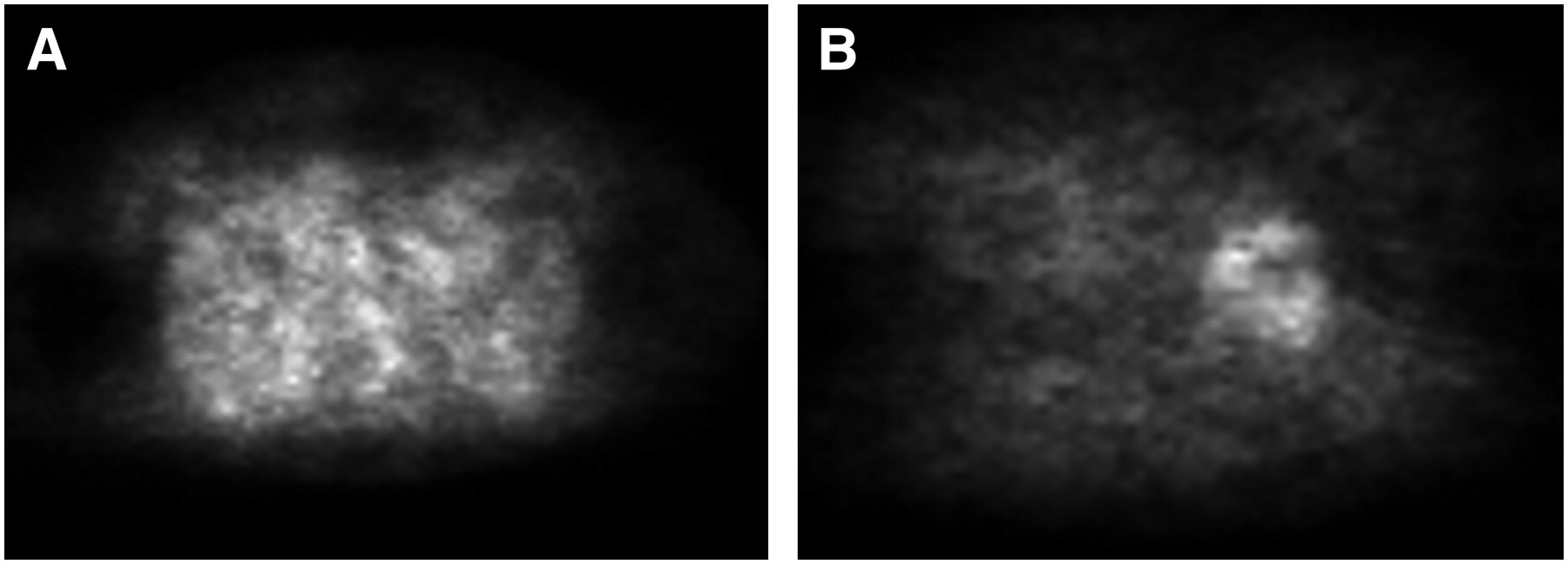
Patient with recurrent GIST in stomach. (A) Transaxial 18F-FDG image (SUV image) at level of upper abdomen shows no significantly enhanced 18F-FDG uptake in stomach. (B) Corresponding transaxial bombesin image (SUV image) at level of upper abdomen shows enhanced bombesin uptake in stomach (SUV, 9.3).
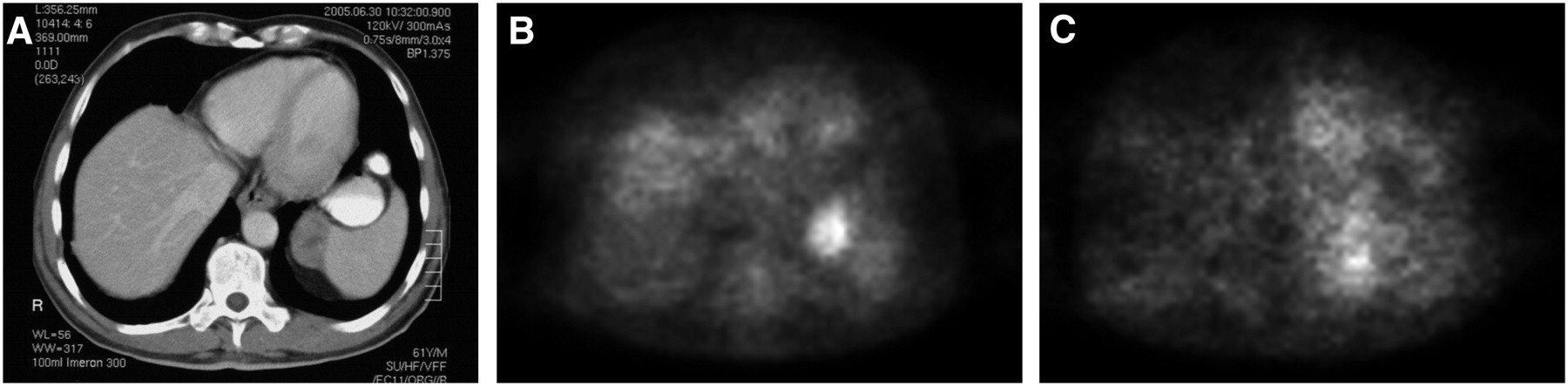
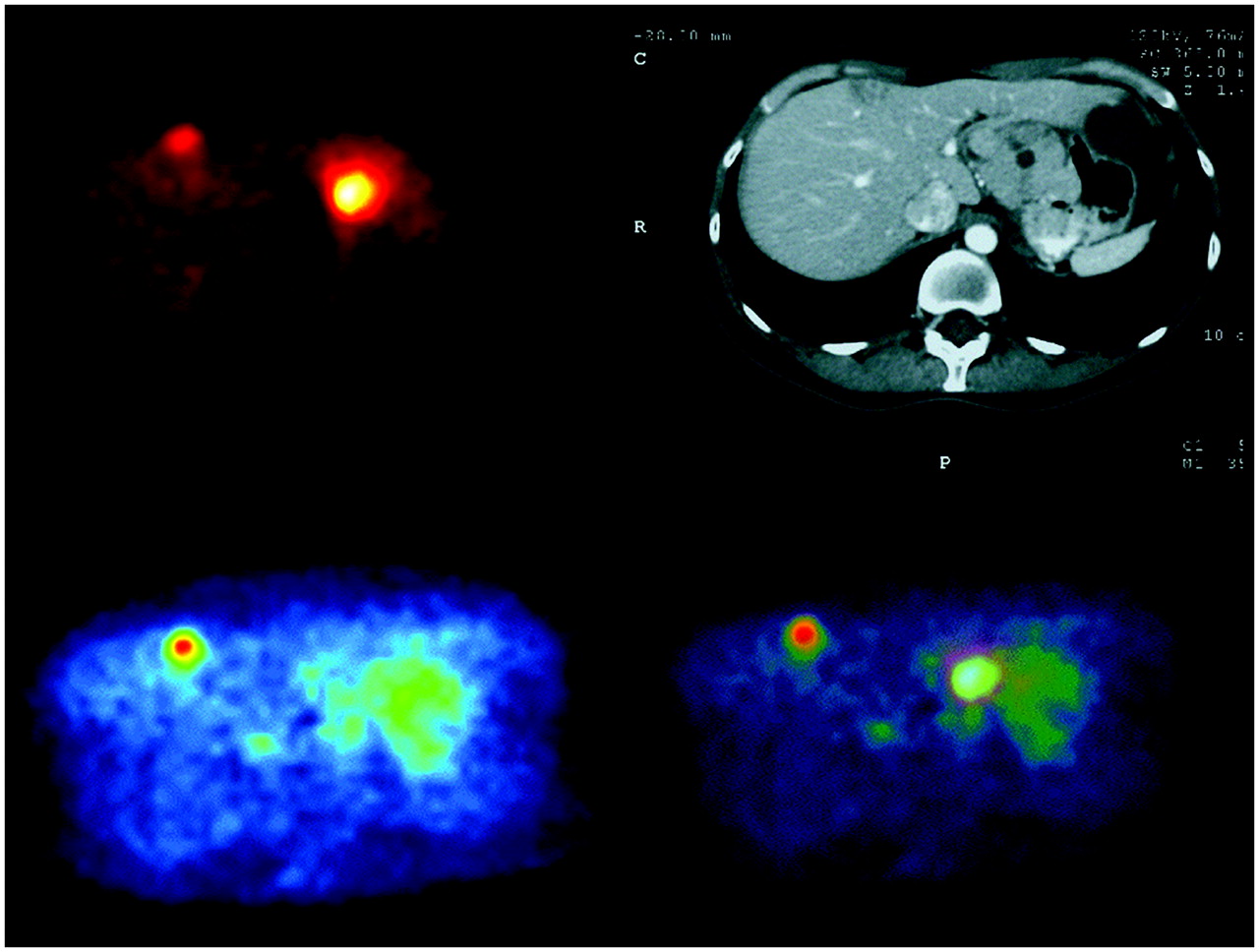
We noted physiologically uniform enhanced 68Ga-BZH3 uptake in the entire pancreas of all patients. 68Ga-BZH3 uptake in the evaluated tumor lesions was generally lower than 18F-FDG uptake, and 8 of 30 evaluated lesions (7/17 patients) could be delineated through the enhanced bombesin uptake. We found no difference in 68Ga-bombesin uptake with respect to imatinib pretreatment. Two of 5 patients who received imatinib before PET demonstrated enhanced 68Ga-BZH3 uptake. Figure 2 shows an example of a patient with GIST of the stomach and a suggestive metastatic lesion medial to the spleen (Fig. 2A). The 18F-FDG images clearly showed enhanced 18F-FDG uptake in this area (Fig. 2B). The bombesin images showed diffuse enhanced uptake ventral to the spleen (Fig. 2C). Figure 3 demonstrates another patient with 2 suggestive lesions on CT, one in the stomach and a smaller one in the right liver lobe. Whereas both lesions could be delineated clearly on the 18F-FDG images because of hypermetabolism, the bombesin images revealed enhanced uptake of the labeled peptide primarily in the smaller lesion in the liver. Histologic examination revealed recurrent GIST of the stomach and a liver metastasis.

(A) CT image of patient with metastatic GIST demonstrates soft-tissue mass medial to spleen. (B) Transaxial 18F-FDG image (SUV image) at level of CT image shows enhanced 18F-FDG uptake (SUV, 3.2) at location of CT finding. (C) Corresponding transaxial bombesin image (SUV image) at level of CT image shows slightly enhanced bombesin uptake (SUV, 2.0) at location of CT finding.

(Top left) Transaxial 18F-FDG image (SUV image) at level of liver demonstrates 2 hypermetabolic areas, one in ventral part of right liver lobe (SUV, 5.8) and another in stomach (SUV, 17.1), in patient with metastatic GIST. (Top right) CT image at same level demonstrates the 2 hypodense lesions in stomach and liver. (Bottom left) Transaxial bombesin image (SUV image) at level of CT image demonstrates clearly enhanced bombesin uptake only in liver lesion (SUV, 2.6). Bombesin uptake in stomach shows slight diffuse enhancement. (Bottom right) Fused image of 18F-FDG and bombesin transaxial slice shows an agreement for both tracers in the liver lesion, whereas the enhanced 18F-FDG uptake in the stomach is assigned to a low-bombesin-uptake area. Histology revealed recurrent stomach tumor and liver metastasis.
The 56- to 60-min SUV for 68Ga-BZH3 was highly variable, with a range of 0.5–9.3 (median, 3.3). The 56- to 60-min SUV for 18F-FDG was higher, with a range of 2.4–17.0 (median, 7.9). k1, k2, and in particular k3 for 68Ga-BZH3 were lower than the corresponding values for 18F-FDG, whereas VB was higher for bombesin (Table 1).
Data Summary
Box plots of 18F-FDG and 68Ga-BZH3 uptake (56- to 60-min SUV) in tumor tissue are presented in Figure 4A. The transport rate constants k1 and k3 and the vascular fraction VB of both tracers are presented in Figure 4B. The data show higher SUV, k1, and k3 values for 18F-FDG than for bombesin. VB was higher for bombesin. No significant correlation was found between the kinetic parameters of bombesin and of 18F-FDG for the evaluated lesions.

(A) Box-and-whisker plot of median SUV for both tracers 56–60 min after injection in malignant lesions. (B) Box-and-whisker plot of median values for both tracers for VB, k1, and k3 in malignant lesions.
We used linear regression analysis to determine the effect of each kinetic parameter (k1–k4 and VB) on global SUV. Analysis of the 18F-FDG data revealed the highest positive F score for k3 (F = 8.5, P = 0.008), followed by k1 (F = 5.7, P = 0.025). The bombesin data could not be analyzed because of the low number of positive lesions.
DISCUSSION
18F-FDG still has a major impact on the diagnostics and management of patients with GIST (13,14). Although 18F-FDG is the tracer of choice, the aim of this study was to investigate the impact of complementary receptor scintigraphy on diagnosis and the potential for a radionuclide treatment, such as 90Y-DOTATOC treatment of patients with neuroendocrine tumors. Furthermore, the study compared the kinetic data of 68Ga-BZH3 with those of 68Ga-DOTATOC and 18F-FDG.
Receptor imaging has found a use in nuclear oncology, with somatostatin receptor imaging being widely used in oncologic patients, primarily those with neuroendocrine tumors. We have reported 68Ga-DOTATOC studies on patients with neuroendocrine tumors, meningiomas, and non–small cell lung cancer (2,15). Bombesin analogs labeled with γ- or β-emitting radionuclides have found some limited use for imaging prostate cancer, breast carcinoma, and small cell lung tumors. Gastrin-releasing peptide receptors were found to be predominantly expressed in human prostate cancer (100%), gastrinoma (100%), and breast cancer (70%), whereas concomitant expression of gastrin-releasing peptide receptors (33%) and bombesin receptor subtype 3 (40%) was found in small cell lung cancer (16). These data are comparable to our currently presented results on GIST patients, only a subgroup of whom demonstrated enhanced 68Ga-BZH3 uptake. However, because of the lack of immunohistochemical studies in this study, the question is open as to whether enhancement of 68Ga-BZH3 uptake was due to overexpression of only one bombesin receptor subtype or of all.
We used a pan-bombesin analog, BZH3, labeled with 68Ga. Experimental results on rats have been reported by Zhang et al. using 111In- and 177Lu-labeled pan-bombesin peptides, BZH1, and BZH2.The authors performed biodistribution studies on Lewis rats bearing a rat pancreatic carcinoma cell line, AR4-2J, which is known to express high levels of bombesin receptors (16). Zhang et al. reported a high uptake for both of these radiolabeled peptides in AR4-2J tumors and in organs—such as the pancreas—positive for gastrin-releasing peptide receptor. The high pancreatic uptake is comparable to our results in GIST patients. We noted homogeneously enhanced 68Ga-BZH3 uptake in the normal pancreatic tissue of all examined patients. Schuhmacher et al. performed biodistribution studies with 68Ga-BZH3 on rats bearing the same pancreatic tumor cell line, AR4-2J (4). The authors found a high affinity for 68Ga-BZH3 and rapid internalization. Clearance of 68Ga-BZH3 from the circulation and from normal tissues negative for gastrin-releasing peptide receptor was fast and resulted in low background activity and high tumor-to-tissue ratios as early as 1 h after injection (4). On the basis of these data, we decided to use a 60-min acquisition protocol for the 68Ga-BZH3 studies. The quantitative analysis was based on the 2-tissue-compartment model because receptor binding is given by k1. Schuhmacher et al. reported a high receptor affinity in cells and a low nonspecific binding of the tracer (<3.5%). Furthermore, they reported a high internalization rate, which is reflected by k3, when using the 2-tissue-compartment model. The fraction of internalized 68Ga-BZH3 activity compared with total cell-associated activity was 85% after 1 h of incubation in AR4-2J cells. This value indicates a primarily enhanced expression of bombesin receptor subtype 1 and bombesin receptor subtype 2.
One important aspect of PET is the possibility of performing noninvasive highly accurate quantitative measurements of tracer concentration in patients. The use of a 2-compartment model is generally an accepted approach to the assessment of 18F-FDG kinetics (10). Concerning bombesin kinetics, k1 is a parameter that reflects receptor binding, and k3 is a parameter that reflects internalization of the tracer. Unfortunately, only a few studies have been performed on humans to assess rate constants in malignant tumors, and to our knowledge, no data have been published on the kinetics of 68Ga-BZH3 in patients. Kinetic data exist for the tracer 68Ga-DOTATOC, a substrate for somatostatin receptor subtype 2, which was applied in patients with meningiomas and neuroendocrine tumors at our institution using the same methodology (17,18). The reported mean k3 for DOTATOC in neuroendocrine tumors was 0.113, in comparison with 0.047 for bombesin in GIST, whereas the reported mean k1 for DOTATOC in neuroendocrine tumors was 0.529, in comparison with 0.5 for bombesin in GIST. The data may indicate a higher internalization rate for DOTATOC than for bombesin.
From the diagnostic point of view, the 18F-FDG studies were superior and revealed enhanced uptake in 25 of 30 lesions. However, 2 lesions in the gastrointestinal tract were false-positive with 18F-FDG, as subsequently shown by clinical follow-up data. Whether these false-positive results could have been avoided by using a combined PET/CT scanner is an open question. Interestingly, a histologically confirmed recurrent stomach tumor that could not be delineated on the 18F-FDG study demonstrated enhanced 68Ga-BZH3 uptake (Fig. 1). It is reported that 18F-FDG primarily measures viable tumor tissue (19). In contrast, it is also known that there is an association between 18F-FDG uptake and proliferation rate (20). Therefore, a possible explanation for the low 18F-FDG uptake may be the low viability or the low proliferative activity as measured by Ki-67 (<10%). Generally, 68Ga-BZH3 uptake was lower than 18F-FDG uptake, and only a subgroup (41%) of the patients demonstrated enhanced uptake. This finding differs from that in 15 patients with neuroendocrine tumors studied with 68Ga-DOTATOC, all of whom demonstrated enhanced DOTATOC uptake (57/63 evaluated lesions) (18). The data differ from the present study, in which only 7 of 17 patients with GIST demonstrated enhanced 68Ga-BZH3 accumulation (mean SUV of 3.3, compared with the surrounding tissue). The data give evidence of a subgroup (41%) of GIST patients who demonstrate enhanced receptor expression. On the basis of these preliminary results, receptor scintigraphy with bombesin cannot be generally recommended. The idea of performing radionuclide therapy—analogous to giving 90Y-DOTATOC therapy to patients with neuroendocrine tumors—cannot be supported by these results because of the relatively low uptake in most patients. Further studies on larger numbers of patients are needed to confirm these results.
CONCLUSION
Quantitative 18F-FDG data showed enhanced viability in 25 of 30 lesions (14/17 patients; median SUV, 7.9). Only 8 of 30 lesions (7/17 patients) demonstrated enhanced 68Ga-BZH3 uptake (median SUV, 3.3). One recurrent GIST in the stomach was delineated only on the 68Ga-BZH3 scans; 18F-FDG uptake was low. The data demonstrate a subgroup of GIST lesions that show enhanced bombesin receptor expression. The meaning of the enhanced 68Ga-BZH3 uptake is not yet certain.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 12, 2006.
- Accepted for publication April 23, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Head-to-Head Comparison of [68Ga]Ga-NOTA-RM26 and [18F]FDG PET/CT in Patients with Gastrointestinal Stromal Tumors: A Prospective Study
- Gastrin-Releasing Peptide Receptor Imaging and Therapy in the Era of Personalized Medicine
- MITIGATE-NeoBOMB1, a Phase I/IIa Study to Evaluate Safety, Pharmacokinetics, and Preliminary Imaging of 68Ga-NeoBOMB1, a Gastrin-Releasing Peptide Receptor Antagonist, in GIST Patients
- Bombesin-Targeted PET of Prostate Cancer
- "To Serve and Protect": Enzyme Inhibitors as Radiopeptide Escorts Promote Tumor Targeting
- Radiopeptide Imaging and Therapy in Europe
- Evaluation of a 1,4,7,10-Tetraazacyclododecane-1,4,7,10-Tetraacetic Acid-Conjugated Bombesin-Based Radioantagonist for the Labeling with Single-Photon Emission Computed Tomography, Positron Emission Tomography, and Therapeutic Radionuclides
- Peptide-Based Probes for Cancer Imaging
- Therapeutic Consequences from Molecular Biology for Gastrointestinal Stromal Tumor Patients Affected by Neurofibromatosis Type 1
- International Union of Pharmacology. LXVIII. Mammalian Bombesin Receptors: Nomenclature, Distribution, Pharmacology, Signaling, and Functions in Normal and Disease States