


Abstract
The clinical utility of 18F-FDG PET in evaluating salivary gland malignancies has not been well defined. We therefore evaluated the utility of 18F-FDG PET in management for patients with salivary gland cancers. Methods: Thirty-four patients with newly diagnosed salivary gland cancers underwent CT and 18F-FDG PET before surgical resection with radiotherapy. The diagnostic accuracies of CT and 18F-FDG PET for detecting primary tumors and neck metastases were compared with a histopathologic reference. We determined the relationship between the maximum standardized uptake value (SUV) of the tumor and clinicopathologic parameters such as sex, age, local tumor invasion, T and N categories, TNM stage, and histologic grade, as well as their associations with disease-free survival (DFS). Results: 18F-FDG PET was more sensitive than CT for the detection of primary tumors (91.2% vs. 79.4%; P < 0.05), cervical metastases (80.5% vs. 56.1%; P < 0.05), and distant metastases in 2 patients at initial staging. High-grade malignancies had higher mean maximum SUVs than did low- and intermediate-grade malignancies (4.6 vs. 2.8; P = 0.011). T and N categories were independent determinants of DFS (P < 0.05), but the maximum SUV (4.0) was not. During a mean follow-up of 25.1 mo, 18F-FDG PET correctly diagnosed local–regional recurrences in 6 patients and new distant metastases in 9 patients. Conclusion: Our findings indicate that, in patients with salivary gland malignancies, 18F-FDG PET is clinically useful in initial staging, histologic grading, and monitoring after treatment but not in predicting patient survival.
Salivary gland tumors are relatively rare, constituting 3% of all head and neck neoplasms. Most salivary gland tumors originate in the parotid gland, with three fourths of parotid gland tumors being benign. However, the majority of minor salivary gland tumors are malignant (1). Salivary gland tumors may be assessed before surgery by clinical evaluation, CT, or MRI, which is not necessarily specific to the types of tumors (2). Fine-needle aspiration biopsy (FNAB) is also commonly used, but its accuracy is not completely reliable in differentiating benign from malignant tumors or in histologic grading, with a reported accuracy of about 85% in detecting parotid gland malignancies (2). 18F-FDG PET has been shown to be superior to conventional imaging in evaluating patients with head and neck malignancies (3–5). In patients with squamous cell carcinomas and lymphomas, the major types of head and neck malignancies, 18F-FDG PET is now used in initial staging, management of recurrent cancers, and therapeutic monitoring (6–8). The pathology of salivary gland tumors differs from that of other head and neck tumors, and the utility of 18F-FDG PET in evaluating salivary gland cancers is now being investigated (9–14). Prior studies revealed that 18F-FDG PET alone, however, cannot be used to classify salivary gland tumors as benign or malignant (9–11). In addition, previous studies did not adequately define the role of 18F-FDG PET in management for patients with salivary gland malignancies (13). We therefore evaluated the role of 18F-FDG PET in preoperative staging, histologic grading, and prediction of therapy outcomes in patients with salivary gland malignancies.
MATERIALS AND METHODS
Patient Population
Patients presenting with histologically confirmed, newly diagnosed salivary gland cancers between October 2001 and March 2005 were enrolled in this study. All study patients were assessed by FNAB as well as by CT and 18F-FDG PET before and at fixed intervals after treatment. Patients with lymphomas, non–salivary gland tumors, and tumors metastasizing to the salivary glands; patients previously treated for salivary gland cancers; or patients not assessed by 18F-FDG PET before and after treatment were excluded from this study.
Imaging
All patients in this study underwent PET with an ECAT HR+ scanner (Siemens/CTI), which provided an in-plane spatial resolution of 4.5 mm (reconstructed resolution of images, 10 mm) and an axial field view of 15.5 cm. All patients fasted for at least 6 h before 18F-FDG PET, and their blood glucose concentrations were measured; patients with diabetes mellitus had to have blood glucose levels below 200 mg/dL before the scan. All patients rested for at least 1 h before the 18F-FDG PET scan. Beginning approximately 60 min after the intravenous injection of about 555 MBq of 18F-FDG, whole-body imaging was performed with the patient in the supine position. Data were reconstructed into coronal, sagittal, and transverse sections and a 3-dimensional rotating projection. The standardized uptake value (SUV) was calculated from attenuation-corrected images, the amount of injected 18F-FDG, the body weight of each patient, and the cross-calibration factors for 18F-FDG PET and the dose calibrator.
As a separate staging evaluation, CT of the head and neck was performed with a LightSpeed QX/i scanner (GE Healthcare) or a Somatom Sensation 16 (Siemens Medical Solutions), with a slice thickness of 3–5 mm. Patients were placed in the supine position, and contrast-enhanced axial images were obtained parallel to the occlusal line from the skull base to the upper chest. In selected patients, direct coronal or coronal reconstruction images were also obtained.
Treatment
All but 1 patient with distant metastases underwent resection of the primary tumor with or without neck dissection (Table 1). Supraomohyoid neck dissection (levels I–III) was performed in 13 patients suspected of having high-grade or locally invasive tumors, clinically negative involvement of nodes, or involvement of a single small node. Modified or radical neck dissection (levels I–V) was performed in 14 patients with involvement of multiple nodes or extracapsular nodal spread. Bilateral neck dissection was performed in 1 patient suspected of having bilateral disease. Twenty-seven of 34 patients (79.4%) received postoperative local–regional radiotherapy (mean dose, 62.3 Gy; range, 34.2–68.4 Gy) with single daily fractions. One of 2 patients with distant metastases at initial staging received palliative chemotherapy and radiotherapy, whereas the other underwent primary tumor resection of an adenoid cystic carcinoma despite having lung metastases.
Demographic and Clinical Characteristics of Study Population (n = 34)
Image Interpretation and Histologic Examination
The degree of suspected malignant involvement was based on qualitative visual interpretation of the images and determination of the maximum SUV, a semiquantitative measure of relative 18F-FDG uptake within the regions of interest. 18F-FDG PET images were reviewed to calculate the SUV, and a slice containing the tumor was selected. The maximum SUV of primary tumors was used as a reference for correlation with survival.
CT results were interpreted by experienced radiologists. Nodes were considered to have metastatic involvement when central necrosis or nonhomogeneous enhancement was present, when their largest axial diameter was greater than 1.5 cm in the jugulodigastric region or greater than 1 cm in other cervical regions, or when there was a cluster of 3 or more lymph nodes of borderline size. The 18F-FDG PET and CT readers were unaware of each other's results or of the pathology results.
To correlate CT and 18F-FDG PET results, the primary tumor sites were recorded, and the neck was divided into right and left, with 5 levels each, encompassing surgically accessible regional lymph node groups and based on nodal classification by imaging (15). The neck dissection samples were sorted relative to cervical levels I–V. Primary tumors and lymph nodes were dissected from the specimens and histopathologically examined. Local invasiveness, the histologic grade of the primary tumors, the total number of lymph nodes in the specimen, and the presence or absence of tumors within these nodes were recorded by an experienced pathologist.
Statistical Analysis
The sensitivity of each imaging modality for detecting primary tumors was compared with the histologic data. The sensitivity, specificity, accuracy, and predictive values of each imaging method were calculated on the basis of the presence of positive findings in the neck and at cervical levels and were compared by use of the McNemar test. A 2-tailed P value was used to compare 18F-FDG PET with CT. The χ2 test or the t test was used to compare SUV categories and other clinical variables (sex, age, local tumor invasion, T category, N category, TNM stage, and histologic grade).
Actuarial disease-free survival (DFS) and overall survival rates were calculated by the Kaplan–Meier method. Persistent or recurrent tumor was documented by CT or MRI or by 18F-FDG PET. The time interval for local control and survival endpoints was calculated from the first day of treatment until the date of an event or of the last follow-up. The log-rank test was used to assess the correlation of these endpoints with the SUV and with the aforementioned clinicopathologic variables. The Cox proportional hazards model was used for multivariate analysis. Variables shown to be significant in univariate analysis were selected for the Cox model. A P value of less than 0.05 was considered statistically significant.
RESULTS
The patient cohort consisted of 34 patients (25 men, 9 women) with a mean age of 61 y (range, 25–72 y) (Table 1). The most common sites of primary salivary gland cancers were the parotid and submandibular glands, with salivary duct and adenoid cystic carcinomas being the most common histologic types. The primary tumors were graded histologically as low (n = 9), intermediate (n = 6), or high (n = 19). Local invasion of the extraparenchymal soft tissues, nerve, bone, or skin was detected in 21 of 34 patients (61.8%). Twenty-two patients were in the T3–T4 stage, and 16 had neck metastases. The primary tumors were completely removed in 29 of 33 patients who underwent surgery; their mean ± SD size in the largest histopathologic dimension was 3.1 ± 1.6 cm. Four patients had microscopic residual tumors at the surgical margins.
The sensitivity of 18F-FDG PET and CT for detecting primary tumors was 31 of 34 (91.2%) and 27 of 34 (79.4%), respectively (Table 2). In the other 7 patients, CT was unable to detect definitive primary mass lesions in 5 patients (Fig. 1), and lesions in 2 patients appeared to be multiple metastases from unknown primary sites. The primary tumor sites of the latter 2 lesions were the submandibular glands, and the SUVs of the primary lesions ranged from 2.3 to 4.2. The largest diameter of these 7 lesions was 1.4 ± 0.9 cm, and all lesions were detected by 18F-FDG PET. Of the 3 false-negative findings on 18F-FDG PET, 1 was an acinic cell carcinoma (Fig. 2), 1 was an epithelial–myoepithelial carcinoma of the parotid gland, and 1 was an adenoid cystic carcinoma of the submandibular gland. 18F-FDG uptake was indistinguishable from that of normal glands, with maximum SUVs ranging from 1.5 to 1.9; moreover, the largest diameter of all 3 tumors was less than 2.5 cm. All 3 lesions, however, were detected by CT.

(A) Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows). (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows). Salivary duct carcinoma of 1.7 cm arising in right submandibular gland, with multiple cervical metastases, was demonstrated histologically after surgery. (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy.

(A) Axial CT scan showing well-defined round enhancing lesion in right parotid gland (white arrow). (B and C) Lesion is obscured by normal parotid gland 18F-FDG uptake on PET images (black arrows).
Analysis of CT and PET for Detecting Primary Tumors and Neck Disease in Patients with Salivary Gland Cancers
Fifteen of 28 patients who underwent neck dissection had multiple cervical metastases. Multiple neck diseases were also suspected in 1 patient who had distant metastases at initial staging and so received only palliative chemoradiotherapy. Thus, 16 of 34 patients (47.1%) were thought to have cervical metastases of primary salivary gland cancers. Twenty-eight patients underwent dissection of 117 cervical levels and were included in the analysis of correlation of CT, 18F-FDG PET, and histology (Table 2). 18F-FDG PET accurately detected the presence or absence of cervical metastases in 25 of 28 patients (89.3%), whereas CT was accurate in 22 (78.6%). The sensitivity and specificity of 18F-FDG PET were significantly higher than those of CT (P < 0.05). Among the 117 cervical levels, 18F-FDG PET detected nodal disease accurately in 101 (86.3%), whereas CT was accurate in 93 (79.5%). The sensitivity of 18F-FDG PET was more than 20% higher than that of CT (P < 0.001), whereas the specificities of 18F-FDG PET and CT did not differ statistically (P > 0.05). 18F-FDG PET falsely interpreted neck disease in 3 of 28 patients (10.7%), yielding 2 false-positive findings and 1 false-negative finding. The false-positive findings were attributable to reactive or inflammatory nodes, whereas the false-negative finding was attributable to metastatic lymph nodes measuring less than 1.0 cm in the largest histologic dimension. In addition, 18F-FDG PET correctly detected lung or liver metastases in 2 patients at initial staging.
The maximum SUVs were 3.8 ± 2.1 (range, 1.4–8.7) for primary tumors and 4.9 ± 2.4 for cervical diseases (range, 1.5–8.8) (Table 1). When we used an SUV cutoff of 4.0 to compare SUV category and other clinicopathologic variables (Table 3), we found that only histologic grading was significantly related to SUV category (P = 0.019): high-grade salivary cancers tended to have increased focal 18F-FDG uptake. High-grade salivary malignancies had higher SUVs than did low- and intermediate-grade tumors (4.6 ± 2.2 vs. 2.8 ± 1.3; P = 0.011) (Fig. 3).
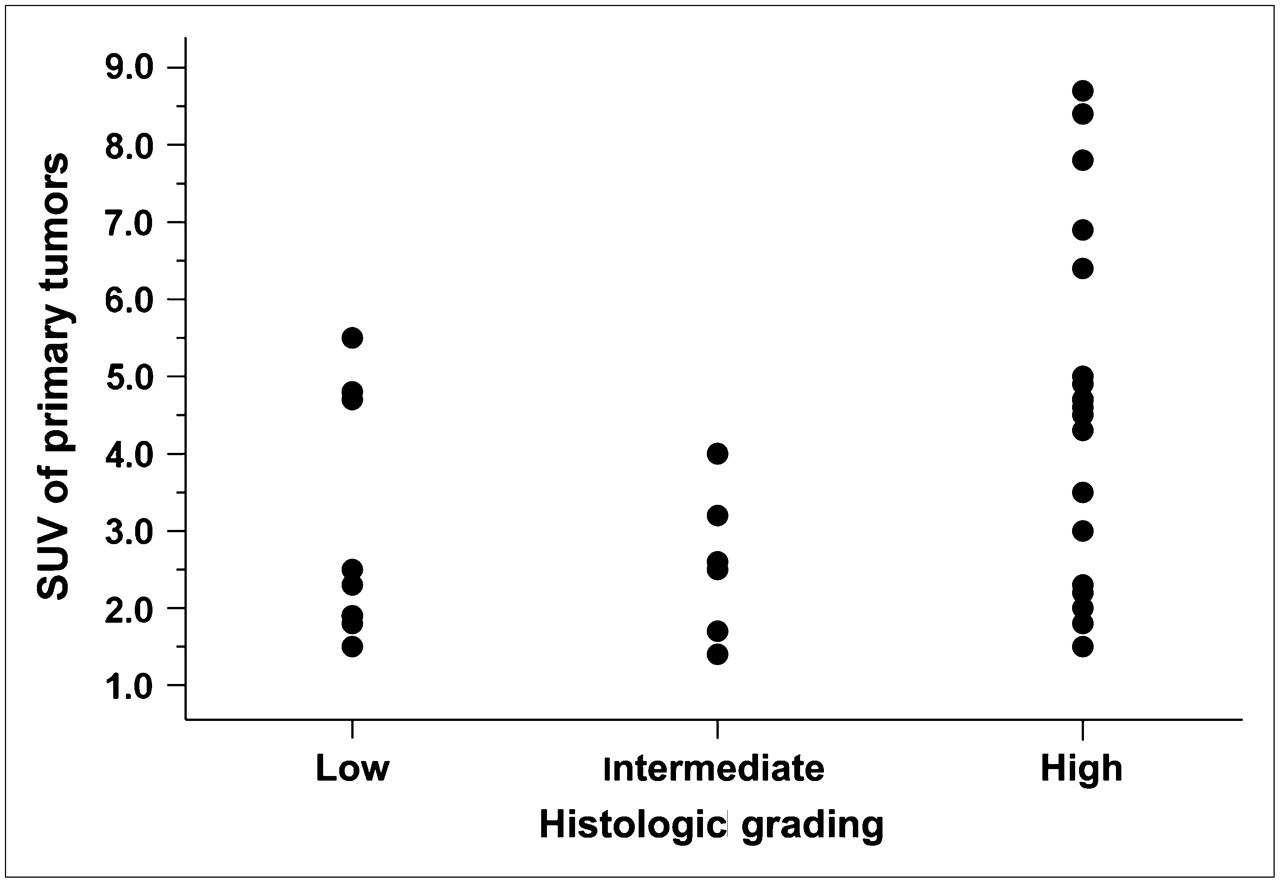
Maximum SUVs of primary tumors according to histologic grade. High-grade salivary malignancies had significantly higher maximum SUVs than did low- and intermediate-grade tumors (P = 0.011).
Analysis of 18F-FDG Uptake of Primary Tumors in Relation to Clinicopathologic Parameters in Patients (n = 34) with Salivary Gland Cancers
At the last follow-up, 22 patients were alive. The mean ± SD follow-up for surviving patients was 25.1 ± 13.7 mo (range, 12.3–56.6 mo). Six patients presented with persistent or recurrent local–regional diseases on FNAB and imaging by CT and 18F-FDG PET, and 9 presented with new distant metastases. At 2 y, actuarial local control was 87.1%, DFS was 57.0%, and overall survival was 66.4%.
The maximum SUV was not significantly higher in the 14 patients who presented with local, regional, or distant failure than in the 20 remaining patients (4.4 ± 2.3 vs. 3.4 ± 1.8; P = 0.164). Univariate analysis for DFS showed that local invasion, histologic grading, T category, N category, and TNM stage were statistically significant (P < 0.02) (Table 4). Patients with SUVs of greater than 4.0 had a somewhat lower 2-y DFS (40.0% vs. 72.2%), but this finding did not reach statistical significance (P = 0.153) (Fig. 4). In multivariate analysis, T category and N category remained statistically significant variables (P < 0.05).

Actuarial DFS according to SUV categories of primary tumors. Survival rates for patients with high 18F-FDG uptake (SUVs, >4.0) tended to be lower than those for patients with low SUVs (≤4.0), but difference was not statistically significant (P = 0.153).
Analysis of Clinicopathologic Factors in Relation to DFS
Twenty-two patients received follow-up CT, and 16 patients underwent follow-up 18F-FDG PET. Local–regional disease recurred in 6 patients, whereas local recurrence or progression was suspected in 4 patients; all were correctly identified by combined interpretation of CT and 18F-FDG PET. Follow-up 18F-FDG PET correctly diagnosed local–regional recurrence in all 6 patients, as shown by biopsy, and new distant metastases in 9 patients (Fig. 1D).
DISCUSSION
Salivary gland malignancy is currently managed primarily by resection of the primary tumor, possibly in combination with neck dissection or subsequent radiotherapy. Proper management requires accurate information about the site and extent of tumors. Our results for 34 salivary gland cancers are in agreement with previous evidence (4,5) suggesting that 18F-FDG PET is more sensitive than CT for detecting primary tumors in the head and neck. However, 18F-FDG PET failed to detect primary tumors in 3 of 34 patients, probably because normal physiologic uptake of 18F-FDG in the head and neck region, including the salivary glands, is common and often mimics or hides tumors (16). Generally, at our institution, the mean ± SD maximum SUV is lower in salivary gland malignancies (3.8 ± 2.1) than in squamous cell carcinomas of the upper aerodigestive tract (7.5 ± 3.4). Salivary gland malignancies with relatively low 18F-FDG uptake may therefore be easily obscured by the normal physiologic 18F-FDG uptake of the salivary glands, with a reported mean SUV range of 1.9–2.9 (16). All of the lesions with false-negative findings on 18F-FDG PET were low-grade malignancies, which generally have lower 18F-FDG uptake than high-grade malignancies, but were correctly detected by CT. Therefore, the combination of 18F-FDG PET and conventional CT or MRI may eliminate the potential drawbacks of 18F-FDG PET alone in detecting primary salivary gland tumors. Further, tumor detection may be increased with 18F-FDG PET/CT scans, which provide both functional and anatomic data and which have better spatial resolution than PET scans alone.
In detecting metastatic neck disease, preoperative 18F-FDG PET was also more sensitive than CT. The 2 false-negative findings on 18F-FDG PET occurred in patients with small tumors (<5 mm), which show 18F-FDG uptake similar to that of normal tissue. In addition, 18F-FDG uptake may be increased by inflammatory processes, contributing to false-positive results (17). These errors may not be corrected when conventional CT or MRI is combined with 18F-FDG PET. Our results for salivary gland tumors confirmed that the higher sensitivity and accuracy of 18F-FDG PET than of CT or MRI may help to determine the necessity and extent of neck dissection in patients with head and neck malignancies (3–5). However, false results on 18F-FDG PET or CT are commonly associated with inherent problems in the imaging modalities (17,18), suggesting that both of these imaging methods may not completely abrogate the need for pathologic staging based on primary resection and neck dissection, particularly in patients with high-grade salivary gland malignancies (19,20).
When we assessed the correlation between 18F-FDG uptake and tumor invasiveness or histologic grade, we found that histologic grading on the basis of clinicopathologic variables was significantly related to 18F-FDG uptake, defined as an SUV of greater than 4.0. High-grade salivary malignancies tended to have higher 18F-FDG uptake than low- or intermediate-grade salivary tumors. This finding is in agreement with previous reports showing that enhanced glucose metabolism, as determined by the SUV, is a strong index of tumor grade in other human malignancies, such as gliomas and soft-tissue sarcomas (21,22). To our knowledge, our study is the first to show a correlation between tumor 18F-FDG uptake and the histologic grade of salivary gland cancers. Because high 18F-FDG uptake can be found in benign salivary tumors, such as Warthin's tumors (9–12,14), however, the preoperative diagnosis of salivary gland masses should include FNAB, CT or MRI, or salivary gland scintigraphy as well as 18F-FDG PET. In addition, the SUV should not be used to differentiate high-grade from low-grade tumors, as the overlap among different tumor grades is too large. Because 18F-FDG PET was not associated with local tumor invasion, this characteristic may be better predicted by CT or MRI.
High 18F-FDG uptake is associated with aggressiveness in head and neck cancers and a low probability of survival (23–25). A similar association has been demonstrated for other human cancers, such as brain, lung, and esophagus cancers and malignant lymphomas (26–29); in all of these, the prognostic value of a high SUV may be independent of the tumor stage. 18F-FDG uptake in patients with salivary gland cancers, however, did not have similar prognostic significance in our study. In univariate and multivariate analyses, a high SUV was not a prognostic factor for survival. This result may have been attributable to the inclusion of patients with salivary gland pathologies and clinical features different from those of squamous cell carcinomas or lymphomas. Because salivary gland malignancies are relatively rare, only 34 patients were included in this study. This factor also may have affected the results for 18F-FDG uptake and survival. The utility of 18F-FDG PET in the monitoring of such patients after treatment is similar to that for other types of head and neck cancers; that is, 18F-FDG PET shows better detection of local–regional recurrences, distant metastases, and second primary malignancies than do conventional imaging modalities (30,31).
To our knowledge, the present study involved the largest series to date evaluating 18F-FDG PET in patients with salivary gland malignancies (9–14). We also focused only on malignant tumors of the salivary glands and tried to minimize potential biases by comparing 18F-FDG PET and CT results with those obtained histopathologically. However, our study may have been limited by the inclusion of various pathologies; by the high proportion of advanced-stage and high-grade malignancies, such as salivary duct carcinomas; by the inclusion of 6 patients with minor salivary gland cancers; and by the relatively short period after treatment. In addition, the retrospective design and the small number of patients may have been important limitations. Another source of potential bias was that we did not routinely perform 18F-FDG PET before treatment for all patients with salivary gland malignancies during the study period. Nevertheless, we found that 18F-FDG PET was clinically useful for evaluating salivary gland malignancies, a type of tumor that has not been studied extensively with 18F-FDG PET.
CONCLUSION
We investigated the clinical utility of 18F-FDG PET in management for patients with salivary gland malignancies. The roles of 18F-FDG PET in initial staging and monitoring after treatment are significant, potentially affecting management for these patients. Histologic grade may be predicted by 18F-FDG uptake, providing useful preoperative information for surgical planning. In contrast to the situation for other head and neck cancers, however, the utility of 18F-FDG uptake for predicting the survival of patients with salivary gland malignancies may not be significant.
Acknowledgments
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health and Welfare, Seoul, Republic of Korea (0620160-1).
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication October 10, 2006.
- Accepted for publication October 31, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endobronchial epithelial-myoepithelial carcinoma of the lung
- Prognostic Value of Preoperative Metabolic Tumor Volume and Total Lesion Glycolysis Measured by 18F-FDG PET/CT in Salivary Gland Carcinomas
- Variety and complexity of fluorine-18-labelled fluoro-2-deoxy-D-glucose accumulations in the oral cavity of patients with oral cancers
- Diagnostic Value of Neck Node Status Using 18F-FDG PET for Salivary Duct Carcinoma of the Major Salivary Glands
- Role of 18F-FDG PET/CT in Management of High-Grade Salivary Gland Malignancies