


Abstract
18F-FDG PET and PET/CT have shown clinical usefulness in the initial staging and follow-up of patients with salivary malignancy. Therefore, we evaluated the utility of 18F-FDG PET in preoperative staging, determining the extent of neck node involvement, and surgical planning for patients with salivary duct carcinoma (SDC) of the major salivary gland. Methods: We evaluated 18 patients with SDC who were assessed by 18F-FDG PET and CT before surgery. The sensitivity, specificity, accuracy, and predictive values of CT and PET/CT for predicting the primary tumor site and determining the extent of neck node involvement at each dissected neck level were evaluated by comparing imaging findings with pathologic nodal stage. Results: The median maximum standardized uptake value of the primary lesions and cervical nodes were 4.7 (range, 1.8–12.1) and 5.8 (range, 1.7–13.0), respectively. The sensitivities of 18F-FDG PET and CT for predicting the primary tumor site were 100% (18/18) and 94.4% (17/18), respectively. In analyzing cervical lymph nodes at 73 dissected neck levels, 18F-FDG PET had a sensitivity of 76.1%, a specificity of 96.3%, a positive predictive value of 97.2%, and a negative predictive value of 70.3%; the corresponding values for CT were 39.1%, 92.6%, 90.0%, and 47.2%, respectively. The sensitivity and negative predictive value were significantly higher for 18F-FDG PET than for CT (P < 0.001 and P = 0.03, respectively).18F-FDG PET determination of the extent of neck node involvement changed the neck dissection regimen in 5 patients (27.8%). Conclusion: SDC of the major salivary gland is a highly metabolic tumor with high 18F-FDG uptake. 18F-FDG PET is useful for evaluating neck node status and for determining surgical planning in patients with major salivary gland SDC.
Salivary duct carcinoma (SDC) is a rare, highly malignant tumor arising from the ductal epithelium of the salivary gland (1). Pathologically, SDC strongly resembles intraductal and invasive mammary duct carcinoma, which is why it was named SDC (1). Because the tumor is clinically characterized by rapid progression, with early nodal involvement and high rates of local recurrence, distant metastases, and tumor-related deaths (2–4), aggressive treatments are warranted. Because regional lymphatic spread is common at the time of diagnosis (5–8), complete surgical resection of the tumor and neck dissection, followed by adjuvant locoregional radiotherapy, are generally recommended in patients with SDC. Therefore, accurate evaluation of the extent of disease in patients with SDC is required to plan appropriate surgical therapy and the postoperative radiotherapy field.
Salivary gland cancer has a different pathology from other head and neck cancers, and although 18F-FDG PET/CT is helpful in differentiating benign from malignant disease in squamous cell head and neck cancer, several studies have shown that it is less accurate in salivary gland cancers (9–11). Recent studies, however, have shown that 18F-FDG PET and PET/CT are clinically useful for the initial staging and follow-up of patients with salivary malignancies (12–15). Therefore, we evaluated the utility of 18F-FDG PET for preoperative staging, determination of the extent of neck node involvement, and surgical planning for patients with SDC.
MATERIALS AND METHODS
Patients
Between January 2002 and July 2010, 29 patients with SDC were treated at the Asan Medical Center; of these, 18 patients were assessed by 18F-FDG PET and CT before surgery. Their clinical data, tumor site, fine-needle aspiration biopsy (FNAB) results, pathologic findings, and TNM classification (sixth ed.) (16) were obtained through review of pathologic, radiologic, and surgical records.
The clinicopathologic features of the 18 patients are summarized in Table 1. Fourteen were men (77.8%) and 4 were women (22.2%). Median age at initial diagnosis was 58 y (range, 39–73 y). Tumors originated from the parotid gland in 11 patients (61.1%), from the submandibular gland in 6 (33.3%), and from the sublingual gland in 1 (5.6%).
Clinicopathologic Characteristics of 18 Patients with SDC
All patients underwent complete surgical resection, including total parotidectomy, total submandibular gland resection, and wide excision for sublingual gland disease depending on the site of the primary tumor. Neck dissection was performed in 16 patients (88.9%). Supraomohyoid neck dissection (levels I–III) was performed in 4 patients (22.2%) with clinically negative involvement of neck nodes. Modified or radical neck dissection at levels I–V (17) was performed in 11 patients (61.1%) with involvement of multiple neck nodes or extracapsular nodal spread, and bilateral neck dissection was performed in 1 patient (5.5%) with bilateral nodal spread. In our institution, neck dissection was recommended for patients with preoperatively diagnosed high-grade tumors of the salivary gland (8): modified radical, radical, or extended radical neck dissection for patients cN-positive and supraomohyoid neck dissection for patients cN-negative. Clinical neck evaluation was performed through physical examination, 18F-FDG PET, and CT before surgery. All patients received postoperative radiotherapy, at a median dose of 60.4 Gy (range, 56–66 Gy), to the tumor bed and ipsilateral neck nodes. Two patients received cisplatin-based concurrent chemoradiation treatment, and 1 patient received preoperative chemotherapy.
Integrated 18F-FDG PET Scans and Contrast-Enhanced CT Scans
18F-FDG PET was performed using an ECAT HR1 scanner (Siemens Medical Solutions USA, Inc.), which provided an axial field view of 15.5 cm. All patients fasted for at least 6 h before 18F-FDG PET, and their blood glucose concentrations were measured; patients with diabetes mellitus were required to have controlled blood glucose levels (<150 ng/mL) before scanning. Each patient received an intravenous injection of approximately 555 MBq of 18F-FDG and rested for at least 1 h before 18F-FDG PET. Sixty minutes after 18F-FDG injection, with the patient supine, whole-body imaging was performed from the head to the mid thigh. Data were reconstructed into coronal, sagittal, and transverse sections and a 3-dimensional rotating projection. Visible lesions with increased tracer uptake were identified, and their 18F-FDG uptake was quantified. The maximum standardized uptake value (SUVmax) was semiquantitatively analyzed according to the equation SUV = A/(ID/LBW), where A is the decay-corrected activity in tissue (in MBq/mL), ID is the injected dose of 18F-FDG (in MBq), and LBW is the patient’s lean body weight.
CT scans (Siemens Medical Solutions) of the head and neck were acquired with a slice thickness of 3–5 mm. Patients were placed supine, and contrast-enhanced axial images were obtained parallel to the occlusal line from the skull base to the upper chest.
Image Interpretation
All imaging findings were retrospectively reviewed. The nuclear medicine physician and radiologist who reviewed the images were aware of the patients’ clinical or FNAB data, which were provided by the referring physician, but unaware of any results of other imaging studies. The nuclear medicine physician had more than 5 years of experience and interpreted the PET images by visual analysis and determination of abnormal 18F-FDG uptake. Abnormal uptake of 18F-FDG was defined as an accumulation outside the normal anatomic structures, or as higher uptake than background activity or asymmetric uptake, which are not normally seen. The radiologist specialized in interpreting the head and neck section of CT scans. CT was evaluated for primary lesions of the salivary gland and regional lymph nodes (18).
Statistical Analysis
The sensitivity, specificity, accuracy, and predictive values of 18F-FDG PET and CT for identifying the extent of neck node involvement at each dissected neck level were evaluated by comparing imaging findings with pathologic nodal stage, with each value calculated using statistical software (version 11.6.1; MedCalc Software). Statistical differences between the imaging modalities were analyzed using the McNemar test. P values of less than 0.05 were considered statistically significant.
RESULTS
Pathologic Features
The median pathologic tumor size was 2.5 cm (range, 1.3–9 cm). Eight patients (44.4%) had pathologic stage T3/T4 tumors, and 10 (55.6%) had pathologic stage T1/T2 tumors. Pathologic nodal involvement was observed in 17 patients (94.4%), with a median 13.0 metastatic nodes (range, 1–68 nodes). Extraparenchymal invasion was observed in 11 patients (61.8%), lymphovascular invasion in 11 (61.1%), and perineural invasion in 7 (38.9%) (Table 1).
Clinical Outcomes
The median follow-up period was 16 mo (range, 4–94 mo). Nodal recurrence was observed in 4 patients (22.2%) at 3–13 mo (median, 8 mo). All nodal metastases developed on the contralateral or undissected ipsilateral neck. There was no neck node failure following postoperative radiation treatment after neck dissection. Distant metastasis developed in 7 patients (38.9%) after a median of 8 mo (range, 3–18 mo), with the most common site being the lungs, followed by the bones and liver. Six patients (33.3%) died of distant failure, whereas 1 (5.6%) with distant metastasis remained alive with stable disease after palliative chemotherapy. At the time of evaluation, 11 patients (61.1%) remained alive with no evidence of disease (Table 1).
18F-FDG PET Findings
Patient characteristics and 18F-FDG PET, CT, and FNAB findings before surgery are summarized in Table 2. FNAB performed on 18 patients correctly classified 18 lesions (100.0%) as malignancies, including 3 (16.7%) diagnosed as SDC, 8 (44.4%) as high-grade carcinoma, 1 (5.5%) as large cell carcinoma, and 1 (5.5%) as low-grade carcinoma, with tumor grade not determined in 5 patients (27.8%).
Each Patient’s Detail
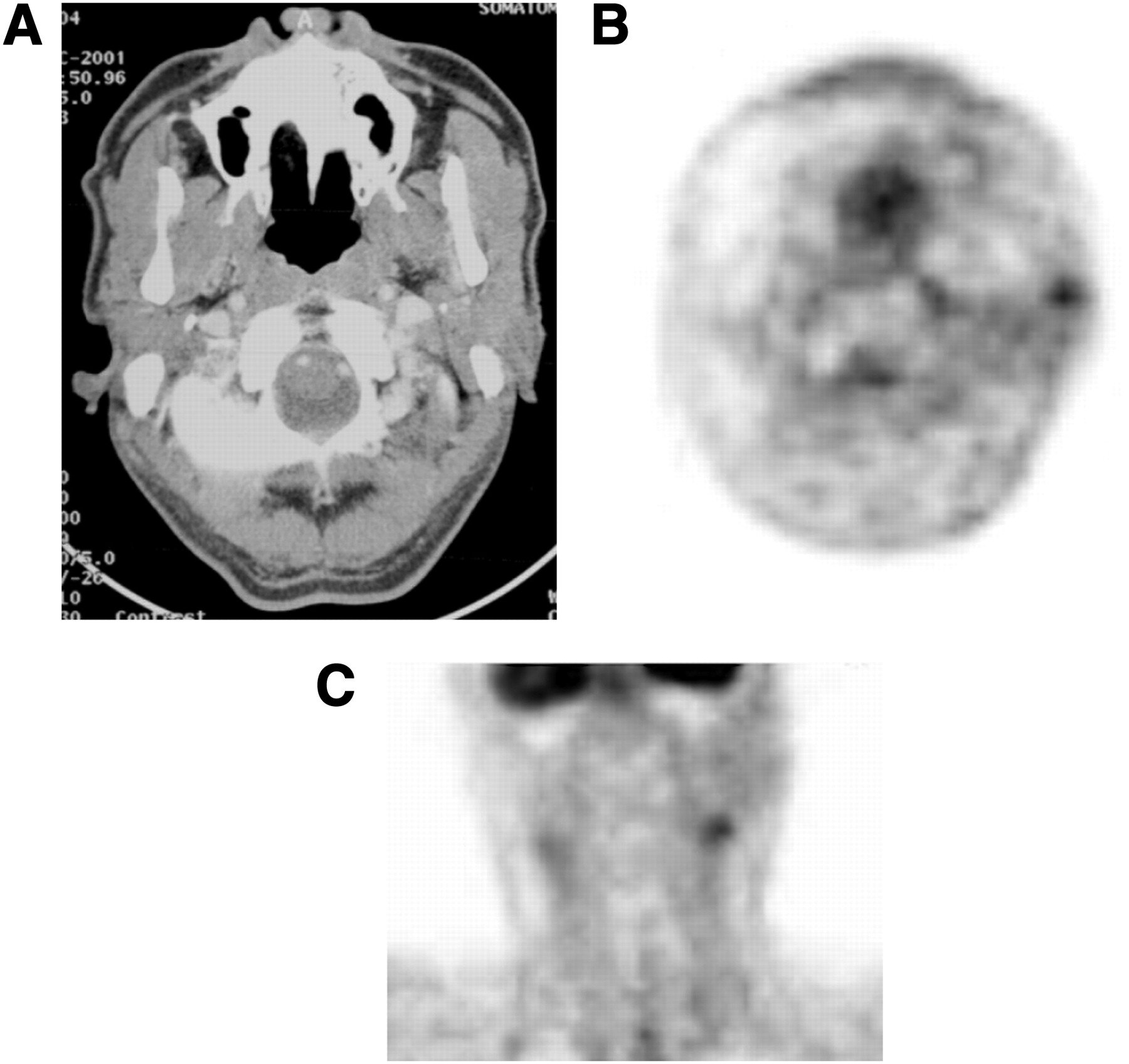
18F-FDG PET identified all 18 primary tumor sites in patients with SDC (Fig. 1). The median SUVmax of the primary lesions was 4.7 (range, 1.8–12.1), and the median SUVmax of the cervical nodes was 5.8 (range, 1.7–13.0). Subsite analysis showed that the median SUVmax of the parotid, submandibular, and sublingual glands was 4.3 (range, 1.8–12), 4.7 (range, 3–12), and 5.9, respectively (Table 3).
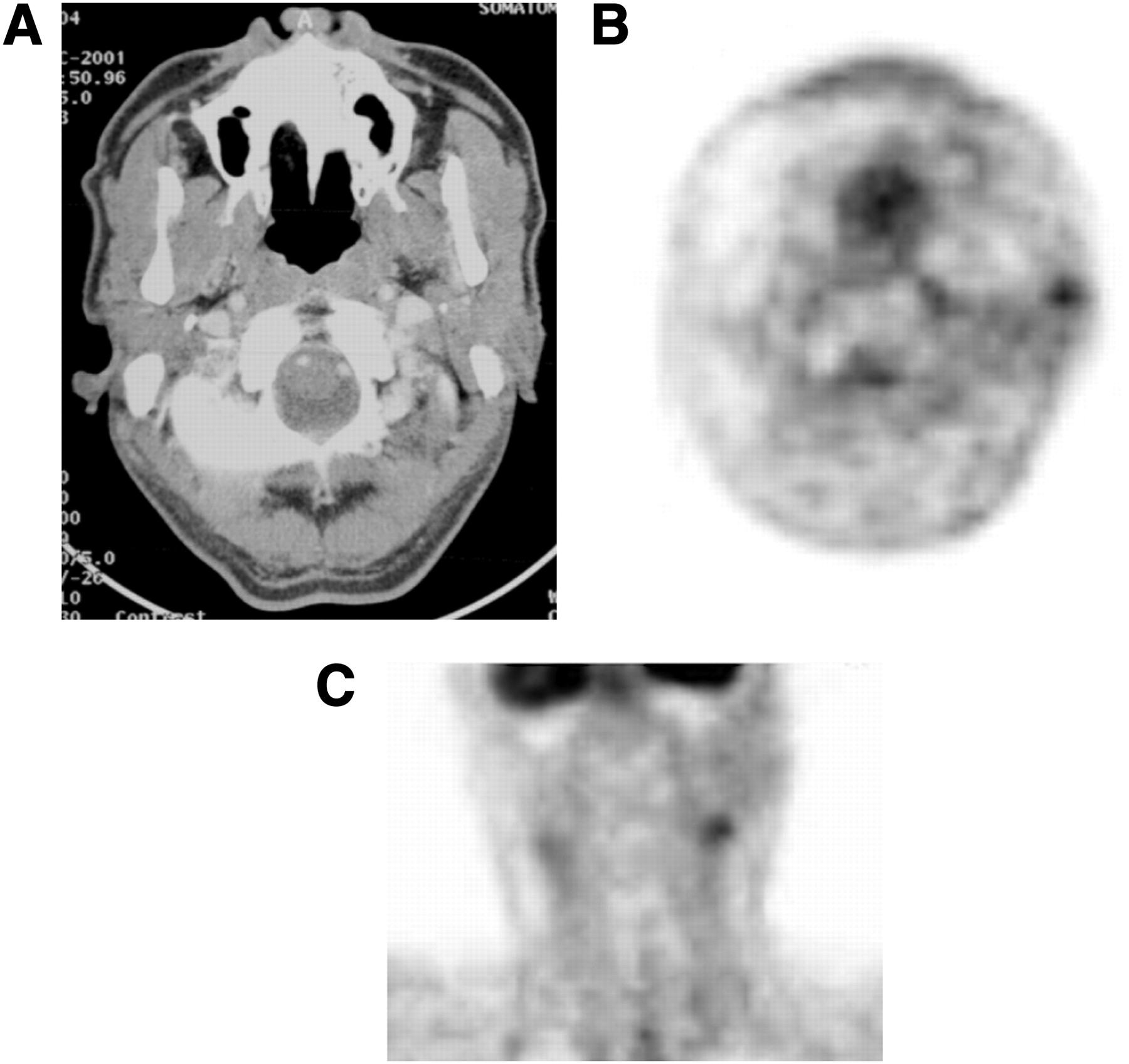
Imaging findings of 65-y-old man with slow-growing mass in left preauricular area. (A) CT image showing no enhancing lesion in left parotid gland. (B and C) 18F-FDG PET image showing focal 18F-FDG uptake by left parotid gland (SUVmax = 2.2) and by left side neck level II (SUVmax = 3.0). Final pathology showed salivary duct carcinoma of parotid gland and level II neck node.
Primary Site and Lymph Node SUV
Cervical lymph nodes were dissected at 73 neck levels, and each neck node was analyzed to determine its diagnostic value (Tables 4 and 5). 18F-FDG PET had a sensitivity of 76.1%, a specificity of 96.3%, a positive predictive value of 97.2%, and a negative predictive value of 70.3%; the corresponding values for CT were 39.1%, 92.6%, 90.9%, and 47.2%, respectively. The sensitivity and negative predictive value were significantly higher for 18F-FDG PET than for CT (P < 0.001 and P = 0.03, respectively).
Analysis of PET and CT for Neck Dissection
Sensitivity, Specificity, and Predictive Values for PET and CT for Neck Dissection
18F-FDG PET determination of extent of neck node involvement led to changes in the elective neck dissection regimen in 5 patients (27.8%): 4 patients (22.2%) from supraomohyoid neck dissection to radical neck dissection and 1 (5.6%) from ipsilateral neck dissection to bilateral neck dissection. In the former 4 patients, 18F-FDG PET showed increased standardized uptake value in multiple ipsilateral neck nodes, whereas CT showed normal findings. Modified or radical neck dissection showed pathologic involvement of multiple levels of neck nodes (Fig. 2). The fifth patient showed increased 18F-FDG uptake by both contralateral and ipsilateral neck nodes, whereas CT showed normal findings in the corresponding contralateral neck nodes. This patient underwent bilateral neck dissection and was found to have N2c disease.

(A) Transaxial 18F-FDG PET image of 62-y-old man with SDC of right parotid gland, showing focal 18F-FDG uptake by right neck level V. (B) CT image showing no significant lymph nodes at same neck level. On basis of results of 18F-FDG PET, type of neck dissection was changed from supraomohyoid to modified or radical. Pathology showed metastatic carcinomas of neck levels I to V.
DISCUSSION
SDC is a rare malignancy, estimated to constitute 1%–3% of all malignant salivary gland tumors (7), which develops predominantly in the parotid glands of elderly men. This malignancy has an aggressive clinical course, with a significant mortality rate of 45%–77% caused by distant dissemination, and frequently presents with lymphatic spread at the time of diagnosis (5,6,19,20). In agreement with previous findings, we observed a high incidence of nodal involvement and a high malignancy-associated death rate in patients with SDC. Management of patients with SDC should therefore be aggressive, including complete surgical resection of the tumor and neck dissection, followed by adjuvant locoregional radiotherapy. Proper management therefore requires accurate information about the primary site and the extent of tumors.
18F-FDG PET has shown greater accuracy than conventional imaging in evaluating patients with head and neck malignancies (21–23), including those with squamous cell carcinomas and lymphomas. 18F-FDG PET is therefore now used for initial staging, management of recurrent cancers, and therapeutic monitoring (9,24,25). In agreement with previous results, we found that adding 18F-FDG PET information to CT was useful in detecting primary tumor sites and in determining the extent of neck node involvement. Because salivary gland malignancies have relatively low 18F-FDG uptake, they can be easily obscured by the normal physiologic uptake of 18F-FDG, with a reported mean SUVmax ranging from 1.87 to 3.20 (23). Generally, in our institution, the mean SUVmax ± SD is lower for salivary gland malignancies (3.8 ± 2.1) than for squamous cell carcinomas of the upper aerodigestive tract (7.5 ± 3.4) (14). In the present study, we also found that the SUVmax of 3 lesions was less than 3.0. These 3 patients, however, showed 18F-FDG uptake by multiple neck nodes or were diagnosed with high-grade carcinoma by FNAB. Therefore, 18F-FDG PET in patients with salivary gland tumors may be more useful in treatment planning than in distinguishing between benign and malignant tumors.
As salivary gland tumors are relatively rare in the head and neck region, only a few studies have assessed the usefulness of 18F-FDG PET or PET/CT in patients with such tumors (9,10,12,14,15,26–28). 18F-FDG PET has shown relatively low accuracy in differentiating malignant from benign disease (9–11,27), especially because of the high SUV of Warthin tumor. However, 18F-FDG PET or PET/CT has been shown useful for initial staging or restaging of salivary gland malignancies (12,14,15,28). In patients with high-grade salivary gland cancers, 18F-FDG PET/CT was found to be highly accurate in predicting the pathologic extent of primary tumors and of neck nodes on a level-by-level basis, with a positive predictive value of 97.6%, compared with 86.0% on CT alone (15). In an examination of 55 salivary gland cancers, 18F-FDG PET had a sensitivity of 74.4% and a specificity of 100% (28). Another study showed that 18F-FDG PET results affected treatment planning in patients with salivary gland malignancies, changing initial treatment planning in 34% of patients and salvage treatment after recurrence in 30% (14). The results presented here are consistent with these previous findings (12,14,15,28) in that our analysis of cervical lymph nodes at 73 neck levels found that 18F-FDG PET had significantly higher sensitivity and negative predictive values than CT. More importantly, the information obtained from 18F-FDG PET had a clinical impact in that it determined the type of neck dissection in 5 patients (27.8%), with pathologic findings in these patients consistent with 18F-FDG PET results.
In the present study, we did not specifically describe the utility of 18F-FDG PET for the follow-up of patients with SDC. However, because the most common pattern of failure is known to be distant metastasis in patients with SDC (8,19,29) and because it often occurs early, follow-up with 18F-FDG PET is likely to be helpful for early detection of distant metastases and for evaluation of treatment response. We usually recommended a follow-up 18F-FDG PET study at 12 wk after postoperative radiation treatment, when locoregional recurrence was found by clinical examination or by follow-up head and neck imaging with CT or MRI, or when follow-up chest radiography or bone scanning showed suggestive abnormalities.
This study had several limitations, including a small number of patients and the fact that 18F-FDG PET was not routinely performed for all patients with SDC during the study period. However, SDC is quite rare, and our use of 18F-FDG PET for staging work-up of 18 patients may provide important information for the management of patients with SDC.
CONCLUSION
We found that 18F-FDG PET was effective for detecting primary sites and the extent of neck node involvement in patients with SDC. This modality may provide useful preoperative information for surgical planning in patients with SDC.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 9, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication September 16, 2011.
- Accepted for publication January 12, 2012.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.