


Abstract
Adult stem cell therapy is expected to improve left ventricular function in patients with myocardial infarction. Because of the low risk of arrhythmia and the maximal concentration at the target tissue, intracoronary infusion of stem cells is preferred. The aim of this study was to investigate the homing and tissue distribution of intracoronary injected peripheral hematopoietic stem cells labeled with 18F-FDG. Methods: Seventeen patients with myocardial infarction were included as the intracoronary injection group (14 males, 3 females; age, 58 ± 12 y). Three patients underwent intravenous stem cell injection as the intravenous injection group (3 males, 0 females; age, 50 ± 20 y). After mobilization with granulocyte colony-stimulating factor (G-CSF), peripheral stem cells were collected by means of apheresis. 18F-FDG labeling of stem cells was performed for 40 min with gentle intermittent mixing at 37°C. The mean labeling efficiency was 72% (range, 46%–95%), and 44.4–175 MBq (1.2–5 mCi) of 18F-FDG-labeled stem cells were injected via an intracoronary catheter after stenting in infarct-related arteries. PET/CT images were obtained with a 3-dimensional acquisition mode 2 h after intracoronary infusion. Results: Two hours after intracoronary infusion, 1.5% (range, 0.2%–3.3%) of injected stem cells accumulated at the infarcted myocardium. Outside of the myocardium, spleen, liver, bladder, and bone marrow showed a high stem cell accumulation. The delayed image of a patient up to 20 h showed a prolonged residence of stem cells at the myocardium. Intravenous injection of stem cells showed a high initial lung uptake with no myocardial activity. Conclusion: We have shown that 18F-FDG-labeled stem cell PET could be used to assess the tissue distribution and to measure the amount of stem cells at a target tissue. 18F-FDG-labeled stem cell PET can be used to measure and optimize the amount of stem cells injected.
Autologous bone marrow stem cell transplantation, using stem cells aspirated from the bone marrow, has been reported to improve myocardial perfusion and cardiac function (1–4). However, peripheral stem cell therapy is a more acceptable method considering its noninvasiveness. Recently, it has been reported that peripheral stem cell therapy could improve cardiac function in patients with myocardial infarction (5).
With regard to the route of administration, intracoronary infusion of stem cells might have an advantage over intravenous injection because of possible maximal delivery to the infarcted myocardium during the first passage of injected stem cells. Furthermore, compared with direct myocardial injection, intracoronary infusion has a low risk of arrhythmia. Because of the high concentration at the target tissue and the low risk of arrhythmia, intracoronary infusion of stem cells was preferred in later studies (2,5,6). Coronary flow blockade after stem cell injection is expected to make stem cells adhere to the myocardial capillaries and to promote cellular migration into the infarcted zone (7).
To evaluate the effect of stem cell therapy, assessments of stem cell homing, distribution, and differentiation are crucial. Despite recent advances in molecular imaging techniques, stem cell tracking using genetically modified cells is still limited in human subjects because of the possible hazard of genetic modification, though unproven. Cell labeling using a radioisotope is an established method in clinical nuclear medicine and has minimal toxicity. Several studies already reported that indium- or technetium-labeled stem cell imaging could be used to monitor the fate of transplanted stem cells (8,9).
PET is an ideal imaging method for stem cell tracking because of its high spatial resolution and high sensitivity. Furthermore, because glucose uptake is a physiologic process, 18F-FDG uptake by stem cells does not require any cellular modification and will occur in vitro in the same manner as in vivo without specific manipulation except for fasting the cells (10,11). Recent preliminary studies indicated that bone marrow stem cells labeled with 18F-FDG could be used to monitor cell homing into the myocardium (11,12). So far, however, the distribution of peripheral stem cells after intracoronary injection has not been elucidated and the usefulness of delayed 18F-FDG PET for the study has not been established. The aim of this study was to evaluate the homing, distribution, and delayed distribution of peripheral stem cells after intracoronary injection of these cells using 18F-FDG-labeled stem cell PET.
MATERIALS AND METHODS
Subjects
We enrolled 17 patients (14 males, 3 females; age, 58 ± 12 y) with an ST-elevated myocardial infarction who were scheduled to undergo elective percutaneous coronary intervention (PCI) and stent implantation at the infarct-related artery. Eleven patients had a history of acute chest pain (<13 d), and 5 had a history of an old myocardial infarction (>90 d) (Table 1).
Patient Characteristics and Percent Activity per Injected Dose at Myocardium
To evaluate the distribution of intravenously injected stem cells, 3 additional patients with acute myocardial infarction were enrolled as the intravenous injection group (3 males, 0 females; age, 50 ± 20 y). The patients in the intravenous injection group also underwent PCI and stent implantation before stem cell injection.
Peripheral Stem Cell Preparation
After successful PCI and stent implantation, granulocyte colony-stimulating factor (G-CSF; Dong-A Pharmaceuticals) was subcutaneously injected at 10 μg/kg body weight for 4 d. Peripheral blood stem cells were obtained using a COBE spectra apheresis system (COBE BCT Inc.) with the mononuclear cell collection method recommended by the manufacturer. Stem cell collection was performed over 60–90 min with an antecubital vein access procedure. The total processing volume of blood ranged from 4,500 to 7,000 mL, and 30–45 mL of apheresis fluid were obtained.
18F-FDG Labeling
A total of 2 mL of apheresis fluid containing ethylenediaminetetraacetic acid (EDTA) as the anticoagulation agent was used for 18F-FDG labeling. Red-blood-cell hemolysis over 30 s was done with 30 mL of distilled water. After 5 min of centrifugation at 1,800 rpm, the pellet containing stem cells was obtained. A total of 175–370 MBq (5–10 mCi) of 18F-FDG in 1 mL of normal saline was mixed with the pellet. Stem cells in this 18F-FDG solution were incubated for 40 min at 37°C with gentle swirling at 5-min intervals. Labeled stem cells were resuspended in 20 mL of normal saline and then centrifuged for 5 min at 1,800 rpm. The labeling efficiency was measured by counting the radioactivity in the pellet and the supernatant. This pellet was resuspended in 1 mL of normal saline and administered immediately by intracoronary injection to the patients. Sixty minutes were required for stem cell labeling procedures.
To examine the stability of 18F-FDG binding, the pellet was incubated with plasma for 3 h. The labeling efficiency after incubation was also measured by counting the radioactivity in the pellet after centrifugation.
For the viability test, labeled stem cells suspended in plasma were stored for 3 h. Cell viability was assessed by trypan blue staining.
Stem Cell Administration and PET/CT Image Acquisition
In the coronary infusion group, 18F-FDG-labeled peripheral stem cells were administered by over-the-wire angioplasty balloon catheter through another coronary catheterization performed 4–5 d after initial PCI. Restoration of TIMI (Thrombolysis in Myocardial Infarction) grade 3 flow and preserved coronary flow reserve measured by coronary Doppler wire were confirmed before stem cell infusion.
In the intravenous injection group, 18F-FDG-labeled stem cells prepared with the same protocol were injected in bolus via a peripheral vein at 4–5 d after PCI.
After 2 h of stem cell injection, whole-body PET images were acquired with the conventional 3-dimensional protocol of 18F-FDG PET using a Gemini PET/CT camera (Philips). Low-dose CT (120 kV, 50 mA) from head to pelvis was acquired for attenuation correction and anatomic localization. Emission PET images were acquired for 2 min 30 s per each bed with a 3-dimensional acquisition mode.
To examine the delayed distribution, an additional 4-h image was acquired in 2 patients and 4- and 20-h images were acquired in another patient.
Dosimetry
Transaxial images from 2- and 4-h acquisitions of a patient were analyzed. A region of interest was drawn manually on transaxial images on the bone marrow, myocardium, liver, spleen, and bladder. The half-life and residence time were calculated for each organ from the time–activity curves of these organs. MIRDOSE3.1 was used to calculate radiation exposure (Oak Ridge Associated University, Oak Ridge, TN).
RESULTS
Stem Cell Labeling with 18F-FDG
Two milliliters of apheresis fluid rich in mononuclear cells were used for 18F-FDG labeling. The mononuclear cell fraction was 84.3% and the remaining cells were primarily neutrophils and their precursor cells. An initial experiment indicated that the best labeling efficiency was acquired with an EDTA-containing sample. The same samples from 1 patient showed different labeling efficiencies: 96% in EDTA, 62% in heparin, and 56% in acid–citrate–dextrose (ACD). Therefore, subsequent samples were treated with EDTA for anticoagulation.
The overall labeling efficiency was 73% ± 17% with EDTA. Finally, 136.9 ± 64.8 MBq (3.7 ± 1.75 mCi) of 18F-FDG-labeled stem cells were prepared. The injected activity of stem cells is presented in Table 1. The heparin-containing sample frequently showed cell aggregation and caused labeling failure. ACD also showed a low labeling efficiency, which was thought to be related to the glucose contained in ACD.
Stability and Viability Test
18F-FDG-labeled stem cells were incubated in plasma for 3 h and resuspended with normal saline. The radioactivity of the stem cell-containing pellet was ≥90%.
For viability assessment, microscopic examination was done on 18F-FDG-labeled stem cells after 3 h of incubation in plasma. Microscopic examination revealed that there were few trypan blue–defective stem cells (Fig. 1).

Trypan blue staining of 18F-FDG-labeled stem cells. There were few trypan blue–defective cells.
Distribution of Stem Cells After Intracoronary Injection
18F-FDG-labeled stem cell PET images were acquired in 17 patients in the intracoronary injection group and in 3 in the intravenous injection group without complication during the injection period (Table 1). A total of 4.5 × 108 leukocytes (8.3% ± 10.2% CD34+ cells) labeled with 18F-FDG was injected.
PET images were acquired after 2 h of stem cell injection. 18F-FDG-labeled stem cells showed physiologic distribution predominantly within the reticuloendothelial system (Figs. 2 and 3). Liver, spleen, and bone marrow showed prominent stem cell uptake. Brain and bladder activity of stem cell imaging were markedly lower than that of the pure 18F-FDG PET image (Table 2).

PET/CT images of 65-y-old man with history of anterior wall infarction. After percutaneous intervention, 18F-FDG-labeled stem cells were injected via intracoronary catheter. PET/CT images were obtained 2 h after injection. Stem cell accumulation at myocardium is well visualized (arrow). Total amount of stem cells at myocardium was 2.1% of injected dose (case 1 of Table 1).

PET/CT image of 30-y-old man with inferior wall infarction (case 2 of Table 1). Total amount of stem cells at myocardium (arrow) was 2.7% of injected dose.
Percent Activity of Intracoronary Injected Stem Cells at 2 Hours After Injection
There was no significant difference in the stem cell amount at the myocardium according to the age of infarction (1.6 ± 0.88 vs.1.48 ± 0.79; P = 0.78, in acute myocardial infarction and old myocardial infarction, respectively).
No correlation was found between the CK-MB (creatine kinase isoenzyme containing M and B subunits) level and stem cell activity at the myocardium (P = 0.372).
Stem Cell Quantification at Myocardium and Changes in Delayed Periods
Stem cell activity was found on myocardium within the territories of infarct-related arteries injected. The calculated amount on myocardium was 1.5% ± 0.8% of injected dose. It ranged from 0.2% to 3.3%. To evaluate the change of tissue distribution and homing at the myocardium, 4-h and 20-h delayed images were acquired in 2 subjects and 1 subject, respectively (Tables 3 and 4). Myocardial uptake persisted until 4-h delayed images and even remained until 20-h delayed images (Figs. 4A and 4B).

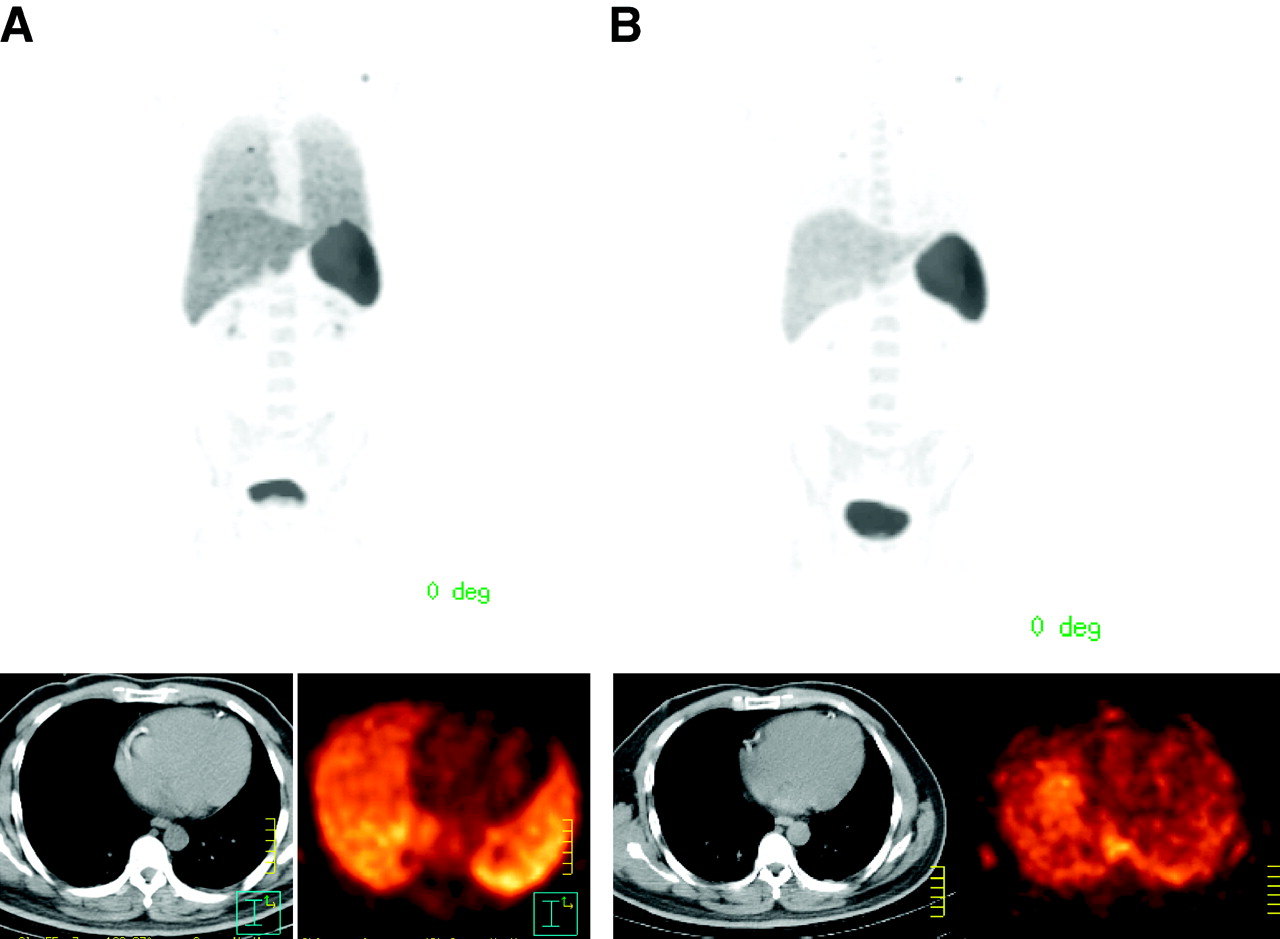
Distribution of stem cells after intracoronary injection at 24 h (A, case 3 of Table 1) and at 2–20 h (B, case 4 of Table 1). Stem cell activity (arrow) remained on 4-h image, and splenic uptake was prominent. Myocardial uptake could be noted on CT-guided anatomic localization on 20-h image.
Distribution of Intracoronary Injected Stem Cells Measured at 2 and 4 Hours After Injection
Distribution of Intracoronary Injected Stem Cells Measured at 2 and 20 Hours
Distribution of Stem Cells After Intravenous Injection
After intravenous injection of 18F-FDG-labeled stem cells, there was no stem cell activity within the myocardium. The whole-body distribution of stem cells after intravenous injection was similar to that of intracoronary injection except for the initial high lung uptake (Table 5). The reticuloendothelial system took up most of the stem cells after intravenous injection. Initial high lung uptake on the 30-min image was cleared away and splenic uptake increased on the 2-h delayed image (Fig. 5).

PET/CT images of 39-y-old male patient with anterior wall infarction (case 18 of Table 1). Stem cells were injected intravenously, and PET/CT images were acquired at 30 min (A) and at 2 h (B). Initial high lung uptake was observed at 30 min and cleared on 2-h image. No myocardial uptake was evident on both images.
Distribution of Intravenously Injected Stem Cells Measured at 2 and 4 Hours
Dosimetry
Similar to white blood cell images, 18F-FDG-labeled stem cell uptake occurred primarily in the reticuloendothelial system. The radiation dose to the myocardium was calculated to be 0.017 mGy/MBq (0.064 rad/mCi) (Table 6).
Radiation Dose of Intracoronary Injected 18F-FDG-Labeled Stem Cells
DISCUSSION
This study demonstrated that 18F-FDG-labeled stem cell PET was feasible to assess stem cell homing and distribution. Stem cell imaging with PET could evaluate the amount of stem cells at the myocardium quantitatively and might be used to assess the adequacy of stem cell injection to the target tissue.
We successfully labeled peripheral stem cells supplied by apheresis with 18F-FDG. Among the different labeling methods available in nuclear medicine, 18F-FDG labeling and imaging with PET had the advantages of high resolution, adequate attenuation correction, and easy accessibility. Stem cells physiologically take up 18F-FDG at adequate temperature and 18F-FDG concentration, resulting in the high labeling efficiency reported in this study. The only requirement was the fasting of the stem cells. Stem cells were believed to undergo minimal damage during the labeling procedures and could preserve migration or proliferation ability. Trypan blue staining showed that stem cell viability was preserved in plasma even 1 h after 18F-FDG labeling. Because only viable cells could contain 18F-FDG in its cytoplasm, the amount of 18F-FDG-labeled cells might mean the viability of the cells. Because of these theoretic advantages, in vivo imaging with 18F-FDG labeling of stem cells was already recommended to track stem cells in animal and human studies (12,13).
Selective intracoronay injection was thought to deliver a maximum concentration of cells homogenously to the injured myocardium during the cells' first passage. This belief was confirmed on 18F-FDG-labeled stem cell PET. The amount of stem cells retained at the myocardium after intracoronary injection was 1.5% on average 2 h after injection in this study. This result is consistent with the amount of bone marrow stem cells injected by the intracoronary route but collected directly by the bone marrow aspiration (12). We demonstrated that intracoronary injected peripheral stem cells also showed substantial homing at the myocardium. Now, the size of stem cells, acquisition time after injection, and method of injection may affect the results, and further comparison studies are needed to determine which cell types are homing better at the target tissue.
The empiric dose of autologous bone marrow to achieve the therapeutic effect was 10–40 × 106 cells in human studies (13). Considering the various sizes of the infracted myocardium and the variable amount of resident stem cells after intracoronary injection, further studies are, of course, warranted to determine the optimal dose of stem cells. Quantification of stem cells at target tissue will be a prerequisite to assess the actual dose of stem cells at the target tissue and to establish an optimal procedure of stem cell therapy. For this purpose, 18F-FDG-labeled stem cell PET has the advantages of high sensitivity and established quantification methodology.
We acquired a 20-h delay image with the 3D acquisition method to determine whether stem cells would remain at damaged myocardium for a substantial time. Because of the short half-life of 18F, counts for the 20-h delayed image quality were not as good as those of 4-h image. However, with the help of CT-guided localization, we could identify remaining stem cell activity at the injured myocardium (Fig. 4). Because of the poor quality and short half-life of 18F-FDG, the 20-h image should not be a routine procedure for evaluating stem cell distribution.
Radiation exposure by 18F-FDG-labeled stem cell imaging might be another obstacle for a routine use of stem cell tracking methods. The radiation dose of 18F-FDG PET calculated in this study was similar to that of 18F-FDG-labeled white blood cell imaging (14). As high radiation exposure to stem cells may cause functional impairment, the imaging method with a minimal dose to stem cells is necessary. Although functional evaluation of stem cells after 18F-FDG labeling was not performed in this study, radiation exposure to stem cells was thought to be permissive according to our dosimetry results compared with indium or technetium labeling.
Intravenously injected stem cells showed high lung uptake on the initial 30-min image and rapid clearance after 2 h. Splenic uptake markedly increased on the 4-h delayed image. As was expected, the amount of stem cells at the myocardium was minimal in the intravenous injection group, and PET images of the myocardium yielded almost the background activity. Initial high lung uptake indicates that intravenous injection of stem cells might represent impediments of these cells in their lung passage. Considering this fact, intravenous injection of stem cells may be an inappropriate method because of the very low concentration of stem cells, if any, at the target tissue.
Although coronary vessel patency was confirmed by angiography before stem cell infusion, several patients showed minimal delivery of stem cells in injured myocardium. The age, acute or chronic status, vascular resistance after PCI, and adequacy of infusion procedure might influence the amount of stem cells at the myocardium. The degree of functional improvement after stem cell therapy is expected to have a correlation with the amount of stem cells at the myocardium, and further study is underway.
111In-Indium oxine or 99mTc-hexamethylpropyleneamine oxime (99mTc-HMPAO) has been widely accepted as an in vivo cell-tracking method. Hematopoetic stem cells and mesenchymal stem cells were successfully labeled with indium oxine or 99mTc-HMPAO in animal studies (8,9,15,16). Although indium oxine imaging has the advantage of delayed imaging because of its longer half-life, poor resolution and higher radiation exposure might limit human application.
CONCLUSION
Stem cell PET with the 18F-FDG labeling method is feasible in human subjects with minimal risk. 18F-FDG-labeled stem cell imaging could be used to evaluate stem cell homing and distribution during the early phase in patients who undergo stem cell therapy. Information on stem cell homing and distribution in human trials might be used to predict the effect of stem cell therapy in terms of optimal stem cell dose calculation and development of adequate administration methods.
Acknowledgments
This study was supported by a grant (SC3070) from the Stem Cell Research Center of the 21st Century Frontier Research Program funded by the Ministry of Science and Technology, Republic of Korea, and by a grant from the Clinical Research Center for Ischemic Heart Disease, Ministry of Health and Welfare (0412-CR02-0704-0001).
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 19, 2006.
- Accepted for publication April 26, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Shattering barriers toward clinically meaningful MSC therapies
- Is There a Role for Intravenous Stem Cell Delivery in Nonischemic Cardiomyopathy?
- Optimized Delivery System Achieves Enhanced Endomyocardial Stem Cell Retention
- Cellular Encapsulation Enhances Cardiac Repair
- 18F-FDG Labeling of Mesenchymal Stem Cells and Multipotent Adult Progenitor Cells for PET Imaging: Effects on Ultrastructure and Differentiation Capacity
- Cardiovascular Molecular Imaging: Focus on Clinical Translation
- Assessment and Optimization of Cell Engraftment After Transplantation Into the Heart
- Priming With Angiopoietin-1 Augments the Vasculogenic Potential of the Peripheral Blood Stem Cells Mobilized With Granulocyte Colony-Stimulating Factor Through a Novel Tie2/Ets-1 Pathway
- Collagen-Based Matrices Improve the Delivery of Transplanted Circulating Progenitor Cells: Development and Demonstration by Ex Vivo Radionuclide Cell Labeling and In Vivo Tracking With Positron-Emission Tomography
- Dynamic Tracking During Intracoronary Injection of 18F-FDG-Labeled Progenitor Cell Therapy for Acute Myocardial Infarction