


Abstract
Detection of vulnerable plaques before rupture is important in preventing acute coronary events such as myocardial infarction. Although therapeutic strategies such as percutaneous transluminal coronary angioplasty appear to prevent coronary occlusion and consequently may lead to improved prognosis in these patients, a method of detecting vulnerable plaques has not been established. A nuclear method that uses an intravascular radiation detector (IVRD) with the plaque-avid tracer 18F-FDG is one of the most promising methods. The catheter-based IVRD consists of a catheter probe (a scintillator and flexible optic fibers), photomultipliers, a controller, and an automatic pullback unit and personal computer. A phantom study demonstrated that this detector was highly sensitive to 18F and enabled the detection of 18F point sources. However, details of the detection system in vivo remain unclear. Methods: To evaluate vulnerable plaques in vivo, we investigated a canine femoral artery and coronary artery using this detector system. Our goal was to estimate the ability of this device to navigate through these arteries and to detect 18F point sources fixed on their adventitia. Results: In the study using a canine femoral artery, the IVRD could detect the point sources with good repeatability. In the study using an open-chest canine model, the catheter probe could easily be advanced into the left descending coronary artery, and the IVRD could detect target sources attached externally to the coronary artery (7- to 15-mm intervals) with good resolution. Conclusion: This newly developed catheter-based IVRD was able to detect, with good resolution, the slight radioactivity from 18F point sources attached to the femoral artery and the coronary adventitia. These results show that catheter-based detection of coronary vulnerable plaques may be feasible.
Acute coronary syndrome is caused by rupture of vulnerable plaques, mostly at the site of mild-to-moderate stenosis of lipid-rich lesions, which often are not visible angiographically (1,2). Therefore, it would be valuable to be able to detect them, through imaging, before a clinical event. Major factors that determine the vulnerability of coronary plaques are the size and lack of consistency of the atheromatous core, the thickness of the fibrous cap, and the presence of inflammation within the cap. Inflammation is important in both the pathogenesis and the outcome of atherosclerosis. Plaques containing numerous inflammatory cells, particularly macrophages, have a high risk of rupture, whereas those with few inflammatory cells are at lower risk. 18F-FDG is a glucose analog that can be used to image inflammatory cell activity (3) and is commercially available in both the United States and Japan.
Vulnerable plaques can be detected through various imaging techniques such as intravascular ultrasound, MRI (angiography), and thermography (4–6). However, few striking results have been reported. In addition, because of body attenuation and partial-volume effects, external techniques using various radiopharmaceuticals are critically limited in the detection of small plaques.
In a previous study, we developed a catheter-based intravascular radiation detector (IVRD) as an endovascular device for the detection of small plaques (7). This device consists of a probe, an automatic pullback unit, and a controller. The probe, which consists of a scintillator and flexible optical fibers, is 1.0 mm in outer diameter—advantageous in navigating coronary artery and stenotic vessels. Because of background radioactivity from the blood pool, heart, and other organs, radiopharmaceuticals that emit short-range charged particles rather than γ-rays are thought to be suited for endovascular detection of small coronary plaques. Therefore, we selected a plastic scintillator for the detection of charged particles. The performance characteristics of the device were assessed with 18F point sources because 18F is a clinically useful charged-particle emitter (positron emitter) and because uptake of 18F-FDG is increased in unstable plaques (8). A phantom study demonstrated that this detector was highly sensitive to 18F and enabled the detection of 18F point sources in the presence of intense background radioactivity (7). However, the details of this detector in vivo remain unclear. In this study, we investigated the ability of this device to navigate through a canine femoral and coronary artery and to detect point sources fixed on their adventitia.
MATERIALS AND METHODS
Radiochemicals
18F-FDG was synthesized by the nucleophilic substitution method with an 18F-FDG–synthesizing instrument (F-100; Sumitomo Heavy Industries, Co. Ltd.) and a cyclotron (CYPRIS-325R; Sumitomo Heavy Industries) in Kyoto University Hospital.
Detector System
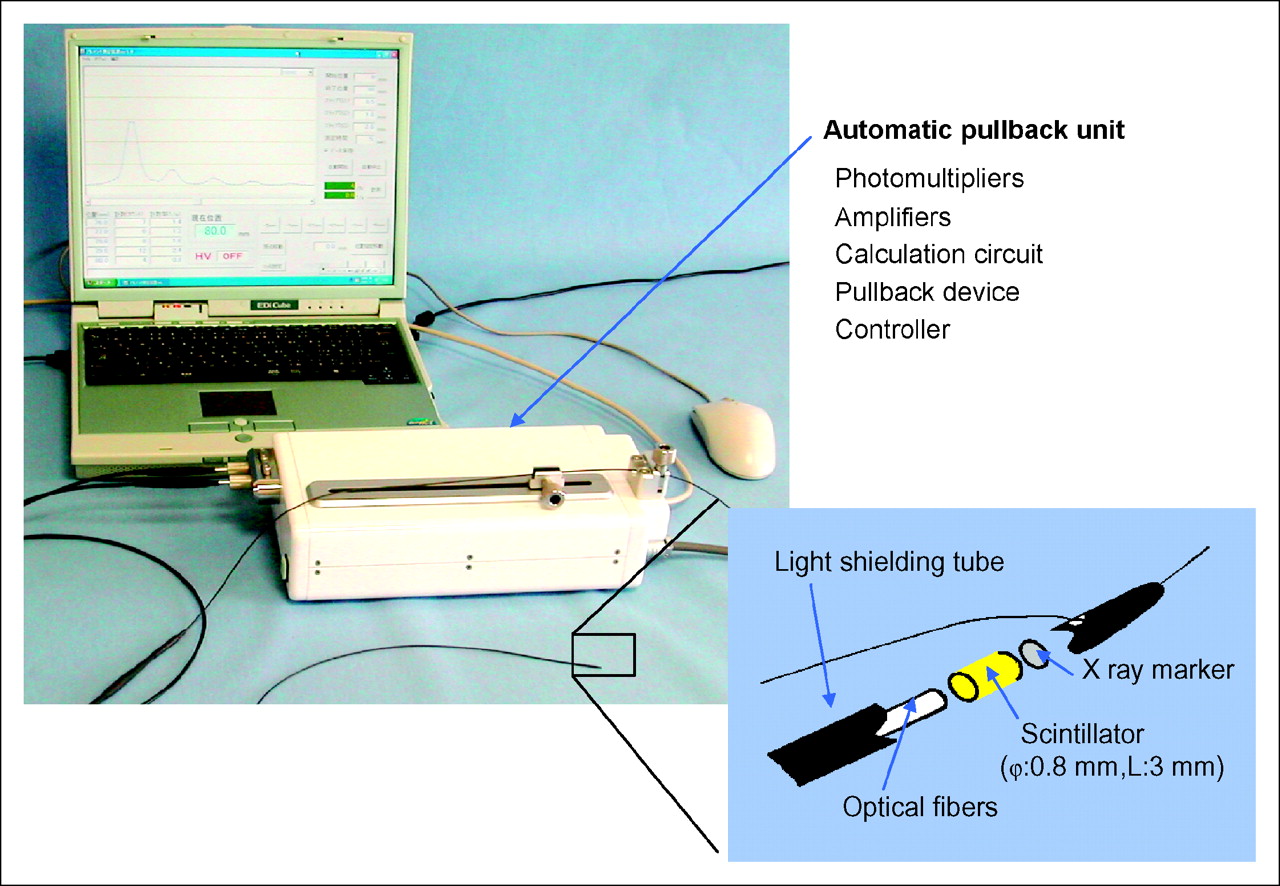
The probe consists of a piece of BC-408 plastic scintillator (Bicron Corp.) formed into a cylinder 0.8 mm in diameter by 3.0 or 5.0 mm in length and a light guide 0.8 mm in diameter by 3.0 m in length (Fig. 1). The outer diameter of the probe is 1.0 mm, because it is covered with a black tube 0.1 mm thick to block light. The light guide, which consists of more than a hundred glass fibers, is divided into 2 equal bundles and connected to 2 photomultiplier tubes (Hamamatsu Photonics) (7). The tubes were operated at voltages of 1,000 V supplied by a high-voltage power supply (C4900; Hamamatsu Photonics). Anode voltage pulses from each photomultiplier were amplified with an SDA01 amplifier (SD Giken, Co. Ltd.) before discrimination by an SDD01 discriminator (SD Giken) with the energy threshold set at 0.1 V. Signals from each discriminator are fed to a coincidence module (SDAD01; SD Giken). The coincidence signals are counted, stored, and processed with a microcomputer-equipped controller. The controller also directs an automatic pullback unit and records the pullback length.
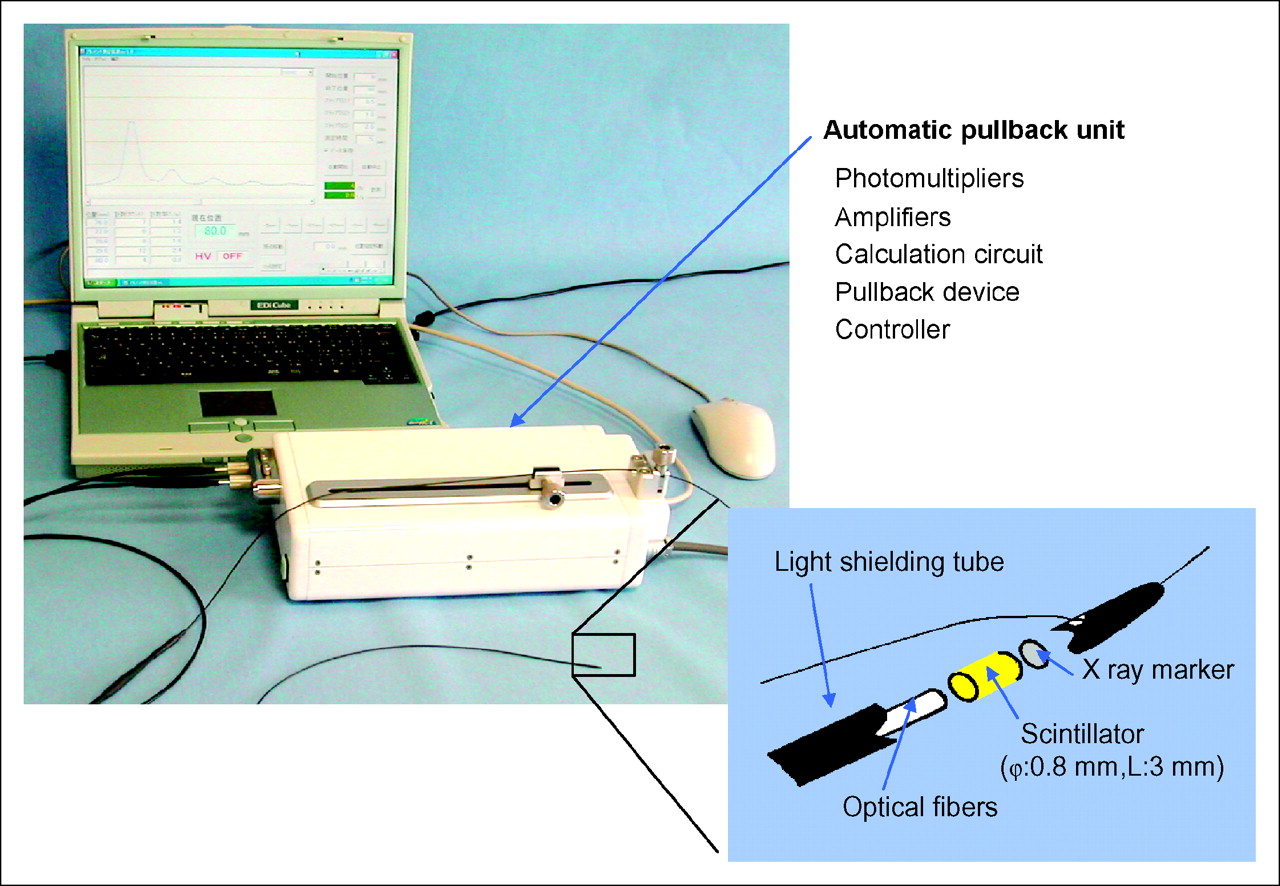
Photograph of IVRD system and schematic figure of catheter probe.
Experiments on Canine Femoral Artery
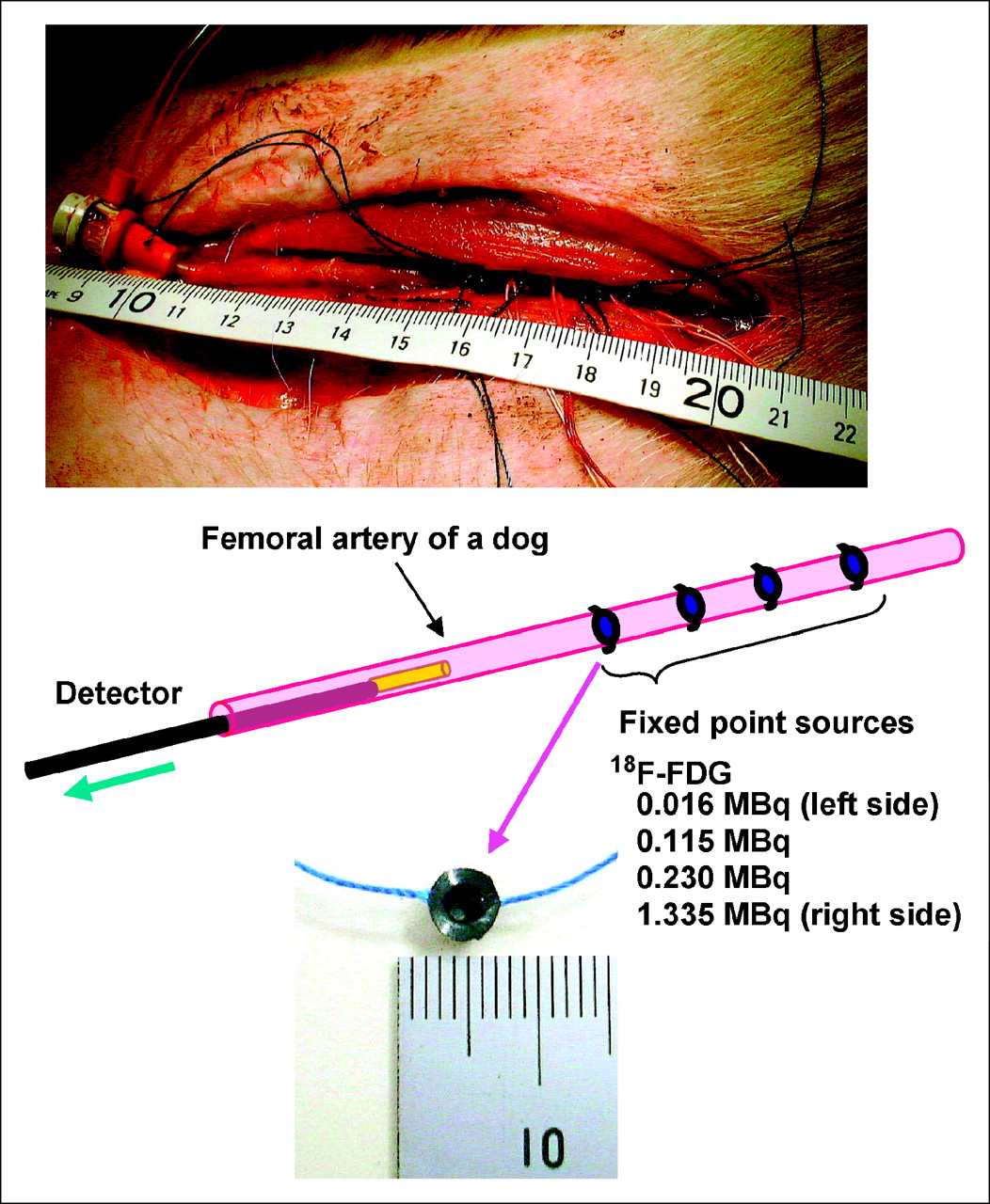
Animal studies were conducted in accordance with our institutional guidelines and were approved by the Kyoto University Animal Care Committee. A 19-kg male dog (HBD; Kitayama Labs Co., Ltd.) was housed in a cage in an air-conditioned room and maintained on a standard diet and water ad libitum. The dog was anesthetized with sodium pentobarbital (Dainippon Pharmaceutical Co., Ltd.), and an incision about 10 cm long was made in the area of its femoral artery. Four point sources 2.2 mm in diameter by 1.5 mm thick and containing 16, 115, 230, or 1,335 kBq of 18F-FDG were made with a polyvinyl chloride cap and polypropylene film and were fixed on the surface of the femoral artery with threads (Fig. 2). The point sources were spaced at 7- to 15-mm intervals. The IVRD probe equipped for a 5-mm-long scintillator was introduced and deployed through a 4-French sheath (Cordis Corp.). Counts were recorded for 5 s at each position as the probe was pulled out. We measured twice to determine reproducibility.
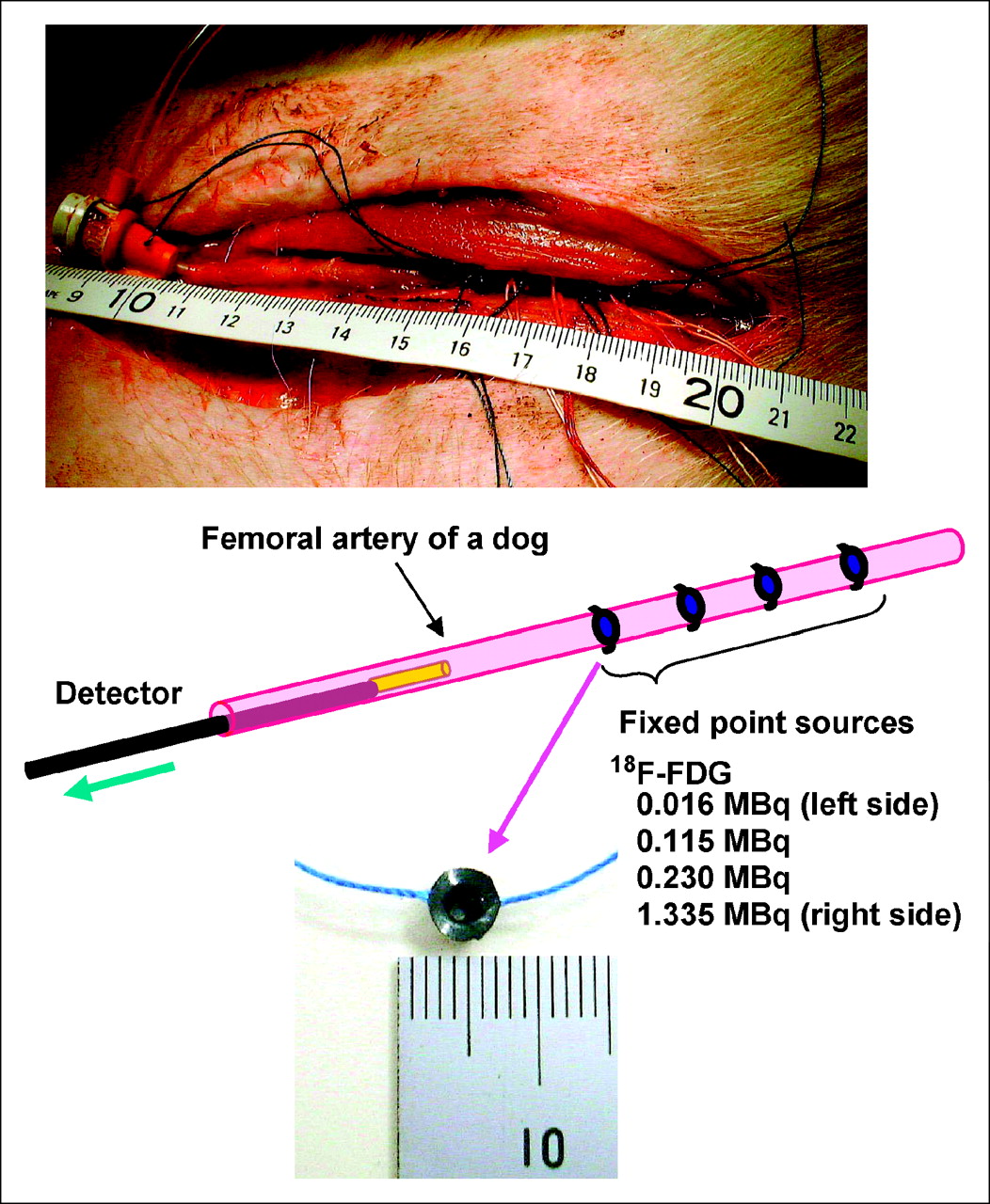
Surgical photograph and study schema for canine femoral artery. Four 18F-FDG point sources were fixed on surface of artery.
Experiments on Canine Coronary Artery
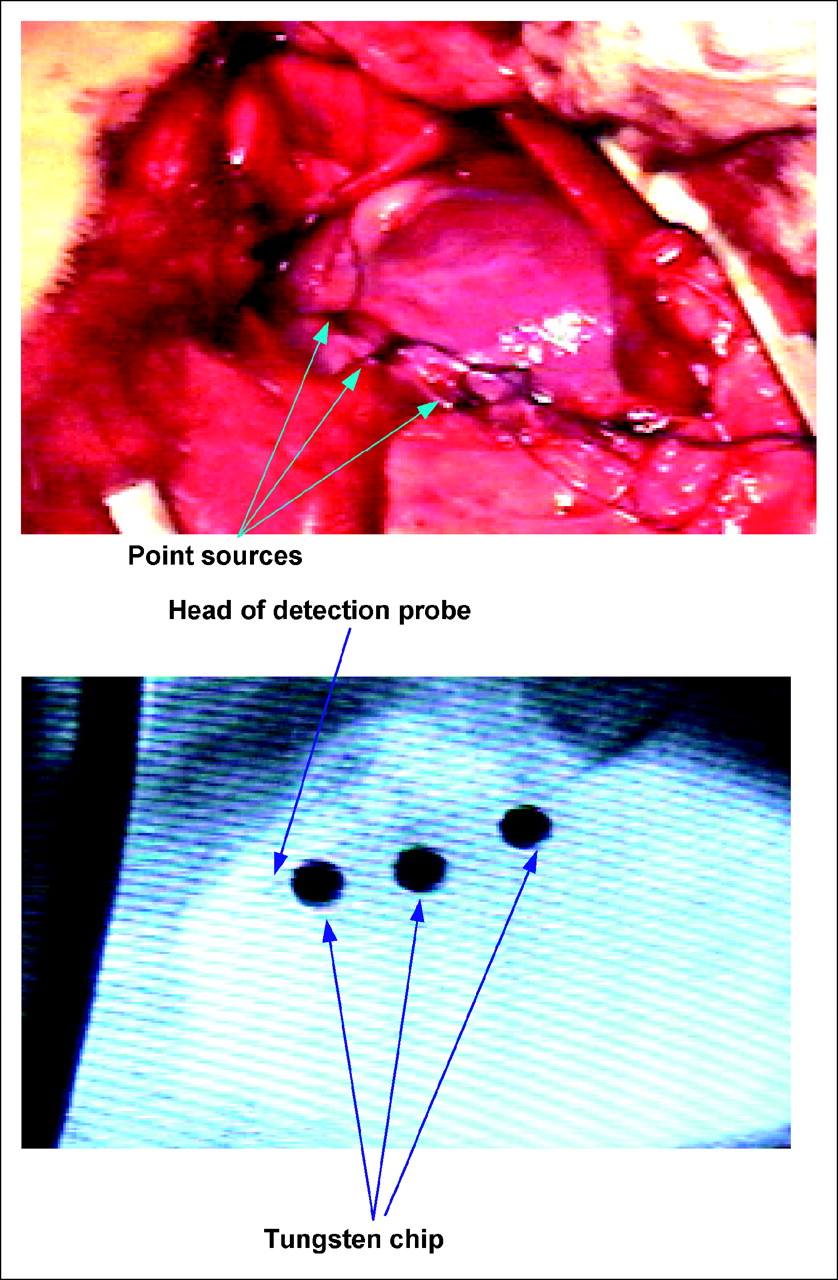
Another male dog, weighing 18 kg, was prepared in the same manner but on a different day, and an incision about 15 cm long was made on the left side of the dog's chest. Three point sources 2.2 mm in diameter by 1.5 mm thick and containing 66, 330, or 1,019 kBq of 18F-FDG were made with a polyvinyl chloride cap and polypropylene film and were fixed on the surface of the left descending coronary artery with threads (Fig. 3). Tungsten chips were also fixed on the coronary artery near the point sources for the radiograph. The radiation markers were about 10, 20, and 35 mm from the orifice of the left descending coronary artery in order of radioactivity (low-energy marker was most proximal). A guidewire was inserted into the left carotid artery through a 6-French sheath using an introducer, as is common in percutaneous coronary interventions. Afterward, a 6-French guiding catheter (Cordis Corp.) was introduced using the guidewire and was brought into the orifice of the left coronary artery. Finally, the IVRD catheter was easily drawn into the left descending coronary artery using the guiding catheter. These procedures and the positioning of the IVRD probe in the heart vessels were verified through fluoroscopy.
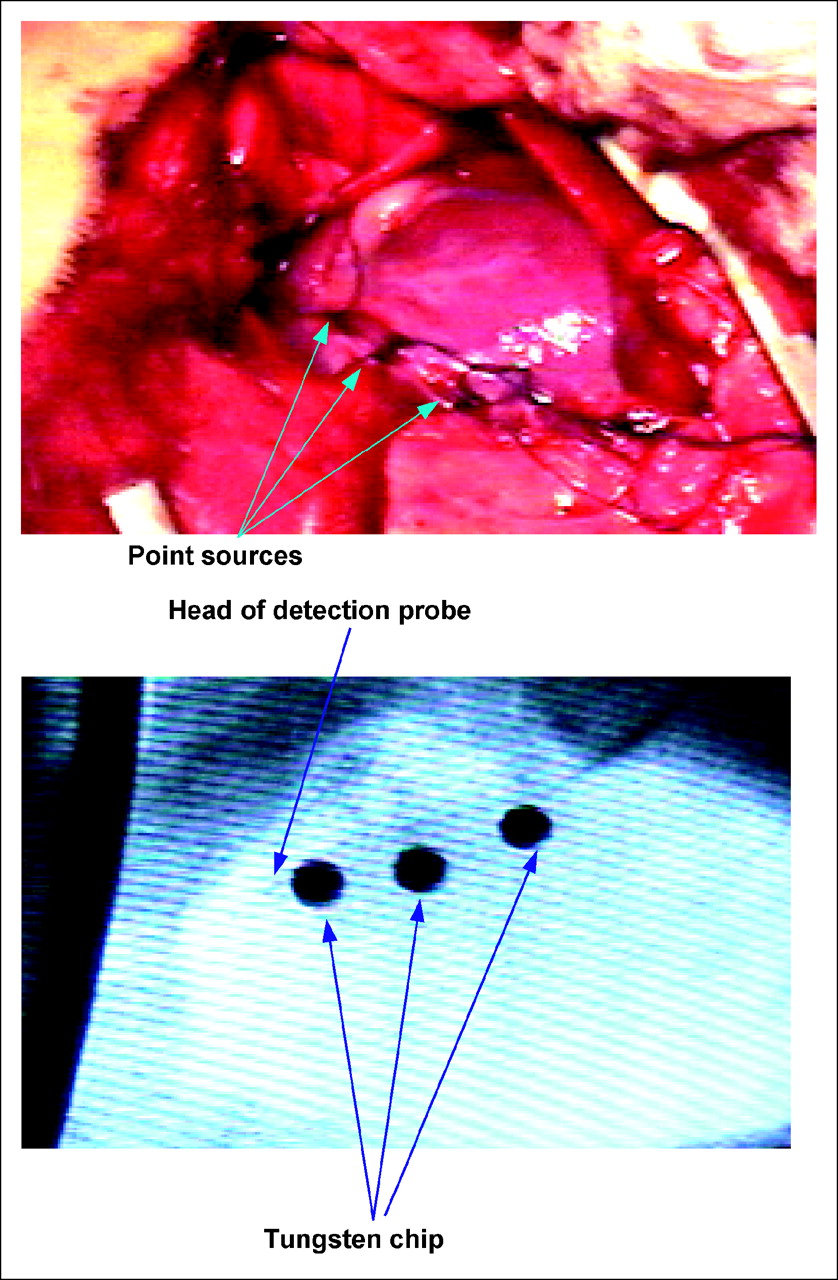
Surgical photograph (top) and radiograph (bottom) of canine heart. Three 18F-FDG point sources (66, 330, and 1,019 kBq) were fixed on surface of left descending coronary artery. Three tungsten chips for the radiograph were placed near the point sources. IVRD head was in distal portion of coronary artery. Point sources were fixed on surface of proximal side.
Counts were recorded for 5 s at each position as the probe was pulled out. We measured twice to determine reproducibility.
RESULTS
Experiments on Canine Femoral Artery
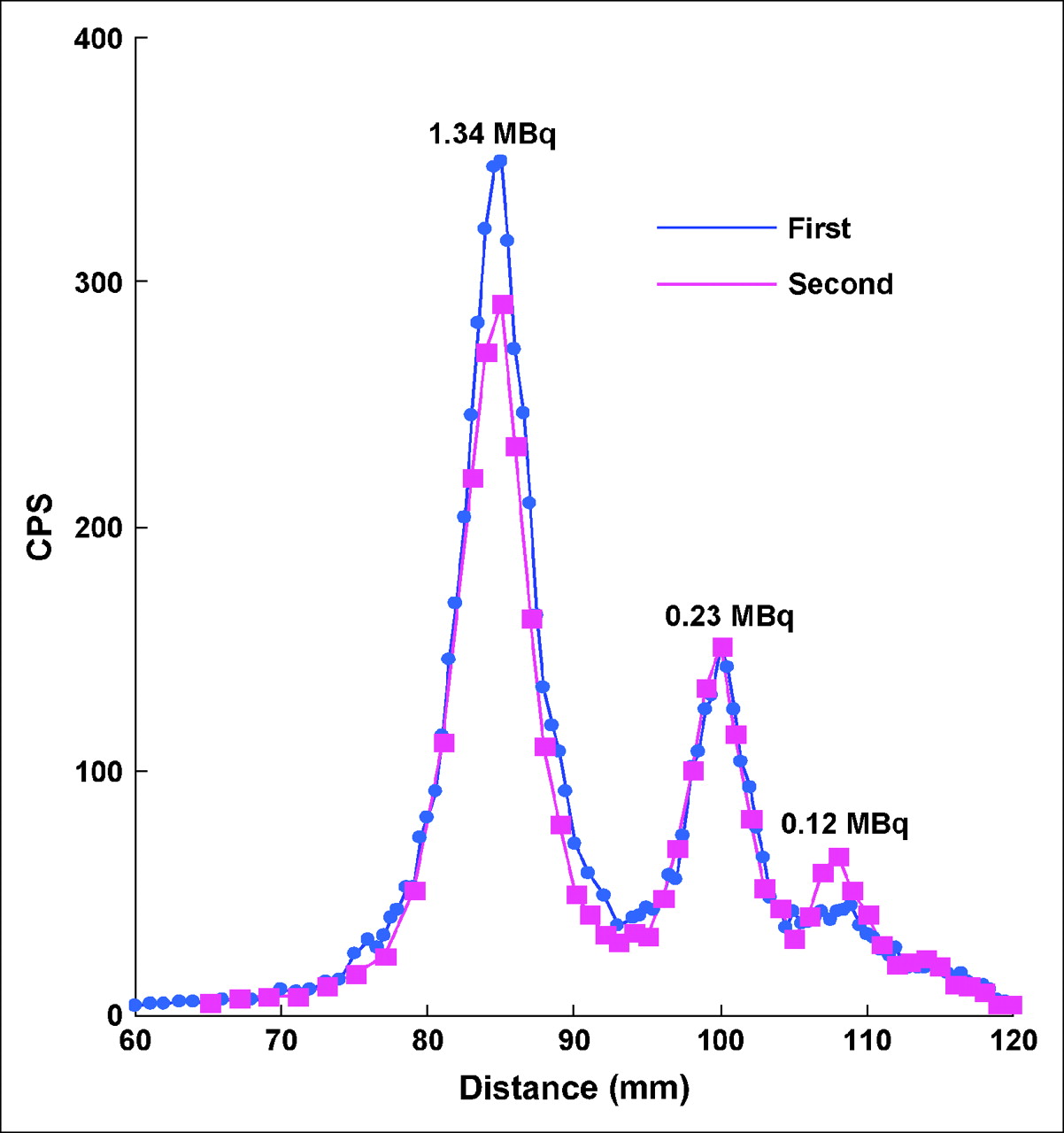
Figure 4 shows the data of 18F point sources detected by the IVRD probe. Three of the point sources (115, 230, and 1,335 kBq) fixed on the surface of the canine femoral artery were detected as relatively broad peaks, although the radioactivity peak of the 16-kBq point source was not clearly displayed.
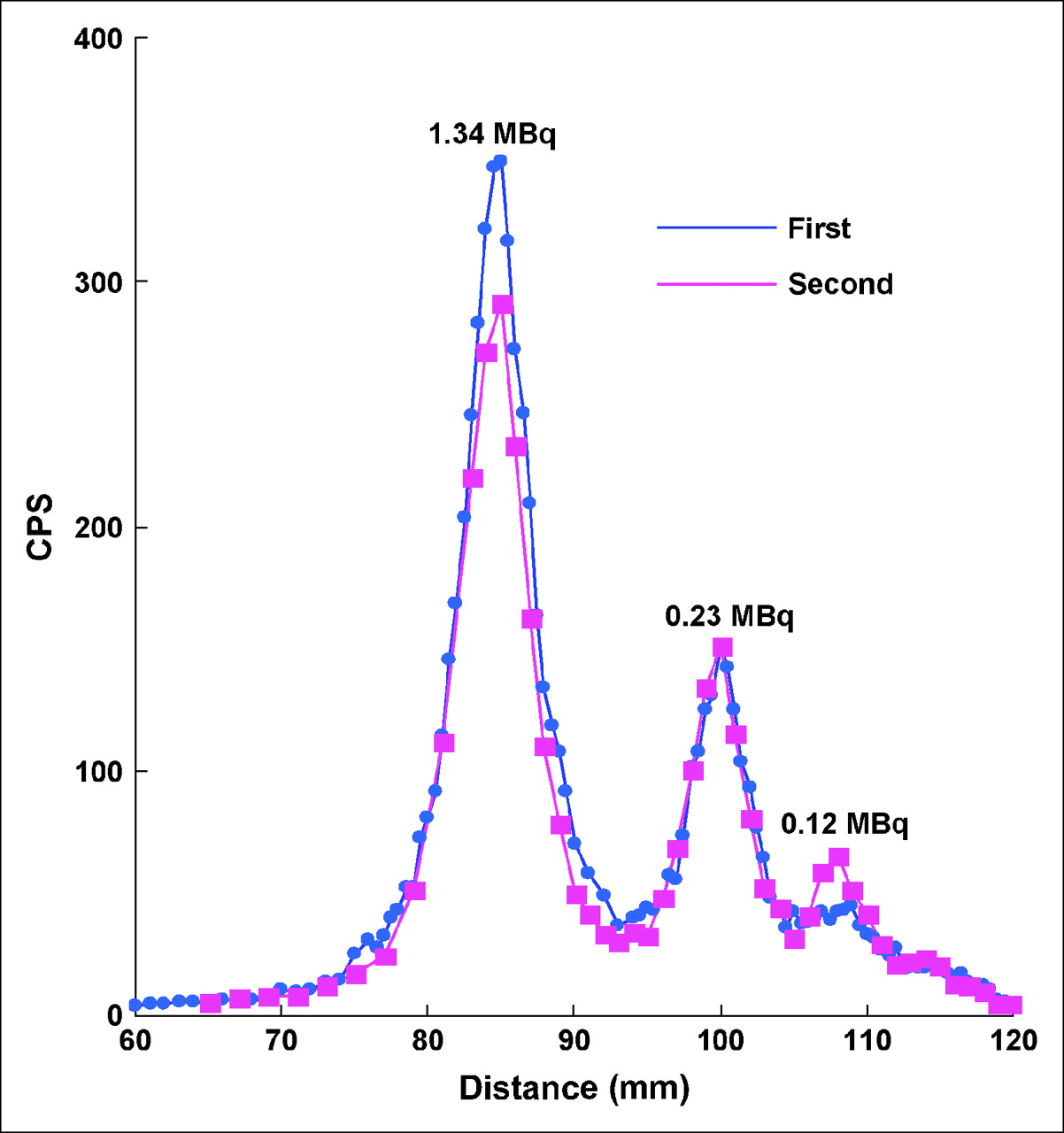
Line response functions of catheter-based radiation detector, obtained from study using canine femoral artery.
Experiments on Canine Coronary Artery
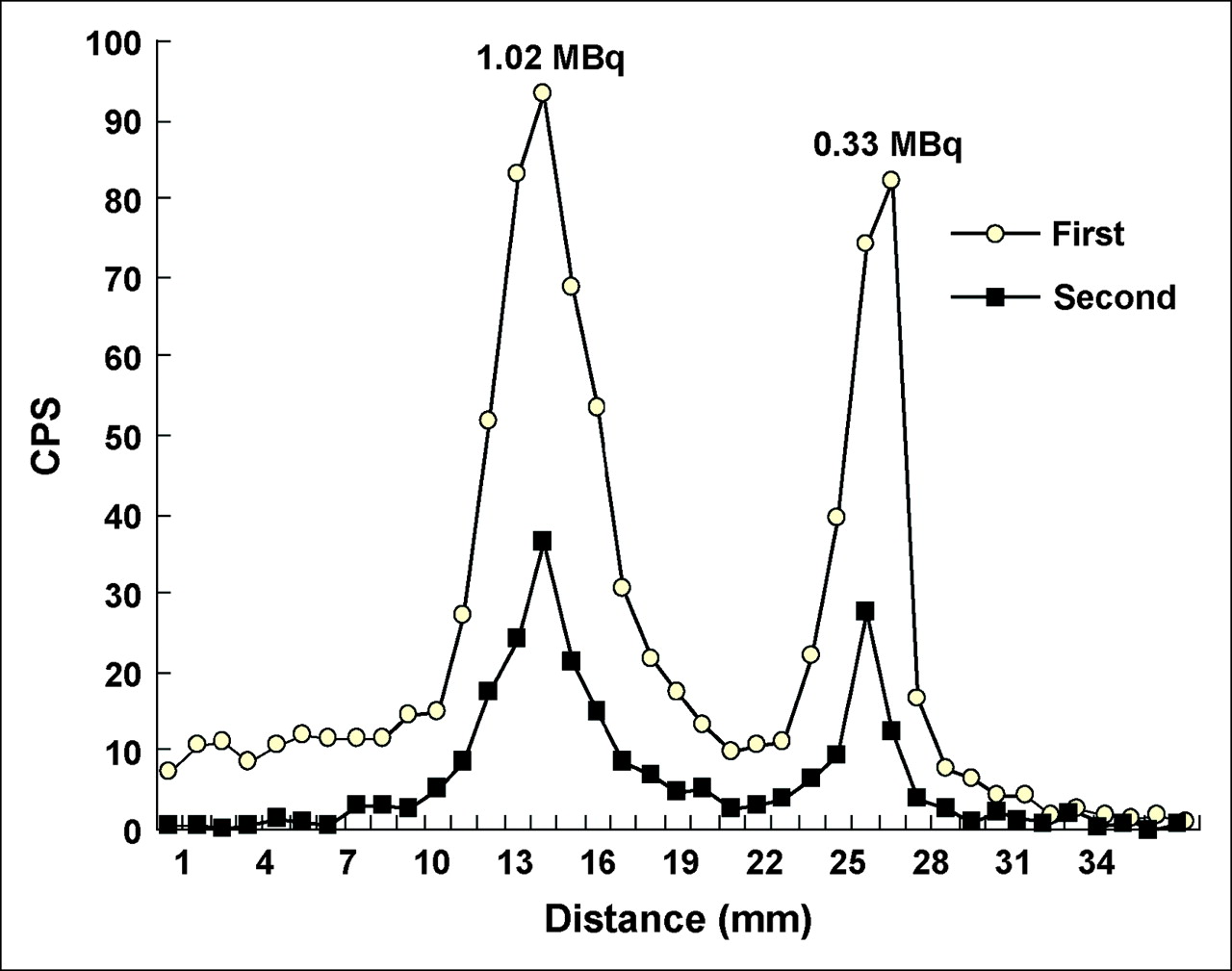
The IVRD probe could easily be advanced from the left carotid artery to the distal portion of the left descending coronary artery using the guiding catheter. Figure 5 shows the scan data of 18F point sources obtained by endovascular detection. Three point sources (66, 330, and 1,019 kBq) fixed on the surface of the canine coronary artery were detected as peaks of radiocounts, although the radioactivity peak of the 66-kBq point source was not clearly displayed.

Line response functions of catheter-based radiation detector, obtained from study using canine coronary artery.
DISCUSSION
This study demonstrated that the IVRD probe was small enough to cross through even the coronary artery and, when used with the coincidence technique (9) previously reported, was highly sensitive in the detection of radionuclide localizing in small lesions. This technique enabled cancellation of the noise signals derived from the photomultiplier and amplifier. As a consequence, the threshold level of the discriminator could be lowered.
This device could navigate the canine femoral and coronary arteries and detected the 18F point sources fixed on their outer surface (Figs. 4 and 5). However, the radioactivity peaks in the femoral artery experiment were relatively broad, and the peak counts were lower than expected from the results of the point source experiments previously reported (7). This finding would be due to the distance between the probe and the point sources, because the canine femoral artery was large (about 4 mm in external diameter) and the point sources were fixed on its outer surface. Therefore, in endovascular scanning of narrow vessels such as coronary arteries, detection of small plaques is expected to be much more sensitive. If the plaques surround the artery, a wide range of radiation from the plaques will be detectable and the unstable coronary plaques will be found without difficulty. However, detection using IVRD will be difficult if the plaques are long and diffuse in the coronary artery, because the peaks of radioactivity will be difficult to isolate precisely.
Our previous report (7) indicated that the IVRD probe should preferentially detect positron particles of 18F rather than annihilation photons. Concerning the effect of background radioactivity, the measurement of charged particles is thought to be advantageous for endovascular detection because of their short ranges. However, the sensitivity of the present device to γ-rays was not zero.
The reason why we measured twice using IVRD was to test the reproducibility and resolution of the system. In addition, it was more important to detect peaks of radioactivity than to determine radiocounts in this study. The distance between the targets and the probe often varies in relatively large vessels such as the femoral arteries; the delay between the 2 measurements was only 10 min; and the IVRD scintillator is 20 times more sensitive to β-rays than to γ-rays. Accordingly, the variation in the distance between the targets and the probe may have affected the radiocounts in the femoral artery study.
Clinical Implications
In therapeutic strategies for acute coronary syndrome, detection of vulnerable plaques before rupture is important. Recently suggested approaches to the detection of vulnerable plaques have included multidetector CT, MRI, intravascular ultrasound, coronary angioscopy, and optical coherence tomography (4,10–13). These modalities might be able to acquire morphologic information about coronary plaques but cannot fully convey physiologic or biologic information. The original technique—that is, detection of a small coronary plaque using a γ-camera outside the body—might be limited because of background activity, body attenuation, and the beating of the heart. This study demonstrated that IVRD with a plaque-avid tracer might be one of the most promising approaches to the detection of vulnerable coronary plaques. Prevention of acute coronary syndrome will be realized if the clinical application of this study becomes possible.
Study Limitations
In this study, the effect of background activity was neglected. Our previous study (7) using a ball phantom demonstrated that this device could detect small 18F point sources in the presence of intense background activity. In addition, the simulation study (14) indicated that the limit for detecting small plaques was 17.5 cps using Kaiser's 3-σ criterion. Detection of unstable plaques by the IVRD might be possible even after systemic injection of 296 MBq of 18F-FDG, because the IVRD study was performed by endovascular scanning and the scintillator is 20 times more sensitive to β-rays than to γ-rays. However, the background activity in the human body and the shapes of the coronary arteries and plaques are not uniform. Further investigations using an animal model of atherosclerosis might be necessary to elucidate this point.
In the coronary artery study, radioactivity (counts per second) was lower at the second measurement than at the first measurement. Reasons for this difference might be the amount of time involved and the short half-time decay of 18F. The interval between the 2 measurements was about 60 min. Because a coronary engaging catheter for canine use was not available, we applied a catheter for human use in this study. Thus, coronary engaging of the catheter was not easy, catheter insertion became necessary twice, and the time consumed was relatively long. However, IVRD procedures did not take long (only about 3−5 min). In a clinical setting, many kinds of coronary catheters are available. Therefore, even in human stenotic arteries, measurements will not take long. Regarding the half-time decay of 18F, the decrease in radiocounts in the coronary study could not be fully explained. Although we could not clarify reasons other than the amount of time involved, damage of the IVRD catheter could not be negligible.
CONCLUSION
Endovascular scanning with our newly developed catheter-based IVRD was able to detect 18F point sources fixed on the surface of canine femoral and coronary arteries. Thus, this detector in combination with charged-particle–emitting radiopharmaceuticals such as 18F-FDG might be useful for the endovascular detection of small lesions such as vulnerable coronary plaques.
Acknowledgments
We thank Nihon Medi-Physics Co., Ltd., Nishinomiya, Japan, for product support and encouragement. We also thank Toru Kanoi (Universal Giken Co., Ltd., Odawara, Japan) and Kazuhiro Saito (SD Giken Co., Ltd., Sakado, Japan) for technical assistance throughout the study.
References
- Received for publication November 4, 2005.
- Accepted for publication February 6, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}