


Abstract
Extraaxillary metastases (i.e., in the absence of axillary involvement) are more likely to develop in patients with inner-quadrant (IQ) breast cancer than in patients with outer-quadrant (OQ) primary tumors. The relative difficulty of identifying extraaxillary metastases may lead to understaging of cancer in these patients. This study examined whether 18F-FDG PET findings were differentially associated with the location of primary tumors, and with long-term prognosis, in IQ and OQ patients. Methods: Follow-up data were obtained for 141 patients whose breast cancer was staged by PET and who were documented to have IQ (n = 42) or OQ (n = 99) primaries. Results were stratified according to PET findings consistent with different metastatic patterns. Data were further analyzed with respect to disease outcome after a mean 3-y follow-up period. Results: Among IQ patients, progressive disease was identified in 26.1%, compared with 13.1% of OQ patients, for a relative risk (RR) of 2.0. Of patients with PET findings of isolated extraaxillary metastases, 36.1% had progressive disease, compared with 10.7% of other patients (RR = 3.4), and 61.9% of IQ patients had isolated extraaxillary metastases identified on PET, compared with 10.1% of OQ patients (RR = 6.1). Conclusion: IQ patients demonstrated a 6-fold greater frequency of PET findings of isolated extraaxillary metastasis, and such findings were associated with triple the risk for disease progression. Patients with IQ tumors could be vulnerable to understaging with conventional staging approaches and may particularly benefit from PET during the staging process.
In the United States, breast cancer ranks second among cancer deaths in women (1), and patients with primary lesions in the inner quadrant (IQ) of the breast have a higher mortality rate than patients with primary lesions in the outer quadrant (OQ) (2–5). IQ primary tumors, which are located in the medial region of the body, have a higher propensity to metastasize to extraaxillary sites without metastasizing to axillary regions (2,6). Because IQ patients have a greater incidence of these isolated metastases, their disease is understaged more frequently.
The higher mortality rate for IQ patients may in part be due to understaging and subsequent undertreating associated with the difficulty of detecting isolated extraaxillary metastases using conventional imaging methods. Several recent studies comparing 18F-FDG PET and conventional diagnostic techniques have reported that PET is more sensitive in detecting metastatic lesions, in particular extraaxillary metastases (7–14), but that PET is less sensitive in identifying axillary lymph node involvement (15–20).
The ability of PET to detect extraaxillary metastases suggests that patients with IQ primary tumors may benefit from the use of PET for staging and restaging evaluations. Recognition of extraaxillary processes early during the course of disease could have profound implications on the future management of, and administration of therapy to, breast cancer patients. Thus, in this study, we set out to evaluate the prognostic value of 18F-FDG PET by looking at the relationship between PET findings of hypermetabolic foci and the clinical outcome of patients with IQ versus OQ primary breast tumors.
MATERIALS AND METHODS
Patient Population
The study population (n = 150) included all breast cancer patients who were referred to our facility for 18F-FDG PET staging examinations through December 2001, for whom documentation allowing retrospective assignment of primary tumors to OQ or IQ locations was retrievable, and for whom longitudinal information on disease assessment was available. Patients with records indicating primary tumors in both IQ and OQ (n = 4) locations or in the areolar region (n = 5) were excluded from this analysis. Data pertaining to each patient’s initial evaluation and subsequent course of therapy were used through a protocol approved by the Office for Protection of Research Subjects of the UCLA Institutional Review Board.
Clinical Data
We obtained clinical data on each patient through review of inpatient and outpatient medical records and through a written study questionnaire completed by the patient’s referring or most recent managing oncologist. The clinical data, which included treatment history, stage of disease, recent tumor marker values, known tumor sites, date of most recent examination, and current disease status, allowed the disease to be classified as progressive or nonprogressive. If the disease was nonprogressive, we required a minimum of 10 mo of clinical follow-up data documenting that the patient’s condition was stable.
PET Imaging
Patients fasted for at least 6 h before intravenous injection of 555 MBq (15 mCi) of 18F-FDG. Whole-body PET emission data were obtained using Siemens ECAT EXACT HR or HR+ scanners (CTI PET Systems) for 6 min per bed position with 2-dimensional acquisition. PET scans were read by the nuclear medicine physicians on clinical service at the time of acquisition, who were unaware of this study and, in most cases, of the quadrant of the primary tumor.
Statistical Analysis
Statistical analysis of risk ratios was performed on collected data organized into a 2 × 2 table. Significant differences in continuous variables between each stratum of n patients were assessed by a 2-sided unpaired t test. Within each group, the strength of the association of PET findings with clinical outcome was assessed by the χ2 test. Ninety-five percent confidence intervals (CIs) for the probability (p) of each stratum of n subjects were calculated as the product of 1.96 and the square root of p(1 − p)/n. Calculation of relative risk (RR) and odds ratios was based on methods described by Gordis, and calculation of CIs was based on methods described by Armitage and Berry (21,22).
RESULTS
Distribution of Hypermetabolic Foci
Review of medical records revealed that more than one fourth of patients had primary tumors in the IQ (28%). The remaining patients had primary tumors in the OQ (66%), in both the IQ and the OQ (3%), or in the areolar region (3%). Review of original PET reports allowed stratification of OQ and IQ patients into subgroups based on whether hypermetabolic foci believed to be consistent with metastatic disease were found. Seventy-two examinations were for initial staging, and 69 were for restaging after one or more courses of therapy. For women who underwent multiple PET examinations, the scan obtained at the time closest to initial diagnosis was used. During follow-up after PET, 108 of the 141 patients received systemic treatment either as adjuvant therapy (n = 68) or for metastatic disease (n = 40). Among those patients, 26% had histories of IQ (n = 28) and 74% had histories of OQ (n = 80) primary tumors, similar to the distribution in the study population overall.
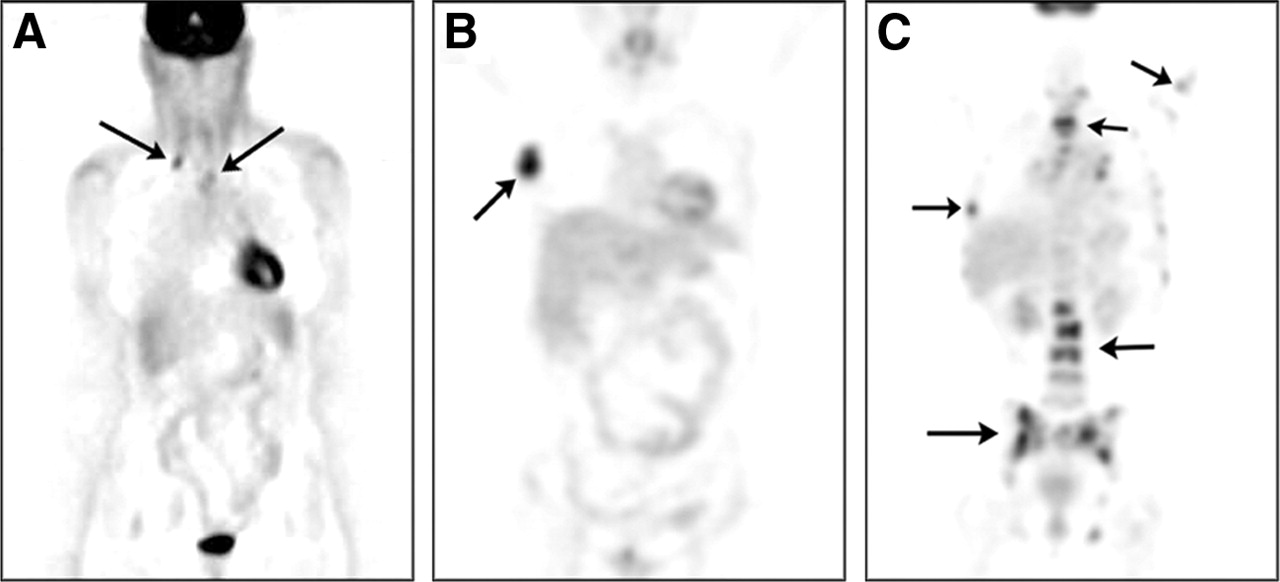
The mean ages of IQ (56 ± 10 y) and OQ (57 ± 14 y) patients were similar. On the basis of findings noted on the 18F-FDG PET reports, patients were stratified into 1 of 4 groups: extraaxillary metastasis only, axillary metastasis only, both extraaxillary and axillary metastases, or no metastasis (Figs. 1 and 2). Some patients had multiple sites of metastasis. Extraaxillary tumor sites included the mediastinal or internal mammary nodes (n = 15), supraclavicular region (n = 10), brain (n = 4), osseous processes such as spine and joints (n = 12), liver (n = 9), and lung or pleural cavity (n = 18). In IQ patients with isolated extraaxillary disease, tumor sites were the brain (n = 4), supraclavicular region (n = 5), mediastinal or internal mammary nodes (n = 1), osseous processes (n = 10), liver (n = 4), and lung or pleura (n = 10). In OQ patients with isolated extraaxillary disease, tumor sites were the supraclavicular region (n = 1), mediastinal or internal mammary nodes (n = 3), osseous processes (n = 2), liver (n = 2), and lung or pleura (n = 3).

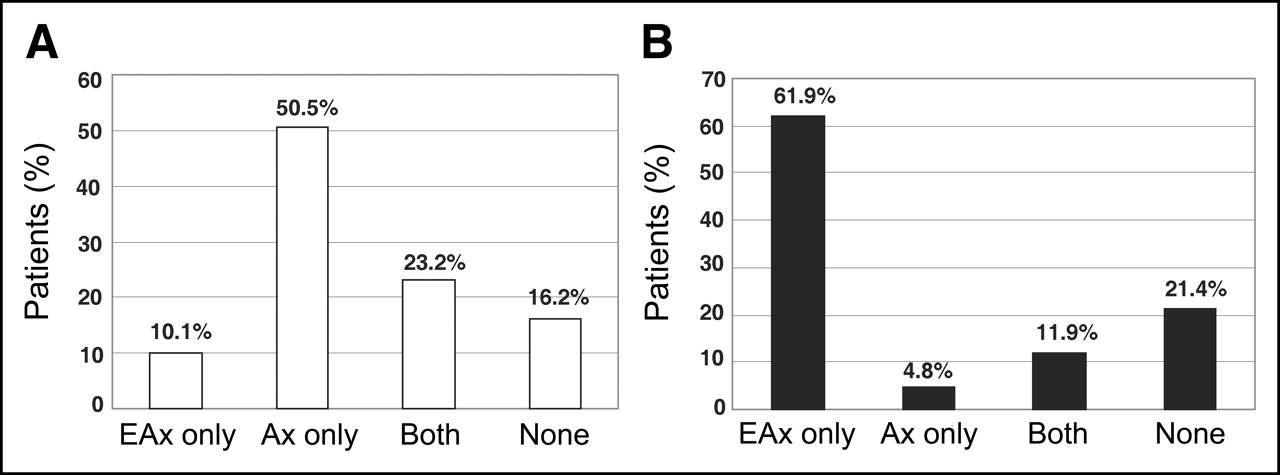
(A) Distribution of PET findings of hypermetabolic foci for 99 OQ patients. (B) Distribution of PET findings of hypermetabolic foci for 42 IQ patients. EAx = extraaxillary; Ax = axillary; both = axillary and extraaxillary; none = no metastases.

Whole-body coronal 18F-FDG PET scans of breast cancer patients, with arrows indicating extraaxillary metastases in chest and supraclavicular regions (A), metastasis in right axilla (B), and axillary and extraaxillary metastases in chest, lumbar, and iliac regions (C).
Within the group of OQ patients, 10.1% (n = 10) had extraaxillary metastases, 50.5% (n = 50) had axillary metastases, 23.2% (n = 23) had both extraaxillary and axillary metastases, and 16.2% (n = 16) had no metastases identified on PET (Fig. 1A). For IQ patients, 61.9% (n = 26) had extraaxillary metastases, 4.8% (n = 2) had axillary metastases, 11.9% (n = 5) had both extraaxillary and axillary metastases, and 21.4% (n = 9) had no identified metastases (Fig. 1B). The IQ group thus exhibited a higher frequency of PET findings for isolated extraaxillary metastasis, whereas the OQ group exhibited a higher frequency of PET findings for axillary metastasis only, and the RR for finding isolated extraaxillary metastases in IQ (61.9%; 95% CI, 48%–76%) versus OQ (10.1%; 95% CI, 0%–33%) patients was 6.13 (95% CI, 3.25–11.55).
Clinical Follow-up
Data obtained for both IQ and OQ patients indicated that, during the average post-PET follow-up of about 3 y, 17% of the 141 patients experienced disease progression whereas 117 (83%) maintained a disease-free or stable clinical course. The average follow-up was 36 ± 13 mo and 35 ± 12 mo for the IQ and OQ groups, respectively. Patients within each group were stratified according to whether their disease was progressive or nonprogressive (stable or regressed). Each of the subgroups based on hypermetabolic foci was also stratified according to such outcome data (Fig. 3).

Breakdown of clinical outcomes and PET findings for different primary-tumor locations.
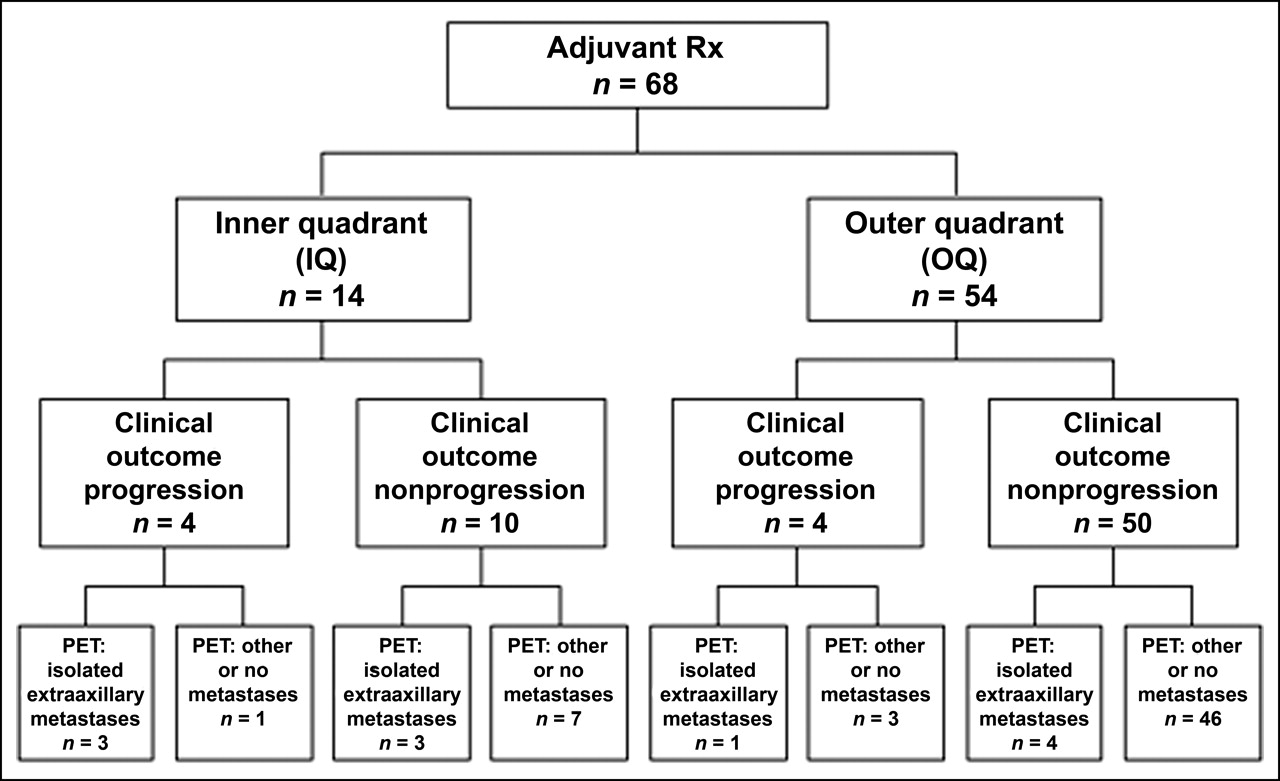
The analysis revealed disease progression among 34.6% (9/26) of IQ patients with isolated extraaxillary metastases, compared with 12.5% (2/16) of IQ patients with other patterns of metastases or no metastases (RR = 2.77, 34.6%/12.5%). The risk for disease progression was 3.96 times greater among OQ patients with PET findings of isolated extraaxillary metastases (40%, 4/10) than among OQ patients with other patterns of metastases or no metastases (10.1%, 9/89). The proportion of IQ patients with progressive disease (26.2%, 11/42) was twice the proportion of OQ patients with progressive disease (13.1%, 13/99). For the entire study group, the frequency of progressive disease documented in patients with PET findings of isolated extraaxillary metastases was 36.1% (13/36), versus 10.5% (11/105) for other patients, for an RR of 3.45. Clinical data allowed further stratification of patients into groups according to the type of post-PET therapy (adjuvant, for metastatic disease, or none) received during follow-up. Among those who received adjuvant therapy (n = 68), 42.9% (6/14) of IQ patients had PET findings of isolated extraaxillary metastases, compared with 9.3% (5/54) of OQ patients (RR = 4.63) (Fig. 4). Similarly, for patients who received post-PET treatment for metastatic disease (n = 40), IQ patients had a greater frequency of PET findings of isolated extraaxillary metastases (RR = 3.50, 87.5%/25.0%). For patients undergoing systemic therapy, quadrant-associated risk of progression was particularly heightened when the therapy was adjuvant; 28.6% (4/14) of IQ patients were documented to have progressive disease, versus 7.4% (4/54) of OQ patients, for an RR of 3.86.

Breakdown of clinical outcomes and PET findings for patients who received adjuvant treatment after PET. Among patients who received adjuvant treatment, 20.6% (14/68) had IQ tumors and 79.4% (54/68) had OQ tumors.
DISCUSSION
In breast cancer patients with primary tumors in an OQ, metastases are more often in the axillary lymph nodes, whereas patients with primary tumors in an IQ more often have extraaxillary metastatic disease. Isolated extraaxillary metastases can go undetected during conventional staging, possibly contributing to the higher mortality rate of IQ patients than of OQ patients. An evaluation of 2,396 breast cancer patients found that those with primary tumors in central or IQ locations had a 30% greater chance for development of distant metastases and a 20% higher mortality rate than did patients with OQ primary tumors (2). Another study found patients with medial primary breast tumors to have double the risk of patients with lateral tumors for relapse of disease and for breast cancer death (3). The higher mortality rate associated with lesions in the IQ may result from the greater difficulty in detecting spread of disease to extraaxillary sites. Accurate staging after initial diagnosis of disease is critical for determining the most appropriate course of therapy and may thereby affect clinical outcome.
The longitudinal clinical information collected here comprises a database of PET findings that one can relate to primary tumor location and subsequent disease course. Patients with and without disease progression did not significantly differ in age at the time of PET or in the length of follow-up. Patients with IQ primary tumors had a 6-fold greater frequency of PET findings of isolated extraaxillary metastasis and a greater risk for development of progressive disease than did patients with OQ primary tumors. In addition, patients who had isolated extraaxillary metastases identified by PET had triple the risk for disease progression of those who did not. This discovery suggests that IQ patients with PET findings of isolated extraaxillary metastases may not have received treatment as adequate as that received by IQ patients with no or other patterns of metastases or by OQ patients overall.
A potential limitation of this study is the question of the generalizability of its results: How closely do patients seen in a tertiary-care university clinical environment compare with patients seen in a community setting? However, all 18F-FDG PET scans were acquired under standard clinical protocols and read by nuclear medicine physicians as standard clinical (nonresearch) studies, after being ordered by referring physicians generally as a “problem-solver,” when they desired more information to help clarify the extent of disease (23).
Other possible limitations of the study data deserve mention. Follow-up for patients after PET averaged 3 y. It is possible that in some patients, disease progression may develop after this period, such that classification of their clinical course as “nonprogressive” is somewhat arbitrary. Nevertheless, the lengths of follow-up for IQ and OQ patients were nearly identical (36 ± 13 mo and 35 ± 12 mo), and this limitation would not affect main conclusions unless progression after follow-up were to occur more frequently in OQ patients than in IQ patients. That situation would seem unlikely, and even if it were to exist, the main observations would still hold from a time-to-progression perspective. As another possibility, selection bias based on differential availability of clinical information for patients with IQ and OQ tumors could occur, but again we cannot envision a way in which this could have occurred that would be likely to alter our main findings. Similarly, any intergroup differences in clinical parameters about which we have incomplete information, such as distribution of TNM stages or number of prior courses of therapy, could serve as possible confounders.
It was not within the scope of this study to consider quantitative information such as the standardized uptake values of PET findings, because many of the scans were obtained before the routine implementation of attenuation correction. Several studies, however (24–27), have found 18F-FDG standardized uptake values to be a probable prognostic factor for assessing the response of breast cancer patients to therapy, and the information obtained from such measurements may well be used to complement the location-based findings of this study.
CONCLUSION
In summary, 18F-FDG PET scans of patients with IQ primary tumors often reveal a pattern of hypermetabolic foci consistent with isolated extraaxillary metastasis. Such patients may particularly stand to benefit from the use of PET to ascertain the actual stage of disease and help ensure that the therapeutic approach is at an appropriate level of aggressiveness.
Footnotes
Received Dec. 3, 2005; revision accepted May 18, 2005.
For correspondence or reprints contact: Daniel H.S. Silverman, MD, PhD, Department of Molecular and Medical Pharmacology, University of California, Los Angeles, 10833 LeConte Ave., Center for Health Sciences, AR-144, Los Angeles, CA 90095-6942.
E-mail: dsilver{at}ucla.edu
Guest Editor: Dominique Delbeke, MD, PhD





{kind=link}
{kind=link}
{kind=link}
{kind=link}