


Abstract
Breast cancer is the most common non-skin type of cancer and the second leading cause of cancer mortality in women. Advances in diagnosis and treatment have led to declines in mortality, despite an increase in breast cancer incidence. An advancing array of both local and systemic therapy options has led to increasingly individualized treatment. Imaging plays a key role in detecting breast cancer and directing its therapy. This continuing education article, part 1 in a 2-part series, provides a comprehensive review of current and future radiotracer imaging methods applied to breast cancer, in the context of breast cancer management strategies and other nonnuclear imaging methods. Part 1 of the review provides an overview of clinical and biologic considerations in breast cancer and covers radionuclide imaging for detection and staging. Part 2 will cover radionuclide imaging of breast cancer response to therapy, other clinical indications for radionuclide breast cancer imaging, and future directions, including molecular imaging.
Breast cancer is the most common non-skin type of cancer and the second leading cause of cancer mortality in women (1). Although the incidence of breast cancer continues to rise, mortality has declined over the past several years (1,2). The decline has been attributed to both early diagnosis and more effective treatment (2). Advances in molecular cancer biology have led to an increased understanding of the biologic factors that contribute to breast cancer pathogenesis and progression. This understanding has already led to new and effective treatments (3), and new targeted therapies continue to be developed and tested (4). Advances in breast cancer molecular biology have also yielded improvements in diagnosis through molecular pathology and molecular imaging (5,6).
Radiotracer imaging studies have played, and will continue to play, an important role in breast cancer care. This continuing education article first reviews classification schemes for breast cancer pathology and staging and then gives an overview of approaches to breast cancer treatment to frame the diagnostic needs for breast cancer care and provide an outline of the categories of diagnostic tasks for which imaging plays a role. The discussion then reviews the application of radiotracer imaging methods to breast cancer diagnosis and treatment in the context of diagnostic needs and other nonradiotracer imaging methods. Part 1 provides an overview of clinical and biologic considerations in breast cancer and covers radionuclide imaging for detection and staging. Part 2 will cover radionuclide imaging of breast cancer response to therapy, other clinical indications for radionuclide breast cancer imaging, and future directions, including molecular imaging.
INCIDENCE, RISK FACTORS, PATHOLOGY, AND CLASSIFICATION
Breast cancer is largely a disease of women, with an annual incidence of 125 per 100,000 in the United States (1). The most well-established risk factors for breast cancer include age, family history and genetics, late first pregnancy, and obesity (7). Age is an important risk factor, and most of the women with breast cancer are postmenopausal; however, breast cancer is not uncommon in premenopausal women and often more aggressive in this group than in postmenopausal women. The recognition of gene mutations in the germ cell line (8)—for example, in the BRCA1 gene—was a major advance in understanding the basis of inherited disease, and a consideration of genetic profile is increasingly incorporated in breast cancer risk assessment, particularly for families prone to breast cancer at an early age.
Features of the pathologic classification of breast cancer are listed in Table 1. Breast cancers arise from the epithelial cells in the breast cancer ducts (9). The most important histologic feature in the primary tumor is the presence or absence of tumor invasion beyond the ductal architecture. Tumors that have not broken through the outer boundaries of ductal structures are termed noninvasive (ductal carcinoma in situ) and rarely metastasize (9), whereas invasive cancers have demonstrated their ability to break through tissue boundaries at the time of diagnosis and can metastasize both through lymphatic and hematologic spread. Other histologic features include the architectural pattern (ductal, lobular, or mixed) and the presence or absence of lymphovascular invasion (9). In addition to morphologic analyses, biopsy material is routinely assayed for phenotypic features that include the expression of hormone receptors (estrogen receptor [ER] and progesterone receptor [PR]) and HER2/neu (also known as cerbB2), typically by immunohistochemistry or fluorescent in situ hybridization. These markers predict tumor aggressiveness and behavior, and are also targets for specific therapy (10).
Pathologic Classification of Breast Cancer
The use of gene-expression profiling methods has yielded further insights into breast cancer phenotype (11). A common classification scheme centers on a model of ductal architecture. At the center of the ductal structure are cells that have the phenotype of ductal epithelial cells and are termed luminal. These cells most often express hormone receptors (ER and PR) and sometimes overexpress HER2 (typically luminal B). At the other extreme are those cells that conceptually have features of the outer myoepithelial cell layer, termed basal cells. These cells most commonly lack expression of ER, PR, and HER2, often termed triple-negative cancers (12). The ability to measure gene expression has also increased the ability to predict tumor aggressiveness and the likelihood of recurrence, and some predictive expression panels are now approved and used in clinical practice (13).
Breast cancer stages are defined in Tables 2 and 3. The most widely accepted system is that of the American Joint Committee on Cancer, which uses a TNM approach (Table 2) (14). There is also a stage classification, which includes groups of TNM categories ranging from early-stage disease (stage I) to late-stage metastatic disease (stage IV) (Table 3). Improved diagnosis and staging, especially sentinel lymph node (SLN) mapping, has resulted in recent updates in the staging definitions (14).
Summary of American Joint Committee on Cancer Staging System for Breast Cancer
Alternative Staging System for Invasive Breast Cancer
TREATMENT OPTIONS
To understand diagnostic needs for breast cancer, it is important to understand the range of approaches to breast cancer treatment (Table 4). With the exception of early- and late-stage disease, almost all breast cancer care involves a combination of locoregional and systemic treatments. Locoregional therapy includes surgery and radiotherapy, and systemic therapy includes chemotherapy (e.g., taxanes), endocrine therapy (hormonal, e.g., aromatase inhibitors), and targeted therapy (biologic, e.g., anti-HER2 drugs).
Current Treatment Options for Breast Cancer
Surgical excision of the primary tumor remains a key feature of the treatment of newly diagnosed breast cancer (15) and can be accomplished by mastectomy, removal of the entire breast, or by breast-conserving surgery, often termed lumpectomy of cancer (15). When lumpectomy is accompanied by postsurgical radiotherapy, breast conservation provides acceptably low rates of local recurrence and similar survival but with preservation of the breast (16). Recent advances in primary breast surgery include oncoplastic methods and improvements in reconstructive surgery to preserve, as much as possible, cosmetic integrity for breast cancer patients (17). For invasive disease, axillary nodal staging is routinely performed at the time of surgery. Approaches include targeted SLN dissection, guided by mapping techniques, and full axillary nodal dissection, guided by anatomic boundaries (18). Axillary sampling is performed largely for diagnostic purposes; the therapeutic value of lymph node removal remains largely unproven (19).
Radiotherapy is commonly used as an adjunct to surgery in locoregional breast cancer treatment (20). Breast radiotherapy is a key component of breast-conservation therapy, and for most tumors, lumpectomy performed without breast radiotherapy leads to unacceptably high rates of local recurrence (16). Therefore, breast radiotherapy is considered an integral part of breast-conservation treatment. Breast radiotherapy has traditionally been performed by fractionated whole-breast irradiation; however, interest in partial-breast irradiation and brachytherapy methods, especially for smaller tumors, has increased (21). Adjuvant chest wall irradiation can also be used in mastectomy patients and is usually reserved for patients with larger tumors or documented chest wall invasion (20). Adjuvant radiotherapy is also used in the treatment of regional nodal basins and has been shown to enhance survival in those patients with multiple axillary nodal metastases (22). Ongoing studies are examining the value of adjuvant radiotherapy in patients with more limited axillary nodal disease. Finally, palliative radiotherapy can be effective in selective treatment of breast cancer metastases to control symptoms or preserve structural integrity in the case of bone metastases.
Among solid tumors, breast cancer is one of the cancers most amenable to systemic therapy, in the form of both cytotoxic chemotherapy and more targeted treatments. One of the significant advances in breast cancer treatment was the recognition that breast cancer is a systemic disease and that even early breast cancer, with apparently limited extent, can give rise to micrometastases, leading to recurrence after apparently complete excision (16). To address this problem, adjuvant systemic therapy is used in addition to locoregional therapy in most invasive cancers and is credited, in part, for a reduction in breast cancer mortality. Systemic cytotoxic chemotherapy is used commonly in more advanced or aggressive tumors, particularly in those that lack ER or PR expression (23). In ER-expressing tumors, adjuvant endocrine therapy is used, typically an aromatase inhibitor or tamoxifen (24). In higher-risk ER-expressing tumors, both chemotherapy and endocrine therapy can be used (23). Both types of treatment are primary therapy for metastatic disease (25). In addition to chemotherapy and endocrine therapy, there is an increasing array of other targeted systemic treatments for breast cancer. Most notable is the development of treatments for patients whose tumors overexpress HER2. These agents (trastuzumab and, more recently, lapatinib) have become key components of both adjuvant and metastatic systemic therapy (3,26). The antiangiogenesis drug bevacizumab was also recently approved for metastatic breast cancer (27). New breast cancer targets continue to be investigated (4) and may be especially important in triple-negative patients (ER/PR/HER2–negative), in whom endocrine and HER2-targeted therapies are unlikely to work (28).
The choice of therapeutic approach depends on the disease burden at presentation, the likelihood of additional spread or progression, patient comorbidities, and patient preference. For noninvasive cancers, local therapy (surgery and radiotherapy) is sufficient. Some studies have suggested that endocrine therapy may reduce the incidence of local recurrence and new primary tumors. For nonmetastatic cancers with invasive disease (other than stage IV and not including those patients with small tumors < 1 cm, which may be treated by local therapy alone in some cases), treatment is typically surgical excision with or without radiotherapy, followed by adjuvant systemic therapy (29). For patients with a larger local disease burden, particularly those with locally advanced breast cancer (LABC; large primary tumor or advanced axillary disease without clinically apparent distant metastases), systemic therapy may be administered in advance of local therapy, often termed neoadjuvant therapy (30). Because breast cancer that is metastatic beyond the regional node (stage IV) is rarely cured, systemic therapy is the primary treatment for metastatic disease, with locoregional treatment reserved for symptom control and used possibly in some patients with limited metastatic disease who may achieve prolonged remissions (25).
DIAGNOSTIC TASKS FOR BREAST CANCER
The diagnostic tasks for breast cancer are summarized in Table 5. For each task, the commonly used methods are listed, with the selected approaches that are either less commonly used or still undergoing clinical testing indicated by parentheses. Perhaps the most important diagnostic task is breast cancer detection. Breast cancers can be discovered by physical examination by the patient or her physician (symptomatic patients) or found by imaging performed for screening in asymptomatic patients. For imaging, the word detection is usually used in conjunction with breast cancer screening, most commonly performed using mammography. Breast cancer diagnosis involves the characterization of a suspected mass or imaging finding and entails tissue sampling to make a definitive diagnosis of cancer versus benign disease. Staging is the determination of the extent of the disease burden in a patient with a known or highly suspected cancer, including the extent of disease in the affected breasts, regional lymph nodes, and distant (systemic) sites. We combine the discussion of breast cancer detection, diagnosis, and staging into a discussion of primary tumor imaging. For patients undergoing systemic therapy in the neoadjuvant or metastatic setting, measuring therapeutic response, which involves some form of imaging in almost all cases, is important. Finally, we include the category of disease characterization, namely measuring the specific biologic characteristics of the tumor to predict its likely behavior, including response to treatment. Although this task has thus far been confined to assays of biopsy material (i.e., nonimaging approaches), we briefly highlight how emerging imaging methods may also play a role in characterizing breast cancer and helping to direct treatment.
Diagnostic Problems for Breast Cancer
DETECTION AND DIAGNOSIS
Overview
Most primary cancers are detected by physical examination or mammography during screening or clinical work-up of a breast lesion (31). Mammography is the primary imaging modality for breast cancer screening, detection, and diagnosis (32). Although mammography is an effective imaging tool, its limitations include moderate sensitivity and specificity (32); therefore, many other imaging modalities have been investigated to complement and increase the diagnostic accuracy of breast imaging. Ultrasound and MRI are important adjuncts to mammography for both diagnosis and characterization of breast cancer and are routinely used in this role (33,34). Ease of use and real-time imaging capability make breast ultrasound one of the methods of choice for guiding breast biopsies and other interventional procedures (35). Breast MRI is rapidly emerging as an important clinical tool, especially for determining extent of disease within the breast, and can also be used to direct biopsy (34). In addition, MRI has shown utility for screening in high-risk women and was recently incorporated into the American Cancer Society recommendations for screening of high-risk patients (36).
PET and Positron Emission Mammography (PEM)
The finding of increased 18F-FDG uptake in cancer spurred interest in the use of 18F-FDG to diagnose primary breast cancers. Most studies have suggested that the degree of 18F-FDG uptake is somewhat correlated with breast cancer phenotype such as histologic type (higher uptake in ductal vs. lobular cancers), tumor histologic grade, and indices of cellular proliferation (higher uptake with higher levels of proliferation) (37,38). Low uptake is seen in ductal carcinoma in situ and well-differentiated forms such as grade I lobular breast cancer (37).
Although whole-body 18F-FDG PET has reasonable sensitivity and specificity in detecting malignant lesions in general, its sensitivity for primary breast cancer is limited. Overall, the sensitivity of 18F-FDG PET in detecting primary breast cancer is 64%−96%, specificity is 73%−100%, positive predictive value is 81%−100%, and negative predictive value is 52%−89% (31). Multiple investigators have demonstrated the diminished ability of 18F-FDG PET to detect a small, well-differentiated in situ breast carcinoma. Kumar et al. (39) evaluated 18F-FDG PET of 85 primary breast cancers and demonstrated that tumor size less than 1 cm and low tumor grade were significant predictors of a false-negative 18F-FDG PET results. Because primary breast cancer detection requires the ability to depict occult, nonpalpable, small (<1 cm) invasive and in situ malignant lesions, whole-body 18F-FDG PET is not used in primary breast cancer detection.
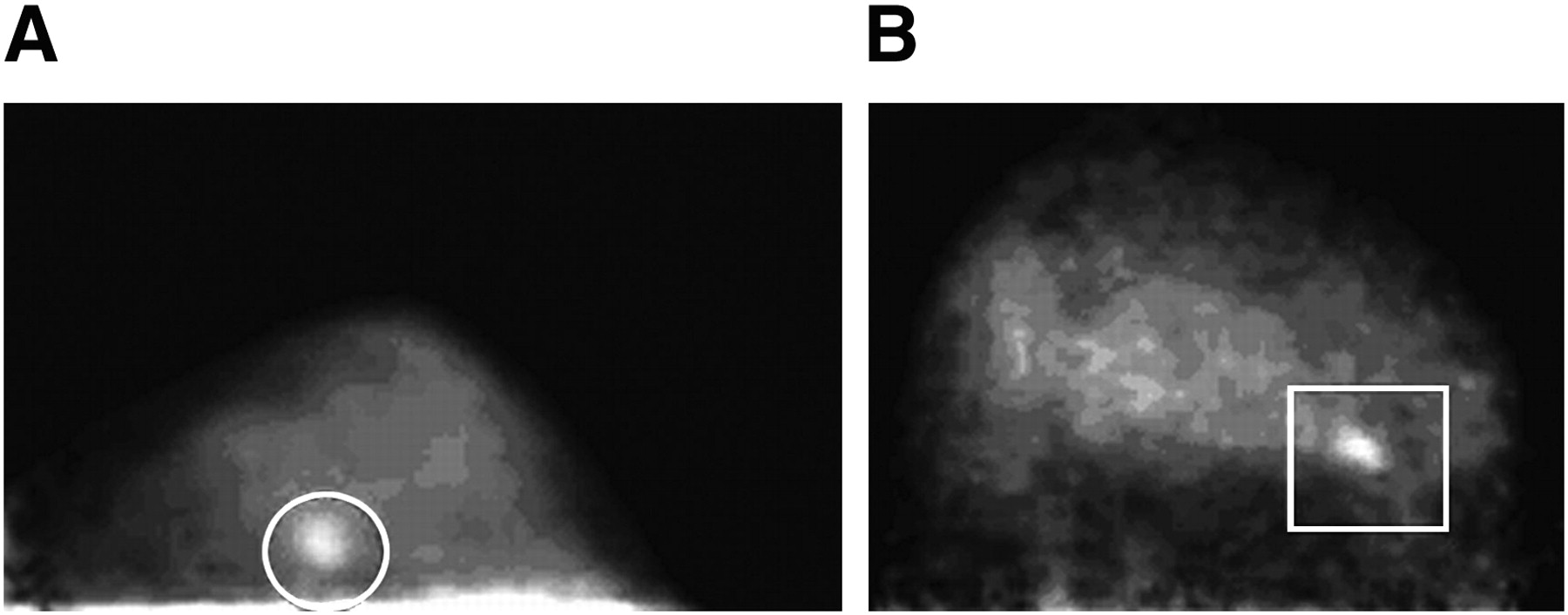
To overcome the limitations of whole-body 18F-FDG PET, dedicated breast PEM units have been developed (Fig. 1) (40). The advantages of PEM, compared with whole-body 18F-FDG PET, include higher spatial resolution, shorter imaging time, and reduced attenuation; PEM also maintains higher count sensitivity. In addition to compression capability, dedicated devices have a small physical footprint, which makes their use in a breast-imaging facility feasible, allows correlation with mammography, and permits PEM-guided biopsy. Early studies demonstrated that PEM is capable of imaging smaller breast cancers than is 18F-FDG PET (40). Moreover, a recent multicenter trial also suggested that PEM may aid in the detection and characterization of both invasive and in situ breast carcinoma (41). Berg et al. reported that 10 of 11 in situ carcinomas were detected by PEM, and 8 of 10 were detected by mammography and ultrasonography (41). The reported limitations for PEM include the imaging of posterior lesions, variable 18F-FDG uptake in small tumors, and false-positive findings from prior biopsy (41,42). Recently, PEM with capability of biopsy has been developed and is being tested (43). However, the clinical data regarding dedicated positron breast-imaging devices are still limited, particularly compared with the large amount of data supporting and validating screening mammography and other adjunctive primary breast-imaging modalities such as ultrasound and breast MRI. Although the PEM devices so far can, in part, overcome the limitations of whole-body 18F-FDG PET in breast cancer detection, the utility of PEM, compared with existing breast-imaging methods, awaits validation in larger prospective trials before more general acceptance and more widespread clinical use.
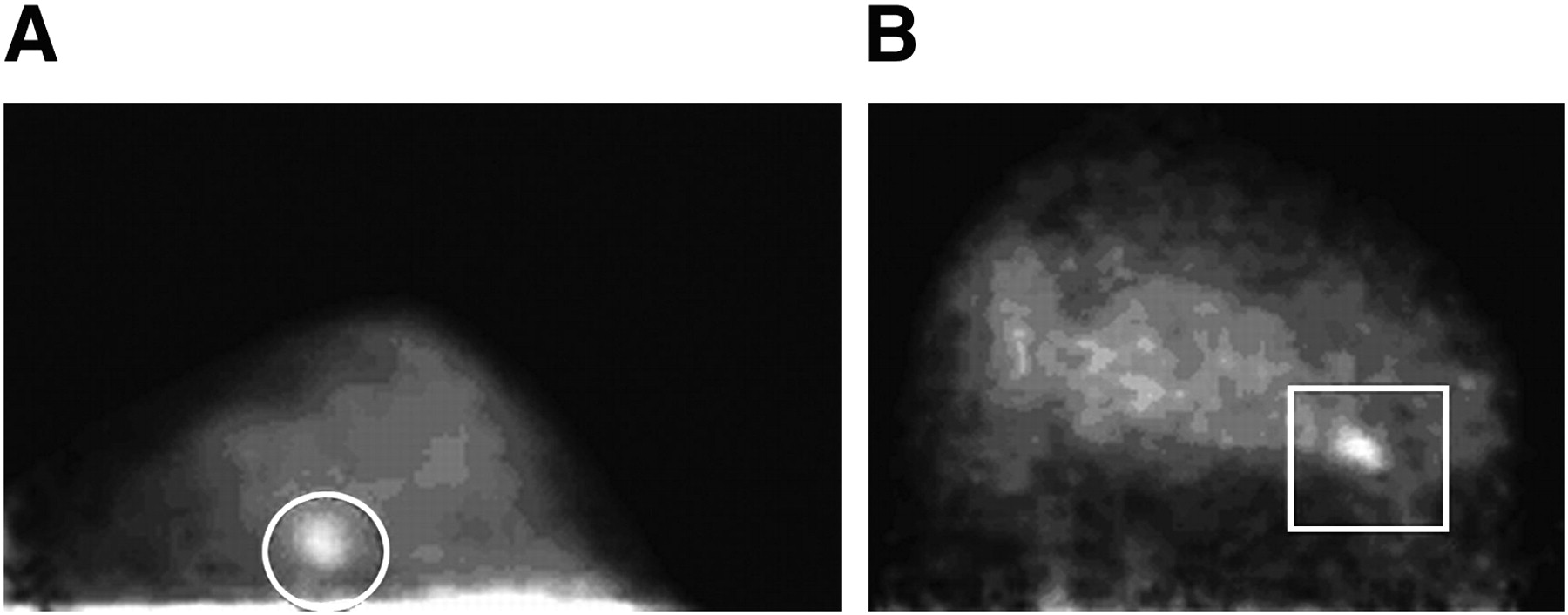
Demonstration of small invasive breast cancer using 18F-FDG PEM. Images from dedicated breast PEM units show 9-mm (circle in A) and 1.3-cm (rectangle in B) invasive cancer. (Adapted with permission of (40).)
Single-Photon Breast Imaging
99mTc-sestamibi and related compounds have also been tested for primary breast cancer imaging. 99mTc-sestamibi is a cationic compound that is transferred across the cell membrane into the cytoplasm and mitochondria and retained by electrical potentials across membrane (44). 99mTc-sestamibi uptake and retention in breast cancer appears to depend on several factors such as regional blood flow, plasma and mitochondrial membrane potential, angiogenesis, and tissue metabolism (45–47). Several studies have reported 99mTc-sestamibi uptake is higher in breast cancers demonstrating more aggressive features, including higher indices of nuclear grade, higher indices of proliferation, greater microvessel density, and high tumor blood flow (46,47), but the precise mechanism of increased uptake and the relative importance of these factors are not completely understood.
Since the first large-series study using prone 99mTc-sestamibi scintimammography in 1994 (48), many studies investigating the diagnostic accuracy of this method in evaluation of suspected breast cancer have been published. Liberman et al. (49) performed a meta-analysis and reviewed literature published up until 1999 on the diagnostic accuracy of this method. Overall sensitivity was 85%, specificity 87%, positive predictive value 88%, negative predictive value 81%, and accuracy 86%. Most (80%) of the studies reported sensitivity and specificity values higher than 80%, with nearly half of them yielding values higher than 90%. Similar results were seen in a large multicenter prospective clinical trial evaluating the efficacy of 99mTc-sestamibi scintimammography for the diagnosis of breast cancer. The sensitivity and specificity of this method were estimated at 93% and 87%, respectively, with an accuracy of 88% (50). However, concern remains that 99mTc-sestamibi scintimammography has limited ability to detect lesions less than 1 cm, with sensitivity lower than 50% in some series (51). 99mTc-sestamibi scintimammography also has comparably lower sensitivity for nonpalpable lesions. False-positive uptake in benign breast lesions, inflammation, hematoma, and fat necrosis can also be seen. As a result of these concerns, 99mTc-sestamibi scintimammography with conventional γ-cameras has not found widespread use for breast cancer detection and diagnosis.
More recently, high-resolution small–field-of-view γ-cameras specific to breast imaging, sometimes called breast-specific γ-imaging (BSGI) or molecular breast imaging, have been developed (52,53). Preliminary data using breast-specific γ-cameras, compared with γ-camera imaging, for evaluating women with breast lesions before biopsy demonstrated improved resolution of breast cancer, with improved visualization of nonpalpable lesions, lesions smaller than 1 cm, and in situ carcinoma (53). Brem et al. reported that BSGI correctly identified 16 of 18 cancers (88.9%) smaller than 1 cm. The authors also found 5 of 6 in situ carcinoma smaller than 1 cm (53). Another study by the same group demonstrated higher sensitivity in detection of in situ carcinoma for BSGI versus mammography or breast MRI (52). As with PEM, larger trials with comparisons to standard breast imaging will be needed to support more widespread use of BSGI. These trials are ongoing.
STAGING
Overview
The extent of spread at presentation is one of the most important prognostic factors for breast cancer patients (14). Staging is also important for recurrent breast cancer. Staging is typically divided into logoregional staging (for regional lymph nodes, especially axillary nodes) and distant or systemic staging (for sites beyond regional lymph nodes). Almost all patients with invasive breast cancer will undergo axillary nodal staging because the presence or absence of spread to axillary lymph nodes is an important consideration for further treatment after surgery (18). For patients with early-stage breast cancer and without evidence of regional nodal spread (stage I or the low end of stage II), systemic staging is not recommended unless there are symptoms (54) because the chance of distant metastases is low and the chance of false-positive findings in staging studies is considerably higher than is the chance of true-positive findings (55,56). For recurrent breast cancer or breast cancer with known metastases, systemic staging is recommended (54). For LABC, especially for patients with advanced axillary nodal disease, the risk of systemic metastases is high enough that systemic staging is often performed as part of the initial evaluation (30).
Locoregional Staging
Lymphoscintigraphy.
The traditional approach to axillary nodal staging was the axillary nodal dissection, in which axillary contents were removed and examined. The morbidity of this process, including a significant incidence of lymphedema, led to the search for a less morbid but equally accurate approach (18). On the basis of work that had been done for melanoma nodal staging (57), the SLN mapping and sampling approach was tested for breast cancer, with good early success (58–60). SLN sampling has emerged as the standard of care for axillary nodal sampling in patients with clinically negative axillae (61). The approach is to identify and sample the nodes that are the first draining nodes (i.e., sentinels in the axillary drainage basin for the breast lesion), yielding a much smaller surgical procedure than full axillary nodal dissection with much less morbidity (18). If sentinel nodes are negative, then the chance of downstream nodal metastases is quite small, and the patient can be spared the full dissection. If the sentinel node shows evidence of metastasis, then an axillary dissection may be needed to determine the extent of axillary spread. The SLN mapping and sampling approach has been thoroughly tested in large clinical trials and shown to be safe and accurate, with patient outcome comparable to that of axillary nodal dissection (62,63).
Some controversies exist regarding the methodology for SLN biopsy (64,65). Typically, a colloidal radiopharmaceutical (99mTc-sulfur colloid in the United States) is injected, and sentinel nodes are identified through imaging (lymphoscintigraphy; Fig. 2), γ-probes, or both (66). Other, more specific agents have been developed and are undergoing testing (67). Some centers use both radiocolloid and visible blue dye to guide SLN sampling, whereas some centers use one of the methods without the other (18).
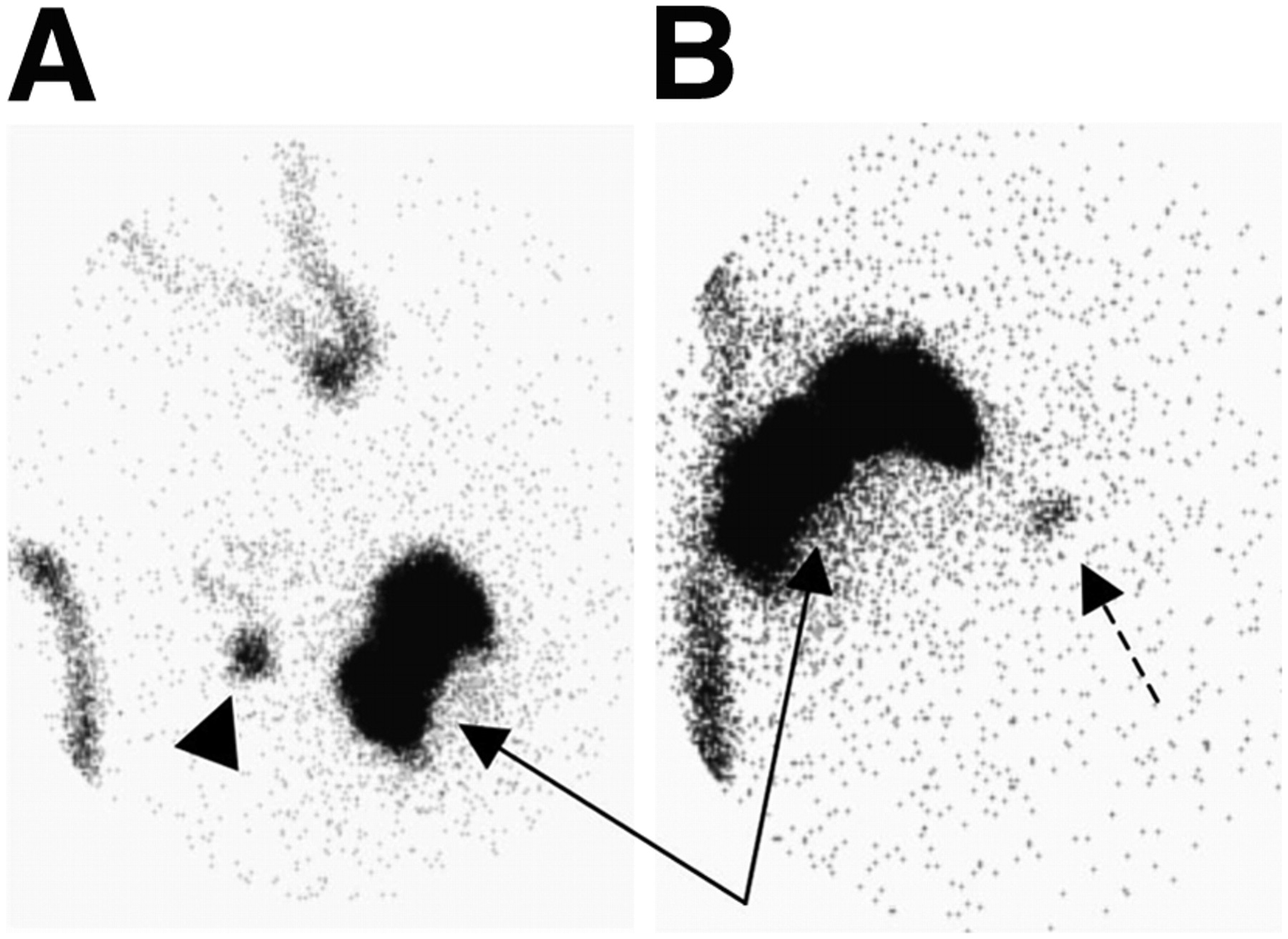
Example of lymphoscintigraphy for SLN mapping. Two sets of anterior images are shown, one focused on axilla (A) and other on more central chest (B), taken after perilesional injection of filtered 99mTc-sulfur colloid (solid arrows). Body outline has been indicated using 99mTc markers. Axillary sentinel node is indicated by arrowhead. IM node is also seen (dashed arrow).
Early studies used perilesional injection of radiotracer or blue dye, under the premise that the area surrounding the tumor would be the most representative of lymphatic drainage pathways (68). More recently, studies have shown that intradermal injection over the lesion site or subareolar injection identifies the same axillary SLN found by perilesional injection (69) and provides similar rates of accuracy for axillary SLN sampling (70). However, most studies done using radiocolloid and lymphoscintigraphy suggest that only perilesional injection provides an accurate depiction of extraaxillary drainage, especially to internal mammary (IM) nodes (68). Studies have shown that approximately 15%−20% of lesions that are not in the upper outer quadrant drain to IM lymph nodes after perilesional injection (71).
The importance of sampling IM nodes is a point of considerable debate (72). Some studies using SLN mapping and lymphoscintigraphy to sample IM lymph nodes showed more than 80% successful sampling of IM nodes when lymphoscintigraphy showed drainage and an approximately 10%−20% positivity rate (73–75). However, routine sampling of IM nodes results in less than a 5% overall rate of positive IM nodes, and it is rare to have IM lymph node metastasis in the absence of axillary nodal metastases (76). As a result, most practices in the United States do not routinely sample IM nodes. With an increasing trend toward intradermal or subareolar injection, spurred by more rapid drainage and a higher success rate (69), along with a trend toward less lymphoscintigraphy because of simplicity and lower expense (18), the sampling of IM nodes using SLN mapping methods is unlikely to be widely used. However, some studies have suggested that knowledge of IM drainage patterns, even without nodal sampling, may provide useful information. Yao et al. (77) found that patients with positive axillary nodes and IM nodal drainage were significantly more likely to relapse and die of breast cancer than those without drainage. Another study found a higher rate of nodal relapse outside the axilla, versus in the axilla, after sentinel node biopsy (78). Such studies prompt careful consideration of the approach to SLN mapping in breast cancer and the potential benefit of perilesional injection and lymphoscintigraphy in selected patients.
18F-FDG PET for Axillary Disease.
Many early studies of 18F-FDG PET for breast cancer were focused on detecting axillary metastases (79). These studies showed sensitivities of largely 85%−90% and higher (79,80), suggesting the feasibility of 18F-FDG PET as a noninvasive method for axillary staging and potential substitute for axillary nodal dissection. However, the population of patients in these earlier studies was heavily weighted toward more advanced breast cancer than found in typical screened populations.
More recent studies with a larger fraction of T1 primary cancers demonstrated lower sensitivities for axillary nodal metastases, as low as 20%−30% (40). These studies also indicated that the sensitivity of 18F-FDG PET for axillary nodal metastases depended on both axillary tumor burden and 18F-FDG uptake in the primary tumor. In a prospective multicenter trial representing one of the largest patient cohorts so far (81), 18F-FDG PET was performed on 360 women with newly diagnosed invasive breast cancer, and the results were interpreted by 3 experienced readers in a masked manner. The PET results were compared with those of pathologic analysis of axillary nodes. Overall, 18F-FDG PET was 61% sensitive and 80% specific for axillary metastases, with a positive predictive value of 62% and a negative predictive value of 79%. Patients who had false-negative PET results had significantly smaller and fewer tumor-positive lymph nodes than true-positive cases.
These results indicate the limitation of 18F-FDG PET in detecting micrometastases and small tumor-infiltrated axillary lymph nodes. Further studies comparing 18F-FDG PET with SLN biopsy support SLN biopsy for early-stage disease and confirm the limited sensitivity of 18F-FDG PET for axillary nodal metastases in this clinical setting (a sensitivity as low as 20%−40%), particularly in small (ranging from 1 to 15 mm) and isolated lesions (40,82). Thus, 18F-FDG PET is not sufficiently accurate to replace SLN biopsy in patients with early-stage breast cancer.
18F-FDG PET may, however, have a clinical role for patients with a high likelihood of axillary metastases, such as those patients with locally advanced disease, and for patients with advanced axillary disease, plexopathy, or symptomatic metastases (Fig. 3) (83). Although SLN biopsy is highly sensitive for axillary metastases in early breast cancer and well tolerated by patients, it requires a prolonged surgical session, lymphoscintigraphy, a considerable pathologic work-up, and additional cost. If some of the patients with axillary metastases could be identified before the SLN biopsy, axillary lymph node dissection may be performed directly without SLN biopsy. To identify the patients with axillary metastases, some have suggested the use of 18F-FDG PET, directed ultrasound with ultrasound-guided biopsy, or a combination of both. For 18F-FDG PET, most of the studies demonstrate specificities in the range of 93%−100% (40,84). The high specificity of 18F-FDG PET could direct the subgroup of patients with axillary disease determined by 18F-FDG PET to targeted sampling (e.g., by ultrasound) or to axillary lymph node dissection and avoid the need for SLN biopsy. This approach has been previously suggested and supported by several studies (65,84–88).
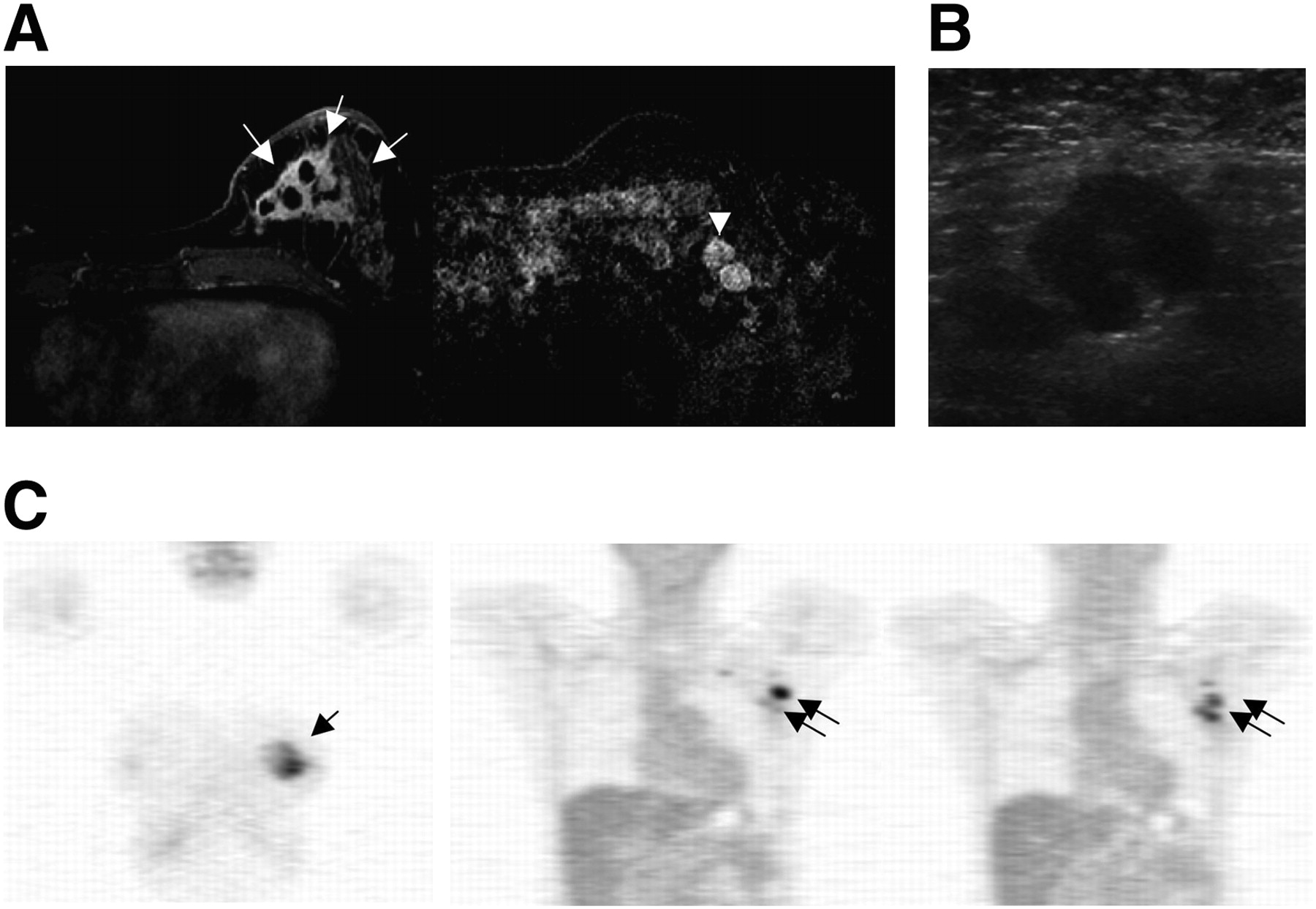
Examples of LABC and regional nodal staging (A–C). Contrast-enhanced MRI (A) demonstrates large breast cancer in left breast (arrows) and abnormally enhancing, rounded lymph nodes in the left axilla (arrowhead). Ultrasound (B) shows rounded lymph node with eccentric cortical thickening and deformed fatty hilum in the left axilla, suspected of being metastasis. Coronal PET images (C) reveal 18F-FDG uptake in primary tumor (arrow) and axillary lymph nodes (double arrows), confirmed by axillary lymph node biopsy.
Axillary ultrasound and needle biopsy are also helpful and commonly used to identify and sample suspected lymph nodes. Ultrasound features for suspected axillary lymph nodes include asymmetric cortical thickening or lobulations, loss of fatty hilum, abnormal shape (rounded appearance), and increased peripheral flow (89). Ultrasound-guided needle biopsy is simple, relatively easy, minimally invasive, and safe (89). Direct visualization of the tumor cells by fine-needle aspiration and cytology or core-needle biopsy and histology confirms axillary metastatic disease and avoids the need for SLN biopsy for confirmation of axillary nodal disease before definitive axillary treatment. Axillary ultrasound to direct needle biopsy of palpable disease is widely used, and some early studies support the use of ultrasound to screen for metastases in patients at high risk for axillary disease based on primary tumor characteristics (90,91). However, the sensitivity of axillary ultrasound is not as good as that of full nodal sampling and histologic examination; thus, histologic confirmation of a negative axilla by nodal sampling is needed if the ultrasound-guided needle biopsy is negative (91).
Other approaches, including MRI and ultra-small superparamagnetic iron oxide particles, have also been applied to breast cancer axillary nodal staging with promising early results (92), but these approaches are at an early stage of testing. For the immediate future, it appears unlikely that any noninvasive imaging method will provide the same sensitivity as that of SLN biopsy. Thus, SLN biopsy will likely remain the procedure of choice for the staging of axillae, ultrasound the procedure of choice for the sampling of palpable nodes or screening of high-risk axillae, and 18F-FDG PET an adjunct tool for high-risk patients and for advanced or recurrent axillary disease, possibly in conjunction with MRI (93).
18F-FDG PET for Other Regional Lymph Nodes.
18F-FDG PET may be helpful in assessing breast cancer spread to regional nodal sites outside the axilla, especially the IM chain. Although IM nodal metastases indicates a higher likelihood of spread or recurrence, these sites are not routinely sampled or evaluated in any systemic fashion in current clinical practice because of their relative inaccessibility and lack of convincing data for improvement in overall survival rate (72). 18F-FDG uptake in the IM node has been reported in some of the studies that have focused on detection of primary or axillary staging, showing IM nodal uptake as high as 25% (94). Moreover, some reports have suggested that IM 18F-FDG uptake predicts treatment failure patterns of disease consistent with IM nodal involvement and progression (95).Tran et al. showed that the likelihood of an extraaxillary lymph node finding on 18F-FDG PET was affected by the position of the tumor (medial vs. lateral). The presence of extraaxillary nodal uptake on 18F-FDG PET, combined with medial tumor location, indicated a high risk of subsequent disease progression (96). A preliminary study by Jones et al. showed the feasibility of detecting IM nodal metastases in early-stage patients using 18F-FDG PET (97), although more data are required to further validate the results.
Distant (Systemic) Staging
Indications and Standard Approach.
The presence of distant metastases, outside the breast and regional nodes, is an important factor predicting prognosis and directing the intensity of care, because metastatic (stage IV) breast cancer has a low likelihood of cure. Because of the low yield, cost, and distress associated with investigating detected abnormalities that are—for the most part—false-positives, baseline systemic staging is neither performed nor recommended (54) before surgery and axillary staging in patients with early-stage breast cancer (56,98,99). In the patients with more advanced disease (such as LABC or inflammatory breast cancer), however, some evidence supports the use of systemic imaging staging at the diagnosis to rule out stage IV disease, which would significantly alter treatment options because of the high likelihood of distant metastases (30,100). Baseline systemic imaging staging needs to survey the chest, abdomen, pelvis, and bones and includes chest radiography or CT, abdominal ultrasound or CT, and bone scintigraphy. According to current National Comprehensive Cancer Network Practice guidelines (54), only chest radiography is recommended for stage I disease, and additional bone scintigraphy may be considered for node-positive stage II disease. However, chest radiography or CT and liver ultrasound or CT may be optionally included for stage II disease with positive lymph nodes and a high index of suspicion. A combination of these standard systemic imaging modalities (typically abdominal CT, bone scanning, and possible chest and pelvis CT) are indicated for stage III disease or higher. 18F-FDG PET or PET/CT is recommended as an option for patients with either recurrent or stage IV disease in earlier breast guidelines and recent PET-specific guidelines (101).
Bone Scintigraphy and Fluoride PET.
Bone is the most common site for breast cancer metastasis, and bone metastases will develop in 30%−85% of patients with metastatic breast cancer during the course of disease (102,103). Bone also represents the first site of metastasis for 26%−50% of patients with metastatic breast carcinoma (103,104). Bone metastases in breast cancer can be osteoblastic (bone formation), osteolytic (bone resorption), or mixed lesions. Up to half of all bone metastases from breast cancer tend to show osteolytic changes. Breast cancer preferentially metastasizes to the spine and pelvis, followed by ribs, skull, and femur (103).
Whole-body bone scintigraphy, namely bone scanning, is the most commonly used method of detecting bone metastases (103). This method shows an increase in osteoblastic activity and vascularity (103,105). The most commonly used radiopharmaceutical is 99mTc-methylene diphosphonate or -hydroxymethylene diphosphonate. The reported sensitivity ranges from 62% to 100%, and specificity ranges from 78% to 100% (103,106). Although a bone scan is generally considered sensitive for detecting bone metastases at reasonable cost, it has low specificity and high false-positive rates because several other diseases such as trauma, degenerative change, or inflammation can mimic bone metastases. False-negative results can occur in the presence of predominantly osteolytic metastases, low bone turnover, or avascular regions (such as necrosis) (103). Anatomic imaging modalities such as CT and MRI provide correlative imaging. CT is particularly useful in evaluating the risk of fracture when the index of suspicion is high. MRI and 18F-FDG PET are useful in evaluating predominantly osteolytic lesions (107,108).
Another way to improve the specificity of bone scanning is to perform additional SPECT studies (109). SPECT is particularly helpful in characterizing solitary lesions in the spine or in differentiating bone metastases from degenerative lesions. For example, if radiotracer uptake is seen in the middle or posterior part of the vertebral body, then the lesion is likely a metastasis rather than a degenerative lesion. Savelli et al. reported the sensitivity and specificity of SPECT to be over 90%, similar to that of MRI studies, although MRI can effectively visualize predominantly lytic lesions as well as blastic lesions (109).
Some studies have examined the use of fluoride (18F−) PET for bone metastases detection and have shown 18F− PET to be superior to bone scanning and SPECT in detecting metastases and differentiating malignant from benign lesions (110–112). The mechanism of localization of fluoride in bone and uptake in bone metastases is similar to that of diphosphonates in that both are deposited in newly mineralizing bone accompanying osteoblastic activity (108). 18F−, compared with 99mTc-labeled conventional bone-scanning agents, has higher bone uptake and faster blood clearance and, combined with the favorable imaging performance of PET, results in a superior target-to-background ratio (108). 18F− PET and PET/CT have been shown to be more accurate than bone scanning for the detection of both osteolytic and osteoblastic lesions in various malignancies including breast cancer and have been suggested as an alternative to bone scanning, mainly in patients at high risk for metastatic bone disease (110,111). Schirrmeister et al. found more metastatic lesions on 18F− PET, compared with bone scanning with additional SPECT, resulting in a change in clinical management in 12% of patients (110). Subsequent prospective studies also demonstrated similar results, although the study population was the group of patients with lung cancer bone metastases. Schirrmeister et al. reported that bone scanning identified 5 of 12 patients, bone scanning with SPECT identified 10 patients, and 18F− PET identified 12 patients (113). A larger-scale study by Hetzel et al. also demonstrated bone scanning and SPECT identified 29 of 33 patients with bone metastases found by spine MRI, and 18F− PET found 31 of 33 patients (114). The authors also found that bone scanning and SPECT, compared with 18F− PET, underestimated the extent of disease in 16 patients. Even-Sapir et al. showed further improved sensitivity for 18F− PET/CT versus PET (111). Although recent studies have successfully shown that 18F− PET has higher diagnostic accuracy in the assessment of bone metastases, longstanding familiarity with bone scanning, concerns for the cost of 18F− PET, and a lack of data on the clinical impact of improved diagnostic accuracy of 18F− PET, compared with bone scanning, have somewhat limited the use of 18F− PET, but its use can be expected to increase with more experience and data.
18F-FDG PET and PET/CT.
The reported sensitivities and specificities of 18F-FDG PET for the detection of distant metastases range from 80% to 100% and from 50% to 97%, respectively (115).
In one of the earliest studies of 18F-FDG PET for staging of systemic breast cancer, Moon et al. evaluated 18F-FDG PET performed in 57 patients with suspected recurrent or metastatic breast cancer and demonstrated that this modality was 93% sensitive and 79% specific (116). 18F-FDG PET, compared with conventional imaging modalities, was also reported to be more sensitive; Mahner et al. showed that 18F-FDG PET was 87% sensitive and 83% specific, whereas combined conventional imaging modalities were 43% sensitive and 98% specific (117). Thus, 18F-FDG PET detected more metastatic lesions than did other imaging modalities including CT and could be helpful by detecting occult metastases that were not otherwise detected in conventional imaging modalities, affecting and changing therapeutic options (Fig. 4).

Examples of systemic staging for breast cancer. 18F-FDG PET/CT demonstrates metastatic disease in left breast extending to chest wall, axillary, supraclavicular, cervical, IM, mediastinal, and hilar nodes (A); areas of abnormal uptake are indicated by arrows. For patient in B, 18F-FDG PET/CT shows extensive nodal metastases in axillary, mediastinal, cervical, and retroperitoneal locations. In patient with recurrent breast cancer in C, initial contrast-enhanced CT image (top left) revealed pericardial effusion and thickening. Subsequent 18F-FDG PET/CT scan (remaining images), obtained without intravenous contrast 3 days later and after pericardiocentesis, shows focal hypermetabolic activity corresponding to pericardial thickening, consistent with pericardial metastases (white arrows and arrowheads). Foci of hypermetabolic activity in both IM and subcarinal lymph nodes (black and blue arrows) are seen, as are bilateral pleural effusions (stars).
The additional sensitivity of 18F-FDG PET/CT for regional nodes and distant disease may be particularly important in staging for LABC. LABC (including a primary tumor larger than 5 cm; skin or chest wall involvement; fixed axillary nodes; positive supraclavicular, infraclavicular, or IM nodes; and inflammatory cancer) has a poor prognosis because of the high incidence of distant metastases during follow-up (118). Currently, the standard approach is neoadjuvant chemotherapy followed by surgery with axillary nodal dissection and radiation. However, some patients with apparent LABC may have occult distant metastases, in which case aggressive therapies with curative intent may not be indicated. Thus, detecting distant metastases in the patients with LABC is crucial for determining treatment. Evidence supports the utility of 18F-FDG PET in LABC at diagnosis. Several studies showed detection rates of confirmed metastatic disease in LABC at diagnosis ranging from 8% to 14% (119–121). 18F-FDG PET is particularly helpful in detecting IM and mediastinal nodal metastases (95,122). These are common sites for metastatic involvement in LABC and are not optimally evaluated with conventional imaging alone. 18F-FDG PET and PET/CT can improve staging and alter therapeutic options in patients with LABC and locoregional recurrence.
18F-FDG PET and PET/CT are helpful in the detection of skeletal metastases but have an important difference from bone scanning and fluoride imaging. Several studies demonstrated that 18F-FDG PET is superior to bone scanning in the detection of lytic and intramedullary metastases but inferior in the detection of primarily osteoblastic lesions. Cook et al. showed that 18F-FDG PET detected lytic metastases often missed by bone scanning, whereas 18F-FDG PET often missed osteoblastic metastases, for which bone scanning is superior (107). Subsequent studies confirmed these findings (40,108). Therefore, 18F-FDG PET complements bone scanning. In standard clinical practice, the combination of bone scanning and CT remains the standard imaging modality when staging is clinically indicated, and 18F-FDG PET and PET/CT are particularly helpful in clarifying difficult or equivocal cases. Ongoing studies will continue to clarify the best use of 18F-FDG PET/CT for staging of systemic breast cancer.
CONCLUSION
Breast cancer is a common disorder in women and a leading cause of death. Imaging plays an important role in the detection, diagnosis, staging, and response evaluation of breast cancer. Radiotracer imaging methods play an important current role in breast cancer staging and response evaluation, including SLN mapping, bone scintigraphy, and 18F-FDG PET/CT. Ongoing trials of dedicated devices for primary tumor imaging using breast-dedicated PET and SPECT may lead to increased use for primary tumor diagnosis and determination of the extent of disease in the breast; however, more studies are needed. Radionuclide imaging plays an important role in axillary staging through its contribution to SLN mapping. Noninvasive methods for axillary nodal detection such as 18F-FDG PET/CT appear to be relatively insensitive for early-stage disease but can play an important role in determining the extent of nodal involvement for more advanced breast cancer, especially LABC. Radionuclide imaging plays an important role in distant metastasis staging for breast cancer patients with locally advanced, recurrent, or metastatic disease. Part 2 of this review will highlight the application of radionuclide imaging to breast cancer response evaluation and targeted breast cancer therapy.
Acknowledgments
We acknowledge the help of Erin Schubert, Lisa Dunnwald, and Lanell Peterson with capturing the images used in the figures and the support of the molecular imaging and breast cancer groups at the University of Washington and Seattle Cancer Care Alliance. This work was supported in part by National Institutes of Health grants CA42045, CA72064, CA90771, and CA124573.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH APRIL 2010.
-
David Mankoff has indicated he receives scientific study/trial support from Pfizer and GE Healthcare. No other potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.
- 87.
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.
- 121.↵
- 122.↵
- Received for publication September 6, 2008.
- Accepted for publication December 23, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes
- Breast Imaging Devices for Nuclear Medicine
- [18F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography in Breast Cancer: When... and When Not?
- Breast Cancer Survivorship and Surveillance
- A Bridge Not Too Far: Linking Disciplines Through Molecular Imaging Probes