


Abstract
Recent studies have shown that vasodilator-induced ischemic electrocardiographic (ECG) changes have incremental prognostic value over normal SPECT myocardial perfusion imaging (MPI) and identify patients at higher risk for cardiac events. The prognostic value of vasodilator-induced ischemic ECG changes in the setting of normal PET MPI has yet to be determined. We sought to determine the prognostic importance of dipyridamole-induced ischemic ECG changes in patients with normal 82Rb PET myocardial perfusion images. Methods: Between 2000 and 2003, 2,029 consecutive patients undergoing dipyridamole stress 82Rb PET at the University of Ottawa Heart Institute were evaluated. Patients with normal PET MPI and interpretable ECGs were enrolled. Electrocardiograms were assessed for ST depression or elevation and patients were categorized into those with and without dipyridamole-induced ischemic ECG changes. Images were graded using the 17-segment model. Follow-up information was obtained by telephone interview, from hospital records, or from treating physicians. All cardiac events (cardiac death, nonfatal myocardial infarction [MI], percutaneous coronary intervention, coronary artery bypass grafting, or angiography) were verified with hospital records. Results: Of the 629 enrolled patients with normal PET MPI, 72 patients had dipyridamole-induced ischemic ECG changes. There was no significant difference between the 2 groups in the combined endpoint (cardiac death, nonfatal MI, and revascularization) at follow-up (mean ± SD, 27.1 ± 13 mo). There were no cardiac deaths in either group. One (1.4%) patient with ischemic ECG changes had a nonfatal MI (0.6% annual event rate). Two (2.8%) patients with ischemic ECG changes required revascularization compared with 11 (2.0%) in the nonischemic ECG group. Conclusion: Normal 82Rb PET confers an excellent prognosis regardless of dipyridamole-induced ST depression.
Dipyridamole- or adenosine-induced ischemic electrocardiographic (ECG) changes are specific for severe coronary artery disease (CAD) and predict adverse cardiac events (1–6). Previous studies have shown that normal SPECT myocardial perfusion imaging (MPI) confers an excellent prognosis with an annual cardiac event rate of <1% (7,8). However, 2 recent studies have demonstrated that patients with normal SPECT MPI but with vasodilator-induced ST depression have significantly increased cardiac events (9,10).
PET has very good diagnostic sensitivity and specificity (89% and 86%, respectively) for CAD (8) and may identify patients with abnormal perfusion not visually present with 99mTc SPECT MPI (11). It is unknown whether dipyridamole-induced ischemic ECG changes have incremental prognostic value in patients with normal 82Rb PET MPI.
MATERIALS AND METHODS
Study Population
Reports of all consecutive patients at the University of Ottawa Heart Institute undergoing clinical dipyridamole stress 82Rb PET MPI between January 2000 and September 2003 were reviewed. Patients over the age of 18 y and with “normal” 82Rb PET MPI (as interpreted by a nuclear cardiologist) were eligible for inclusion. All eligible patients had their perfusion images reviewed by 2 experienced observers who were unaware of clinical data. Patients were enrolled if both observers agreed that the MPI was qualitatively normal. Disagreements in MPI interpretation were resolved by consensus.
Enrolled patients had their rest and stress ECGs reviewed by the same expert observers. Patients were excluded if the PET MPI was abnormal or if there was ECG evidence of a Wolf–Parkinson White pattern, a left bundle branch block, or a ventricular paced rhythm. For patients with more than one PET study, the date of the first normal dipyridamole 82Rb PET MPI was used.
All patients gave informed consent to participate and the protocol was approved by the University of Ottawa Heart Human Research Ethics Board.
Dipyridamole Stress 82Rb PET
Rest Image Acquisition.
Patients abstained from caffeine, xanthine derivatives, and atrioventricular nodal blocking drugs for ≥12 h and fasted (except for medications) for ≥6 h before the study. Each patient was positioned in the Siemens/CTI ECAT ART whole-body scanner equipped with 24 detector rings, allowing the acquisition of 47 contiguous transaxial slices (12). A 4-min 137Cs transmission scan was acquired to confirm proper patient positioning and for attenuation correction (13,14). After the transmission scan, 5–15 MBq/kg of 82Rb were infused over 30 s at rest followed by saline flush (1 min) using a custom infusion system (15). Approximately 2.5 min after tracer infusion, a static emission scan was acquired for 7.5 min.
Dipyridamole Stress Image Acquisition.
Dipyridamole was administered intravenously (0.14 mg/kg/min for 5 min). Eight minutes after initiation of dipyridamole infusion, 5–15 MBq/kg 82Rb were administered and static uptake images were acquired as described. Aminophylline (2 mg/kg) was infused 12 min after initiation of dipyridamole infusion. After dipyridamole stress imaging, a 4-min transmission scan was acquired for attenuation correction of the stress data (16).
Transaxial images were reconstructed using filtered backprojection with an 18-mm Hann window of the ramp filter, then reoriented into short-axis sections, and displayed in a standard format (8).
Image Interpretation
All PET images were reviewed by 2 experienced observers. Visual analysis of myocardial perfusion used a 17-segment model and a 5-point grading system (0 = normal radiotracer uptake, 1 = mildly reduced, 2 = moderately reduced, 3 = severely reduced, and 4 = absence of radiotracer uptake) (17). The sum stress score (SSS), sum rest score (SRS), and sum difference score (SDS) were calculated.
ECG Interpretation
All ECGs were interpreted using the recommended criteria from the American College of Cardiology and American Heart Association practice guidelines for exercise testing (18). Ischemic ST depression was defined as horizontal or downsloping ST depression of ≥1.0 mm at the J point that was sustained for 80 ms or upsloping ST depression of ≥1.5 mm at 80 ms beyond the J point. ST elevation was present if ≥1.0 mm was present at the J point and was sustained for ≥60 ms. Disagreements were resolved by consensus.
Patient Follow-Up
Patient follow-up was performed through telephone interviews, hospital records, local death records, and referring physicians. Information collected included cardiac death, nonfatal myocardial infarction (MI), revascularization (coronary artery bypass grafting [CABG], and percutaneous coronary intervention [PCI]), and coronary angiography. All data were confirmed with hospital records.
Statistical Analysis
Continuous measures are presented as mean ± SD. The Wilcoxon signed rank test was used to test univariate relationships between continuous measures and ECG groups. Categoric measures are presented as counts with percentages. The Fisher exact test was used to test univariate relationships between categoric measures and ECG groups. Survival estimates were described with Kaplan–Meier curves and compared with the log-rank test. All tests used P < 0.05 for the critical value of statistical significance. Analyses were performed using SAS version 8.02.
RESULTS
Between January 2000 and September 2003, 2,029 patients had dipyridamole stress 82Rb PET MPI at the University of Ottawa Heart Institute. A total of 93 patients were excluded for a left bundle branch block or paced rhythm (90 patients), age <18 y (2 patients), and a Wolf–Parkinson White pattern (1 patient). Of the remaining 1,936 patients, 694 had a normal myocardial perfusion scan, of which 74 patients had ischemic ECG changes and 620 patients did not. Total follow-up was 90.6% with 65 patients refusing the study or lacking follow-up information. Thus, the study was comprised of 629 patients (with follow-up data): 72 (11.4%) patients had ischemic ECG changes and 557 patients had no ischemic ECG changes. Two of 65 patients without follow-up data had ischemic ECG changes and the remaining 63 patients had no ischemic ECG changes.
The baseline characteristics of the patients with and without dipyridamole-induced ischemic ECG changes were compared (Table 1). Dipyridamole-induced ECG changes were more commonly seen in women (83% and 70%; P < 0.03) but there was no significant difference in the other baseline characteristics.
Patient Demographics
Rest and Dipyridamole Stress 82Rb PET
Patients with ischemic ECGs had higher heart rates and blood pressures at rest and with stress (Table 2). However, there was no significant difference in the SSS, SRS, and SDS between the 2 groups (Table 2). All patients with dipyridamole-induced ischemic ECG changes had horizontal or downsloping ST depression. None of the patients had abnormal upsloping ST depression, ST elevation, or arrhythmia with dipyridamole stress. Of the 72 patients with dipyridamole-induced ST depression, 29 (40%) patients had ST depression of 1.0 mm, 34 (47%) patients had ST depression of 1.1–1.9 mm, and 9 (13%) patients had ST depression of ≥2.0 mm. Fifty-seven (79%) patients had ST depression in multiple leads.
Rest and Dipyridamole Stress 82Rb PET in Patients With and Without Ischemic ECG Changes
Cardiac Events
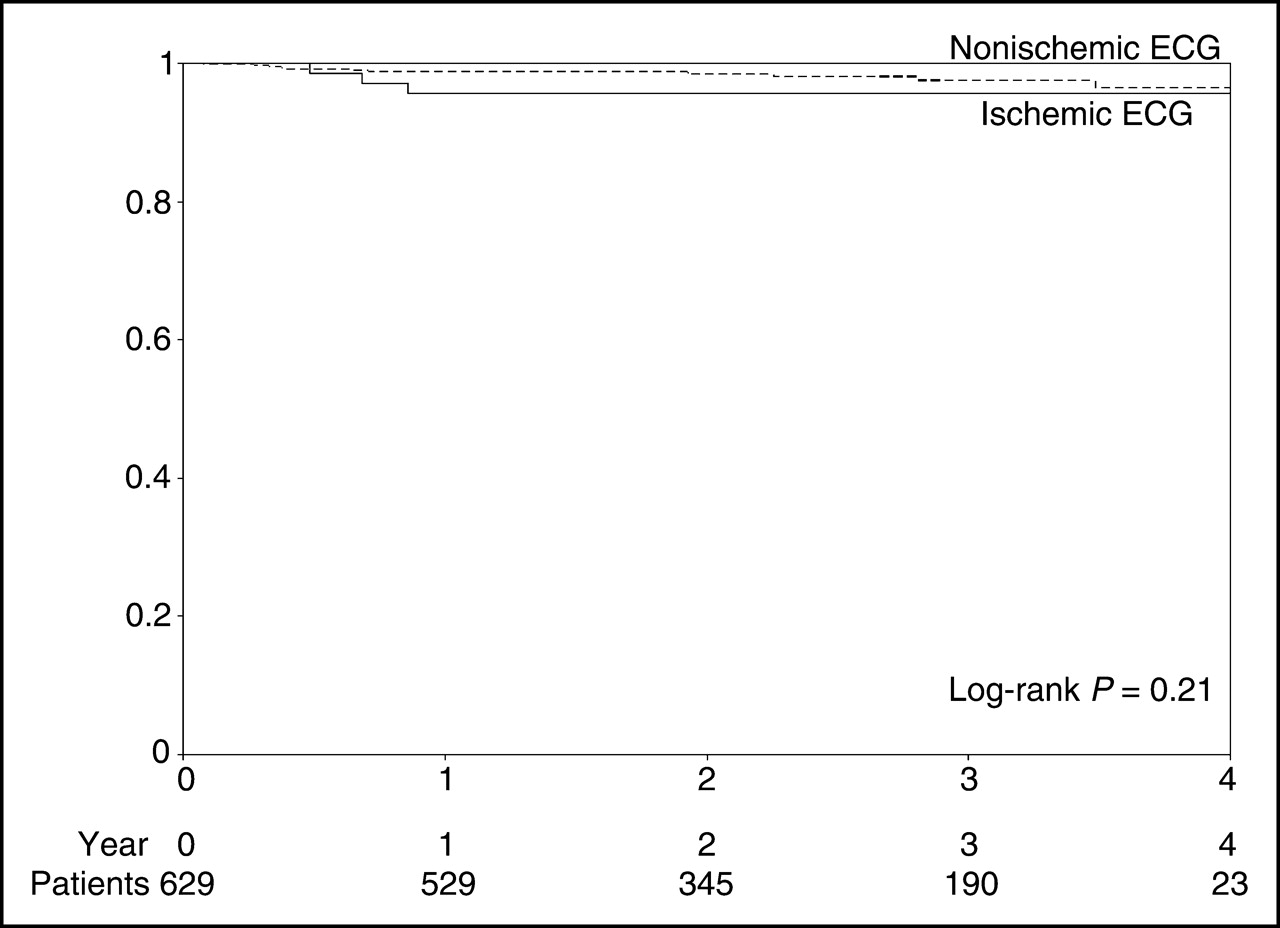
During the mean follow-up duration of 27.1 ± 13.0 mo, there were no cardiac deaths and only 1 nonfatal MI. The total event rate for cardiac death and nonfatal MI in our patient population (normal 82Rb PET MPI) was 0.2%. There was no significant difference in the incidence of cardiac death, nonfatal MI, revascularization, or coronary angiography between the 2 groups (Table 3). In the ischemic ECG group, 1 (1.4%) patient had a nonfatal MI and 2 (2.8%) patients required revascularization. In the nonischemic ECG group, there were no cardiac deaths or nonfatal MIs. Eleven (2.0%) patients required revascularization. There was no significant difference in the composite endpoint (cardiac death, nonfatal MI, and revascularization) between the 2 groups (4.2% and 2.0%; P = NS) (Fig. 1). Patients with ischemic ECG changes had an annual event rate of 0.6% for cardiac death and nonfatal MI and 1.9% annual event rate for cardiac death, nonfatal MI, and revascularization. Cardiac events in the ischemic ECG group were not predicted by the severity of ST depression or the number of leads with ST depression.
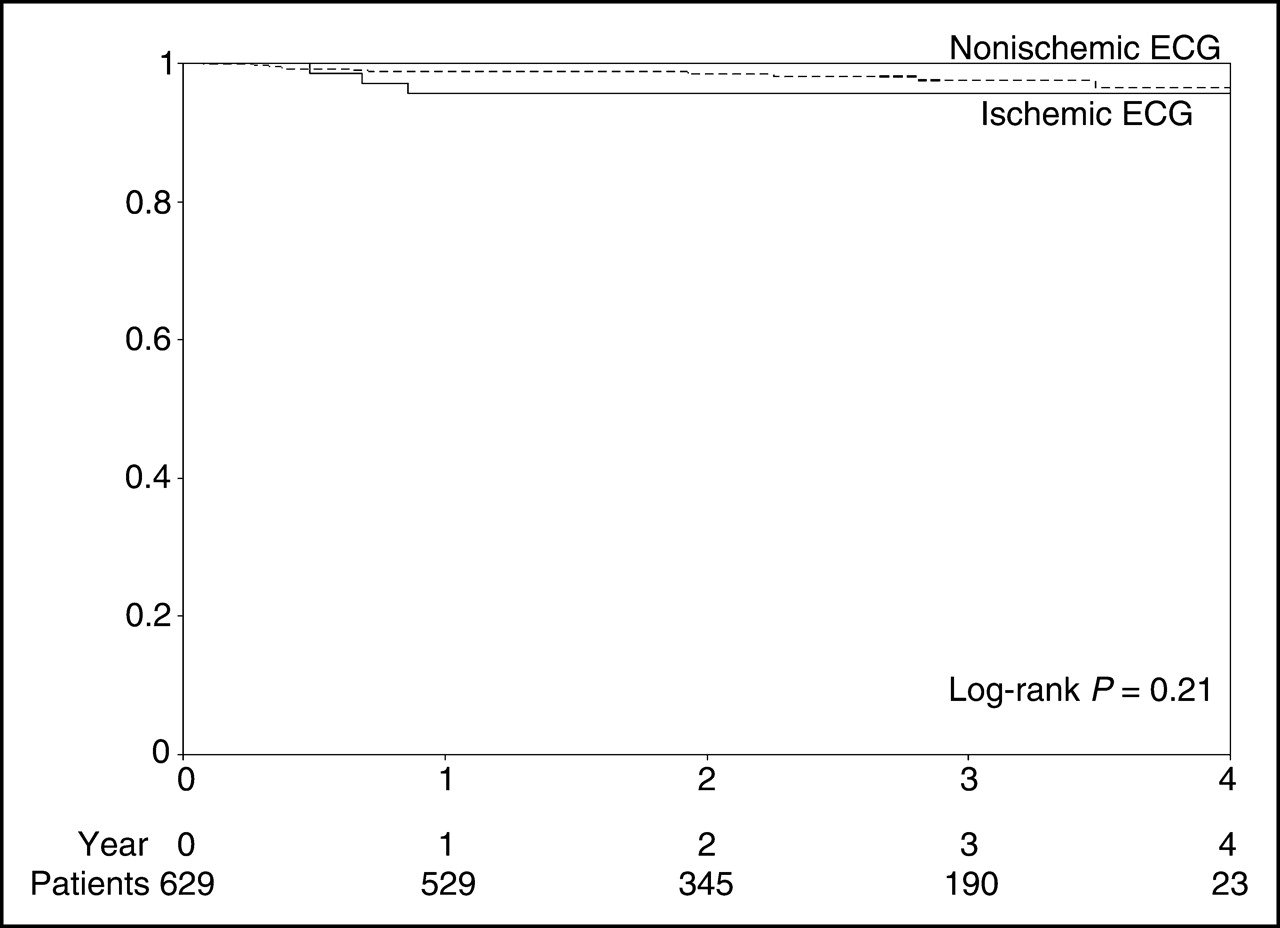
Kaplan–Meier survival curve for cardiac death, nonfatal MI, and revascularization.
Cardiac Events
DISCUSSION
These data demonstrate that normal 82Rb PET MPI portends a good prognosis irrespective of dipyridamole-induced ECG changes. Patients with dipyridamole-induced ischemic ECG changes and a normal 82Rb PET MPI have a low annual event rate for cardiac death, nonfatal MI, or revascularization.
Exercise-induced ST depression has a specificity of 77% for significant CAD (19). Clinicians often disregard exercise-induced ST depression if SPECT MPI is normal. However, it has been demonstrated that vasodilator-induced ST depression is 91% specific for reversible perfusion defects (6). Until recently, the clinical significance of vasodilator-induced ST depression and normal SPECT MPI was unclear.
Overall, patients with normal SPECT MPI have an annual mortality rate of <1% (7,20–22). Patients with normal adenosine SPECT have a slightly higher annual cardiac event rate (0.7%) compared with those patients undergoing exercise stress (0.4%) (7). However, patients with normal SPECT MPI but with vasodilator-induced ST depression had an approximately 5% annual rate for cardiac death and nonfatal MI (9). A similar study by Abbott et al. confirmed a high cardiac death and nonfatal MI rate in patients with ischemic ECGs (10.6%) compared with controls (1.5%) at 29 ± 12 mo follow-up (10). In the same study, the cardiac death, nonfatal MI, and revascularization rate was 24.2% compared with 4.0% in the control group.
Our study demonstrates patients with normal 82Rb PET have good prognosis regardless of ECG changes. Studies evaluating the overall prognostic value of PET are limited. Marwick et al. noted that defect severity with PET was related to outcome (23). Preliminary data from our group support these findings (24). The current study extends these observations to the ECG changes in a population of patients with normal PET perfusion. The incremental value of the ECG observed in SPECT studies is not observed with negative (or “low-risk”) PET MPI.
Dipyridamole-Induced ST Depression
The enrollment of patients with “false-positive” vasodilator-induced ST depression may dilute the “true-positive” patients at higher risk for cardiac events. A higher incidence of false-positive stress-induced ECG changes may occur in women and in patients with hypertension.
It is accepted that women are more likely to have false-positive ST depression with exercise stress. Our results and those of Klodas et al. suggest that women were more likely to develop dipyridamole-induced ECG changes (9). The mechanism by which exercise induces ST depression in women is unknown but may be due to a greater catecholamine release (25), hormonal differences, or microvascular dysfunction (26). A similar mechanism with vasodilator stress may increase the prevalence of false-positive ST depression in women.
Our patients with ischemic ECG changes had higher heart rates and blood pressure at rest and with stress (Table 2). It has been hypothesized that heart rate, hypertension, and left ventricular hypertrophy may play a role in vasodilator-induced ECG changes (10,27–29). These findings may also account for false-positive ST depression.
Comparison with Previous Studies Using SPECT MPI
Klodas et al. (9) and Abbott et al. (10) have each performed similar studies with SPECT MPI. Both groups demonstrated that vasodilator-induced ischemic ECG changes had incremental prognostic value over normal SPECT MPI. In spite of our patient population being similar to those of these previous studies (Table 4), our event rates appear much lower (Table 5).
Baseline Characteristics of Patients with Vasodilator-Induced ST Depression
Cardiac Events in Patients with Vasodilator-Induced ST Depression and Normal MPI
The difference between our study and the previous SPECT studies may be attributable to the overall improved sensitivity of PET (8). Go et al. have previously demonstrated that 82Rb PET is more sensitive than 201Tl SPECT (93% and 76%) for the detection of CAD (11). Another possible explanation is that PET may have accuracy superior to that of 99mTc SPECT in patients with small hearts. It has been previously demonstrated that the diagnostic accuracy of SPECT may be reduced in women and in patients with small hearts due to γ-camera resolution (30,31). Our study, as well as those of Klodas et al. (9) and Abbott et al. (10), demonstrated that ischemic ECGs and normal MPI occurred more commonly in women. In our study, an analysis of body mass index was performed and no significant difference was found between the 2 groups. However, further analysis revealed that our patients with ischemic ECGs had a smaller mean body surface area (1.8 ± 0.2 vs. 1.9 ± 0.3 m2; P < 0.01) and were shorter (162.2 ± 8.3 vs. 166.0 ± 10.0 cm; P < 0.01). The results of the current study may suggest that the diagnostic accuracy in patients with small hearts is maintained by PET.
The higher cardiac event rates seen in patients with vasodilator-induced ST depression and normal SPECT MPI may be attributable to triple-vessel disease or balanced ischemia. However, in our study, all 3 patients with ischemic ECG changes and cardiac events underwent coronary angiography and only 1 patient (with previous CABG) had significant triple-vessel disease.
Limitations
This was a single-center retrospective study and was subject to selection bias. The 2 previous SPECT studies by Klodas et al. (9) and Abbott et al. (10) were also retrospective studies of similar design and would potentially have been subject to similar bias.
It is difficult to make direct comparisons between our study and the 2 previous SPECT studies because there may be significant differences in patient populations. Studies have demonstrated that patients undergoing pharmacologic stress have a higher mortality than those who undergo exercise stress MPI (7). Previous vasodilator SPECT MPI studies may have enrolled higher risk patients because lower risk patients underwent exercise stress SPECT MPI. Since all PET patients underwent dipyridamole stress (without the option of exercise stress), it is possible that our PET population was of lower risk than those in the vasodilator SPECT studies. We do not believe that this is the case. At our institution, PET patients are almost exclusively referred by cardiologists, who typically see a higher risk patient population. It is also possible that PET MPI was performed in patients with an “equivocal” SPECT MPI. Women with a breast attenuation artifact on SPECT were referred for PET, thus accounting for the higher prevalence of women with normal PET MPI. Our population, compared with that of the 2 previous SPECT studies, shared a similar prevalence of CAD, MI, and revascularization.
Our sample size, though larger than that of similar previous SPECT studies, was small and was not adequately powered to assess a statistically significant difference between the 2 groups. Our event rate in the ischemic ECG group was very small and no definitive conclusions can be made regarding the effects of hypertension or sex. However, we can conclude that normal PET (regardless of ECG changes) confers a good prognosis.
The annual rate for cardiac death, nonfatal MI, and revascularization in patients with ischemic ECGs (1.9%) appears higher than that of patients without ECG changes (0.9%), but this difference was not statistically significant. There were very few cardiac deaths and nonfatal MIs in our study, but it is possible that a difference does exist between the 2 groups. To detect a statistically significant difference between the 2 groups, a sample size of >4,000 patients (with normal MPI and interpretable ECGs) would be required. On the basis of our results, 11,350 patients would have to undergo dipyridamole 82Rb PET MPI before normal PET MPI could be achieved in 4,000 patients.
Sixty-five (9.4%) patients refused to participate in the study or were lost to follow-up. The baseline characteristics of the patients without follow-up were compared with those with follow-up information (Tables 6 and 7). Patients without follow-up were younger, more commonly men, and less likely to be dyslipidemic.
Patient Demographics: Patients Lost to Follow-Up or Refused to Participate in Study
Rest and Dipyridamole Stress 82Rb PET in Patients With and Without Follow-Up
Although 9.4% of patients refused or were lost to follow-up, we were able to obtain follow-up in 97.3% of patients with ischemic ECG changes; therefore, we do not believe that we have significantly underestimated the risk in this population. Follow-up in the nonischemic ECG group was lower (88.7%) and could result in either an underestimation or an overestimation of the true cardiac event rate. Marwick et al. studied the incremental value of 82Rb PET and determined that normal 82Rb PET had an annual mortality rate of 0.9% (24). This mortality rate in Marwick’s study was higher than that of our study and, since each event was confirmed with hospital records, we do not believe that the cardiac events have been overestimated. If our study has underestimated the cardiac events in the nonischemic ECG group, the difference in cardiac event rates between the ischemic and nonischemic ECG groups would have been smaller and less significant.
Our study population did not undergo SPECT MPI but we did compare our patient population with the patient population of the 2 previous SPECT studies (9,10) and they appeared similar. Though the results are hypothesis generating, this study raises that possibility of PET MPI being used to further risk stratify patients with normal SPECT but with vasodilator-induced ST depression (Table 4). Future studies are required to confirm our findings. A prospective study enrolling patients with vasodilator-induced ST depression and normal 99mTc SPECT MPI who undergo further risk stratification with 82Rb PET may confirm our results.
CONCLUSION
The excellent prognosis of normal 82Rb PET is maintained regardless of dipyridamole-induced ST depression.
Acknowledgments
The authors extend their gratitude to May Aung, Jane Baker, Laurie Bennet, Margaret Berry, Kristine Black, Manon Blais, Sandina Cordani, Kim Gardner, Debbie Gauthier, Linda Garrard, Lyanne Golanowski, Karen Mostert, and Kate van den Broek for preparation of the data and the manuscript. This project was supported in part by grants from the Canadian Institute for Health Research, the Heart & Stroke Foundation of Canada, and the Ontario Research and Development Challenge Fund. Further support was received by the International Fellowship Program at the University of Ottawa and the International Fellowship at Uehara Memorial Foundation, Japan.
Footnotes
Received Dec. 23, 2004; revision accepted Mar. 23, 2005.
For correspondence or reprints contact: Benjamin J.W. Chow, MD, University of Ottawa Heart Institute, 40 Ruskin St., H1-PET Centre, Ottawa, Ontario, Canada, K1Y 1W2.
E-mail: bchow{at}ottawaheart.ca
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Competency-Based Medical Education: Do the Cardiac Imaging Training Guidelines Have it Right?
- Prognostic Value of PET Myocardial Perfusion Imaging in Obese Patients
- Myocardial perfusion scintigraphy: past, present and future
- Establishing the Prognostic Value of Rb-82 PET Myocardial Perfusion Imaging: A Step in the Right Direction
- Reducing Radiation Dose in Rest-Stress Cardiac PET/CT by Single Poststress Cine CT for Attenuation Correction: Quantitative Validation
- Positron emission tomography and molecular imaging
- Frequent Diagnostic Errors in Cardiac PET/CT Due to Misregistration of CT Attenuation and Emission PET Images: A Definitive Analysis of Causes, Consequences, and Corrections
- The Year in Cardiac Imaging
- What is the Prognostic Value of Myocardial Perfusion Imaging Using Rubidium-82 Positron Emission Tomography?