


Abstract
Involuntary patient motion from insufficient patient preparation may lead to local misregistration of PET/CT images and, thus, can invalidate the attempt to fuse the resulting images. We estimate the efficacy of selected patient support structures in reducing the likelihood of patient motion in the area of the head and neck during whole-body PET/CT studies. Methods: Motion of the head and neck was estimated in 51 healthy volunteers during simulated whole-body PET/CT studies using an infrared camera–based tracking system. Four patient positioning schemes (arms down) were studied, with the neck placed on a standard PET head holder with no support at the sides (setup A), on a special head holder fitted with a subject-specific mold from construction foam (setup B), on a vacuum-lock bag (setup C), and on a special head holder fitted with a vacuum-lock bag (setup D). We report the average motion of the head and neck as the difference in the position of a set of target points between the simulated CT image and PET image of the head and neck. To estimate the efficacy of additional patient support measures in clinical practice, we reviewed the misregistration of the head and neck in whole-body PET/CT studies of 10 patients each who were imaged using setups A and C by comparing the mean translational and rotational alignment parameters from a semiautomatic linear registration approach needed to realign the CT and PET images. Results: Average translational and rotational misalignment of the head and neck was highest for setup A, at 7 mm and 1°, respectively. Misalignment was reduced to a minimum of 1.4 mm and 0.3° for setup D. Setup B resulted in a similar reduction in patient motion of the head and neck: 2.4 mm and 0.4°, whereas setup C provided only somewhat improved support, with a resulting average misalignment of 4.5 mm and 0.7°. In clinical PET/CT, we found setup C to reduce translational misalignment of the CT and PET images of the head and neck to 2 mm, compared with 6 mm for setup A, whereas no significant reduction of rotational misalignment was observed. Conclusion: Average motion of the head and neck in unrestrained subjects during whole-body PET/CT examinations can be reduced by use of rigid positioning aids, such as foam molds, or vacuum-lock bags. Vacuum-lock bags are reusable, quickly adaptable, and olfactory neutral and can be used routinely, either alone or in combination with a head holder, in whole-body PET/CT for high-quality examinations.
The combination of anatomic and molecular information, such as that from CT and PET, has been shown to hold potential for an improved diagnosis in clinical oncology (1–3). The concept of combined PET/CT was first proposed a few years ago (4). Initial PET/CT studies demonstrated the feasibility of acquiring CT and PET data on the same patient during a single scanning session. Such data can provide better intrinsic spatial correspondence than can similar datasets acquired on different tomographs at different times (5,6).
Nevertheless, spatial coregistration throughout the extended coaxial imaging range is sometimes compromised by involuntary patient motion during the combined examination. Respiratory motion, for example, has been shown to potentially yield CT and PET data that are misregistered in anatomic regions of high mobility, such as the lower thorax and the diaphragm (7–9). If significant, this misregistration can propagate through CT-based attenuation correction into a biased tracer distribution (7,9,10).
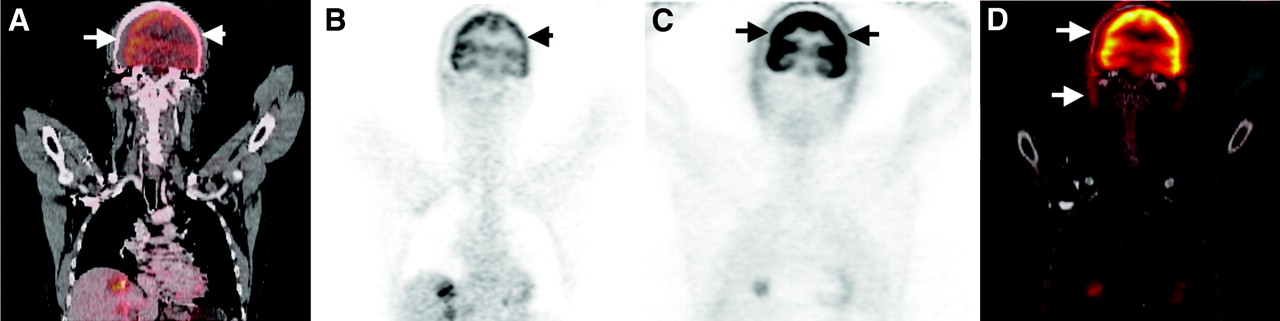
Involuntary patient motion may also be due to relaxation of muscles during the combined examination, which takes about 20–35 min for a whole-body (WB) acquisition (11,12). The likelihood of muscle relaxation increases with scanning time; therefore, body regions such as the head and neck, with the largest time differences between the CT and the PET portions, are prone to misregistration (Fig. 1).

(A) Limited coronal view of WB FDG PET/CT study with severe misalignment (arrows) in area of head and neck. (B and C) PET image after CT-based attenuation correction (B) demonstrates biased FDG uptake (arrow), which appears normal on uncorrected PET image (C). (D) Fused CT and uncorrected PET illustrate magnitude of misalignment.
Hypothetically, however, adequate patient positioning and added patient support can minimize misregistration of PET/CT datasets and, as a consequence, improve the accuracy of diagnostic information. In this study, we evaluated the magnitude and frequency of misalignment in the area of the head and neck on WB PET/CT studies for a variety of patient-positioning schemes.
MATERIALS AND METHODS
Simulated WB PET/CT Scans
Because we lacked a PET/CT tomograph with accurate motion tracking at the time of the study, we simulated a series of WB PET/CT examinations on a standard PET tomograph, an ECAT EXACT HR+ (CPS Innovations) (13) equipped with an infrared motion-tracking system (14).
We assume a standardized WB PET/CT acquisition protocol (12), with patients being positioned headfirst supine in the scanner, with the neck centered inside the gantry (Fig. 2A). First, a topogram was acquired, followed by a spiral CT scan in the craniocaudal direction (0 ≤ t ≤ tCT, where t = scan time and tCT = time at the end of the CT scan). The patient was then moved toward the rear of the gantry, where a multibed PET emission scan commenced with retracing of the imaging range in the craniocaudal direction. We assumed a coaxial imaging range of 8 bed positions with an emission scan time of 3.5 min per bed position. Therefore, the neck of the subject was back in the original position inside the gantry after about 30 min. Figure 2B illustrates the position of the subjects with respect to the coordinate system of the motion-tracking device.
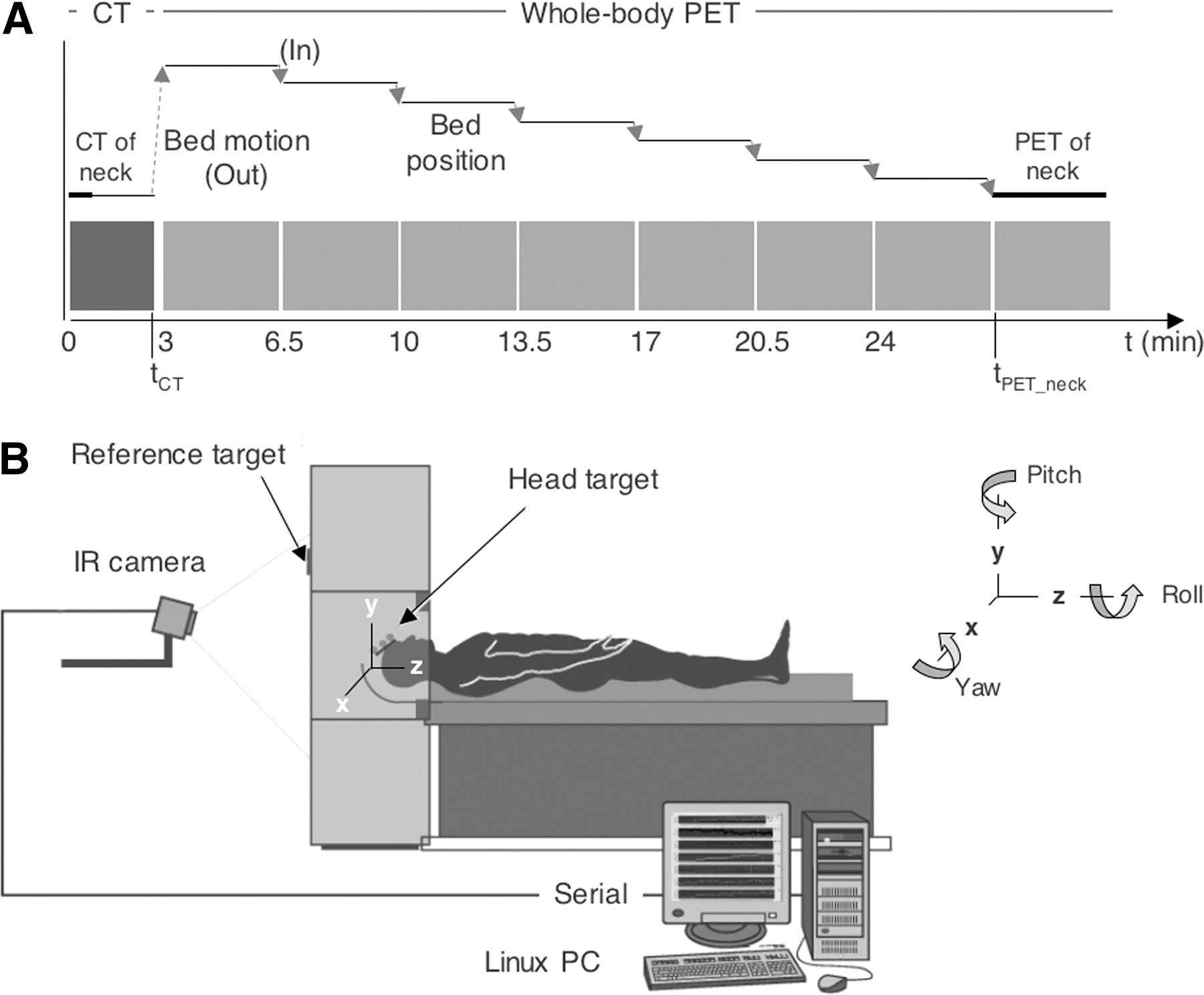
(A) Timeline of simulated WB PET/CT study and bed motion. Each plateau represents physically stationary bed position; connecting arrows indicate bed motion. (B) Drawing illustrates arrangement of motion-tracking device with coordinate system for monitoring misregistration of head and neck by means of 3 rotational and 3 translational parameters. IR = infrared.
Neck Support
This study included 51 healthy volunteers (40 male and 11 female). All were positioned with 1 of the 4 different support structures for the head and neck. For setup A (10 subjects), a disposable, cotton-filled cushion of 25 × 40 × 5 cm was used. This cushion supported the neck and lower head (Fig. 3A) and was placed on a standard ECAT head holder made of carbon fiber.
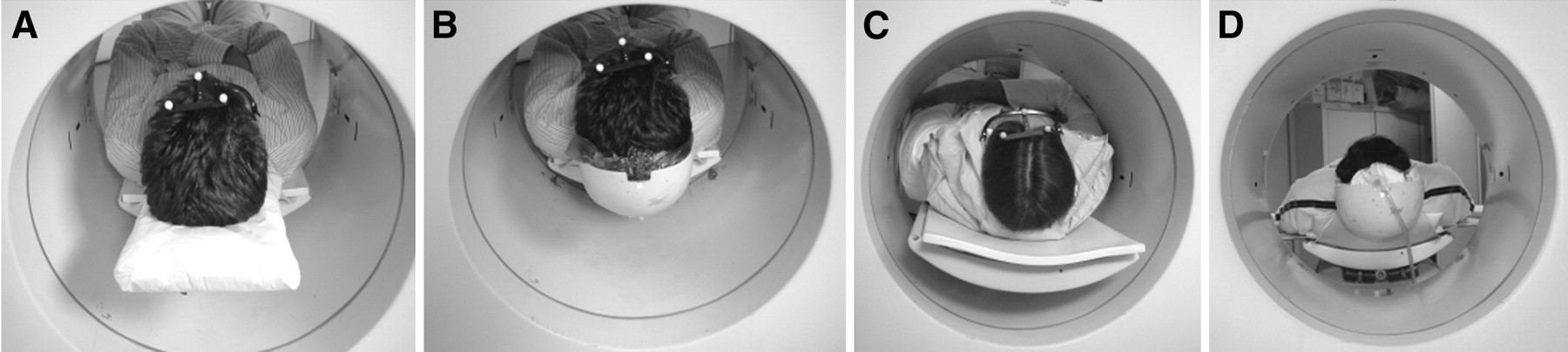
Supports for head and neck in simulated WB PET/CT studies: disposable cushion (A), head holder with disposable construction-foam insert (B), vacuum-lock bag (C), and smaller vacuum-lock bag (D) inside head holder shown in B. Photographs were taken from rear of PET tomograph used for simulations.
For setup B (17 subjects) a modified head holder was used in combination with a custom-made mold of construction foam (Fig. 3B). The left and right sides and the tip of the head holder were curved halfway up to the level of the ears and the cranium. A nonleaking plastic bag was filled with the construction foam (2K; Ultrament GmbH) and fitted between the subject’s head and the inside of the head holder (Fig. 3B). Hardening of the construction foam took less than 2 min, and the subject’s head was held in place by a trained technologist during that time. The foam support was disposed of after the study.
For setup C (12 subjects), subjects were placed on a foam bean bag (MED-TEC). This type of support is also referred to as vacuum-lock bag since an attached pump is used to extract the air from the bag, thus providing an adaptable and reusable patient support for single-time or repeated scanning in a fixed position. In our study, the vacuum-lock bag was butterfly-shaped, 45 × 60 × 2 cm, and filled with 2-mm diameter foam pellets of a low density. First, the bag was slightly filled with air and fitted to the subject’s neck. The technologist then extracted the air from the bag via the attached electric pump, while the cushion was supported further and fitted more tightly to the neck and lower head (Fig. 3C). Because this vacuum-lock bag did not fit into the curved head holder used for setup B, it rested on the pallet without further restraints.
Setup D (12 subjects) combined setups B and C. A reusable small (35 × 60 × 1 cm) vacuum-lock bag (Fig. 3D) was custom-made (Additec GmbH) for the Institute of Medicine in Jülich to replace the disposable construction-foam supports (Fig. 3B). The small vacuum-lock bag was also placed inside the curved head holder (B).
None of the volunteers was claustrophobic or had undergone a WB PET or PET/CT study before. At a mean age of 27 y, volunteers for this simulation study were younger than the general oncology patients referred to the participating PET/CT site (University Hospital Essen). Similar to patients undergoing standard clinical PET/CT, the subjects in this study were asked to remain still for the entire simulated scan procedure.
Infrared Camera to Track Patient Motion
An optical tracking system (Polaris; Northern Digital) was used to monitor the position of the head and neck during the simulated scan. The tracking device used infrared light to monitor the location of several passive, reflective markers. The device consisted of a camera (emitter and receiver) that was mounted behind the PET tomograph facing the rear gantry (Fig. 2B), a set of 3 target markers, and another set of reference markers. The reference markers were mounted on the rear of the gantry and remained stationary inside the active area of the camera. The 3 nonstationary, reflecting target markers were mounted on a plastic frame that attached to a pair of plastic goggles. All subjects were asked to wear those goggles fitted tightly against their head and supported by their nose and ears, with the marker points held in place just above the top of their head, while they faced the infrared camera (15). The active field of measurement of the tracking device was 100 cm, starting 85 cm from the infrared camera. The manufacturer quotes a tracking accuracy of 0.35 mm root mean square within this range.
Estimating Motion of Head and Neck in WB PET/CT Studies
All volunteers were positioned head-first, supine, with their arms down, with their legs resting on a low-density support, and with their head and neck centered inside the field of view of the tomograph. The bed position was fixed during the first 2.5 min to simulate the topogram and spiral CT scan (Fig. 2A), which was assumed to correspond to the time needed to acquire a topogram and a spiral CT scan as part of the clinical PET/CT examination (tCT). With the subject lying still, the bed was then moved out of the tomograph by 21 cm to simulate the first bed position (lower pelvis). The bed was moved back in by 3 cm after every 3.5 min, to simulate the duration of an individual bed position, until, at 27.5 min (tPET_neck), the subject’s head was back in the original position. The distance of the simulated bed steps was chosen such that the target points were always in the active field of view of the infrared tracking system.
Motion of the head and neck was estimated for each subject from the difference in the position of the 3 target points at the time of the last bed position (neck), at tPET_neck, with respect to the initial position at tCT. The absolute difference, that is, the PET/CT misregistration, was reported in 3 rotational and 3 translational components. The 3 rotational parameters are the pitch, yaw, and roll, which describe the rotation around the y-, x-, and z-axes, respectively (Fig. 2B). The 3 translational displacements, Δx, Δy, and Δz, were measured in the x, y, and z directions, respectively.
Motion of the marker points was tracked for all subjects in the 4 different positioning scenarios (Fig. 3A–Fig. 3D). For each positioning scenario, we report the mean of the absolute rotational (pitch, yaw, roll) and translational displacements (Δx, Δy, Δz). For each subject in setups A–D, we calculated the absolute displacement, Δr, as the square root of the sum of the squared translational displacements Δx, Δy, and Δz and report the mean of the individual Δr values, <Δr>, for setups A–D. Similarly, we report the mean of the average rotational displacements, <rot>, for setups A–D.
RESULTS
Figure 4 shows the rotational and translational displacement of the reference markers between the CT and the PET portions of the simulated WB PET/CT scan for the 4 positioning schemes (setups A–D). The misregistration between the CT and the PET images of the head and neck was largest for subjects in setup A, in which the neck was supported only by a cotton-filled cushion placed on the head holder. With all other additional support structures (setups B–D), overall displacement of the head and neck was less than for setup A. The rotational and translational displacements of the reference markers, representing the PET/CT misregistration of the head and neck, averaged over all subjects in each setup (A–D) are listed in Table 1.

Boxcar plots for PET/CT misregistration in the 3 translational (Δx, Δy, Δz) and 3 rotational (pi, pitch; ya, yaw; ro, roll) parameters for subjects in setup A, head holder (A); setup B, head holder with construction foam (B); setup C, vacuum-lock bag (C); and setup D, head holder with vacuum-lock bag (D).
Average (±SD) Absolute Displacement (Rotation [Pitch, Yaw, Roll] and Translation [Δx, Δy, Δz]) of Reference Markers for Subjects in Groups A–D
We estimate a mean rotation of 1.0° and a mean translation of 7.0 mm of the reference markers for setup A. Use of the curved head holder with the disposable construction foam insert (setup B) significantly reduced motion of the head and neck between the simulated CT and PET examinations (Student t test, P < 0.05) around the y- and z-axes, that is, pitch and roll, but not around the x-axis (yaw) (P = 0.1). In addition, misregistration was reduced significantly along the x- and y-axes but not along the main scanner axis (z) (P = 0.07). Use of the reusable vacuum cushion without any additional restraints (setup C) produced a statistically significant reduction in misalignment of the head and neck only for the rotation around the main scanner axis (roll) and for vertical translation (y-axis). When the disposable foam insert of setup B was replaced with the smaller vacuum bag of setup D, motion of the head and neck was reduced significantly in all directions except for the rotation around the x-axis (yaw) (P = 0.07).
Overall, the mean rotational displacement was reduced to 0.4° (P < 0.05), 0.7° (P = 0.1), and 0.3° (P < 0.05) for setups B, C, and D, respectively, compared with 1° for setup A. The respective average translational displacements, <Δr>, were 2 mm (P < 0.05), 4 mm (P = 0.06), and 1.4 mm (P < 0.05), compared with 7 mm for setup A.
DISCUSSION
We estimated the efficacy of 4 head and neck support schemes during simulated WB PET/CT examinations. Our results indicated that, among the different positioning devices, a curved head holder fitted with a custom-made vacuum-lock bag appeared most effective in reducing involuntary motion of the head and neck (Fig. 3). This observation was limited somewhat by the assumption that there was no relative motion of the head and neck and that both could be regarded as rigidly joined for the purpose of this study. Because none of the positioning devices used in this study preferentially supported the head or the neck, we believe that the 3 target markers attached to the head of the subjects were sufficient to track motion of the head and neck.
Within this limitation, we were able to show that misregistration of the head and neck was largest when patients were positioned without restraint of the area of interest (setup A). The measured average translational and rotational misalignment was 7 mm and 1°, respectively, and the maximum was 12 mm and 2°, respectively, with a large spread of head-and-neck motion in the vertical direction (Δy) (Table 1 and Fig. 4A). Motion of the head and neck was reduced significantly when the curved head holder was combined with the custom-fitted foam insert (setup B). The resulting average translational and rotational misalignment was only 2 mm and 0.4°, respectively, with a maximum misalignment of 8 mm or 1° in different subjects. However, this setup was ineffective in reducing the translational misregistration along the main scanner axis, as indicated by the relatively large spread in Δz (Fig. 4B). It appears likely that the neck was restrained insufficiently as a result of a nonevenly distributed foam support, with more volume being pushed into the head holder than below the neck in front of it, thus indicating the importance of careful patient positioning even with additional positioning aids at hand.
By comparison, the butterfly-shaped vacuum-lock bag of setup C reduced, in particular, the roll rotation around the main scanner axis z and the translation along the anteroposterior direction (Δy). The efficacy of setup C can be explained by the support volume that extends even beyond the bilateral boundaries of the curved head holder in setup B and thus reduces both the misregistration and the intersubject variability of the misregistration around the main scanner axis z (Fig. 4C). Nevertheless, combination of the curved head holder and the vacuum-lock bag (setup D) resulted in the most significant and least variable reduction in translational and rotational misalignment (Table 1), because of the particularly rigid encasement of the head and neck at either side of the lower head and along the entire axial range of the head and neck (Fig. 3).
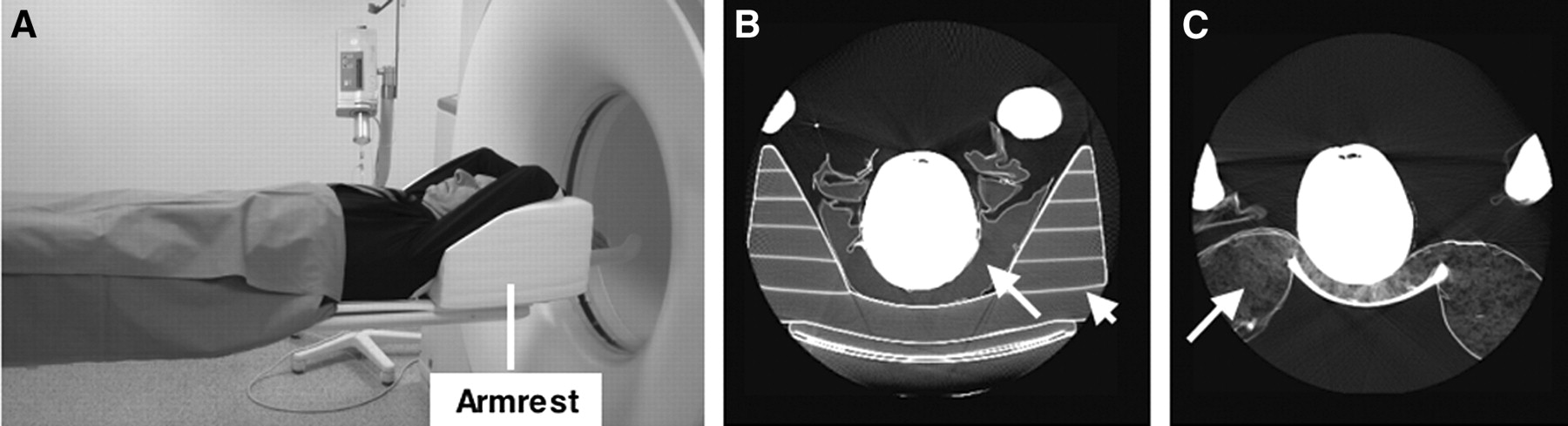
In practice, however, similarly curved head holders are not available commercially. To evaluate the efficacy of a versatile patient-positioning scheme in clinical PET/CT practice, we propose combining a generic arm support (Fig. 5A) made of semirigid foam (MED-TEC) and the vacuum-lock bag from setup C. In combination with the custom-fitted vacuum-lock bag, which is placed between the neck of the patient and the foam-based armrest (Fig. 5B), a potentially effective support of the head and neck for lengthy WB PET/CT studies might be provided.
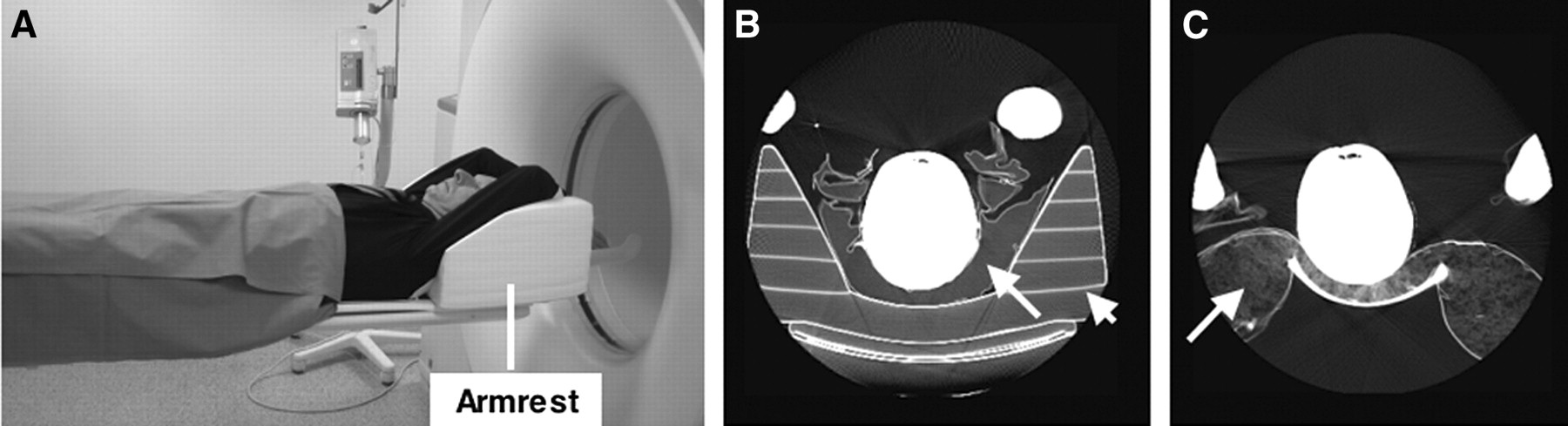
(A) Patient positioning in clinical PET/CT scanner with armrest to support arms above head during combined scanning. (B and C) Axial CT images (windowed) illustrate patient positioning with vacuum-lock bag (arrow) placed inside armrest (arrowhead) (B) and with head supported by cushion (arrow) placed in front of armrest (C). Measured CT attenuation values of cushion, armrest, and vacuum-lock bag were −970 HU, −900 HU, and −940 HU, respectively.
This hypothesis was tested in clinical practice on groups of 10 patients referred for a WB PET/CT study. In group 1, patients were positioned with their head resting on a cushion and their arms raised above the head and supported only by the arm support (Fig. 5C) for the 30-min duration of the combined examination (12). Patient positioning in group 2 was the same, except the head was positioned with the vacuum-lock bag from the volunteer study (Fig. 3C). All patients were scanned on a commercially available PET/CT tomograph (Biograph Emotion Duo; Siemens Medical Solutions).
Because motion of the head and neck could not be monitored in real time, we evaluated the misalignment of the head and neck on the reconstructed WB images. We extracted sets of contiguous axial CT and PET images that covered the range from the tip of the cranium to the lower neck from the WB PET/CT image volumes. The resulting 20 subvolumes were transferred to a commercially available image registration platform (Fusion7D; Mirada Solutions). For each patient, automatic linear registration of the CT and PET volumes was performed, and the mean translational and rotational displacement of the PET images with respect to the CT images was calculated with reference to the center of the image volume. The difference in motion of the head and neck, that is, the displacement of the head and neck between the CT and PET portions of the combined examination, was accepted as a measure of the efficacy of the particular patient positioning.
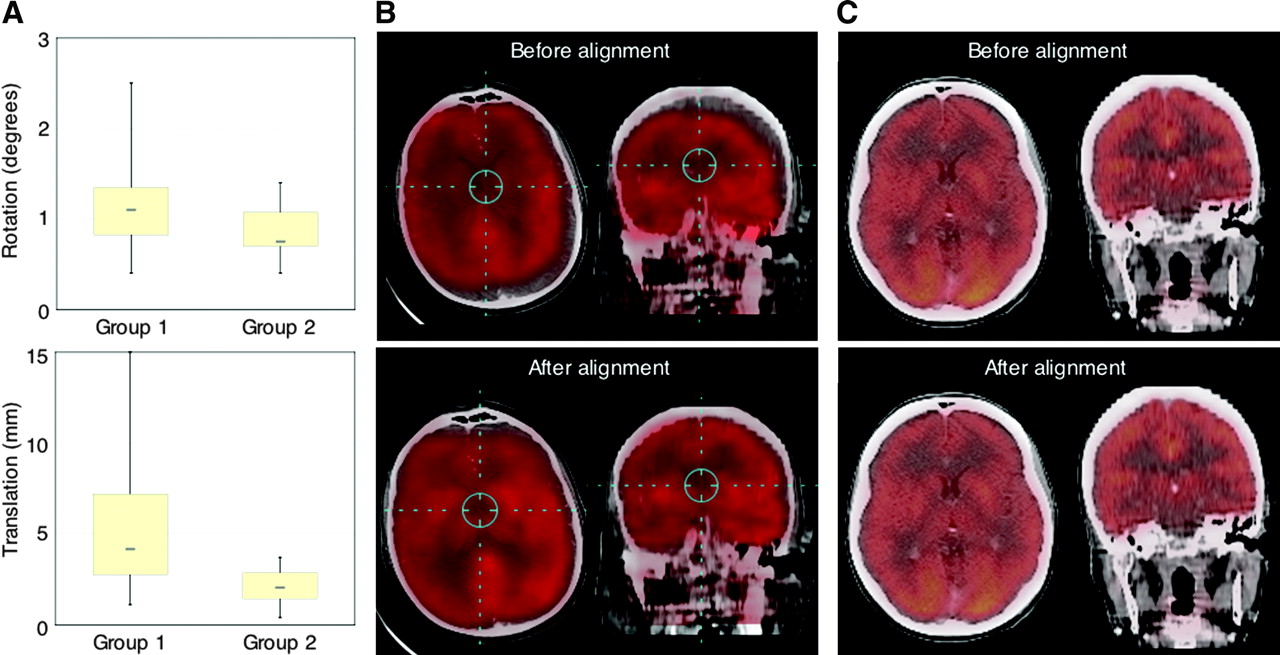
We found that the average rotational and translational displacement in group 1—with the armrest only—was 1.2° ± 0.6° and 6 ± 5 mm, respectively (Fig. 6A). This displacement was reduced in group 2—with the additional vacuum-lock support—to 0.9° ± 0.3° and 2 ± 1 mm, respectively. The reduction in translation was statistically significant (Student t test, P < 0.05). The maximum displacement was reduced from 2.5° and 15 mm in group 1 to 1.4° and 3.7 mm in group 2 (different subjects). Figures 6B and 6C show examples of fused PET/CT images of patients from group 1 and 2, respectively, before and after linear image registration.

(A) Boxcar plots of center-to-center misalignment of head and neck in WB PET/CT studies of patients with standard neck support (group 1) and with vacuum-lock support (group 2). (B and C) Examples of axial (left) and coronal (right) fusion images are shown before and after linear realignment for group 1 (B) and group 2 (C). Effect of realignment is significant in patients without head restraint (group 1) and less noticeable in group 2 because of better intrinsic patient positioning.
This clinical study validated our findings from monitoring patient motion in volunteers and supported the use of a vacuum-lock bag (in combination with an armrest). The main difference between the clinical and the volunteer study was the position of the arms. Keeping the arms above the head for PET/CT examinations is required to avoid serious streak artifacts on CT. In clinical practice, armrests are provided to allow patients to be more comfortable and thus reduce the likelihood of involuntary motion. An armrest could not be used in our volunteer study because most positioning schemes were based on a head holder that did not allow for the use of an additional armrest to keep the arms up (Fig. 3). Nevertheless, in both the volunteer and clinical study, additional head-and-neck restraints were shown to be effective in limiting local misalignment compared to unrestrained patients with the same position of the arms (up or down).
Adequate patient positioning in clinical routine requires support structures of low density, particularly when used in combination with CT equipment. All positioning aids in our simulation and clinical studies were of low CT density (−900 HU to −1,000 HU) and did not cause image artifacts. Short setup times are essential for routine use of positioning aids, to limit exposure of the staff to radiation from the injected patient. In our study, a single technologist could complete the patient setup in 4 min (setup B) or less, with an average setup time of 2 min.
Routinely applied patient supports should also be reusable and, if possible, adaptable to the patient. Although alignment was better with the construction foam (setup B) than with the vacuum-lock bag alone (setup C), the accumulated costs for using disposable foam-based positioning aids in a high-throughput scenario can be quite high. In contrast, vacuum-lock bags are reusable and can be tailored to specific needs, such as positioning the entire trunk or the neck only, by varying the size, packing fraction, and coating of the bags. Furthermore, vacuum bags do not cause discomfort to the patient. Although the cost of these bags may be offsetting, this cost may soon be justified in reasonable-throughput scenarios when compared with the cost of disposable foam inserts and the volume of waste they create.
Finally, our simulation and patient studies indicated that the accuracy of coregistration in the head and neck in WB PET/CT studies was more reliable when additional positioning aids were used. Any residual misregistration between CT and PET (as shown for the head and neck in this study) may partially invalidate PET/CT image fusion and propagate into a biased tracer distribution after CT-based attenuation correction. This motion-induced bias can be estimated from the effect of head motion on PET of the brain as shown by an independent study (15) that indicated visual and quantitative distortion of the recovered PET tracer distribution when the motion of the head exceeded one half the full width at half maximum of the spatial resolution of the PET scanner (16). Our clinical study showed that the mean misregistration in the head and neck could be reduced to 2 mm, which is less than the full width at half maximum of current WB PET tomographs. Nevertheless, when imaging of the head and neck is the primary objective, separate acquisition protocols for the neck and torso should be considered to help increase patient comfort and eliminate systematic artifacts, such as those caused by the position of the arms with respect to the CT field of view (12,17).
CONCLUSION
Average motion of the head and neck in unrestrained subjects during WB PET/CT examinations can be reduced by use of rigid positioning aids, such as foam molds, or vacuum bean bags. In this study, the use of subject-tailored foam molds together with a shell-type head holder was slightly more efficient than the use of a vacuum-lock bag without additional restraints. However, vacuum-lock bags are reusable, quickly adaptable, and olfactory neutral and therefore appear preferable among the positioning devices tested in this study, most likely in combination with a carbon-fiber head support or additional restraints.
Acknowledgments
We thank our technologists Nicole Boden, Janina Marchese, Slavko Maric, and Bärbel Terschüren for their assistance during these studies and Chandra Chatterjee, PhD, and Mirada Solutions for further support.
Footnotes
Received Sep. 1, 2004; revision accepted Dec. 8, 2004.
For correspondence or reprints contact: Thomas Beyer, PhD, Department of Nuclear Medicine, University Hospital Essen, Hufelandstrasse 55, D 45122 Essen, Germany.
E-mail: thomas.beyer{at}uni-essen.de
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Technical Considerations in Brain Amyloid PET Imaging with 18F-Florbetapir
- Value of a Lower-Limb Immobilization Device for Optimization of SPECT/CT Image Fusion
- Does Reducing CT Artifacts from Dental Implants Influence the PET Interpretation in PET/CT Studies of Oral Cancer and Head and Neck Cancer?
- Can PET/CT Replace Separate Diagnostic CT for Cancer Imaging? Optimizing CT Protocols for Imaging Cancers of the Chest and Abdomen
- Correction of Head Movement on PET Studies: Comparison of Methods
- Reply: Adequate Evaluation of Image Registration in Hybrid PET/CT.