


Abstract
As SPECT/CT technology evolves, its applications and indications need to be evaluated clinically for more efficient and cost-effective use. This retrospective study evaluated the clinical value of simultaneously acquired 99mTc-sestamibi SPECT/CT versus conventional SPECT in diagnosing and locating parathyroid adenomas or hyperplasia in patients with primary hyperparathyroidism. Methods: Immediately and 60 minutes after intravenous administration of 740–925 MBq of 99mTc-sestamibi, static planar images of the neck and chest were obtained. SPECT/CT images were acquired 30 minutes after injection. Two experienced masked readers independently evaluated whether conventional SPECT images provided information beyond what was available from the planar images either by changing the diagnosis or by better locating the glands and whether the SPECT/CT images provided information beyond what was available from the planar plus conventional SPECT images. Forty-eight consecutive patients with a clinical diagnosis of primary hyperparathyroidism were included in the study. The 32 whose scans showed positive results underwent surgical resection and were examined histopathologically. Results: Planar and SPECT imaging, with or without CT fusion, identified 89% of the surgically confirmed diseased parathyroid glands. Use of SPECT/CT changed the diagnosis in only 1 patient (2%) from positive to negative and better located the glands in only 4 patients (8%). SPECT/CT was particularly helpful in locating the 2 ectopic parathyroid adenomas diagnosed in this cohort. Tracer retention in diseased glands did not correlate with histologic characteristics. Also, biochemical markers did not correlate with the scan findings. Conclusion: SPECT/CT has no significant clinical value additional to that of conventional SPECT for parathyroid imaging except in locating ectopic parathyroid glands. Eliminating the CT acquisition will spare patients the additional time, radiation exposure, and expense.
Hyperparathyroidism, whether primary or secondary, is usually a clinical and chemical diagnosis (1). Preoperative imaging procedures are used to identify and accurately locate the affected parathyroid gland or glands (2). Radionuclide scintigraphy has proved to be a reasonably accurate method for locating parathyroid adenoma or hyperplasia (3–5). It can be performed using the dual-phase 99mTc-sestamibi (6) or 99mTc-tetrofosmin (7) imaging techniques. Alternatively, the subtraction imaging technique can be performed using either 99mTc-pertechnetate and 201Tl or 99mTc-sestamibi (8) or 99mTc-tetrofosmin and 99mTc-pertechnetate or 123I (9). Multiple methods to improve the identification of diseased parathyroid glands have been attempted. Some investigators have emphasized the importance of the addition of lateral views to the dual-phase 99mTc-sestamibi technique to better locate the affected gland (10). The addition of SPECT to radionuclide scintigraphy has been proven to increase the sensitivity and accuracy of locating abnormal glands (11–13). Static and SPECT imaging, using a pinhole collimator, has also been recommended by several research groups to better locate the glands (14,15).
Two recent case reports described the accurate location of ectopic parathyroid adenomas by fusing 99mTc-sestamibi SPECT and CT slices using fusion software (16,17). Kaczirek et al. have indicated the value of SPECT/CT acquisition using γ-camera–mounted anatomic x-ray tomography in 4 patients with ectopic parathyroid adenomas (18).
As SPECT/CT evolves, its applications and indications need to be evaluated clinically for more efficient and cost-effective use. To our knowledge, no studies have used a large number of patients to evaluate the clinical value of simultaneous SPECT and CT image acquisition using γ-camera–mounted anatomic x-ray tomography to locate parathyroid adenoma or hyperplasia. Our goal in this study was to evaluate the additive value of SPECT images to planar images and of SPECT/CT images to planar plus SPECT images. We hypothesized that fused SPECT/CT would provide additional information for diagnosing and locating parathyroid adenomas or hyperplasia.
MATERIALS AND METHODS
After obtaining Institutional Review Board approval, we included 48 consecutive patients with primary hyperparathyroidism who underwent SPECT/CT parathyroid imaging between May and November 2003. There were 32 women and 16 men, with a mean age of 58.2 y (range, 28–83 y).
Image Acquisition
The patients received 740–925 MBq (20–25 mCi) of 99mTc-sestamibi by intravenous injection. Anterior planar images of the neck and chest were obtained immediately after the injection and 60 min later, each for 10 min, using a high-resolution low-energy parallel-hole collimator and a large-field-of-view dual-detector γ-camera with a mounted CT scanner (Hawkeye; General Electric Medical Systems). SPECT and CT images of the same area were obtained at 30 min after injection over a 360° arc, using 120 frames at 23 s per frame and 3° angles. The images were acquired into a 128 × 128 matrix and reconstructed using a 2-dimensional ordered-subset expectation maximization iterative technique (10 subsets and 2 iterations), both with and without CT-based attenuation correction and a Hanning 3-dimensional postfilter (cutoff frequency, 0.85 cycles/cm). The CT part was acquired at a slice step of 10 mm, a slice time of 14 s, a current of 2.5 mA, and a voltage of 140 kV. The SPECT acquisition took approximately 25 min, whereas the CT acquisition took approximately 10 min.
Image Interpretation
Two experienced nuclear medicine physicians interpreted the images. Each physician read the images independently while unaware of any clinical or radiologic information about the patients. The readers indicated whether the scan was negative or positive for locating the diseased parathyroid gland after reading the planar images alone, then the planar and SPECT images, and finally the planar and SPECT/CT images. Each reader had to respond to the following questions after SPECT and SPECT/CT interpretation: Did it change the diagnosis? Did it help in locating the gland? or Was it not helpful? Focal retention of tracer in abnormal parathyroid glands was visually compared between the early and the delayed images. Also evaluated were whether the thyroid gland had a normal or a multinodular appearance and whether the findings correlated with surgical and pathologic findings after surgical resection. We defined the identification rate as the percentage of diseased parathyroid glands, confirmed at surgery, to have been the glands identified at planar plus SPECT imaging, versus planar plus SPECT/CT imaging.
Biochemical Markers
The preoperative intact parathyroid hormone (PTH), free serum calcium (fCa), and total serum calcium (tCa) levels were also recorded to evaluate whether the scan findings and accuracy correlated with the level of biochemical markers. These levels were also recorded because their normalization indicated the adequacy and completeness of surgery.
Statistical Analysis
Interobserver agreement was evaluated using the McNemar test (P = 0.0 and κ = 1.0 indicate excellent agreement). The correlation between the chemical markers of primary hyperparathyroidism and the scan findings was evaluated using a paired Student t test with a significance level of P < 0.05.
RESULTS
All 48 patients underwent immediate and 1-h delayed planar imaging as well as SPECT/CT, except for 1 patient who did not undergo delayed planar imaging because of obvious findings on the early planar and SPECT/CT images. Three patients underwent additional delayed planar imaging 1.5–2.5 h after injection. Reader 1 interpreted 38 scans as positive for the presence of parathyroid adenoma, 2 as positive for ectopic parathyroid adenoma, and 8 as negative, whereas reader 2 interpreted 36 scans as positive for parathyroid adenoma, 2 as positive for ectopic parathyroid adenoma, and 10 as negative. In evaluations of the additive value of SPECT and SPECT/CT, the first reader found that SPECT was helpful for locating the gland in 9 patients (18.8%), caused a change in diagnosis in 11 patients (22.9%), and had no additive value to planar imaging in 28 patients (58.3%). The corresponding evaluations generated by reader 2 were 20 (41.7%), 12 (25%), and 16 (33.3%), respectively. In evaluating the additive value of SPECT/CT above planar plus conventional SPECT, reader 1 found that using SPECT/CT images changed the diagnosis for 1 patient (2%) from positive to negative, helped locate the parathyroid adenoma for 4 (8%), and had no effect for 43 (90%). The corresponding evaluations generated by reader 2 were 0 (0%), 4 (8%), and 44 (92%), respectively (Table 1). Thus, compared with conventional SPECT, SPECT/CT was minimally useful. However, both readers found SPECT/CT useful in accurately identifying and locating the 2 ectopic parathyroid adenomas in the study cohort (Figs. 1 and 2). The 2 readers agreed in their response for 29 of 48 patients while reading the SPECT images and for 45 of 48 patients while reading the SPECT/CT images. The κ-value was 0.39 with P = 0.00 for SPECT interpretation and 0.00 with P = 0.91 for SPECT/CT interpretation, indicating fair interobserver agreement for SPECT evaluation but good agreement for SPECT/CT evaluation.
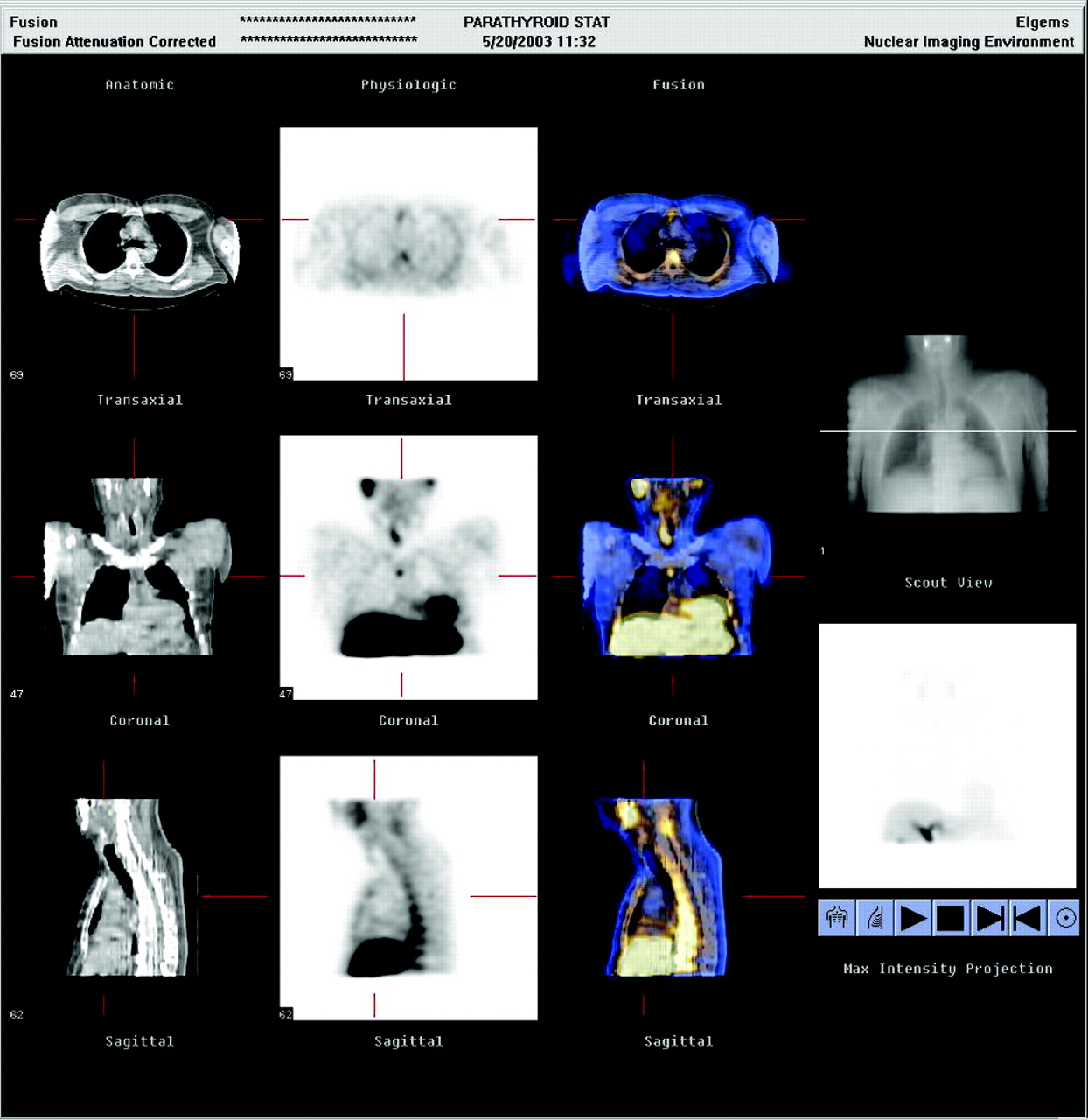
SPECT/CT helped accurately locate ectopic intrathymic parathyroid adenoma in patient with primary hyperparathyroidism and left hemithyroidectomy.
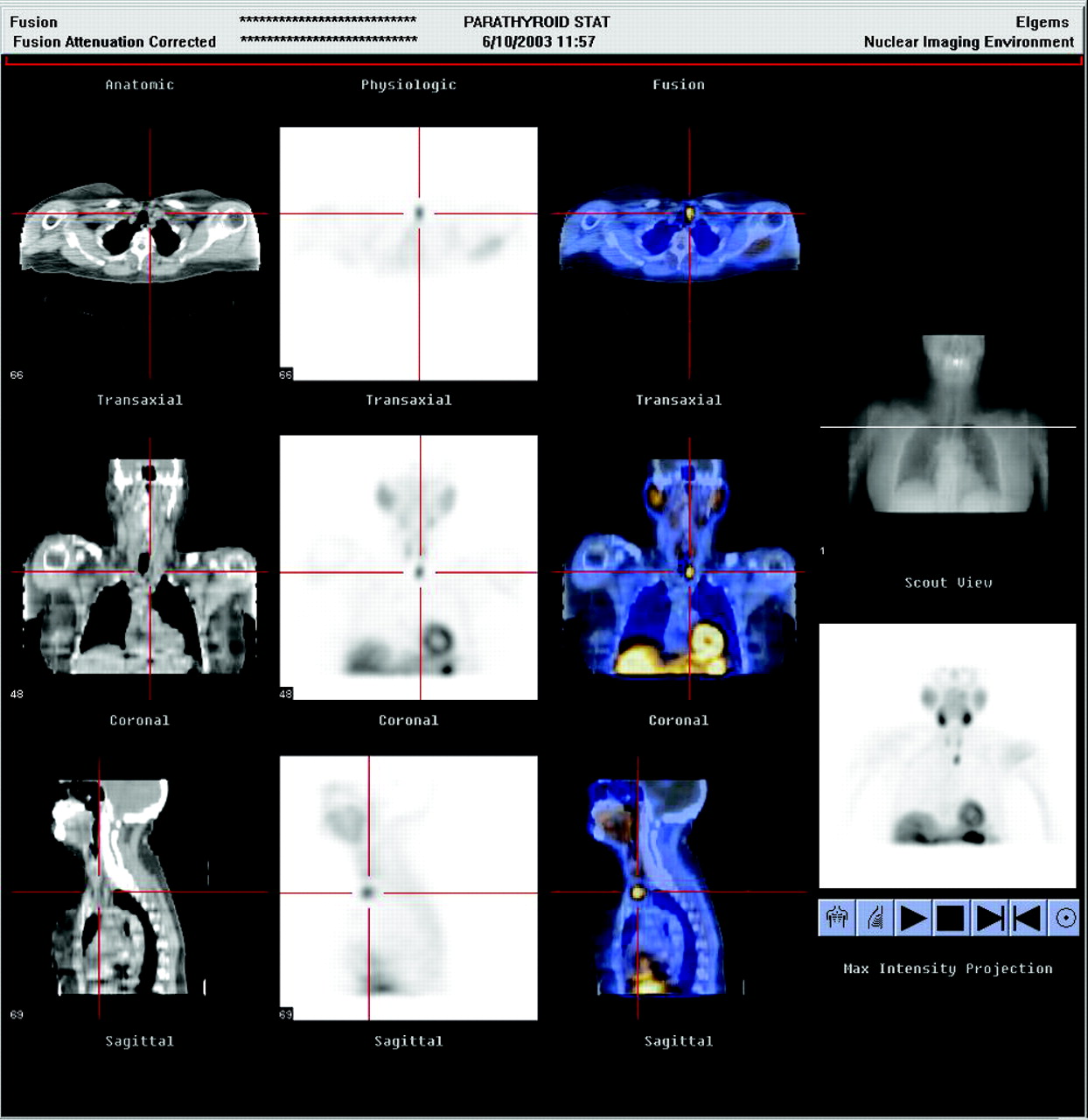
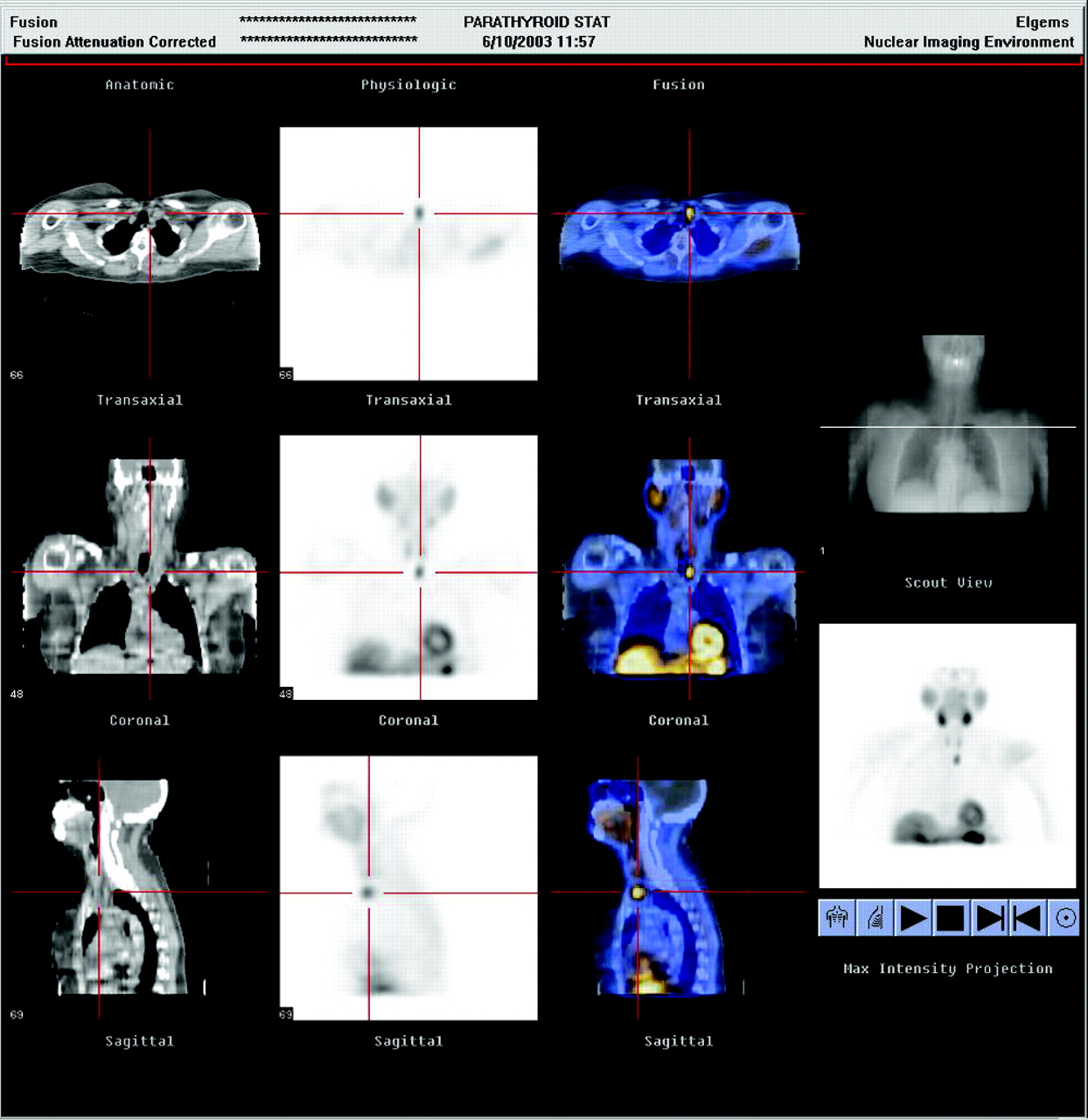
SPECT/CT accurately located ectopic parathyroid gland behind left sternoclavicular joint. Locating gland helped with planning preoperative parathyroidectomy to minimize dissection.
Additive Value of SPECT and SPECT/CT for Diagnosis and Localization of Parathyroid Disease
Thirty-five diseased parathyroid glands were resected from the 32 patients whose scan results were positive. Sixteen patients did not undergo surgery, 10 because of negative results on scans and other radiologic examinations. There is a tendency in our institution to repeat noninvasive imaging until a diseased parathyroid gland is identified rather than to operate blindly. The remaining 6 patients did not undergo scanning because they had comorbidity with a primary cancer (n = 2), refused the operation (n = 1), or were lost to follow-up (n = 3). Thirty-four patients had normal thyroid gland, 8 multinodular, 4 total thyroidectomy, and 2 hemithyroidectomy. The ability of planar imaging plus SPECT, and of planar imaging plus SPECT/CT, to identify the diseased parathyroid gland in patients who underwent the operation was 86% in patients with normal thyroid glands and 100% in patients with multinodular glands, with a total identification rate of 89%. Thus, there was no difference in the identification rate with the addition of the CT portion of the study. Three patients had 2 glands involved although the parathyroid scan showed only 1 gland involved. In 1 patient, the removed tissue was a thyroid nodule. Interestingly, even with SPECT/CT the location of the involved gland was incorrectly identified in 8 patients: When the scan indicated that an inferior gland was involved, the gland was surgically identified to be superior, and vice versa. However, the gland was always on the same side of the neck whether right or left, thus still decreasing neck dissection when compared with total neck exploration.
Thirty of the total removed glands were adenomas, 4 were hyperplastic, and 1 was a thyroid nodule. The delayed tracer retention pattern did not differ between the hyperplastic glands and the adenomas. Delayed tracer retention was noted in 3 of the hyperplastic glands. On the other hand, 17 of the adenomas showed retention, 12 showed washout, and 1 patient did not undergo delayed imaging. The scintigraphically unidentified second involved gland in 3 patients was hyperplastic in 1 patient and adenomatous in the other 2 patients. Thus, the pattern of tracer retention or washout cannot predict the pathology of the involved gland.
Mean PTH, tCa, and fCa levels were not significantly different between the patients with positive scan findings and the patients with negative scan findings (PTH = 186.7 and 123.5 pg/mL, respectively, P = 0.12; tCa = 10.3 and 10.5 mg/dL, respectively, P = 0.61; fCa = 1.33 and 2.0 mmol/L, respectively, P = 0.44). All patients who underwent surgery demonstrated a decrease in their chemical markers, with a mean intact PTH of 74 (reference range, 10–65 pg/mL), a mean tCa of 9.2 (reference range, 8.4–10.2 mg/dL), and a mean fCa of 1.22 (reference range, 1.13–1.32 mmol/L). Only 1 patient demonstrated normalization of his intact PTH level but persistently elevated tCa and fCa levels postoperatively. These findings indicated the adequacy and completeness of the operations in all patients.
DISCUSSION
We attempted to evaluate the usefulness of SPECT/CT in the evaluation of parathyroid adenomas and hyperplasia over conventional SPECT. The SPECT/CT images did not significantly affect the interpretation or localization of diseased parathyroid glands except in 2 patients with ectopic parathyroid glands. Elimination of the CT portion can reduce image acquisition time by 10 min and patient radiation dose by 0.9 mSv (annual allowable limit for the public is 2.5 mSv). Therefore, we recommend the use of SPECT/CT only for locating ectopic parathyroid glands.
Of note was the difference in interobserver agreement about the usefulness of conventional SPECT in addition to planar scanning. Reader 1 found SPECT helpful in identifying diseased glands for 9 patients, whereas reader 2 found it helpful for 20 patients. The difference occurred because reader 1 considered focal retention of tracer on delayed planar images to be consistent with parathyroid adenoma whereas reader 2 depended frequently on SPECT images to identify pathologic processes in or posterior to the thyroid gland. However, both readers agreed that fusing CT images with SPECT images provided little additional information on parathyroid glands that were in the correct anatomic location.
We could not evaluate the sensitivity and specificity of SPECT/CT because 16 patients did not undergo surgery (10 because of negative scan findings). Thus, the actual number of false-negatives and true-negatives is unknown. Therefore, we used the term identification rate instead of the term sensitivity to evaluate the accuracy of our imaging method. Overall, we had good identification rates of 89% in all patients and 100% in patients with multinodular thyroid gland. These are higher than the previously reported decreased sensitivity of 71% for patients with multinodular goiter, compared with 91% for patients with normal thyroid glands (13). This difference might be due to the small number of patients with multinodular thyroid glands in our study population.
We did not observe a statistically significant relationship between the chemical markers of hyperparathyroidism and the identification rate of the involved parathyroid gland as previously suggested by Staudenherz et al. (13) and Parikshak et al. (19). Our findings agree with those of Clark et al., who previously reported a lack of correlation between biochemical markers or thyroid gland pathology and imaging sensitivity (20). Similarly, there was no particular difference in the pattern of tracer retention or washout between hyperplastic glands and adenomatous glands with comparable identification rates. Our finding agrees with that of Wakamatsu et al., who previously demonstrated comparable sensitivities of 36.7% and 39.7% for the identification of hyperplastic and adenomatous glands, respectively (2).
In our study, the involved parathyroid gland (superior or inferior) was misidentified in 8 patients. Misidentification can result in more extensive intraoperative dissection to find the involved gland, thus leading to a larger surgical scar and longer operative time and defeating the purpose of accurately locating the involved gland for minimally invasive surgery. However, in all cases the involved gland was on the same side as the scintigraphically identified abnormal gland. This is believed to be due to the growth pattern of superior parathyroid adenomas, which tend to enlarge inferiorly behind the thyroid gland, thus appearing to be an inferior thyroid adenoma. This has to be taken into consideration when interpreting parathyroid scans. Clark et al. have observed a similar problem and have suggested the addition of lateral images to the standard imaging protocol (10). Additionally, the use of an intraoperative γ-probe is highly recommended for better locating the glands in such cases (21). Also of note is the difficulty we faced in identifying involvement of a second parathyroid gland in 3 patients. This difficulty supports the importance of combining preoperative imaging with intraoperative PTH level measurement to identify pathologic residual parathyroid gland after removal of the scintigraphically identified parathyroid adenoma or hyperplasia (22).
Although this study was retrospective, all patients were imaged consistently, increasing our confidence in the results. The lack of operative results for patients with negative scan findings hinders the complete evaluation of false-negative SPECT or SPECT/CT findings. However, considering the increasing trust of surgeons in parathyroid nuclear scans and the adoption of minimally invasive surgery, it would be difficult to conduct a prospective study in which patients with negative scan results still undergo surgery.
Finally, we recommend that SPECT/CT be reserved for ectopic parathyroid adenomas and that planar and conventional SPECT be used for normally located parathyroid adenomas or hyperplasia.
CONCLUSION
SPECT/CT has no significant additive value over conventional SPECT for identifying or locating a normally located parathyroid adenoma or hyperplasia in patients with primary hyperparathyroidism. However, SPECT/CT is important for locating ectopic parathyroid adenomas. Exclusion of the CT part from the routine parathyroid imaging protocol saves the patient from unnecessary radiation exposure and imaging time.
Footnotes
Received Mar. 26, 2004; revision accepted Sep. 17, 2004.
For correspondence or reprints contact: Isis W. Gayed, MD, Department of Nuclear Medicine, Unit 83, University of Texas M.D. Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030.
E-mail: igayed{at}di.mdacc.tmc.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Simulated Fewer-Angle SPECT/CT Imaging Protocol for Parathyroid Adenoma
- Bilateral neck exploration in patients with primary hyperparathyroidism and discordant imaging results: a single-centre study
- Parathyroid Imaging and Localization Using SPECT/CT: Initial Results
- Improved Delineation of Parathyroid Lesions in Patients with Chronic Renal Failure Using Magnified Pinhole Imaging
- Incremental Value of 131I SPECT/CT in the Management of Patients with Differentiated Thyroid Carcinoma
- Preoperative 123I/99mTc-Sestamibi Subtraction SPECT and SPECT/CT in Primary Hyperparathyroidism
- SPECT/CT
- Tomoscintigraphy Improves the Determination of the Embryologic Origin of Parathyroid Adenomas, Especially in Apparently Inferior Glands: Imaging Features and Surgical Implications
- Comparison of SPECT/CT, SPECT, and Planar Imaging with Single- and Dual-Phase 99mTc-Sestamibi Parathyroid Scintigraphy
- Subtraction SPECT for Parathyroid Scintigraphy Based on Maximization of Mutual Information
- Procedure Guideline for SPECT/CT Imaging 1.0