


Abstract
The recent approval of 2 radiolabeled antibodies against cluster designation 20–positive lymphoma has led to a resurgence of interest in radioimmunotherapy. As was the case with chemotherapy development, progress has been most marked in the hematologic neoplasms, both in myeloablative and in nonmyeloablative therapeutic strategies. Success in the radioimmunotherapy of solid tumors has lagged because of the immunogenicity of murine proteins and the relatively slow clearance of humanized intact immunoglobulins. Genetic engineering has enabled the development of a variety of antigen-binding constructs of various sizes and immunobiologic characteristics. Developments in radiochemistry as well as production of an increasing number of radionuclides with therapeutic potential or optimal imaging characteristics have spurred tailored therapeutic strategies that include dosimetry and considerations of tumor burden. Such progress has generated pivotal studies that will establish the radiobiologic paradigms for successful radioimmunotherapy of solid tumors. This review will describe seminal studies that have paved the way to an understanding of radioimmunotherapy in solid tumors. Finally, the authors’ views of the future of this promising cancer therapy will be presented.
Although it has been only 2 years since the Food and Drug Administration (FDA) approved the use of the first radiolabeled antibody, radioimmunotherapy (RIT) has been the subject of investigations since the early 1970s. As one of many promising therapeutic strategies that are encompassed by the magic-bullet concept, RIT uses an antibody that recognizes tumor-associated antigens and carries cytotoxic radionuclides to a target, thereby destroying cancer cells. The approval of 2 radiolabeled antibodies in the treatment of non-Hodgkin’s lymphoma has offered hope about the role of RIT in the management of cancer. Nevertheless, the development of effective RIT faces many challenges. The success of RIT thus far has been driven by the results seen in hematologic tumors, whereas solid tumors have been less responsive.
Currently, the only radiolabeled antibodies with FDA approval are for the treatment of B-cell non-Hodgkin’s lymphoma. Several trials of various antibodies for the treatment of non-Hodgkin’s lymphoma have demonstrated a satisfactory response in relapsed and refractory disease, as well as potential for use with certain chemotherapeutic agents and autologous stem cell transplantation (1–5). The results of RIT for solid tumors have been less encouraging. Response to RIT has been studied in various tumor types, including breast, ovary, colorectum, kidney, prostate, and brain, although no response has been sufficiently promising to warrant further development with nonmyeloablative RIT. The initial clinical trials on solid tumors have, however, shed considerable light on antigen-binding construct design, optimal radionuclides for tumors of various sizes, and treatment delivery systems that will result in novel approaches to targeted radiopharmaceutical therapy.
Designing optimal RIT for solid tumors depends on many variables. Choosing a construct for solid tumors, which are generally large and heterogeneous, is of particular concern. Factors to consider when designing therapy include immunogenicity, heterogeneity of antigen expression, uptake by tumor secondary to vascular and tumor permeability, deleterious effects on normal tissues, and residence time in the body (6,7). Recombinant techniques, as well as the development of small antigen-binding constructs, are just some of the methods being used to address the optimal targeting of a tumor.
The choice of the optimal construct and radionuclide is part of the challenge of designing therapy for solid tumors that is the most effective and that offers the fewest limitations. An understanding of RIT therefore requires an understanding of the potential and limitations of radionuclides and antigen-binding constructs. These will be outlined, followed by proposed strategies for rational treatment designs that address the biologic complexity of solid tumors.
ANTIBODY CONSTRUCTS
The move from polyclonal antibodies to murine monoclonal antibodies (mAbs) brought into focus the inherent immunogenicity of xenogeneic proteins. The production of human antimouse antibodies after murine mAb administration precludes effective multiple-dosing regimens. The use of chimeric antibodies, in which a gene for the human immunoglobulin constant region is fused with the murine variable (Fv) region, has significantly reduced immunogenicity. Humanized antibodies are generated from the gene of the antigen-binding or complementarity-determining region on a human IgG background. These are also used as a less immunogenic alternative to murine antibodies. Development of these types of antibodies will be an essential part of treatment regimens that require multiple administrations for optimal response, although the development of human antihuman antibodies has been seen occasionally.
One method of improving tumor penetration and clearance from normal tissues is the use of small constructs. Fab′ and F(ab)′2 are 2 such constructs that are being investigated in mouse models and humans with good results. Single-chain antigen binding proteins (sFv) are linear constructs of light and heavy Fv fragments that clear rapidly from the blood and may have lower renal retention than do Fab′ fragments. Other constructs with rapid clearance are minibodies, which consist of 2 sFv fragments linked by a component of the heavy-chain region (e.g., CH3), and diabodies, which comprise 2 sFv fragments joined chemically by disulfide bonds or by genetic engineering of the sequences.
RADIONUCLIDES
A major consideration in the development of RIT is the choice of radionuclide. Characteristics such as physical and chemical properties, fate after antibody metabolism in vivo, and the nature of the radiation are determinants of the suitability of a radionuclide for therapy. Cytotoxic radionuclides may be divided into 3 groups of radiochemicals: halogens (iodine, 211At), metals (90Y, 67Cu, 213Bi, 212Bi), and transitional elements (186Re). Radionuclides can further be categorized into 4 types of cytotoxic agents: pure β-emitters (67Cu, 90Y); α-emitters (213Bi, 211At), β-emitters that emit γ-radiation (177Lu, 186Re, 131I), and Auger emitters and radionuclides that decay by internal conversion, including 125I and 67Ga (Table 1).
Therapeutic Radionuclides and Their Half-Lives, Energy, and Range in Tissue
131I is the most widely understood radionuclide for the treatment of cancer. 131I is a mainstay of the treatment of thyroid cancer, and thus its biodistribution has been well studied. 131I offers the advantages of high-energy γ-emissions for imaging, long half-life, and a simple protein labeling process. Although the high-energy γ-emissions have created potential concerns about the safety of patients and their contacts, recent guidelines will permit many patients receiving RIT with 131I to be treated as outpatients. Hospitals in the United States may release patients only if the expected exposure to an individual due to proximity to the patient is no greater than 5 mSv (500 mrem) (8).
131I is not the optimal nuclide when conjugated with antibodies that are internalized via the lysosomal pathway after the antibody–antigen interaction. This process leads to dehalogenation of the complex and release of the radionuclide, thus limiting tumor dose. Because of these limitations, other radionuclides have been studied. 90Y, a pure β-emitting metal, has been widely studied as a high-energy alternative to 131I. 90Y is an attractive choice for RIT involving internalized antibody–antigen complexes, as radiometal antibodies are infrequently degraded internally. The success of 90Y for use in RIT is evident, as the first RIT to be approved by the FDA was an anti–cluster designation 20 antibody conjugated to 90Y (Zevalin; Biogen Idec Pharmaceuticals). One limitation of yttrium, however, is its affinity for bone. In a situation in which 90Y is detached from the chelating agent, bone marrow could thus receive unacceptably high levels of radioactivity.
Rhenium isotopes have been under investigation for use in RIT. Both 186Re and 188Re have been linked to antibodies. 188Re has the advantage of being easily generated with a 188W generator. Its short half-life of 17 h renders it suitable for locoregional therapies or for therapies with small molecules that clear from the body rapidly. Because of its physical properties, including longer half-life, 186Re has been more extensively studied. Rhenium nuclides have γ-emissions, which allow for easy detection of distribution and clearance by external scintigraphy. Early clinical trials have exploited the γ-emissions of 186Re to analyze absorbed doses to tumors and normal organs and have demonstrated its safety for RIT of solid tumors (9).
Recent developments in radiochemistry have led to the increased interest in α-emitters for therapy. α-Particles are high-energy helium nuclei with high-linear-energy transfer. α-Particles have a range of only 50–80 μm, making them most useful for individual cells, such as micrometastases and circulating tumor cells. In fact, 213Bi conjugated to a humanized anti-CD33 antibody is being evaluated in clinical trials for the treatment of advanced myelogenous leukemia. In addition to 212Bi and 213Bi, which are generated as eluates from 224Ra and 225Ac generators, cyclotron-produced 211At is under investigation as therapy for several tumor types. Clinical trials have been reported using 211At-labeled chimeric antitenascin antibody 81C6 for gliomas (10).
In vivo generators of α-particles are being investigated for their ability to deliver cytotoxic particles to micrometastases. These generators overcome the limitations posed by the short half-lives of most α-particles. These “nanogenerators” have been studied in various tumor types in mice. One study conjugated a 225Ac generator to an internalizing antibody that targeted Her-2/neu (trastuzumab) to study its efficacy in treating disease in a mouse model of advanced ovarian cancer (11). This generator produces 3 α-particle–emitting radioisotopes, including 213Bi.
Auger emitters deposit high-linear-energy transfer over extremely short distances and are therefore most effective when the decay occurs in the nucleus and less so when the decay occurs in the cytoplasm (12). 125I is the prototypical radionuclide, but its long half-life renders it less than optimal for therapy. Other similar radionuclides that have been studied, although not with antibodies, have included 111In. In both cases, the amount of radioactivity necessary is economically prohibitive. A radionuclide that is gaining increasing attention in this category is 67Ga. Improvements in chelation chemistry have resulted in stable radioimmunoconjugates with 67Ga, and clinical trials are planned by us and several other groups.
RIT FOR SOLID TUMORS
Most clinical RIT studies on solid tumors have been performed on colon cancer. Secreted antigen systems such as carcinoembryonic antigen (CEA) and TAG-72 (sialyl Tn); cell surface antigens including 17-1A, Lewis Y (Ley), and A33; and stromal antigens, notably fibroblast activation-protein-α, have been studied, both at this center and elsewhere. This section will highlight key phase 1 and 2 trials, particularly ones targeting colon cancer, as well as selected trials that are in early stages.
CEA
Starting with a radioiodinated polyclonal anti-CEA antibody (13), Goldenberg et al. pioneered the use of antibodies in the detection and therapy of cancer. This group has subsequently performed RIT studies with 131I-labeled murine and humanized anti-CEA antibodies (14–17). A recent phase 2 trial of 21 patients treated with 131I-labeled humanized anti-CEA mAb (hMN-14; Immunomedics, Inc.) studied response to RIT in both patients with small-volume metastasis refractory to treatment and patients who had undergone surgical resection of metachronous liver metastases with curative intent (18). Each patient received a single dose of 2,220 MBq/m2 (60 mCi/m2), which was previously demonstrated to be the maximum tolerated dose. Between both groups of patients, the study demonstrated an overall response rate of 58%, with a mean duration of response of 9 mo. Of the 9 patients receiving RIT in an adjuvant setting after surgery, 7 remained disease free at 36 mo after treatment. Although these results appear promising, they underscore the suitability of current methods of RIT for small-volume disease rather than bulky disease.
In another effort to develop nonimmunogenic antigen-binding constructs against CEA, Raubitschek’s group at the City of Hope Medical Center have performed studies with a chimeric antibody. The initial dose-finding study established no mass dependence on tumor targeting and no evidence of immunogenicity (19). Subsequent RIT studies with 90Y-labeled antibody (20) demonstrated that radionuclide toxicity was, again, nuclide dependent. No responses were observed in this nonmyeloablative trial, prompting a myeloablative trial (21), the final results of which are awaited. The observation that nonmyeloablative RIT with intact IgG is unlikely to result in major responses has spurred the development of various antigen-binding constructs (22), which are now being produced for clinical study.
Begent et al. have also performed studies using 131I-labeled antigen-binding constructs (whole IgG, F(ab)′2 fragments, cross-linked divalent and trivalent versions). Although there was selective targeting of iodinated sFv to tumor, the degree of uptake was perhaps not adequate to result in responses with 131I (23). Begent et al. have continued their pioneering studies by developing a single-chain Fv fragment of their anti-CEA antibody. This sFv construct is grown in E. coli and exhibits impressive targeting abilities (24).
TAG-72
mAb CC49 is a murine IgG targeting the antigen (Tn/sialylTn) expressed on a tumor-associated mucin, TAG-72, that is expressed heterogeneously in most adenocarcinomas and thus is a potential target for RIT in several cancers. CC49 IgG exhibits high reactivity against tumor cells in most adenocarcinomas from colorectum, ovary, breast, stomach, and pancreas, with very little reactivity against normal tissues (25). After an initial study comparing CC49 with its lower-affinity counterpart B72.3 had shown CC49 to have better relative uptake in colorectal cancer (26), phase 1 studies with 131I-CC49 in colorectal cancer demonstrated excellent tumor targeting and low levels of toxicity at a maximum tolerated dose (MTD) of 2,775 MBq/m2 (75 mCi/m2) (27). Further trials, however, have demonstrated tumor doses of 0.19–6.67 Gy (19–667 rad) but no objective tumor responses (28). Dose-limiting toxicity was hematopoietic and nuclide dependent. Moreover, in 12 of the 13 patients studied, human antimouse antibodies developed.
An attempt to reduce immunogenicity by administration of an immunosuppressive agent, deoxyspergualin, demonstrated less than satisfactory results (29), and so humanization of the antibody was embarked on. To ensure that clearance of the humanized antibody was as close as possible to that of the murine intact IgG, the CH2 domain of the chimeric antibody was deleted. Initial clinical trials (30) have shown that clearance and targeting characteristics are indeed comparable and that the novel protein is nonimmunogenic. Retention of the CH3 domain retains the immunobiologic functions of the antibody, and therefore a phase 1 trial to assess both the immunobiologic properties of CH2-deleted huCC49 and the safety of 131I-labeled antibody is under way.
The initial studies on colon cancer were followed by phase 1 and phase 2 studies on a variety of other solid tumors, notably breast and prostate cancers (30–33). Alvarez et al. performed a phase 1/2 trial of intraperitoneal 177Lu-CC49 mAb in 27 patients with recurrent ovarian cancer (34). The MTD was 1,665 MBq/m2 (45 mCi/m2), and the dose-limiting toxicity was bone marrow suppression. In most patients with gross disease, the disease progressed after therapy. Prolonged disease-free survival was observed only in patients with microscopic disease. Since then, intraperitoneal RIT with 131I-CC49 has also been performed on ovarian cancer (35) and combination therapy is being investigated (36).
In all these studies, there has been excellent tumor targeting but no significant clinical responses. As is the case with most antigen–antibody systems in solid tumors, the limitations in the clinical application of radiolabeled CC49 IgG are primarily due to normal tissue toxicity, immunogenicity, and relatively poor penetration into tumor. Genetically engineered sFvs are one way to potentially overcome some of these limitations. The sFvs had accelerated clearance from the vasculature, excellent penetration into the tumor from the vasculature, reduced immunogenicity, and higher tumor-to-background ratios than did corresponding IgG, F(ab′)2, or Fab′ fragments in animal models (37–40). Early studies at this center by Larson et al. (41) of a 123I-labeled sFv CC49 in human metastatic colorectal carcinoma demonstrated rapid distribution and clearance from the body via the kidneys and the feasibility of same-day imaging of the metastatic tumors in patients with colorectal carcinoma. However, because of their small size and monovalency, sFvs clear the body too rapidly to allow for sufficient tumor uptake and retention for therapeutic applications. Moreover, early sFvs were generated in bacterial systems and may not have been stable in vivo.
A33
A33 is a promising target for RIT in colon cancer. The A33 antigen, a transmembrane glycoprotein, is not secreted and is highly expressed by cells of colonic origin. In addition, mAb A33 is rapidly internalized into a cell after binding to the A33 antigen on the cell membrane. All these factors promote rapid tumor localization as well as high uptake by tumors. Phase 1/2 studies of 131I-mAb A33 RIT were performed on patients with colon cancer (42). Again, dose-limiting toxicity was nuclide dependent, and the MTD was determined to be 2,775 MBq (75 mCi) of 131I per square meter. Although the isotope showed variable uptake in normal bowel, gastrointestinal symptoms were mild or absent.
We also investigated 125I-murine A33, as the radioiodinated antibody appears to not undergo catabolism after internalization (probably via the macropinosome). This phenomenon could provide a therapeutic advantage if antibodies internalize and therefore transport low-energy electron-emitting isotopes close to the tumor cell nucleus (43). A phase 1/2 study of 125I-labeled mAb A33 demonstrated low rates of toxicity but only modest response rates (44). MTD was not reached with doses of up to 13 GBq/m2 (350 mCi/m2) of 125I-mAb A33. Of the 21 patients, 1 demonstrated a mixed response based on imaging studies and 2 patients with stable disease demonstrated decreased serum CEA levels. Higher levels of response were seen in patients who pursued further chemotherapy (carmustine, vincristine, fluorouracil, and streptozocin) after RIT, suggesting a potential role of combined RIT and chemotherapy. Humanized A33 has been investigated by our group; it is less immunogenic and has a biodistribution profile comparable to that of the murine protein. Studies comparing the efficacy of combined radiosensitizing chemotherapy (capecitabine) and RIT with 131I-huA33 are currently under way.
OTHER ANTIGENIC SYSTEMS STUDIED
Antibody 17-1A (murine IgG2a), which reacts against the surface epithelial antigen KSA, has also been studied with different radionuclides. The internalizing properties of murine antibody 17-1A make it attractive as a carrier for 125I. The antibody was chimerized, and a pilot clinical trial of increasing doses of 125I-chimeric 17-1A in patients with metastatic colorectal cancer was conducted (45). This trial, performed at the University of Alabama in Birmingham, corroborated our results that high-dose outpatient RIT with a 125I-labeled internalizing antibody could be achieved without significant patient toxicity or radiation hazard.
Our team has attempted to identify targets not only on cancer cell surfaces but also on other components of the tumor, including stroma and vasculature. We developed a novel targeting approach to colon cancer therapy by developing an antibody, F19, against fibroblast activation protein-α. Fibroblast activation protein-α is highly expressed by activated fibroblasts abundant in most solid tumors, including more than 95% of primary and metastatic colorectal carcinomas, but is not expressed by normal tissue (other than healing scars).
Further studies were performed to define the toxicity, imaging, and biodistribution characteristics of 131I-labeled mAb F19. Because of selective localization in the tumor, with minimal uptake in the normal tissues, lesions as small as 1 cm could be visualized by scintigraphy (46). The easy accessibility of the fibroblast activation protein–positive tumor stromal fibroblasts to circulating mAb prompted the humanization of this antibody, now named sibrotuzumab. Phase 1 mass dose-finding studies have been completed with this novel protein (47), and RIT studies are being performed.
Ovarian carcinoma has a high mortality rate, because most ovarian carcinomas are detected at a late stage. In addition to CC49 antibodies, various other antibody–antigen systems have been studied in ovarian cancer. MX35 is expressed homogeneously in 90% of epithelial ovarian cancers and is also expressed in epithelial cells of the lung, sweat glands, kidney, collecting ducts, thyroid, fallopian tube, cervix, and uterus (48). Several studies using 131I- and 125I-labeled mAb MX35 showed excellent localization to sites of ovarian tumors, including micrometastases in the peritoneal wall (49). MOv18 targets the membrane folate receptor that is highly expressed on ovarian carcinoma cells. 131I chimeric MOv18 mAb was studied in 3 patients and showed moderate visualization of tumor sites, tumor-absorbed doses of 600–3,800 cGy, and stable disease for 2 to >6 mo (50). Moreover, administration of the antibody was not associated with development of human antichimeric antibodies. Intraperitoneal RIT using 90Y-labeled murine anti-HMFG1 (analogous to the muc-1 antigen) as an adjuvant to chemotherapy compared with chemotherapy alone has shown increased overall survival in patients who received the RIT compared with those who received chemotherapy alone (51). Ovarian cancer is limited to the peritoneal cavity for most of its natural progression, and therefore intraperitoneal therapies have always held promise for a disease with limited treatment options.
Systemic RIT studies with anti-muc1 antibodies have been performed largely on breast cancer. Unlike most of the studies above, which used radioiodine initially and then studied other radionuclides, the studies with a novel humanized anti-muc1 antibody, BrE3, were performed with 90Y (52). These studies showed that targeting using 111In as a surrogate (53) was excellent and that phase 2 trials to establish efficacy were justified, especially since the humanized BrE3 antibody has immune effector function in vitro.
Limited studies with intrathecal RIT have also shown promise. Intrathecal RIT has potential, as radiation in the closed compartment is more likely to have efficacy when its retention can be enhanced by conjugation to a large molecule that will transit slowly into the systemic compartment. Most studies have been performed with β-minus–emitting nuclides (54–61), which may be less than ideal because the energy may be deposited outside the intrathecal space to varying extents depending on the nuclide. In this respect, α-emitters may be ideal, as they deposit high-linear-energy transfer radiation over submillimeter distances (62). No studies have progressed to phase 2 or higher; however, this is more a function of nuclide availability and patient characteristics than of lack of promise.
The Ley antigen is a blood group–related antigen that is expressed in a high proportion of epithelial cancers, including breast, colon, ovarian, and lung cancer, and therefore is an attractive target for mAb-directed therapy. Early studies with anti-Ley antibodies performed using chemoimmunoconjugates demonstrated significant gastrointestinal toxicity without significant efficacy (63). Pastan’s group has studied another anti-Ley antibody, labeled with either 111In to study biodistribution or 90Y for therapy (64). The phase 2 study demonstrated good tumor localization, and the MTD was found to be 740 MBq of 90Y. Those investigators are now developing trials to study the efficacy of the radioimmunoconjugate in advanced gastrointestinal malignancy. They have also investigated an immunotoxin (65), and this holds promise for single-chain anti-Ley proteins conjugated with radionuclides. The Ley antigen is abundantly expressed in both gastric and ovarian cancers, which are limited to the peritoneal cavity for much of their natural course. We have therefore initiated a phase 1 intraperitoneal RIT study using 90Y labeled to another humanized anti-Ley antibody, hu3S193, initially generated at our center (66), in ovarian cancer patients with minimal residual disease (Fig. 1).

Anterior (left) and posterior (right) images at various times after intraperitoneal administration of 111In-labeled humanized anti-Ley antibody hu3S193.
CARBONIC ANHYDRASE IX
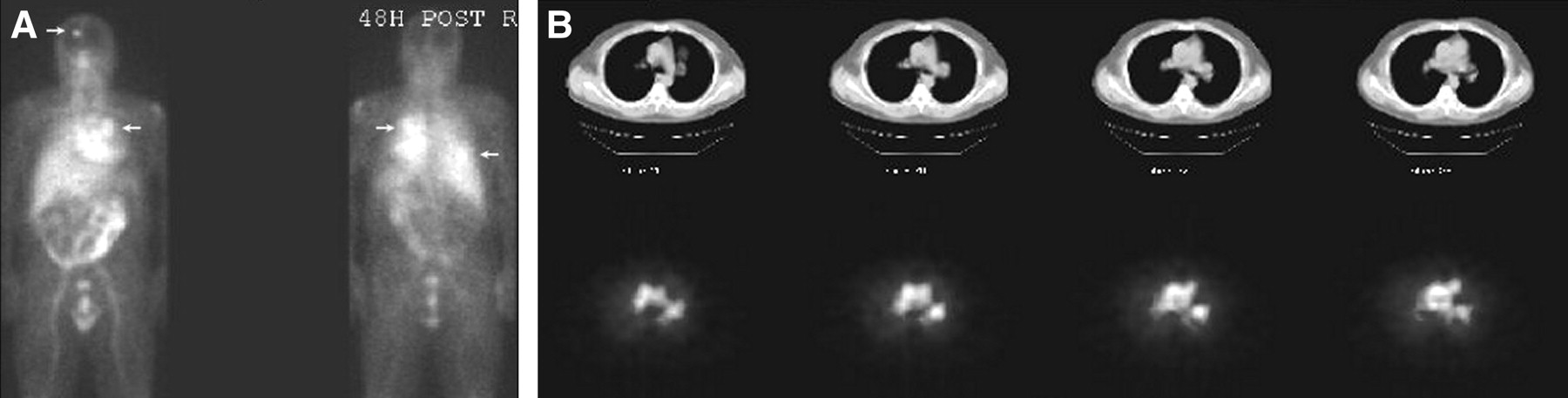
Carbonic anhydrase IX is expressed in more than 80% of primary renal cell carcinomas and therefore is an excellent therapeutic target for a cancer refractory to chemotherapy and whose 5-y survival rate is less than 10%. Antibody G250, developed by Oosterwijk et al., recognizes carbonic anhydrase IX, with normal tissue cross-reactivity limited to biliary epithelium (67). An early study of mouse mAb G250 demonstrated excellent targeting to renal tumors, but treatment was limited by the development of a host immune response (68). This is particularly significant, as it precludes the use of multiple administrations, a method that is thought to be crucial for treatment of heterogeneous, bulky solid tumors. Recent phase 1 studies have used 131I chimeric mAb G250 as a less immunogenic alternative to mG250. One such study examining distribution of antibody uptake in tumors used a diagnostic dose of 131I cG250 before a single large radioimmunotherapeutic dose. To evaluate the effect of dose fractionation on safety and efficacy, we simultaneously started a single large-dose RIT study based on escalating amounts of 131I and a study of fractionated cG250 using ≤1,110-MBq (30 mCi) 131I-cG250 doses in a schema based on whole-body radiation-absorbed dose (69). The trial of fractionated cG250 demonstrated differential distribution of radioactivity after each treatment dose (Fig. 2). In this study, the MTD of 131I was found to be 0.75 Gy and dose-limiting toxicity was hematologic. Preliminary calculations suggest that dose-limiting whole-body radiation-absorbed dose is not different in “rapidly” fractionated and single-large-dose treatment schemata (J.A. O’Donoghue and S.H. Bender, et al., unpublished data, July 2004).

(A) Anterior (left) and posterior (right) whole-body images obtained 3 d after administration of 131I-chimeric G250. Targeting to known lesions in scalp, hilum, and lung is excellent. (B) CT (top row) and SPECT (bottom row) coregistered images demonstrate uniform distribution throughout left hilar mass in same patient.
Because the G250 antibody binds to epithelial cells of the large bile duct and gallbladder, and because biliary cancer is sensitive to radiation, RIT with cG250 may have clinical benefits in the treatment of biliary cancer patients. These cancers are particularly difficult to treat because of the late stage at diagnosis. The 131I-labeled antibody WX-G250 RIT is designed to identify the tumor cells and deliver tumor-destroying doses of radiation directly to the tumor cells. Clinical phase 1/2 trials with WX-G250RIT in biliary cancer patients appear promising (70). Because the antigen is expressed on both normal biliary tissue and biliary cancers, the evaluation of differential expression is important to the selection of an appropriate RIT model, and we are therefore evaluating differential in vivo expression of tumor antigen expression using quantitative PET and 124I-cG250.
PROSTATE-SPECIFIC-MEMBRANE ANTIGEN (PSMA)
Although prostate cancer has received much attention because of the success of diagnostic biomarkers, the success of RIT for the disease has lagged. Studies of 131I-murine CC49 mAb failed to show an objective response (71). Subsequently, studies have attempted to increase antigen expression using interferon pretreatment (72). Fourteen patients received 7 doses of interferon followed by treatment with 2,775 MBq (75 mCi) of 131I-CC49 per square meter. Although TAG-72 expression seemed to be upregulated, as evidenced by increased tumor localization, no significant response was achieved. Moreover, in 12 of the patients, human antimouse antibodies developed.
PSMA is not a secreted antigen and has been identified as an excellent target for RIT for prostate cancer. Studies of PSMA mAb 7E11/CY356 labeled with 90Y demonstrated no therapeutic efficacy, probably because this antibody targets an internal epitope of PSMA, thus targeting only dead or dying tumor cells. In contrast, mAb J591 targets the external domain of PSMA (73). Phase 1 studies of 90Y- and 177Lu-labeled humanized J591 mAb are under way (74).
PRETARGETING STRATEGIES
To enhance the efficacy of RIT, multistep targeting strategies have been under development. These methods are designed to minimize the radiation to normal tissue that is due to a prolonged residence in the body. One approach uses the interaction of avidin and biotin. The targeting antibody is biotinylated before injection. After injection, avidin is injected in order to bind to the antibody in the tumor. Finally, radiolabeled biotin is injected and attaches to the avidin in the tumor. The use of a clearing agent may further reduce the amount of antibody in normal tissues (Fig. 3).

Tumor pretargeting with bispecific construct. Bispecific agent (e.g., bispecific antibody or antibody/streptavidin fusion) is administered and saturates antigenic sites on tumor. Subsequently, a small radionuclide carrier is administered and binds to the tumor-localizing bispecific agent.
Early studies of pretargeted RIT designed to evaluate its safety and therapeutic ratio have demonstrated a mean tumor-to-marrow absorbed dose ratio of 63:1, which is an order of magnitude greater than the 6:1 ratio usually seen in conventional RIT (75). Further studies of pretargeted treatment with mAb NR-LU-10-streptavidin and 90Y-biotin in refractory colorectal adenocarcinoma demonstrated a mean tumor absorbed dose of 0.5 ± 0.2 cGy/MBq, which was significantly higher than the dose estimates to the kidney (0.3 ± 0.1 cGy/MBq) and to the bone marrow (0.1 mGy/MBq). Despite these impressive ratios, only 8% of patients showed a major response to therapy. Moreover, although hematologic toxicity was not a limiting factor, nonhematologic toxicities were significant (76). It is anticipated that dose-limiting toxicity with most multistep techniques will not be hematologic but probably renal. Renal toxicity poses additional issues, as nephropathy is usually not evident until several years after renal insult.
Promising results using the pretargeting approach have been seen in gliomas. Studies of biotinylated antitenascin mAb with 90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid biotin as the radionuclide have demonstrated a response as the sole therapy for recurrent disease as well as in the adjuvant setting (77).
Bispecific constructs that react against a radiometal–chelate complex, on the other hand, are unlikely to be immunogenic and therefore hold promise as therapeutic agents. Studies are now being planned that would use these novel systems to deliver higher amounts of relative tumor radiation-absorbed dose than would be possible with single-step radiolabeled-antibody methods (78,79).
STRATEGIES FOR FUTURE STUDIES
The RIT studies described above demonstrate that the early lack of success in solid-tumor RIT has been an impetus for the development of a plethora of constructs linked to radionuclides with varying radiobiologic characteristics. Patient-based dosing, fractionated therapy, and multistep targeting are just some of the methods being investigated to optimize treatment. A new generation of intelligently designed clinical trials is beginning. These trials share some characteristics:
Advances in Radiochemistry
These have led to successful clinical trials of labeling Auger emitters and α-emitters to conjugates and pharmaceuticals resulting in stable compounds. Also, the development of positron emitters such as copper, yttrium, and iodine has the potential to allow PET-based dosimetry. These will permit calculation of tumor radiation-absorbed doses permitting accurate dose delivery. Although 131I, 186Re, and 188Re are ideal radionuclides for external scintigraphy, surrogate γ-emitters must be used to evaluate the distribution and clearance of pure β-emitters. 111In has been considered to be an appropriate surrogate for 90Y. Their half-lives are almost identical, and both are readily incorporated into the same metal chelating agents. A recent study using PET to compare 86Y and 111In as surrogates for 90Y showed that, although 111In and 86Y have similar biodistributions, 86Y remained longer in organs such as bone (80). Given the slower clearance kinetics and bone-seeking properties of yttrium, 86Y is a more suitable surrogate for 90Y. This feature has been used to obtain extremely accurate dosimetry in bone-seeking radiopharmaceuticals (81) and in radiolabeled peptides (82).
Genetic Engineering
The development of nonimmunogenic antibody constructs, as well as pretargeting strategies such as an affinity-enhancement system, appears to enhance tumor-to-nontumor ratios and may increase radiation doses to tumor more selectively than do directly labeled antibodies. The pretargeting studies described above demonstrate that although development of this strategy is still in the early stages, it holds great potential. Approaches to genetic modification of antigen-binding constructs to make them suitable for RIT have focused on decreasing size, usually entailing a change to univalency, as with single-chain constructs. Moreover, production in bacterial systems results in deglycosylated proteins that may thus have suboptimal affinity or avidity characteristics. Making bivalent diabodies has resulted in molecules that are significantly retained in the kidney (83), thus raising the specter of unacceptable nephrotoxicity. Several groups have attempted to retain bivalency and minimize renal accumulation by adding other moieties—notably, the CH3 domain (84)—or adding cytotoxic agents such as tumor-necrosis factor dimers (85).
Understanding Radiobiology
Using radionuclides with physical characteristics tailored to the individual disease will improve our ability to treat tumors appropriately. Creating smart systemic targeted radiotherapy depends not only on carefully selecting appropriate antigen targets and antibody constructs but also on choosing radionuclides appropriate for the extent and type of disease. Choosing α-emitters for microscopic disease or energetic β-minus emitters for bulky disease, with use of emitter strengths that are proportional to disease bulk, will maximize efficacy while limiting side effects to normal tissue whenever possible. A prime concern with these multiple agents will be toxicity. It will therefore be important to combine nuclides with differing pharmacodynamic properties (e.g., combining bone-seeking β-minus–emitting 90Y with 67Ga, which has Auger emission and is cleared largely through the gastrointestinal tract) for therapy. The concept of sequential therapies with different nuclides based on tumor burden and other characteristics will also play a role in nuclide selection. There appears to be little doubt, however, that combination RIT will be as important to successful therapy as combination chemotherapy has been.
Combination Multimodality Therapy
Using chemotherapy and external-beam radiotherapy in conjunction with RIT earlier in the treatment of solid tumors has the potential to maximize the potential of RIT. Complementary modalities have great potential: A chemotherapeutic agent such as paclitaxel may not only have independent cytotoxicity but also act as a radiosensitizer and enhance the efficacy of RIT. We are investigating the potential of small-molecule inhibitors such as Iressa (Astra Zeneca) that can cause downstream metabolic effects changing tumor uptake of, as well as the susceptibility of tumor cells to, RIT. Agents that change the hypoxic fraction of tumors may also enhance RIT efficacy. Use of multiple modalities can cause changes in tumor permeability and vascularity that permit radioimmunoconjugates to access otherwise-unreachable tumor regions. The use of antiangiogenic agents is particularly of great interest: these agents (86) actually decrease tumor uptake of radioimmunoconjugate and, conversely, decrease egress of radioimmunoconjugate if the antiangiogenic agent is administered at an as yet undetermined time after RIT. These exciting studies are currently being designed in preclinical models and will soon be applied clinically.
Administration Schedule
Use of fractionated multidose RIT instead of single-larger-dose RIT may result in a slower rate of cell repopulation. Theoretic models have compared the effects of single-large-dose administration and rapid fractionation (87). Although a single large dose may produce a high rate of cell killing, fractionated therapy offers the advantages of lower toxicity and prolonged tumor response. In addition, similar to the rationale behind multimodality therapy, preceding doses may cause architectural changes in the tumor that may allow subsequent doses to target previously inaccessible regions. However, our studies with fractionated and single-large-dose RIT have shown no advantage to safety or improvement in total tumor radiation-absorbed dose. We are currently analyzing the data to determine whether the intratumoral distribution of radioactivity has changed (69). Nevertheless, fractionation may have promise when combined in a multimodality therapeutic strategy.
These strategies will pave the way toward tailored RIT for solid tumors that is both safe and effective. After the success of RIT for hematologic cancers, there is little doubt that RIT will find its niche in cancer therapy, both in the adjuvant situation and in bulky disease. Because cancer therapy must target both isolated cancer cells and bulky tumors, combination RIT, given either sequentially or simultaneously, will soon be a crucial player in the era of molecular therapeutics.
CONCLUSION
At a time when molecular medicine is becoming a reality, RIT has already proven its role in the treatment of non-Hodgkin’s lymphoma and is poised to find a role in the treatment of solid tumors. Humanized and other nonimmunogenic antigen-binding constructs by themselves are finding their place in cancer therapy, as are small molecules that modulate a variety of processes from cell surface receptor expression to intracellular enzyme activity. The toxicity inherent in radioactivity will dictate that the role of RIT eventually be weighed against the benefits and side effects of a multitude of targeted molecular therapies. Nevertheless, the result may well be treatments that exploit multiple cellular processes sequentially, each rendering the tumor more amenable to treatment by the next, with RIT finding a place in the vast new armamentarium that awaits the future of targeted therapy.
Footnotes
Received Apr. 20, 2004; revision accepted Jun. 10, 2004.
For correspondence or reprints contact: Chaitanya Divgi, MD, Weill Medical College of Cornell University, Memorial Sloan-Kettering Cancer Center, 1275 York Ave., New York, NY 10021.
E-mail: divgic{at}mskcc.org
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 131I-IITM and 211At-AITM: Two Novel Small-Molecule Radiopharmaceuticals Targeting Oncoprotein Metabotropic Glutamate Receptor 1
- 89Zr-DFO-J591 for ImmunoPET of Prostate-Specific Membrane Antigen Expression In Vivo
- Reduced Myelotoxicity with Sustained Tumor Concentration of Radioimmunoconjugates in Rats after Extracorporeal Depletion
- Antibody Pretargeting Advances Cancer Radioimmunodetection and Radioimmunotherapy