


Abstract
The aim of this study was to evaluate the possibility of decreasing the myelotoxicity associated with radioimmunotherapy (RIT) by extracorporeal depletion of radioimmunoconjugates (RIC) from the circulation. The optimal combination of radionuclide and the time interval between injection of the RIC and the subsequent extracorporeal depletion procedure was assessed in immunocompetent rats, with respect to both myelotoxicity and tumor concentration of RIC. Methods: Rats were injected with 177Lu- or 90Y-labeled antibody conjugate (mAb-DOTA-biotin) (mAb is monoclonal antibody; DOTA is 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid) and subjected to removal of the conjugate from the circulation by extracorporeal affinity adsorption treatment (ECAT) 12, 24, or 48 h after injection. Myelotoxicity was assessed by analysis of blood parameters for 10 wk. The effect of ECAT on the tumor concentration of RIC was evaluated in parallel by scintillation camera imaging in rats injected with 111In-labeled RIC. Results: ECAT reduced the blood content of RIC by 95%. Thus, myelotoxicity was significantly milder in animals subjected to ECAT than that in controls. The timing of ECAT influenced the rate and level of bone marrow recovery, with an earlier recovery in animals subjected to ECAT early after injection. The toxicity-reducing effect of ECAT was more distinct in animals injected with 177Lu-labeled RIC than in animals injected with 90Y-labeled RIC. Scintillation camera imaging of tumors before and after ECAT revealed that subjecting animals to ECAT at 12 h after injection considerably reduced the total activity in tumors (34%), whereas the effect was lower at both 24 h (18%) and 48 h (18%) after injection. Conclusion: ECAT can efficiently reduce myelotoxicity associated with RIT, and the concentration of RIC in tumor can be sustained, provided ECAT is performed at an optimal time after antibody administration. The choice of radionuclide for RIT in combination with ECAT is important, as the physical half-life is crucial for the toxicity-reducing potential of ECAT at a specific time.
The principle of radioimmunotherapy (RIT) consists of using monoclonal antibodies (mAbs) recognizing tumor-associated antigens as carriers of cytotoxic radionuclides to tumor tissue. In the treatment of lymphoma, the use of radioconjugated mAbs has been shown to be more effective than the naked antibody itself (1–3), which per se has an antitumoral effect (4). RIT of solid tumors has been less successful (5), which is primarily due to the poor accessibility and low radiosensitivity of solid tumors. Intact mAbs slowly diffuse from the vasculature into and through the tumor, resulting in slow, limited accretion of antibodies in solid tumors (6). The outcome is a low tumor-to-normal tissue activity ratio (T/N ratio), which can result in normal tissue toxicity when the high activities needed for therapy are administered. The dose-limiting factor is myelotoxicity caused mainly by the slow clearance of mAbs from the circulation. Numerous strategies have been proposed to overcome the low T/N ratio and to reduce the myelotoxicity associated with RIT (7,8).
Extracorporeal depletion of radioactivity in blood is one strategy to overcome the problem of low T/N ratios and reduce the toxicity in normal organs, and, specifically, extracorporeal affinity adsorption treatment (ECAT) has been shown to selectively and quickly eliminate radiolabeled antibodies from the blood (9). The selectivity of ECAT is based on the biotin-avidin system utilizing the high-affinity interaction between avidin and biotin. Antibodies are radiolabeled and biotinylated using a trifunctional protein reagent comprising 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid (DOTA) and biotin (10). By passing whole blood extracorporeally through a column coated with avidin, the radioimmunoconjugates (RIC) are adsorbed in the column and eliminated from the circulation. Our group has earlier demonstrated that ECAT can eliminate 90%–95% of RIC from the circulation of rats and significantly increase the T/N ratio in a syngeneic rat tumor model (9). Similar results were also obtained in patients (11). Several parameters must be considered when selecting the optimal time after injection for performing ECAT. Sufficient amounts of RIC should be allowed to accumulate in the tumor tissue before they are eliminated from the circulation. On the other hand, shortening the time between the injection of RIC and ECAT is crucial in limiting myelotoxicity. The effective half-life of the RIC is also important and must be considered when optimizing delay before ECAT. To investigate the importance of the these parameters, a series of experiments was performed. First, the myelotoxicity of 177Lu- or 90Y-labeled, tumor-binding RIC in combination with ECAT at different times after injection was investigated. Subsequently, the impact of ECAT, conducted at different times points after injection, on the concentration of RIC in tumor tissue was studied. The aim of the study was to investigate the effect of 2 radionuclides and the time interval between injection of the RIC and the subsequent ECAT in immunocompetent rats, with respect to the tumor concentration of RIC and myelotoxicity.
MATERIALS AND METHODS
mAb and Immunoconjugate
Chimeric (mouse/human) monoclonal IgG1 antibody BR96 (Seattle Genetics, Inc.), binding the tumor-associated glycoprotein Lewis Y (LeY) was used. LeY is expressed on the majority of human epithelial tumors, including breast, gastrointestinal (GI) tract, non–small cell lung, cervix, ovary, and some melanomas (12). As with the majority of tumor-associated mAbs, BR96 also reacts with some normal tissue, primarily the epithelial cells of the GI tract (12). BR96 was conjugated with the trifunctional chelator 1033 (MitraTag; Mitra Medical AB), carrying a DOTA moiety and a biotin moiety (10), as described previously (13,14). Briefly, 80 μg of the 1033 per mg BR96 were added to BR96 (in 50 mmol/L N-(2-hydroxyethyl)piperazine-N′-(2-ethanesulfonic acid) (HEPES), 1 mmol/L diethylenetriaminepentaacetic acid (DTPA) buffer, pH 8.5) and incubated for 2 h at room temperature and then overnight at 4°C. After conjugation, the conjugate was transferred to 0.25 mol/L ammonium acetate buffer (pH 5.3) by dialysis (Slide-A-Lyzer Dialysis Cassette; 10,000 molecular weight cutoff, Pierce), eliminating any free 1033. The number of 1033 molecules per BR96 molecule was determined by the 4′-hydroxyazobenzene-2-benzoic acid photometric method (15).
RIC
The same procedure was used for labeling with 177LuCl3 (MDS Nordion), 90YCl3 (MDS Nordion), and 111InCl3 (MDS Nordion). Both the 1033-BR96 in 0.25 mol/L ammonium acetate buffer and the radionuclide solutions were preheated at 45°C for 10 min. The 1033-BR96 solution was then added to the radionuclide-containing vials and incubated at 45°C for 15 min. The reaction was quenched with an excess of DTPA for 5 min. The 111In-1033-BR96 was purified, because of a radiochemical yield of <90%, using a PD-10 column (Sephadex G-25M; Amersham Biosciences AB). The radiolabeled immunoconjugates were diluted in 1% human serum albumin. The radiochemical purity of the labeled immunoconjugates was determined by instant thin-layer chromatography (ITLC) (1 × 9 cm silica gel–impregnated fiberglass sheet, eluted in 0.1 mol/L ethylenediaminetetraacetic acid). High-performance liquid chromatography (HPLC) (7.8 × 300 mm molecular sieving column, SEC S3000; Phenomenex, eluted in 0.05 mol/L sodium phosphate at 1.0 mL/min) was used to control the radiochemical purity and to detect signs of aggregation or fragmentation. To ensure that the labeling had not affected the biotin moiety of the 1033 molecule, the avidin-binding ability of the RIC was assessed. An adsorption column packed with approximately 0.3 mL Mitra avidin-agarose (Mitra Medical AB) was used. A 50-μL sample of RIC was added to the column and incubated for 10 min at room temperature. The column was washed 8 times with 0.5 mL phosphate-buffered saline containing 0.05% Tween 20, and the liquid from each washing was collected separately in tubes. The activity in the column and in each tube was measured with a NaI(TI) detector. The avidin-binding fraction was expressed as the percentage of radioactivity in the column in relation to the sum of the radioactivity in the tubes and the column.
Syngeneic Rat Tumor Model
Immunocompetent rats of the Brown Norwegian (BN) strain (Harlan) were used. As demonstrated by immunohistochemistry, BN rats express the BR96 epitope in some normal tissues, such as the GI epithelium, hence mimicking the human situation (Hans-Olov Sjögren and Ingrid Hellström, oral communication, January 2003). BN7005-H1D2 is a single-cell clone of a rat colon carcinoma originally induced by 1,2-dimethylhydrazine in a BN rat. BN7005-H1D2 cells were cultured in RPMI 1640 medium (EuroClone) supplemented with 10% fetal calf serum (FCS), 1% sodium pyruvate, 1% 1 mol/L HEPES buffer solution, and 14 mg/L gentamicin (EuroClone) at 37°C in a humidified atmosphere with 5% CO2. Cells were washed in saline, trypsinized, and washed in medium plus 10% FCS. Animals were inoculated subperitoneally with 3 × 105 cells (in 50 μL of medium). Experiments to investigate the tumor accretion of mAbs were initiated 12–14 d after inoculation (tumor size, 10 × 10 mm). The animals were kept under standard conditions, were fed standard pellets, and had access to fresh water. Studies were conducted in compliance with Swedish legislation on animal rights and protection and were approved by the Swedish Ethics Committee.
ECAT
The extracorporeal system included a 403U/C12 pump (W-Marlow Alitea AB) with a 15-cm silicone tube (1.6-mm inner diameter, 6.35-mm outer diameter). The column housing consisted of a modified 2-mL polypropylene syringe (9 × 30 mm) with a 72-μm filter at the bottom. The column was packed with 1.5 mL avidin-agarose (Mitra Medical AB) with about 0.5 mL NaCl above as an extra air trap. Polyvinyl chloride (PVC) tubing (1-mm inner diameter) was used for medical lines. An air trap consisting of PVC tubing (9.5-mm inner diameter) was connected to trap any air bubbles before the blood was returned to the animals. The extracorporeal circuit had a volume of about 3.5 mL. Before ECAT, the system was flushed with heparin solution (20 IU/mL heparin in 9 mg/mL NaCl) as an anticoagulant. The system is illustrated in Figure 1.
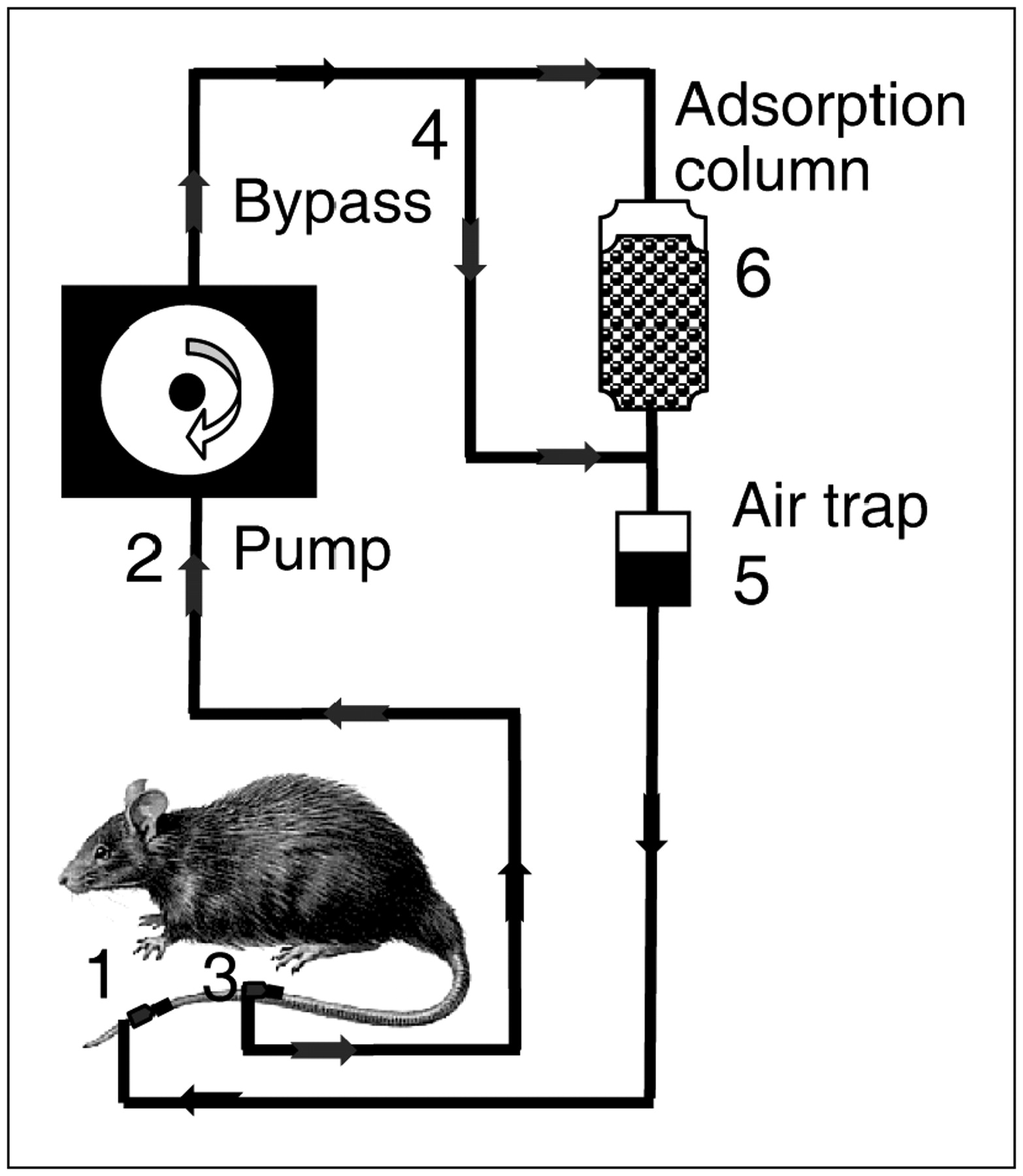
Experimental ECAT setup. Cannula is inserted into one of lateral tail veins (1) for return of blood and is connected to extracorporeal system (regulated by the pump (2)). For blood access, another cannula is inserted into ventral tail artery (3). When cannulas are inserted, extracorporeal circulation is begun in bypass mode (4) without column connected. Once the circuit is filled with blood and any air bubbles in circuit have been collected in the air trap (5), column (6) is connected to the circuit and affinity adsorption is begun.
Thirty minutes before insertion of the cannulas (Neoflon, 0.7 × 19 mm; Becton Dickinson), a 2% glyceryl nitrate salve (The National Cooperation of Swedish Pharmacies) was applied to the entire tail of each rat to dilate the blood vessels. The animals were anesthetized with forene (Isofluran; Abbott Scandinavia AB) using a U-400 anesthesia unit (AgnTho's AB–for Biomedical Research). The rats were first anesthetized in a 1.4-L induction chamber (3.3% Isofluran, 575 mL/min air flow) and then placed on a heating pad (30°C). Anesthesia was sustained through anesthesia masks connected to the same anesthesia unit as the induction chamber. A cannula was carefully inserted into one of the lateral tail veins (1–2 cm from the tip of the tail) for the return of blood. The cannula was secured to the tail with adhesive tape and connected to the extracorporeal system. To prevent coagulation and to confirm that the cannula was inserted correctly, heparin solution from the extracorporeal circuit was infused for a few seconds and then stopped (regulated by the pump). For blood access, another cannula was inserted into the ventral tail artery, approximately 5 cm from the tip of the tail. This cannula is accurately inserted when there is a continuous flow of blood through the cannula. Before connecting the cannula to the extracorporeal circuit, a blood sample was collected. As soon as the artery cannula was connected to the system, the extracorporeal circulation was begun in bypass mode (column not connected).
The heparin solution present in the system was infused to prevent clotting, and the whole circuit was filled with blood bypassing the column. When the circuit was filled with blood and any air bubbles in the circuit had been collected in the air trap, the avidin column was connected to the circuit and the affinity adsorption was begun. Blood was pumped through the column at a rate of 0.4 mL/min. ECAT was performed on 6 rats in parallel. During ECAT, the rats were anesthetized at a lower level of anesthesia (2.0% Isofluran; 575 mL/min air flow) and placed on heating pads (30°C) to keep them warm. After about 2 h (approximately 3 blood volumes; blood volume estimated to be 65 mL/kg body weight) of affinity adsorption, the procedure was stopped and the blood in the circuit was returned to the rat. A blood sample was collected from the arterial cannula before withdrawal of the cannulas. The tail was compressed to stop bleeding.
Effects of ECAT on Bone Marrow Toxicity
Non–tumor-bearing male BN rats (230–250 g) were used in this experiment to evaluate various intervals between injection of the RIC (177Lu or 90Y) and subsequent ECAT with regard to myelotoxicity. The rats were injected intravenously with 150 μg 177Lu-1033-BR96 (activity of 800 MBq/kg body weight) or 150 μg 90Y-1033-BR96 (activity of 400 MBq/kg body weight). On the basis of earlier studies, these activities were expected to result in dose-limiting toxicity. The rats were subjected to ECAT at different times after injection according to Table 1. Blood samples were collected from the tail artery twice a week for 10 wk after injection and white blood cell counts (WBC), platelet counts (PLT), and red blood cell counts (RBC) were analyzed in a Medonic Cell Analyzer-Vet CA530 (Boule Medical) to evaluate the myelotoxicity. At the time of blood sampling, the body weight and physical condition of the animals were recorded.
Experimental Setup, ECAT Efficiency, and Weight Loss in Myelotoxicity Study
Tumor Accretion
Tumor-bearing male BN rats weighing 230–250 g were used to evaluate various intervals between injection of the RIC and the ECAT procedure with regard to tumor accretion. 111In was chosen because of its favorable imaging properties. Rats were injected intravenously with 150 μg 111In-1033-BR96 labeled with 40 MBq 12–14 days after inoculation with tumor cells. The rats were subjected to ECAT at different times after injection according to Table 2. Scintillation camera imaging was performed before and after ECAT using a scintillation camera (SMV DST-Xli; Sopha Medical) equipped with a medium-energy collimator to determine whole-body activity and tumor activity. A 25% energy window was centered over the 172-keV photopeak and a 20% energy window was centered over the 245-keV photopeak. The activity change in the tumors after ECAT was investigated by defining a region of interest (ROI) covering the tumor in the images before ECAT and then comparing the same ROI in the images after ECAT. After correction for the decay of 111In, the activity change in tumors was calculated by comparing the activity before and after ECAT. An estimate of the blood content in the tumors was made using the same ROI in the images taken immediately after injection of the RIC. This activity was then corrected for effective half-life.
Experimental Setup and Activity Reduction After ECAT in Tumor Accretion Study
Calculations of Theoretic Accumulated Activities in Blood and Tumor with Simulated ECAT
Because the activity concentration in blood can be used for bone marrow dosimetry (16), we calculated the area under the curve (AUC) for blood activity based on pharmacokinetic and biodistribution data obtained in previous studies (14) to predict the effect of ECAT on the myelotoxicity after RIT. Bone marrow dosimetry was not performed because neither the red marrow blood ratio (RMBLR) nor the appropriate S values are known with sufficiently high accuracy. ECAT at 12, 24, and 48 h after injection with 177Lu- or 90Y-labeled RIC was simulated by a reduction of the blood activity of 95%, and the AUCs for tumor and blood activity were calculated. It was assumed that tumor activity does not increase after the assumed time of ECAT and that the ECAT does not decrease the tumor activity reached at the time of ECAT. The tumor-to-blood activity ratio (T/B ratio) after ECAT at each time was then calculated. The calculations were performed using GraphPad PRISM software (GraphPad Software, Inc.). The calculated AUC for blood and tumor were used for comparison analyses with the achieved blood toxicity and tumor uptake in the present investigation.
Statistical Analysis
All data are presented as median values unless stated otherwise. Data between groups were compared using the Kruskal–Wallis test with the Dunn post-test when appropriate. Analyses were performed with GraphPad PRISM software. P < 0.05 was considered statistically significant.
RESULTS
Preparation of RICs
After conjugation, the average number of 1033 molecules per BR96 molecule was determined to be 2.6. The specific activity was 166.5 MBq/nmol for 177Lu-1033-BR96, 137.8 MBq/nmol for 90Y-1033-BR96, and 38.1 MBq/nmol for 111In-1033-BR96. ITLC showed the radiochemical purity to be 98% for 177Lu-1033-BR96, 91% for 90Y-1033-BR96, and 99% for 111In-1033-BR96. No aggregation or fragmentation was observed with HPLC. The avidin-binding fraction exceeded 90% for the 3 RICs at the time of injection.
Evaluation of Bone Marrow Toxicity After ECAT at Different Times After Injection
ECAT.
The extracorporeal affinity adsorption procedure was conducted 12, 24, or 48 h after the injection of 177Lu-1033-BR96 or 90Y-1033-BR96, with 3 rats in each of the 6 groups (Table 1). Blood was pumped at a rate of 0.4 mL/min for 2 h. Blood samples taken before and after ECAT were analyzed for activity content. The efficacy of the adsorption was calculated in percentage (Table 1). A mean of 95% (range, 91%–97%) of the activity in the blood was eliminated at all time points.
Body Weight Loss.
During the first 7 days after injection of RIC the animals lost weight, reaching a nadir on days 5–7 (Table 1). The weight loss was more profound in the groups of animals receiving 90Y-1033-BR96 than in the groups receiving 177 Lu-1033-BR96. After day 7, all animals began to gain weight. The animals in the control groups (not subjected to ECAT) lost weight a second time 6–7 weeks after injection and displayed symptoms of dehydration (impaired skin elasticity). Dose-limiting toxicity was reached in the control groups, and these rats were killed because of their poor condition 8–9 weeks after injection (>20% weight loss).
Blood Parameters.
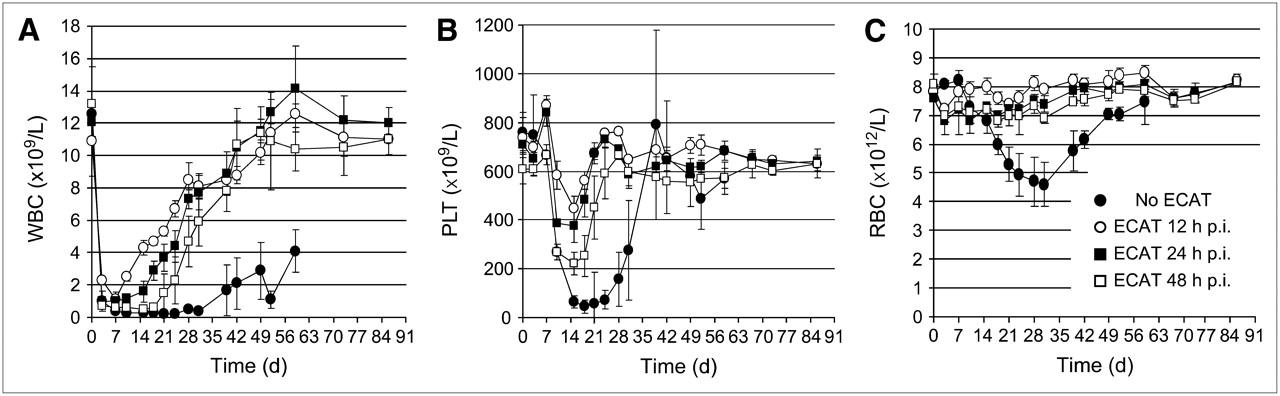
Bone marrow toxicity was monitored by quantification of WBC, PLT, and RBC. For both 177Lu-1033-BR96 and 90Y-1033-BR96, all groups showed a dramatic decrease in WBC during the first week after injection (falling to 1%–10% of initial values) (Figs. 2A and 3A). A relationship was seen between the time of ECAT and the recovery in WBC (Figs. 2A and 3A), particularly in the animals injected with 177Lu-1033-BR96 (Fig. 2A). In animals receiving 177Lu-1033-BR96 (Fig. 2A), a clear pattern was seen between the start of recovery of WBC and the time point for ECAT, with a statistically significant difference (P < 0.05) between the different times, 12 h after injection on day 10, 24 h after injection on day 15–18, and 48 h after injection on day 21–24. All animals subjected to ECAT had recovered WBC 2 mo after injection. The control group (not subjected to ECAT) continued to show low WBC (20% of initial WBC) after 2 mo, and these animals were sacrificed 8–9 wk after injection.

WBC (A), PLT (B), and RBC (C) as function of time after injection (p.i.) when rats were injected with 800 MBq/kg 177Lu-conjugated, biotinylated BR96 and subjected to ECAT 12 h after injection (○), 24 h after injection (▪), and 48 h after injection (□). Results from control animals (not subjected to ECAT) are also plotted (•).

WBC (A), PLT (B), and RBC (C) as function of time after injection (p.i.) when rats were injected with 400 MBq/kg 90Y-conjugated, biotinylated BR96 and subjected to ECAT 12 h after injection (○), 24 h after injection (▪), and 48 h after injection (□). Results from control animals (not subjected to ECAT) are also plotted (•).
Animals subjected to ECAT 12 h after injection of 90Y-1033-BR96 began to recover on day 21, while the 3 other groups (controls, ECAT 24 h after injection, and ECAT 48 h after injection) did not start to recover until days 30–35 (Fig. 3A). Animals belonging to the ECAT 12-h postinjection group began to recover significantly earlier (P < 0.05) regarding WBC than the other groups. No significant difference in start of recovery of WBC was seen between the ECAT 24-h postinjection group, the ECAT 48-h postinjection group and the control group for rats injected with 90Y-1033-BR96. However, the control group recovered slower than all animals subjected to ECAT. The control group without subsequent ECAT had low WBC (45% of initial WBC) after 2 mo, and these rats were sacrificed 8–9 weeks after injection.
The effects on PLT showed a clear relationship between the time of ECAT and both the nadir (P < 0.05) and the time to recovery (P < 0.05), with a higher nadir and a faster recovery the earlier ECAT was performed. This pattern was seen for both 177Lu-1033-BR96 and 90Y-1033-BR96 (Figs. 2B and 3B). However, as for WBC, the effect of ECAT was more apparent in animals injected with 177Lu-1033-BR96. All animals showed a recovery to their initial PLT after 2 mo, and no bleeding was detected during the study period.
No substantial decrease in RBC was seen in rats injected with 177Lu-1033-BR96 and subjected to ECAT. The control group, however, displayed a decrease of 40% relative to the initial value, with a nadir on day 31 after injection (Fig. 2C). A tendency toward a relationship between the decrease in RBC and the time of ECAT was seen in rats injected with 90Y-1033-BR96 (Fig. 3C).
Influence of ECAT on Tumor Concentration of RIC
After correction for the decay of 111In, the reduction of RIC in the tumor after ECAT was 34% for animals subjected to ECAT 12 h after injection, 18% for ECAT 24 h after injection, and 18% for ECAT 48 h after injection (Fig. 4). The whole-body clearance of RIC was affected by the timing of ECAT, with a higher clearance the earlier ECAT was performed (Table 2). The activity content in tumors represented by RIC in tumor blood vessels at the time of ECAT was calculated to be 33% (range, 25%–47%) of total tumor activity for animals subjected to ECAT 12 h after injection, 17% (range, 12%–23%) for animals subjected to ECAT 24 h after injection, and 13% (range, 10%–16%) for animals subjected to ECAT 48 h after injection.

Scintillation camera images (A) of tumor in 1 animal in each group (12, 24, and 48 h after injection) before ECAT (top row) and after ECAT (bottom row) showing that activity in surrounding tissues is efficiently eliminated by ECAT, whereas activity in tumors is sustained. Reduction in activity in tumors is shown for groups (n = 6) subjected to ECAT 12, 24, and 48 h after injection of RIC (B).
Calculations of Theoretic Accumulated Activities in Blood and Tumor with Simulated ECAT
When ECAT was simulated at different times after injection, the AUC for blood activity was more reduced the earlier ECAT was simulated. The AUC for tumor activity was reduced at the earliest time point, 12 h after injection, but was unaffected at 24 and 48 h after injection, as maximal tumor uptake is reached at 24 h in this particular tumor model. These results were similar for both 177Lu-labeled (Figs. 5A–5D) and 90Y-labeled RIC. According to these calculations, the T/B activity ratio was highest for 177Lu when ECAT was simulated 24 h after injection and for 90Y when ECAT was simulated 12 h after injection. The T/B activity ratio was 2.0 for 177Lu at ECAT 24 h after injection and 1.7 for 90Y at ECAT 12 h after injection These calculations corresponded well with the achieved in vivo data, which showed a sustained tumor concentration after ECAT when corrected for RIC in blood vessels (Fig. 4) and significantly reduced myelotoxicity when ECAT was performed 24 h after injection of 177Lu-BR96 and 12 h after injection of 90Y-BR96 (Figs. 2 and 3).
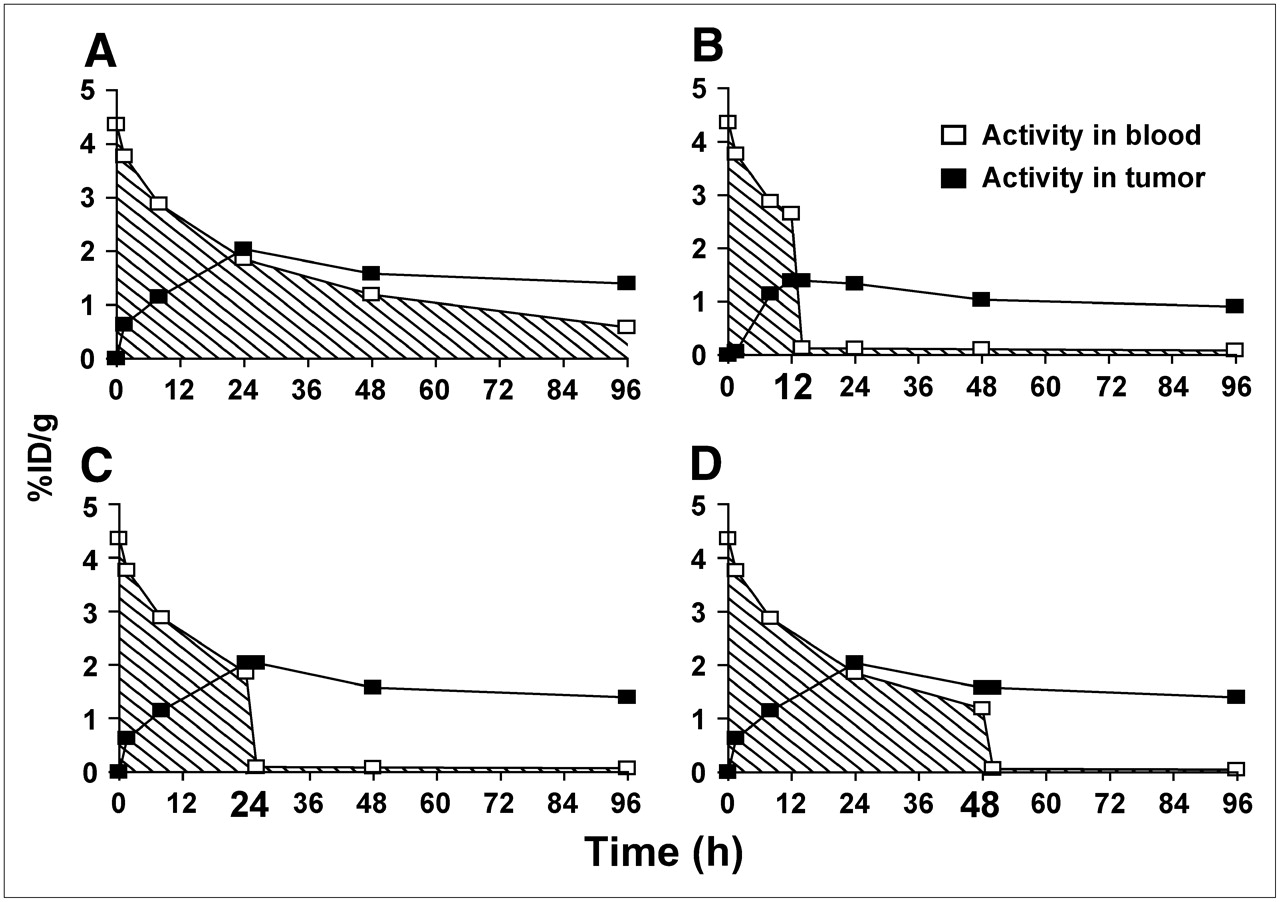
AUC for blood (hatched area) and tumor activity is plotted for control animals not subjected to ECAT (A), ECAT simulated at 12 h after injection (B), at 24 h after injection (C), and at 48 h after injection (D) for animals injected with 177Lu-conjugated, biotinylated BR96. %ID/g = percentage injected dose per gram.
DISCUSSION
The ECAT procedure is unique compared with other T/N improving strategies, in that the elimination of RIC from the blood is fast and effective, thus decreasing the exposure of radiation-sensitive tissues. Some of the disadvantages associated with 2- or 3-step pretargeting could be circumvented or reduced, such as clinical complexity with regard to optimization of each of the injections, degradation of mAbs due to the long interval between the injection of mAbs and subsequent targeting of molecules, and the high absorbed dose in the reticuloendothelial system. In this study, ECAT reduced blood activity by approximately 95%. As a result, the myelotoxicity was significantly milder in animals subjected to ECAT than in control animals not subjected to the procedure. In the control groups, dose-limiting toxicity was reached with the administered activities of 800 MBq/kg 177Lu or 400 MBq/kg 90Y. These control animals displayed late-phase toxicity, resulting in acute weight loss combined with signs of dehydration and had to be sacrificed 8–9 wk after injection. The cause of these symptoms was not yet studied but is believed to be the prolonged suppression of neutrophils in combination with radiation-induced intestinal damage (cell loss and altered crypt integrity), resulting in bacterial infection and loss of electrolytes and fluid (17,18). The control animals had not recovered in WBC counts 2 mo after injection. No late-phase toxicity or body weight loss was seen in the animals subjected to ECAT after 6 mo, at which time the study was terminated. The animals showed complete recovery with regard to blood parameters within 2 mo after injection.
As expected, the timing of ECAT influenced the rate and level of bone marrow recovery, with earlier recovery in animals subjected to ECAT early after injection. The effect of ECAT in reducing myelotoxicity was more profound in animals injected with 177Lu-1033-BR96 than in animals injected with 90Y-1033-BR96. Although the groups subjected to ECAT 24 and 48 h after injection of 90Y-1033-BR96 had significantly reduced bone marrow toxicity compared with the control groups, only the group subjected to ECAT 12 h after injection of 90Y-1033-BR96 displayed a major reduction in toxicity comparable to the effects seen in all groups subjected to ECAT after injection of 177Lu-1033-BR96. This indicates that the physical half-life of the radioisotope used for RIT affects the toxicity-reducing potential of ECAT at a specific time after injection. In this model the longer physical half-life of 177Lu versus 90Y (6.7 vs. 2.7 d) is better suited for RIT in combination with ECAT, as only a fraction of the absorbed dose has been deposited in the bone marrow prior to ECAT 24 h after injection when the maximum tumor uptake is attained. The longer particle range of 90Y (maximum penetration depth, 12 mm) also contributes to a higher absorbed dose in the bone marrow due to cross-dose from the surrounding tissue. The contribution of cross-dose to the total absorbed dose in the bone marrow will be lower for 177Lu because of its shorter particle range (maximum penetration depth, 1.5 mm). This difference in toxic effect of cross-dose is more evident in small animals and less important in humans because of the greater distances between adjacent organs (19).
Scintillation camera imaging of tumors before and after ECAT revealed that subjecting animals to ECAT 12 h after injection considerably reduced the activity in tumors (34%), whereas the effect was lower at 24 h (18%) and 48 h (18%) (Fig. 4). Imaging demonstrated that the activity in tumor blood vessels represents approximately 33%, 17%, and 13% of the total tumor activity, measured by scintillation camera imaging, in this tumor model 12, 24, and 48 h after injection, respectively. This indicates that at 24 and 48 h after injection, ECAT eliminates only the RIC in tumor blood vessels and maximal tumor accumulation of RIC is reached. However, at 12 h after injection fewer RIC have penetrated into the extravascular tumor tissue and a greater fraction of tumor activity is represented by RIC in the blood vessels.
According to the AUC calculations (Fig. 5), the most favorable AUC ratios for the T/B ratio would be obtained when the ECAT procedure is performed 24 h after injection of 177Lu-BR96 and 12 h after injection of 90Y-BR96. These calculations corresponded well with the in vivo data, which showed significantly reduced myelotoxicity when ECAT was performed at these times (Figs. 2 and 3). A preliminary study in this animal model shows that it is possible to increase the maximal tolerable dose (MTD) of 177Lu-BR96 2 times and the MTD of 90Y-BR96 1.5 times when ECAT is performed 24 h after injection. These results correspond well with the calculations presented in Figure 2. This is supported by an ongoing dose-escalating phase-1 study investigating ECAT of biotinylated and 90Y-labeled rituximab in patients with refractory B-cell lymphomas, where a dose level of 21 MBq/kg has been evaluated without any signs of more severe hematologic toxicity (Ola Lindén and Jan Tennvall, oral communication, July 2006). This finding should be compared with the established MTD of 15 MBq/kg with 90Y-ibritumomab tiuxetan (Zevalin; Biogen Idec) without ECAT in similar patients.
Several methods of reducing the side effects of RIT have been investigated in mice. Examples are secondary antibodies (20,21), avidin chase (22,23), antioxidant vitamins (24), and hemoregulatory peptides (25). Results show that these strategies can reduce the myelotoxicity to a certain extent. However, the most successful results have been seen when RIT is combined with peripheral blood progenitor cell transfusions (PBPC). In a clinical study (26) it was found to be possible to increase the MTD of 131I-labeled antibodies 2.5 times in combination with PBPC. By using ECAT, it is also possible to reduce the toxicity in other radiosensitive organs at higher doses—that is, liver, lungs, and kidneys. ECAT has been evaluated in the clinic and shown to be both safe and effective in reducing radioactivity in critical organs (11), but it still remains to be elucidated how much the MTD of radiolabeled antibodies can be increased when combined with ECAT.
CONCLUSION
Our studies demonstrate that ECAT can efficiently reduce myelotoxicity associated with RIT and that the concentration of RIC in the tumor can be sustained provided that ECAT is performed 24 h after antibody administration.
When ECAT was performed 12 h after injection, the radioactivity in the tumor was significantly reduced, reflecting a reduction of RIC in the tumor blood vessels. With the present study design the toxicity-reducing effect of ECAT was more evident in animals injected with 177Lu-labeled RIC than in animals injected with 90Y-labeled RIC, indicating that the choice of radionuclide for RIT in combination with ECAT is crucial for the toxicity-reducing potential of ECAT at a specific time. The results of this study indicate that, with optimization of these parameters, ECAT offers the potential to increase the MTD in RIT considerably.
Acknowledgments
We thank Dr. Peter Senter (Seattle Genetics, Seattle, WA) for kindly providing the mAb BR96. Furthermore, we express our gratitude to Prof. Scott Wilbur (University of Washington, Seattle, WA) for having developed the MitraTag. We also thank Lars Lindgren for excellent technical assistance. This research was supported by grants from The Swedish Research Council, The Swedish Cancer Society, The Swedish Medical Society, Mrs. Berta Kamprad's Foundation, Gunnar Nilsson's Foundation, Lund University Medical Faculty Foundation, and The Lund University Hospital Fund.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 15, 2006.
- Accepted for publication November 3, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.