


Abstract
Therapeutic efficacy in radioimmunotherapy depends, among other things, on the choice of the radionuclide. The aim of the present study was to determine the most suitable radionuclide for radioimmunotherapy with monoclonal antibody MN-14 to carcinoembryonic antigen in an experimental model of small peritoneal metastases of colorectal origin. Methods: In nude mice with intraperitoneal LS174T tumors (diameter, 1–3 mm), the biodistributions of MN-14 labeled with 131I (131I-MN-14), 186Re-mercaptoacetyltriglycine (186Re-MN-14), and 88Y-diethylenetriaminepentaacetic acid (DTPA) (88Y-MN-14) after intravenous and intraperitoneal administration were determined. Subsequently, the therapeutic efficacies of equally toxic activity doses of 131I-MN-14 (9.25 MBq per mouse), 186Re-MN-14 (9.25 MBq per mouse), 90Y-MN-14 (3.15 MBq per mouse), and MN-14 labeled with 177Lu-DTPA (177Lu-MN-14) (8.33 MBq per mouse) after intraperitoneal administration were determined. Results: Each of the radioimmunoconjugates preferentially accumulated in tumor nodules, both after intravenous administration and after intraperitoneal administration. Values for clearance from blood were similar for all radioimmunoconjugates. The uptake of 88Y-MN-14 in the liver and spleen was significantly higher than the uptake of 131I-MN-14 or 186Re-MN-14. Maximal uptake values (mean ± SD) in tumors were 58 ± 7 percentage injected dose per gram of tissue (%ID/g) for 131I-MN-14 (24 h after administration), 83 ± 19 %ID/g for 186Re-MN-14 (72 h after administration), and 148 ± 89 %ID/g for 88Y-MN-14 (192 h after administration). Dosimetric analysis of the biodistribution data estimated that the radiation doses guided to the tumor by intraperitoneally administered 131I-MN-14, 186Re-MN-14, 90Y-MN-14, and 177Lu-MN-14 were 150, 100, 45, and 200 Gy, respectively. The median survival time of control mice, treated with unlabeled MN-14, was 42 d, whereas the median survival times of mice treated with 131I-MN-14, 186Re-MN-14, 90Y-MN-14, and 177Lu-MN-14 were 100 d (range, 58–142; P < 0.0001), 72 d (range, 46–84; P = 0.0002), 82 d (range, 46–142; P < 0.0001), and 136 d (range, 56–142; P < 0.0001), respectively. At the completion of the experiment (142 d after tumor cell inoculation), no residual disease was found in 8 of 9 long-term survivors (131I, n = 3; 90Y, n = 1; and 177Lu, n = 4). Conclusion: The uptake of 88Y-MN-14 in small peritoneal LS174T xenografts was higher than the uptake of 131I-MN-14 or 186Re-MN-14. The present study indicates that 131I and 177Lu are the most suitable radionuclides for the radioimmunotherapy of small peritoneal metastases.
Radioimmunotherapy—the use of radiolabeled monoclonal antibodies (mAbs) against tumor-associated antigens—has not fulfilled its promise for solid cancers as it has for hematologic malignancies. Besides the limited radiosensitivity of carcinomas compared with hematologic malignancies, solid tumors are generally characterized by a limited vascular supply, heterogeneous uptake of the antibodies in the tumors, and elevated interstitial pressure in combination with a relatively long transport distance in the interstitium (1). Radioimmunotherapy therefore is considered more suitable for the treatment of microscopic or minimal residual disease, allowing radiolabeled mAbs to achieve uptake in tumors high enough to result in tumoricidal radiation doses.
An important issue in radioimmunotherapy is the selection of the radionuclide. β-Emitting isotopes, such as 131I and 90Y, are the most commonly used radionuclides in radioimmunotherapy. 186Re and 177Lu are β-emitting radionuclides that have been considered for radioimmunotherapy more recently. The physical characteristics of these 4 radionuclides, however, differ significantly with respect to half-life, the presence of γ-radiation, the energy of the β-emission, and consequently the maximum depth of penetration of the β-particles in tissue, as summarized in Table 1.
Physical Characteristics of β-Emitters Used Most Often in Radioimmunotherapy
Koppe et al. previously characterized an experimental model of small peritoneal metastases with the human colon carcinoma cell line LS174T (2). In this model, radioimmunotherapy with mAb MN-14 labeled with 131I was very effective in delaying the development of peritoneal carcinomatosis, even at relatively low activity doses. Therapeutic efficacy in this model might be improved by use of other radionuclides with more favorable characteristics for radioimmunotherapy.
In the present study, experiments were performed with the aim of selecting the most suitable radionuclide for the radioimmunotherapy of small peritoneal metastases of colorectal origin. For this purpose, a series of experiments first was performed to investigate the biodistribution of MN-14 labeled with 131/125I, 186Re, or 88Y in nude mice with small intraperitoneal xenografts of colon cancer. Then, the therapeutic efficacy of MN-14 labeled with 131I, 186Re, 90Y, or 177Lu was assessed and correlated with the results of the biodistribution experiments.
MATERIALS AND METHODS
Animal Model for Small Peritoneal Metastases
Male nude BALB/c mice (Charles River Laboratories), 8–9 wk old and weighing 20–25 g, were used in the experiments. Mice were allowed to become accustomed to laboratory conditions for at least 1 wk before experimental use. Mice were housed under nonsterile standard conditions (temperature, 20°C–24°C; relative humidity, 50%–60%; 12 h of light and 12 h of dark) in filter-topped cages (5 mice per cage), with free access to animal chow (Snif Voer) and water. Peritoneal metastases were induced as described previously (2). In brief, mice were inoculated intraperitoneally with 106 LS174T cells (CCL 188; American Type Culture Collection) suspended in 500 μL of RPMI 1640 medium in a 2.5-mL syringe by use of a 23-gauge needle. In this model, the first macroscopic tumor nodules are seen 7–10 d later, whereas bulky peritoneal carcinomatosis develops 3–5 wk after tumor cell inoculation. All experiments were approved by the institutional animal welfare committee of the University Medical Center Nijmegen and were conducted in accordance with the principles set forth by the Revised Dutch Act on Animal Experimentation (1997).
mAb
Murine mAb MN-14 is a high-affinity (association constant, 109 L/mol) class III anti–carcinoembryonic antigen (CEA) immunoglobulin G1 (IgG1) antibody produced by a hybridoma cell line culture kindly provided by Immunomedics, Inc. (3). The antibody was purified by protein A chromatography as described previously (4). Purity was checked by fast protein liquid chromatography on a Biosep 3000 column (Phenomenex); elution was done with phosphate-buffered saline (PBS; pH 7.2) at 1 mL/min.
Radioiodination
The antibody was radioiodinated with 125I or with 131I (Amersham Biosciences or MDS Nordion, respectively) by use of the IODO-GEN method (1,3,4,6-tetrachloro-3α,6α-diphenylglycoluril; Pierce Biotechnology, Inc.) (5). Briefly, the antibody and 125I or 131I were incubated at room temperature in 85 μL of PBS (0.10 mol/L; pH 7.4) in a glass vial coated with 50–100 μg of IODO-GEN. After 10 min, the reaction was stopped by the addition of 100 μL of a saturated tyrosine solution. The reaction mixture then was separated on a PD-10 column (Amersham Biosciences); elution was done with PBS and 0.5% bovine serum albumin (BSA). The labeling efficiency of all of the radioiodination reactions exceeded 90%. In the biodistribution experiments, the specific activities of 125I-MN-14 and 131I-MN-14 were 41 and 78 kBq/μg, respectively. The specific activity of 131I-MN-14 in the therapy experiments was 0.96 MBq/μg.
186Re Labeling
186ReO4− was obtained from Tyco Mallinckrodt Medical BV. The specific activities of the ReO4− batches used in the biodistribution and therapy experiments were 37 and 65 GBq/mg, respectively. The antibody was labeled with 186Re by use of S-benzoyl-mercaptoacetyltriglycine (S-benzoyl-MAG3) as a chelator as described by Visser et al. (6). Briefly, 180 μg of MAG3 (1.0 mg/mL) was incubated with 150 μL of Na2CO3 (1.0 mol/L), 150 μL of Na2SO3 (100 mg/mL), and 696 MBq of 186ReO4− (100 μL) in a boiling water bath (10 min). The solvent was evaporated, and the solid phase was incubated for another 15 min. After derivatization of 186Re-MAG3 with 2,3,5,6-tetrafluorophenol (100 mg/mL in acetonitrile:H2O, 9:1), the derivatized 186Re-MAG3 ester was purified on a Sep-Pak C18 cartridge (Waters Corp.) and then reacted with 900 μg (biodistribution experiments) or 400 μg (therapy experiments) of a concentrated MN-14 solution at pH 9.5. The mean numbers of MAG3 groups per MN-14 IgG molecule in the biodistribution and therapy experiments were 2.6 and 4.1, respectively. The 186Re-MAG3-MN-14 conjugate (hereafter referred to as 186Re-MN-14) was purified on a PD-10 column. The overall labeling efficiencies of the 186Re labeling procedures performed in the biodistribution and therapy experiments were 36% and 18%, respectively, resulting in specific activities of 0.12 and 0.33 MBq/μg, respectively.
88Y, 90Y, and 177Lu Labeling
All conjugation and labeling procedures were performed under strict metal-free conditions. To allow labeling of the antibody with 88Y, 90Y, and 177Lu, MN-14 was conjugated with isothiocyanatobenzyl-diethylenetriaminepentaacetic acid (ITC-DTPA; Macrocyclics). Briefly, ITC-DTPA was conjugated to MN-14 in NaHCO3 buffer (0.1 mol/L; pH 8.2) by use of a 100-fold molar excess of ITC-DTPA as described by Ruegg et al. (7) with minor modifications (conjugation period of 1 h at room temperature). The DTPA-MN-14 conjugate was purified by extensive dialysis against ammonium acetate buffer (0.1 mol/L; pH 5.0). The number of DTPA ligands per antibody molecule was determined by the method of Hnatowich et al. (8). The purified DTPA-MN-14 conjugate (ratio of DTPA to MN-14, 2.5:1; 0.8 mg/mL) was incubated with 88Y (Isotope Products Europe Blaseg), 90Y (The Perkin-Elmer Corp.), or 177Lu (University of Missouri Research Reactor) in ammonium acetate buffer (0.1 mol/L; pH 5.4) at room temperature for 20 min. The specific activities of the 88Y-DTPA-MN-14, 90Y-DTPA-MN-14, and 177Lu-DTPA-MN-14 preparations (hereafter referred to as 88Y-MN-14, 90Y-MN-14, and 177Lu-MN-14, respectively) were 48.1 kBq/μg, 370 kBq/μg, and 1.48 MBq/μg, respectively.
Quality Control for Radiolabeled Preparations
All radiolabeled MN-14 preparations were purified by gel filtration on a PD-10 column; elution was done with PBS supplemented with 0.5% BSA. For all preparations, the amount of free radiolabel was determined by instant thin-layer chromatography with silica gel strips (Gelman Sciences, Inc.) and with citrate buffer (0.1 mol/L; pH 6.0) as the mobile phase. The radiochemical purity of all radiolabeled antibody preparations used in the experiments exceeded 96%.
The immunoreactive fraction (IRF) of the radiolabeled MN-14 preparations, except for 90Y-MN-14, at an infinite antigen excess was determined with freshly trypsinized LS174T cells essentially as described by Lindmo et al. (9) with minor modifications. Briefly, a fixed amount of labeled antibody (10,000 cpm) was incubated with increasing concentrations of LS174T tumor cells (1.2 × 106–20 × 106 cells per milliliter) in 0.5 mL of binding buffer (RPMI 1640 medium containing 0.5% BSA and 0.05% NaN3). A duplicate of the lowest cell concentration was incubated in the presence of an excess of unlabeled antibody to correct for nonspecific binding. After 6 h of incubation at 37°C, the cells were washed, and activity in the pellet was determined by use of a well-type γ-counter. The inverse of the tumor cell–bound fraction was plotted against the inverse of the cell concentration, and the IRF was calculated from the y-axis intercept. The IRFs (mean ± SD) of the radiolabeled preparations used in the biodistribution and therapy experiments were 89.3% ± 6.5% and 77% ± 6.1%, respectively. Labeled antibody preparations were administered within 2 h after radiolabeling.
Biodistribution After Intraperitoneal or Intravenous Administration
To assess the effects of both the route of administration and the radiolabel on the biodistribution of radiolabeled MN-14, mice were inoculated intraperitoneally with 106 LS174T tumor cells suspended in RPMI 1640 medium (500 μL). Ten days later, mice received 1.22 MBq of 186Re-MN-14 intraperitoneally and 0.481 MBq of 88Y-MN-14 intravenously or vice versa (5 mice per group). Mice were killed by O2:CO2 asphyxiation and dissected at 24, 48, 72, 96, or 192 h after the administration of the radiolabeled antibody preparations (5 mice per group). At dissection, tumors, blood, liver, spleen, kidneys, intestine, lungs, muscle, and the right femur were sampled, blotted dry, and weighed. Activity was measured in a shielded well-type γ-counter (Wizard; Pharmacia-LKB). To correct for physical decay and to calculate the uptake of the radiolabeled antibody in each sample as a fraction of the injected dose, counts in aliquots of the injected doses were determined simultaneously. The results were expressed as the percentage injected dose per gram of tissue (%ID/g). Because it was shown in a previous study that at protein doses exceeding 25 μg, the uptake of radiolabeled antibody MN-14 in tumors tended to be lower (2), the total protein dose of each preparation was adjusted to 10 μg per mouse (total, 20 μg per mouse) by adding unlabeled MN-14 when necessary. The results were compared with the previously reported data on the biodistribution of radioiodinated MN-14 after intravenous or intraperitoneal administration in the same model (2).
Estimation of Radiation Dose Administered to Tumors
The biodistribution data were used to calculate the areas under the curve (AUCs), corrected for physical decay. Subsequently, the data were processed by use of the MIRDOSE3 software program (Oak Ridge Associated Universities) (10) to estimate the radiation dose absorbed by the tumor (tumor absorbed radiation dose) for 131I-MN-14, 186Re-MN-14, 90Y-MN-14, and 177Lu-MN-14 at 50% their maximal tolerated activity doses (MTDs). For this purpose, it was assumed that the biodistributions of both 90Y-MN-14 and 177Lu-MN-14 would have been similar to that of 88Y-MN-14.
Radioimmunotherapy Studies
Ten days after intraperitoneal tumor cell inoculation, groups of 10 mice received intraperitoneal injections of 131I-MN-14 (9.25 MBq per mouse), 186Re-MN-14 (9.25 MBq per mouse), 90Y-MN-14 (3.15 MBq per mouse), 177Lu-MN-14 (8.33 MBq per mouse), and unlabeled MN-14 (control). These doses represented equally toxic activity doses of the respective radionuclides, that is, equal to 50% their respective MTDs. The MTD of each antibody-bound radionuclide after intraperitoneal administration was defined as the activity dose below the lowest dose that resulted in either the death of any animal in groups of 5 animals or a body weight loss of more than 20% and was empirically determined as described previously (11). The MTDs of 131I-MN-14, 186Re-MN-14, 90Y-MN-14, and 177Lu-MN-14 after intraperitoneal administration were 18.5, 18.5, 6.29, and 16.65 MBq, respectively. Preparations were administered in 400 μL of PBS supplemented with 0.5% BSA. The protein dose was adjusted to 20 μg by adding unlabeled MN-14 to a fraction of the primary radioimmunoconjugate preparations when necessary. Because the labeling efficiency was lower than anticipated, the protein dose of the 186Re-MN-14 preparation was 28 μg.
Mice were monitored daily, and body weight and abdominal circumference were measured twice per week as described previously (2). Besides death, a humane endpoint was defined as a decrease in body weight of 20% or more or an increase in the abdominal circumference of 10% or more attributable to intraperitoneal tumor growth, compared with the body weight or abdominal circumference measured on the day of tumor inoculation. When either one of these criteria was met, mice were killed by O2:CO2 asphyxiation and cervical dislocation. All intraperitoneal tumor deposits were meticulously dissected and weighed. The experiment was terminated at 142 d after tumor cell inoculation, when the remaining mice were euthanized and dissected. The abdominal cavity was conscientiously inspected. The liver, spleen, lungs, pancreas, greater omentum, and diaphragm were removed for routine histopathologic hematoxylin–eosin staining and immunohistochemical staining with a rabbit anti–human CEA polyclonal antibody (A0115; Dakocytomation) (12).
Statistical Analysis
Statistical analysis was performed by use of GraphPad InStat 3.00 software (GraphPad Software). Single comparisons were analyzed by use of the 2-tailed, Welch-corrected, unpaired t test or the nonparametric, 2-tailed Mann–Whitney U test. For the biodistribution experiments, uptake in tissues and levels in blood were compared by use of a 1-way ANOVA. Bonferroni correction for multiple testing was applied. For the therapy experiments, survival curves were compared by use of the log–rank test. All tests were 2 sided; the level of statistical significance was set at a P value of <0.05.
RESULTS
Biodistribution of Radioiodinated MN-14
The biodistribution of radioiodinated MN-14 in this model of small peritoneal metastases after intraperitoneal or intravenous administration was described previously (2). In brief, from 24 h on, the levels in blood of intraperitoneally injected 131I-MN-14 and intravenously injected 125I-MN-14 were similar. In the first 24 h after administration, the intraperitoneal route resulted in higher uptake in tumors than the intravenous route. From 48 h after administration on, tumor uptake with the intraperitoneal route was similar to that with the intravenous route (approximately 50 %ID/g). When corrected for the physical decay of 131I, the AUCs for the levels in blood were similar after both routes of administration (0.56 and 0.58 h × MBq/g), whereas the AUC for uptake in tumors after intraperitoneal administration was somewhat higher (2.46 vs. 1.96 h × MBq/g).
Comparison of Biodistributions of Radioiodinated MN-14, 186Re-MN-14, and 88Y-MN-14 After Intraperitoneal Administration and After Intravenous Administration
The mean tumor weight for the mice that received radioiodinated MN-14 was comparable to that for the mice that received 186Re-MN-14 or 88Y-MN-14 (19.5 ± 24.2 and 16.1 ± 16.6 mg, respectively; P = 0.50). The levels in blood of radioiodinated MN-14, 186Re-MN-14, and 88Y-MN-14 after intraperitoneal and intravenous administration are shown in Figure 1. From 24 h after administration on, the levels in blood of all of the radioimmunoconjugates were similar after both routes of administration. The tissue distributions of 186Re-MN-14 and 88Y-MN-14 after both routes of administration are summarized in Tables 2 and 3, respectively. At all time points, the uptake in the liver and spleen of 88Y-MN-14 was higher than that of radioiodinated MN-14 and 186Re-MN-14 after both routes of administration. The uptake in the liver of 88Y-MN-14 remained higher after intravenous administration than after intraperitoneal administration throughout the experiment, whereas the values for uptake in the spleen were similar at all time points. From 48 h after administration on, the uptake of 88Y-MN-14 in bone (represented by the femur) was significantly higher than that of 186Re-MN-14. However, the maximum uptake of 88Y-MN-14 in bone was very low (2.6 ± 0.3 %ID/g at 72 h after intravenous administration). Values for uptake in other normal tissues were similar for all of the radioimmunoconjugates after both routes of administration.
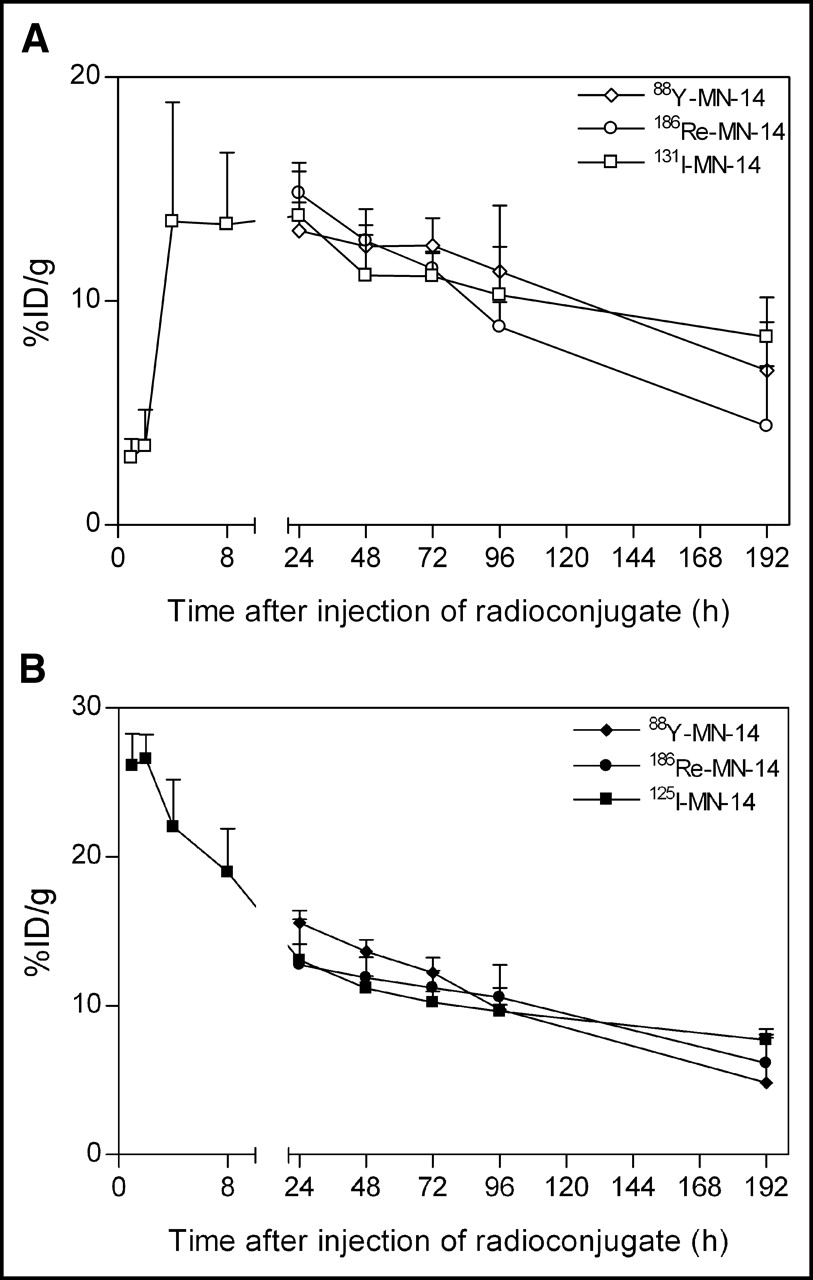
(A) Levels in blood after intraperitoneal administration of 131I-MN-14, 186Re-MN-14, and 88Y-MN-14. Values are given as mean ± SD (5 mice per group). (B) Levels in blood after intravenous administration of 125I-MN-14, 186Re-MN-14, and 88Y-MN-14. Values are given as mean ± SD (5 mice per group).
Tissue Distributions of Intraperitoneally and Intravenously Administered 186Re-MN-14 in Nude Mice Bearing Intraperitoneal LS174T Colon Cancer Xenografts
Tissue Distributions of Intraperitoneally and Intravenously Administered 88Y-MN-14 in Nude Mice Bearing Intraperitoneal LS174T Colon Cancer Xenografts
Figure 2 shows the uptake in tumors of 131I-MN-14, 186Re-MN-14, and 88Y-MN-14 after intraperitoneal and intravenous administration. The uptake in tumors of 88Y-MN-14 was higher than that of 186Re-MN-14 or radioiodinated MN-14 at all time points, except for 24 h after intravenous administration. The maximum values for uptake in tumors after intraperitoneal administration of 131I-MN-14, 186Re-MN-14, and 88Y-MN-14 were 58.5 ± 6.8 %ID/g (24 h after administration), 83.4 ± 18.5 %ID/g (72 h after administration), and 148.1 ± 89.4 %ID/g (192 h after administration), respectively.
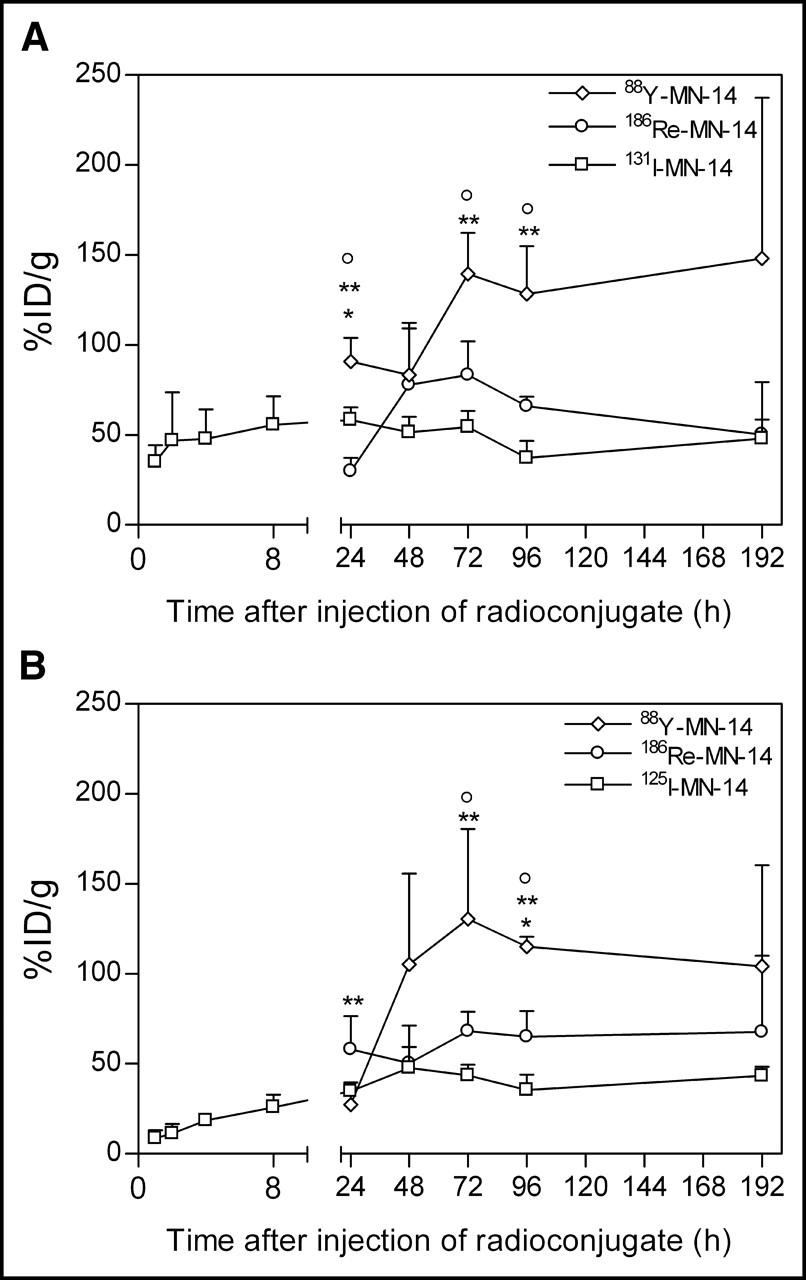
(A) Uptake of 131I-MN-14, 186Re-MN-14, and 88Y-MN-1 in peritoneal LS174T tumor xenografts after intraperitoneal administration. Values are given as mean ± SD (5 mice per group). Double asterisks indicate significant differences between 88Y and 186Re, single asterisks indicate significant differences between 186Re and 131I, and circles indicate significant differences between 88Y and 131I (1-way ANOVA with Bonferroni correction). (B) Uptake of 125I-MN-14, 186Re-MN-14, and 88Y-MN-14 in peritoneal LS174T tumor xenografts after intravenous administration. Values are given as mean ± SD (5 mice per group). Double asterisks indicate significant differences between 88Y and 186Re, single asterisks indicate significant differences between 186Re and 125I, and circles indicate significant differences between 88Y and 125I (1-way ANOVA with Bonferroni correction).
The ratios of the uptake of the radiolabeled mAbs in tumor and the blood levels of the radiolabeled mAbs (tumor-to-blood ratios) after intraperitoneal and intravenous administration are shown in Figure 3. From 24 h after administration on, the tumor-to-blood ratio of radioiodinated MN-14 remained relatively stable (between 4.0 and 6.0), whereas the tumor-to-blood ratio of 186Re-MN-14 steadily increased to 12.0 at 192 h after administration. The tumor-to-blood ratio of 88Y-MN-14 was higher than those of both radioiodinated MN-14 and 186Re-MN-14 at every time point. The maximum tumor-to-blood ratio of 88Y-MN-14 was reached at 192 h after intravenous administration (mean ± SD, 24.7 ± 11.0).
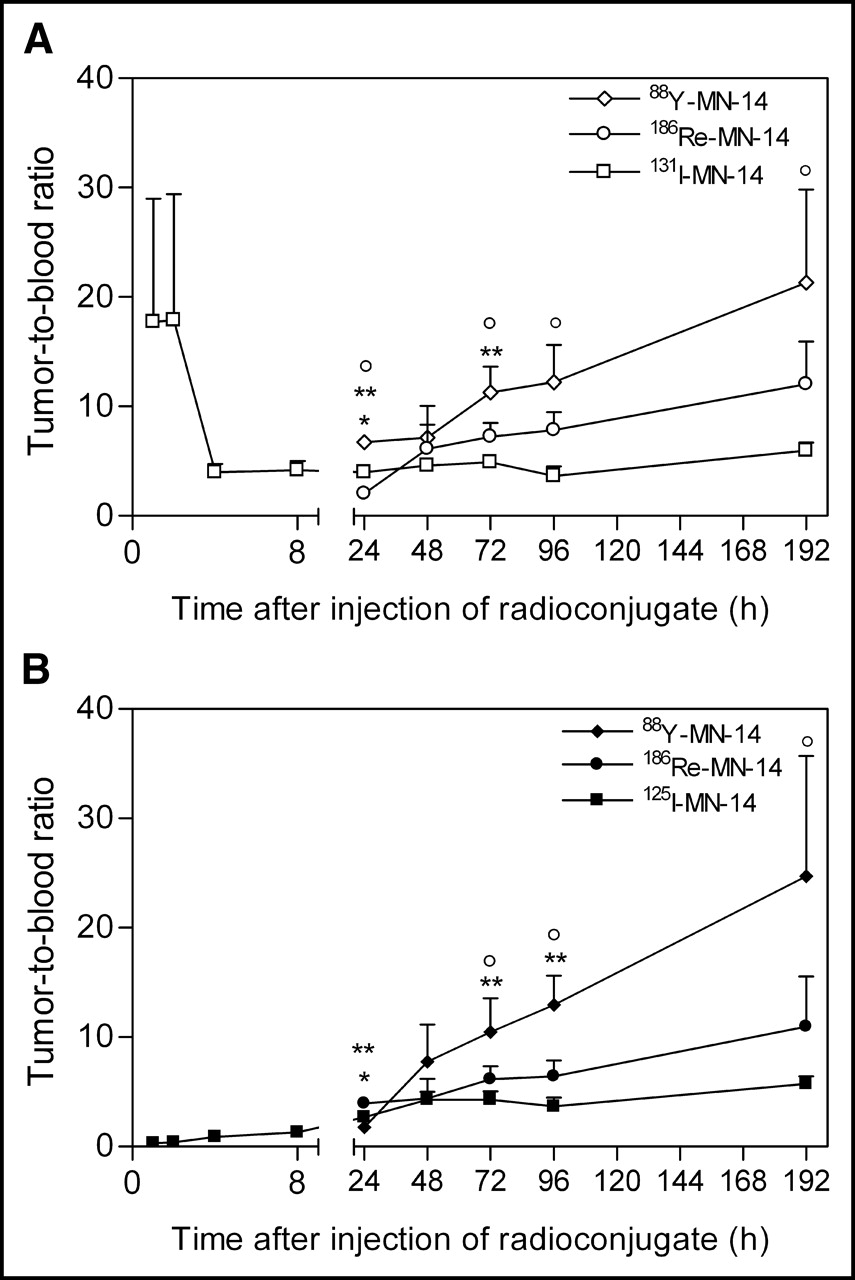
(A) Tumor-to-blood ratios after intraperitoneal administration of 131I-MN-14, 186Re-MN-14, and 88Y-MN-1 in mice bearing peritoneal LS174T tumor xenografts. Values are given as mean ± SD (5 mice per group). Symbols are as described in the legend to Figure 2A. (B) Tumor-to-blood ratios after intravenous administration of 125I-MN-14, 186Re-MN-14, and 88Y-MN-14 in mice bearing peritoneal LS174T tumor xenografts. Values are given as mean ± SD (5 mice per group). Symbols are as described in the legend to Figure 2B.
Tumor Absorbed Radiation Dose
Dosimetric analysis of the biodistribution data (summarized in Figs. 2 and Tables 2 and 3) by use of MIRDOSE3 methodology indicated that intraperitoneal administration of equally toxic activity doses (50% the MTDs) of 131I-MN-14 (9.25 MBq per mouse), 186Re-MN-14 (9.25 MBq per mouse), 90Y-MN-14 (3.15 MBq per mouse), and 177Lu-MN-14 (8.33 MBq per mouse) would result in tumor absorbed radiation doses of 150, 100, 45, and 200 Gy, respectively. For these calculations, it was assumed that the weight of the tumor nodules was 10 mg, corresponding to a diameter of 2.6 mm.
Radioimmunotherapy
Three mice developed subcutaneous tumors at the site of tumor cell inoculation and therefore were excluded from the analysis. Thirty-three mice were killed when their abdominal circumference had increased by 10% because of intraperitoneal tumor growth. The tumor weight (mean ± SD) in these mice was 2.23 ± 1.10 g. Furthermore, 5 mice were killed because of 20% loss of body weight, and 3 additional mice were killed because of poor clinical condition without weight loss reaching 20% or abdominal circumference increase reaching 10%. The tumor weights in these mice were 1.52 ± 1.16 and 1.79 ± 0.41 g, respectively; these values were not statistically significantly different from the tumor loads found in the 33 mice mentioned above (P = 0.35).
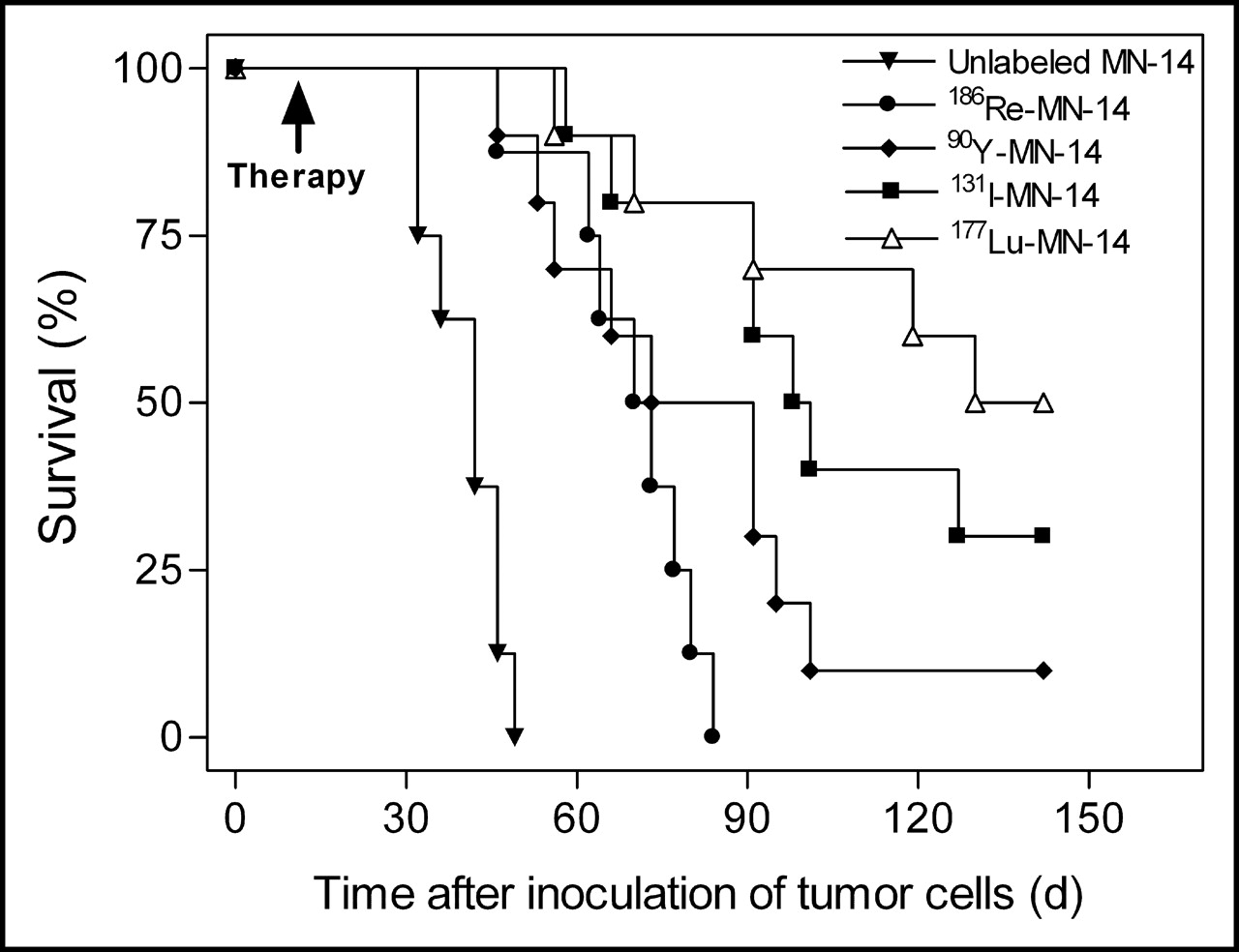
The survival curves for the different treatment groups are shown in Figure 4. The median survival time for the control mice, which received unlabeled MN-14, was 42 d (range, 32–49). The median survival times for the mice treated with equally toxic activity doses of 131I-MN-14 (9.25 MBq), 186Re-MN-14 (9.25 MBq), 90Y-MN-14 (3.15 MBq), and 177Lu-MN-14 (8.33 MBq) were 100 d (range, 58–142; P < 0.0001), 72 d (range, 46–77; P = 0.0002), 82 d (range, 46–142; P = 0.0001), and 136 d (range, 56–142; P < 0.0001), respectively (P values, determined by use of the log-rank test, were for comparisons with mice receiving unlabeled MN-14 [control mice]). The P values for the differences among the survival curves for the various treatment groups are shown in Table 4.

Survival curves for mice bearing peritoneal LS174T tumor xenografts after intraperitoneal administration of 131I-MN-14 (9.25 MBq per mouse), 186Re-MN-14 (9.25 MBq per mouse), 90Y-MN-14 (3.15 MBq per mouse), 177Lu-MN-14 (8.33 MBq per mouse), and unlabeled MN-14 (8–10 mice per group). P values for comparisons of survival curves for various treatment groups are given in Table 4.
P Values for Comparisons of Survival Curves for Mice Treated with Unlabeled MN-14 or MN-14 Labeled with Equally Toxic Activity Doses of 186Re, 131I, 90Y, and 177Lu
At the end of the experiment (142 d after tumor cell inoculation), 9 mice (5 treated with 177Lu-MN-14, 3 treated with 131I-MN-14, and 1 treated with 90Y-MN-14) had no signs of intraperitoneal tumor growth. At dissection, 1 mouse treated with 177Lu-MN-14 had some tumor growth (total intraperitoneal tumor load, 0.65 g), whereas in the remaining 8 mice, there was no evidence of disease. On histopathologic examination of the diaphragm, greater omentum, pancreas, liver, spleen, and lungs, no residual disease was found in any of these mice.
DISCUSSION
The primary aim of the present study was to select the most suitable radionuclide for radioimmunotherapy of small peritoneal metastases of colorectal origin. Radioimmunotherapy with 177Lu-MN-14 resulted in the best median survival time, 136 d; this survival time was significantly better than that seen after treatment with 186Re-MN-14 (72 d) or 90Y-MN-14 (82 d) but did not differ significantly from that seen after treatment with 131I-MN-14 (100 d). No residual tumor was found by histopathologic examination 142 d after tumor cell inoculation in 4 of 10 mice treated with 177Lu-MN-14, 3 of 10 mice treated with 131I-MN-14, and 1 of 10 mice treated with 90Y-MN-14; these mice were considered cured at the end of the study.
In the biodistribution experiments, 88Y-MN-14 resulted in much higher uptake in tumors than did either 125/131I-MN-14 or 186Re-MN-14. The higher uptake of 88Y-MN-14 in the tumor nodules probably reflects the longer tumor residence time of 88Y than of 125/131I or 186Re, which ensues from differences in intratumoral catabolism among the various radiolabels (13). Although anti-CEA mAbs, such as MN-14, that bind to CEA epitopes on the tumor cell surface are internalized only slowly and to a limited extent (14,15), intratumoral catabolism of antibodies has been shown to be significant not only for rapidly internalized antibodies but also for antibodies that bind to the cell surface (16). After internalization by cancer cells, radiolabeled antibodies are enzymatically degraded and metabolized in lysosomes (17,18). After intralysosomal metabolism of mAbs that are radioiodinated by conventional methods, the radioiodinated tyrosine residues are excreted, thereby reducing the residence time of the radioiodine label in tumors (13). After catabolism of mAbs labeled with 88/90Y-DTPA or 177Lu-DTPA, the catabolic products are the radiolabeled chelators bound to amino acids such as lysine (e.g., 88Y-DTPA-lysine) (19,20). Whereas radioiodinated tyrosine is excreted by cells, 88/90Y-DTPA-lysine or 177Lu-DTPA-lysine metabolites are trapped within lysosomes. Furthermore, because antibodies are metabolized by the liver and spleen, intracellular entrapment of the 88Y radiolabel may also explain the higher uptake in these organs of this radiolabel than of 125/131I or 186Re. To date, the fate and processing of 186Re-MAG3-labeled antibodies bound to the surface of tumor cells have not been fully elucidated. Various studies, however, have shown that 186Re is not retained in cells after intracellular catabolism (17,21). The higher uptake of 186Re-MN-14 in tumors and the higher tumor-to-blood ratios of 186Re-MN-14 than of radioiodinated MN-14 in our experiments, however, suggest that the catabolic product of 186Re-MN-14 (presumably 186Re-MAG3-lysine) may be released from cells at a lower rate than radioiodotyrosine.
In the therapy experiments, the administered activity doses of the different radioimmunoconjugates represented 50% the MTDs of the various radionuclides. The therapeutic efficacy of 90Y-MN-14 was much lower than that of 177Lu-MN-14 but did not differ significantly from that of 131I-MN-14 or from that of 186Re-MN-14. Because of a high mean β-emission, 935 keV, and consequently a relatively high tissue penetration depth (maximum, 12 mm), irradiation of small peritoneal metastases of only a few millimeters with 90Y-MN-14 in this model is inefficient, because approximately 70% of the radiation energy is deposited outside the tumor xenografts. Furthermore, because of high-energy β-emission, the MTD of 90Y-labeled IgG is lower than those of antibodies labeled with 131I, 186Re, and 177Lu, which are similar. Indeed, dosimetric analysis of the biodistribution data indicated that the tumor absorbed radiation dose for 90Y-MN-14 was much lower than those for the other radiolabels. Esteban et al. (22,23) studied the effects of 90Y-based radioimmunotherapy with anti-CEA mAb ZCE025 in a similar model of small-volume peritoneal LS174T carcinomatosis. In that study, a clear dose–response effect was observed, although residual viable tumor growth was still found on histologic examination of mice 5 wk after administration of 4.44 MBq. Furthermore, Sharkey et al. (24) showed that in a mouse model of micrometastatic colon carcinoma in the lungs, radioimmunotherapy with 131I was more effective than that with 90Y. Therefore, 90Y seems to be more appropriate in radioimmunotherapeutic applications for larger tumors, a conclusion in keeping with the findings of other investigations (15,25).
Although the dosimetric analysis correctly predicted that 177Lu would be more efficacious than 186Re and 90Y, the apparently higher tumor absorbed radiation dose for 186Re than for 90Y did not result in improved survival. This discrepancy may be explained by several factors. First, the suboptimal protein dose of the 186Re-MN-14 preparation (28 μg) could have had a negative impact on therapeutic efficacy, because it was previously demonstrated that tumor uptake is optimal up to antibody protein doses of 25 μg. Second, this discrepancy could have been attributable to inaccuracies in the dosimetric analysis, because blood, bone marrow, liver, and spleen were not included as source organs in this analysis. It is possible that the relatively high uptake of 90Y-MN-14 in the liver and spleen (approximately 7 %ID/g after intraperitoneal administration) in combination with the high-energy β-emission (maximum tissue penetration depth, 12 mm) contributed to the sterilization of the small peritoneal metastases in the upper abdomen. Another explanation for the observed discrepancy between the survival time and the tumor absorbed radiation dose may be the failure of the animal model to reveal small differences in therapeutic efficacy.
Treatment of mice with 177Lu-MN-14 resulted in the highest median survival time, 136 d; however, this survival time did not differ significantly from that obtained after treatment with 131I-MN-14 (100 d) (P = 0.36). Given the longer intratumoral residence time of 177Lu than of 131I or 186Re, the former radionuclide, with a medium-energy β-emission (maximum tissue penetration depth, 2.5 mm) and a half-life of almost 1 wk, seems to be very well suited for the treatment of microscopic or small-volume disease. From a clinical point of view, the radiophysical characteristics of 177Lu may be more favorable than those of 131I or 90Y. First, because the half-life of 177Lu (6.7 d) is longer than that of 90Y (2.3 d), bone marrow toxicity may be lower because less of the decay occurs in the early time period after administration, when levels in blood are relatively high and uptake in the tumor is still low. Simultaneously, after intratumoral accumulation of the radiolabeled antibody, the tumor is irradiated over a prolonged period of time. Finally, the low-abundance, moderate-energy γ-rays emitted by 177Lu pose fewer radiation safety issues than do those of 131I for the patient’s family and for health care personnel. In fact, promising results were reported by Alvarez et al. (26), who treated 27 patients with chemotherapy-refractory ovarian cancer by using intraperitoneal radioimmunotherapy with 177Lu-labeled IgG antibody CC-49. Antitumor effects were noted even at lower dose levels, whereas patients with microscopic disease showed longer disease-free survival than did historic controls.
CONCLUSION
The uptake of 88Y-MN-14 in small peritoneal LS174T xenografts was higher than that of 186Re-MN-14 or 131I-MN-14. At equally toxic activity doses, the therapeutic efficacy of 177Lu-MN-14 was better than that of 186Re-MN-14 or 90Y-MN-14 but did not differ significantly from that of 131I-MN-14, in keeping with the results of the dosimetric analysis. The results of these studies indicate that 177Lu and 131I are the most suitable radionuclides for the radioimmunotherapy of small peritoneal metastases and may be the best candidates for adjuvant treatment of patients at high risk for the development of intraperitoneal relapse of colorectal cancer.
Acknowledgments
Part of this study was supported by a grant from The Netherlands Organization for Health Research and Development (grant number 920-03-220). We thank Gerry Grutters and Hennie Eikholt (Central Animal Laboratory, University Medical Center Nijmegen) for excellent technical assistance in the animal experiments, Anneke Voss (Department of Pathology, University Medical Center Nijmegen) for help in the histopathologic examinations, and Wil Buijs, PhD (Department of Nuclear Medicine, University Medical Center Nijmegen), for help in the dosimetric analysis.
Footnotes
Received Sep. 8, 2003; revision accepted Jan. 14, 2004.
For correspondence or reprints contact: Manuel J. Koppe, MD, Department of Surgery, University Medical Center Nijmegen, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands.
E-mail: m.koppe{at}chir.umcn.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 64Cu-Intraperitoneal Radioimmunotherapy: A Novel Approach for Adjuvant Treatment in a Clinically Relevant Preclinical Model of Pancreatic Cancer
- SPECT- and Fluorescence Image-Guided Surgery Using a Dual-Labeled Carcinoembryonic Antigen-Targeting Antibody
- Pretargeted 177Lu Radioimmunotherapy of Carcinoembryonic Antigen-Expressing Human Colonic Tumors in Mice
- Therapeutic Potential of 90Y- and 131I-Labeled Anti-CD20 Monoclonal Antibody in Treating Non-Hodgkin's Lymphoma with Pulmonary Involvement: A Monte Carlo-Based Dosimetric Analysis
- Adjuvant and Combined Radioimmunotherapy: Problems and Prospects on the Road to Minerva
- Radioimmunotherapy Is an Effective Adjuvant Treatment After Cytoreductive Surgery of Experimental Colonic Peritoneal Carcinomatosis
- Electron- and Positron-Emitting Radiolanthanides for Therapy: Aspects of Dosimetry and Production
- In vitro and In vivo Targeting Properties of Iodine-123- or Iodine-131-Labeled Monoclonal Antibody 14C5 in a Non-Small Cell Lung Cancer and Colon Carcinoma Model
- Determining Maximal Tolerable Dose of the Monoclonal Antibody BR96 Labeled with 90Y or 177Lu in Rats: Establishment of a Syngeneic Tumor Model to Evaluate Means to Improve Radioimmunotherapy
- In vivo Evaluation of 177Lu- and 67/64Cu-Labeled Recombinant Fragments of Antibody chCE7 for Radioimmunotherapy and PET Imaging of L1-CAM-Positive Tumors