


Abstract
Standard staging of esophageal and gastroesophageal junction (GEJ) tumors substantially lacks accuracy. The aim of this study was to investigate whether the addition of PET with 18F-FDG is a valuable gain in the initial staging. Methods: Between January 1996 and January 2002, 18F-FDG PET was performed in 74 patients. Conventional staging included CT in all patients and well-performed endoscopic ultrasonography (EUS) in 52 patients. They were compared with 18F-FDG PET with pathology and follow-up of suspicious lesions as the gold standard. Results: PET identified 70 primary tumors (sensitivity, 95%). Sensitivity to identify locoregional metastases was highest for EUS (69%) but was not different for CT and PET (44% and 55%, respectively). PET was able to identify distant nodal disease in 71% (17/24 patients) compared with 29% (7/24 patients) after combined CT/EUS alone (P = 0.021). Sensitivity to detect distant nodal and systemic (M1) disease increased with PET (78% vs. 37%; P = 0.012). PET upstaged 15 patients (15/74; 20%) correctly as M1 disease, missed by CT/EUS, and correctly downstaged 4 patients (5%) from M1 to M0 disease. However, false upstaging and downstaging was encountered in 5 (7%) and 3 (4%) patients, respectively. Conclusion: PET improves the currently applied staging of esophageal and GEJ tumors, particularly by ameliorating the detection of M1 disease.
Adequate staging of esophageal cancer including CT and endoscopic ultrasonography (EUS) will avoid useless surgery. However, with standard diagnostic strategy, >30% of the distant metastases are radiographically occult and surgery is still performed in a considerable number of patients with distant metastases (M1) (1,2). Moreover, the overall survival after curative intended resection does not exceed 25%, with an overall median disease-free survival of only 12 mo (3). This can be explained by the presence of micrometastases or undetected metastases at the time of surgery (4). Conventional staging methods consisting of both CT and EUS (CT/EUS) use anatomic alterations to detect local unresectability or metastatic disease. Low accuracy in determining curative intended surgery is caused by low sensitivity and low specificity of these traditional staging methods, indicating the need for a different approach. In contrast to conventional anatomic imaging, PET is based on metabolic alterations in tumor tissues. Nearly all malignant tumors present a high uptake of 18F-FDG as the result of an increased anaerobic glycolysis. In previous studies, 18F-FDG PET was found to be valuable in detecting previously unknown metastases in esophageal cancer (5–10). Routinely performed 18F-FDG PET in the preoperative work-up of these tumors may therefore reduce the number of unnecessary surgical procedures. The objective of this study was to evaluate the performance of 18F-FDG PET in staging esophageal and gastroesophageal junction (GEJ) tumors compared with conventional staging, using histologic examination as the gold standard.
MATERIALS AND METHODS
Patients
Between January 1996 and January 2002, 74 consecutive patients with a resectable carcinoma of the thoracic esophagus and GEJ were entered in a study with 18F-FDG PET staging. Adenocarcinoma occurred in 62 patients and 12 patients had a squamous cell carcinoma. Patient characteristics are presented in Table 1. Approval of our medical ethics committee was obtained and all patients had given written informed consent. All tumors were conventionally staged as resectable with curative intent. Patients with signs of unresectable or incurable disease on CT, EUS, and ultrasound (US) of the neck were not included for PET scanning.
Characteristics of 74 Patients with Carcinomas of Esophagus or GEJ
General Methods
Staging methods were analyzed without knowledge of the results of each staging procedure, including that of PET and pathology. Tumors were classified according to the current International Union Against Cancer TNM staging system (11). Two experienced nuclear medicine physicians without knowledge of the conventional staging results analyzed all PET scans. All PET scans were performed within 2 wk after completion of the conventional staging. In case of disconcordance between the traditional staging methods, the positive results of one procedure overruled the negative results of the other based on standard clinical results.
Conventional Staging
All patients underwent the best-available conventional staging procedure, including ultrasonography of the neck, CT of the thorax and abdomen, and EUS whenever possible. Cervical ultrasonography revealed no abnormality in the 74 included patients. In 32 patients, the CT scans were performed in our institute on fourth-generation units (SR7000 [Philips Medical Systems] or Somatron Plus 4 spiral CT [Siemens Medical Systems]) and in 42 patients, CT scanning occurred in the referring hospital. After approval of good quality, all scans were revised at the time of initial staging and, recently, all available CT scans were revised again and scored by an experienced oncologic radiologist who was unaware of the previous results.
Visible primary tumors on CT were categorized as T+, invisible as T0, and as T4 in case of suspected invasion in juxtaesophageal structures. Depending on the localization of the primary tumor, suspected nodes were classified as locoregional (N1) or distant metastases (M1a or M1b). Technical details of CT scans in this population are described in Table 2.
Tumor and Staging Characteristics of 74 Patients and Influence on Accuracy for Assessment of M1 Disease
Adequate EUS examination was performed in 54 patients (73%). Forty-six patients were examined with a radial scanner (GF-UM20; 7.5–12 MHz, Olympus) and in 8 patients we used a small-caliber EUS probe (MH-908; 7.5 MHz, Olympus). Later in the study, fine-needle aspiration biopsy (FNAB) of suspicious nodes was performed with a 22-gauge, 8-cm needle via a separate linear array echo-endoscope (Benelux, FGUX-36; 5–7.5 MHz, Pentax).
PET Imaging
18F-FDG was produced as described by Hamacher et al. with a radiochemical purity of >98% (12). For data acquisition we used an ECAT 951/31 with 31 planes over 10.9 cm or an ECAT HR+ positron camera (Siemens/CTI) with 63 planes over a 15.8-cm axial field of view. After fasting overnight, 400–580 MBq 18F-FDG were administered intravenously (6 MBq/kg). Data acquisition started 90 min after injection in whole-body mode, for 5 min per bed position. For attenuation correction, transmission images were obtained for 3 min per bed position. Images were reconstructed using iterative techniques and read from computer monitors. Both corrected and uncorrected images were evaluated for tracer uptake by the primary tumor and categorized as T0 or T+. Depending on the location of hot spots and the distance to the primary tumor, nodes were classified as N0, N1, M1a positive, or M1b positive by translation of PET findings to the TNM system.
Surgery
Surgery was denied when presumed distant metastases on 18F-FDG PET were confirmed pathologically or identified by specific radiographic examination, including bone scintigraphy and MRI, depending on the hot spot localization. All resections included dissections of the posterior mediastinal lymph nodes and abdominal nodes along the celiac, left gastric, splenic, and common hepatic arteries, the so-called 2-field lymphadenectomy. Tumors located near or above the level of the carina were always approached by a right thoracotomy, after initial laparotomy. Tumors of the GEJ and distal esophagus were usually resected by a left thoracoabdominal approach. Resection was not performed in tumors fixed to surrounding vital structures or with distant nodal involvement (celiac trunk, paraaortic or retropancreatic) and initially unsuspected organ metastases. As a rule, macroscopically suspected distant nodes (M1a) and organ lesions (M1b) were biopsied during laparotomy.
Gold Standard
Comparison between traditional staging methods and 18F-FDG PET findings was validated by FNAB or pathologic examination of each resection specimen as the gold standard for each TNM category. Surgical findings strongly suggesting tumor fixation to adjacent structures were regarded as the gold standard for T4 stage. The gold standard for nodal metastases was exclusively obtained by pathologic verification of resection specimens after 2-field lymphadenectomy or surgical node biopsies. The gold standard for M1b disease was based on pathology whenever possible or identification by specific radiographic techniques and clinical or radiographic follow-up of suspected PET lesions during 6 mo after initial staging. The gold standard for the T stage and nodal metastases (N stage) could not always be determined when surgery was denied because of pathologically confirmed M1b metastases identified by 18F-FDG PET.
Statistical Analysis
Sensitivity, specificity, and accuracy to identify nodal and organ metastases were determined and compared between conventional staging methods and 18F-FDG PET. Standard definitions were used to calculate these parameters (13). Differences in sensitivity, specificity, and accuracy were analyzed by McNemar testing for paired variables, corrected for continuity. P < 0.05 was considered to be significant
RESULTS
Surgery
Of the 74 patients, resection with curative attempt was performed in 40 patients (54%). Of the 28 patients who underwent an explorative laparotomy, 18 (64%) had M1 disease, 14 (50%) had fixation to vital structures (T4) precluding resection, and 4 patients had a combination of both T4 and M1 disease. Six patients (6/74; 8%) were not enrolled for surgery because of histologically confirmed metastases on 18F-FDG PET (Table 1).
Primary Tumor
The gold standard of the T stage (histologically and surgically) could be assessed in 54 patients (73%). In the other 20 patients, the T stage could not be determined adequately because of M1 disease at the time of initial staging or during surgery. The pathologic tumor stage (pT) could be determined in the 40 patients who underwent an esophageal resection (Table 1). Histologic examination revealed 9 pT1, 3 pT2, 25 pT3, and 3 pT4 tumors. Seventeen tumors, 3 after curative intended resection, were considered as T4.
CT demonstrated the primary tumor in 62 of 74 patients (sensitivity, 84%). The nonvisualized tumors (n = 12) were staged as pT1 (n = 4), pT2 (n = 2), and pT3 (n = 1), and the tumor stage could not be determined on CT in the other 5 patients. EUS was successfully performed by visualizing the primary tumor in all 54 patients (sensitivity, 100%). Accuracy for EUS in determining the T stage could be calculated in 42 patients with the gold standard for the T stage. In the other 12 patients, the gold standard of the T stage could not be determined given an overall accuracy of 67% (28/42). Seven tumors were understaged (17%) and 7 others (17%) were overstaged. The primary tumor was visualized in 70 patients by 18F-FDG PET (sensitivity, 95%). The missed tumors were all classified as pT1 and were <0.5 cm at final pathologic examination.
Regional Lymphatic Metastases
The gold standard for regional nodes (N1) could be assessed in 61 patients. Table 3 gives an overview of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy for the assessment of regional node metastases in the different staging modalities. Forty patients underwent resection with concomitant 2-field lymphadenectomy. The tumor was not resectable in the other patients, but biopsy of suspicious lesions confirmed the presence of nodal metastases. The gold standard of regional nodes could not be assessed in 13 patients. In 6 patients, surgery was denied because of pathologically confirmed M1 disease preoperatively, and 7 patients underwent laparotomy or thoracotomy for locally extended tumors without biopsy of regional nodes.
Sensitivity, Specificity, PPV, NPV, and Accuracy in Different Staging Modalities Assessing Nodal (N) Metastases
CT was able to predict N1 metastases in 17 of 39 evaluated patients (sensitivity, 44%). Due to reconstruction artifacts, assessment by CT was not possible in 1 patient with pN1. EUS was performed in 43 of the 61 patients with adefined gold standard. Regional nodes were positive in 26 tumors and EUS was able to predict nodal disease in 18 of these N1 tumors (sensitivity, 69%). However, with identification of 4 false-positive lesions, specificity of EUS was lower than that of CT (76% vs. 90%, respectively). 18F-FDG PET could predict nodal metastases in 22 of 40 N1-positive tumors (sensitivity, 55%). In 6 of the 21 node-negative tumors, 18F-FDG PET falsely indicated N1 disease (specificity, 71%). Of the 6 false-positive PET scans, one had a multifocal tumor representing different hot spots in the esophageal region, and pathologic examination in 2 other patients revealed anthracosilicosis, probably responsible for the peritumoral hot spot. Sensitivity and specificity of 18F-FDG PET for assessing N1 disease were comparable with the performance of CT. Although EUS had the highest sensitivity to predict regional node metastases, this difference was not significant (EUS = 69% sensitivity vs. PET = 55% and CT = 44% sensitivity; Table 3).
Distant Nodal Disease
The gold standard of distant nodal disease defined as M1a by the TNM staging system could be assessed in 72 patients (Table 4). Two other patients had confirmed M1b disease precluding surgical exploration and, therefore, the gold standard was not accessible in these patients. M1a was present in 24 patients (33%). The involved distant nodes were located around the celiac trunk or paraaortic in 21 patients. One patient also had mediastinal paraaortic involvement, and supraclavicular node metastases were confirmed in 3 patients. Conventional staging methods (CT/EUS) correctly identified M1a disease in 7 patients (sensitivity, 29%; 7/24). The false-negative distant nodes in the remaining 17 patients were located along the abdominal aorta (n = 13), supraclavicular (n = 3), and mediastinal (n = 1). Two patients with suspected regional nodes along the left gastric artery were falsely staged as M1a, precluding resectability by conventional methods. In 1 patient it was based on CT alone and in the other patient EUS was false-positive.
Sensitivity, Specificity, PPV, NPV, and Accuracy in Different Staging Modalities Assessing Distant Node (M1a) Metastases: Gold Standard Assessable in 72 Patients
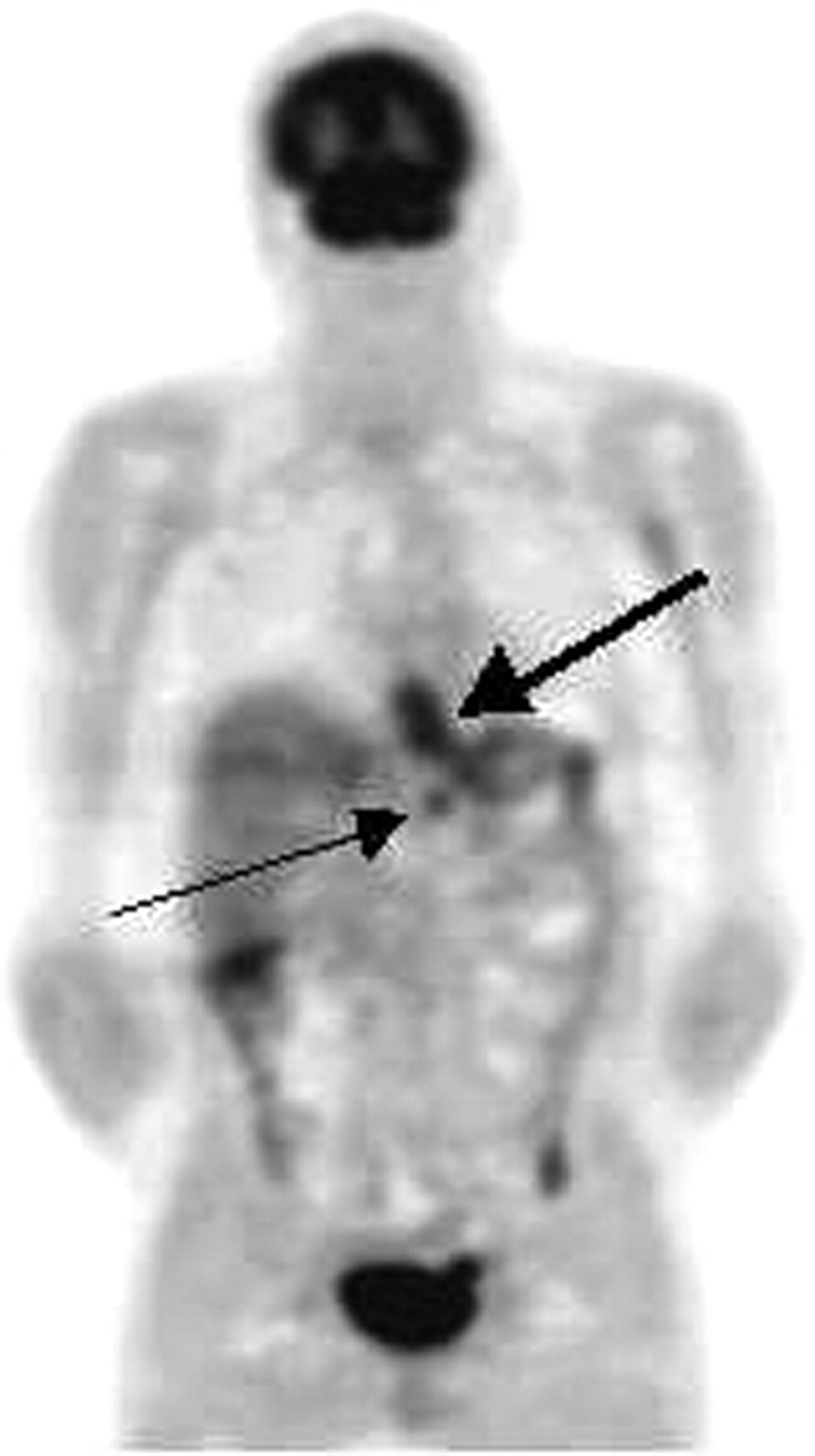
PET correctly revealed distant nodal involvement in 17 of the 24 patients with M1a disease (sensitivity, 71%). The difference in sensitivity between 18F-FDG PET and conventional staging appeared to be significant (71% vs. 29%; P = 0.021), with a correct upstaging as M1a in 12 patients (16%; 12/74). Correct upstaging with PET identifying distant lymph node metastases is illustrated in Figures 1 and 2. 18F-FDG PET missed distant M1a metastases in 7 patients and the location of all was paraaortic in GEJ tumors. Both PET and CT/EUS was false-negative in 3 of these 7 patients by missing these abdominal node metastases, resulting in false downstaging in 4 patients when using PET alone. PET revealed only one false-positive lesion in the assessment of distant nodal involvement. The location of this hot spot was supraclavicular, probably caused by asymmetric muscular activity. Echographically guided biopsies and long-lasting follow-up did not yield metastatic disease. Table 4 gives an overview of the assessment in different staging modalities.
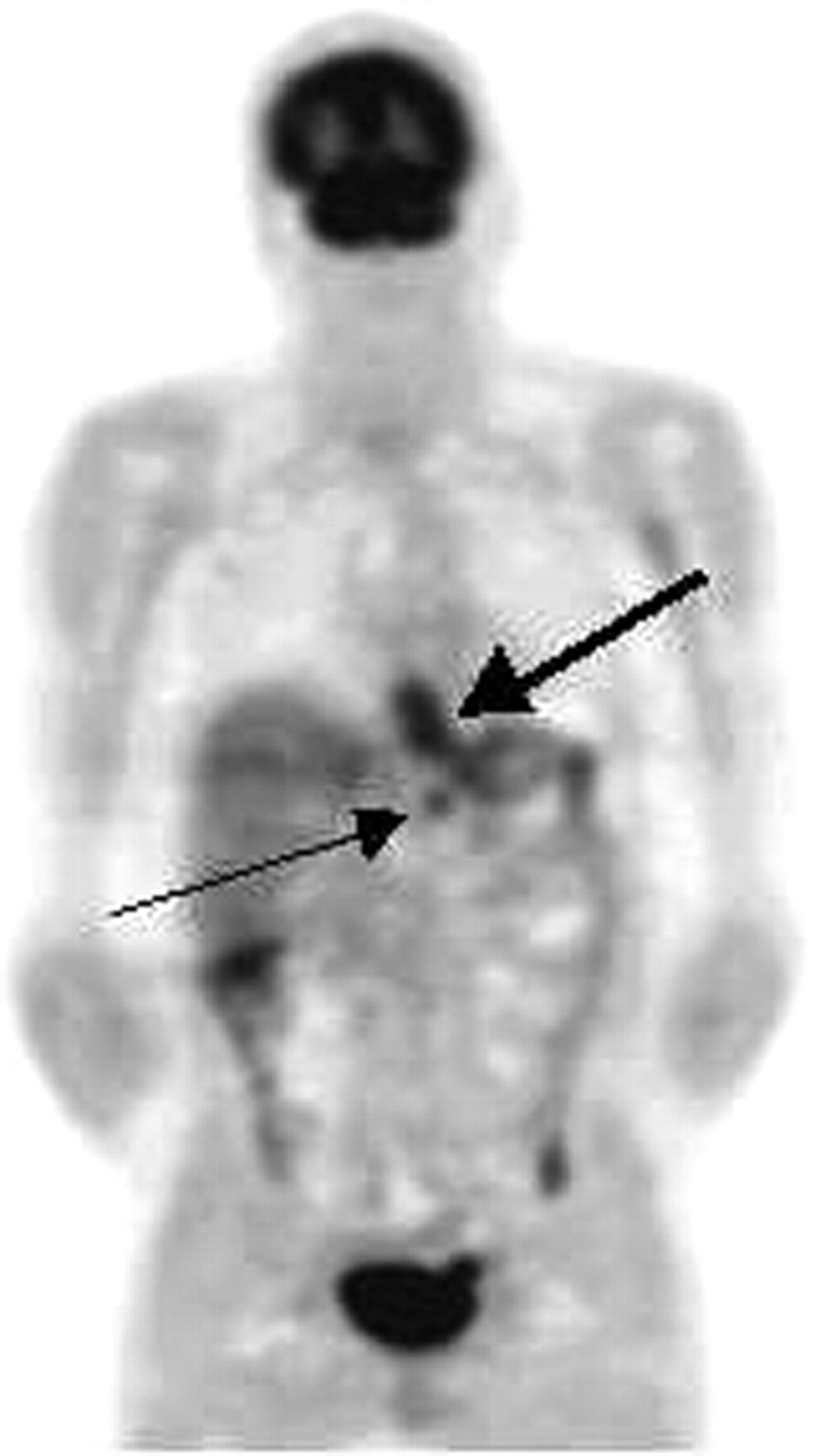
Upstaging with 18F-FDG PET of histologically proven distant lymph node metastasis at celiac region in patient with GEJ tumor. Conventional staging was negative for distant nodal metastases. Thick arrow indicates primary tumor; thin arrow indicates lesion at celiac trunk region.
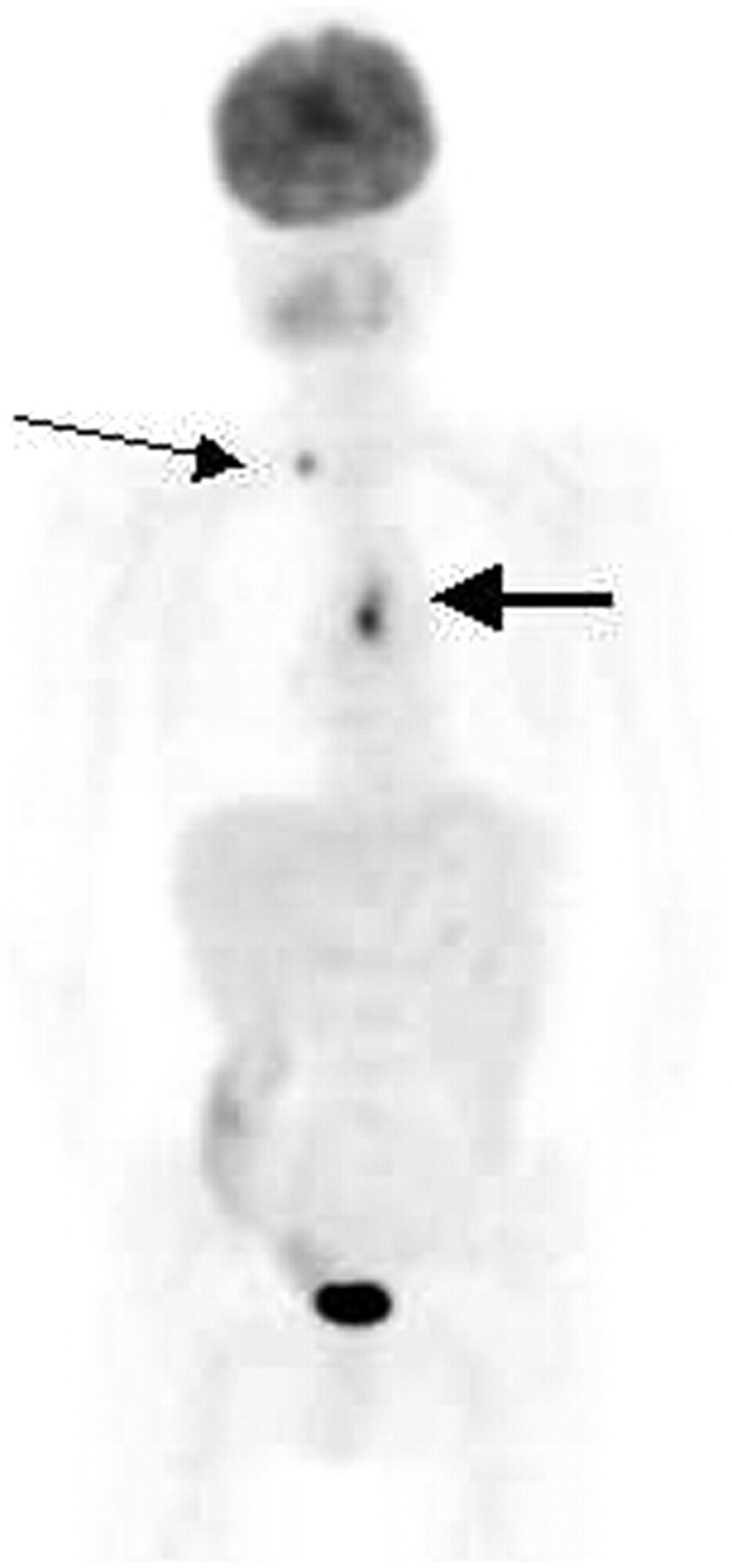
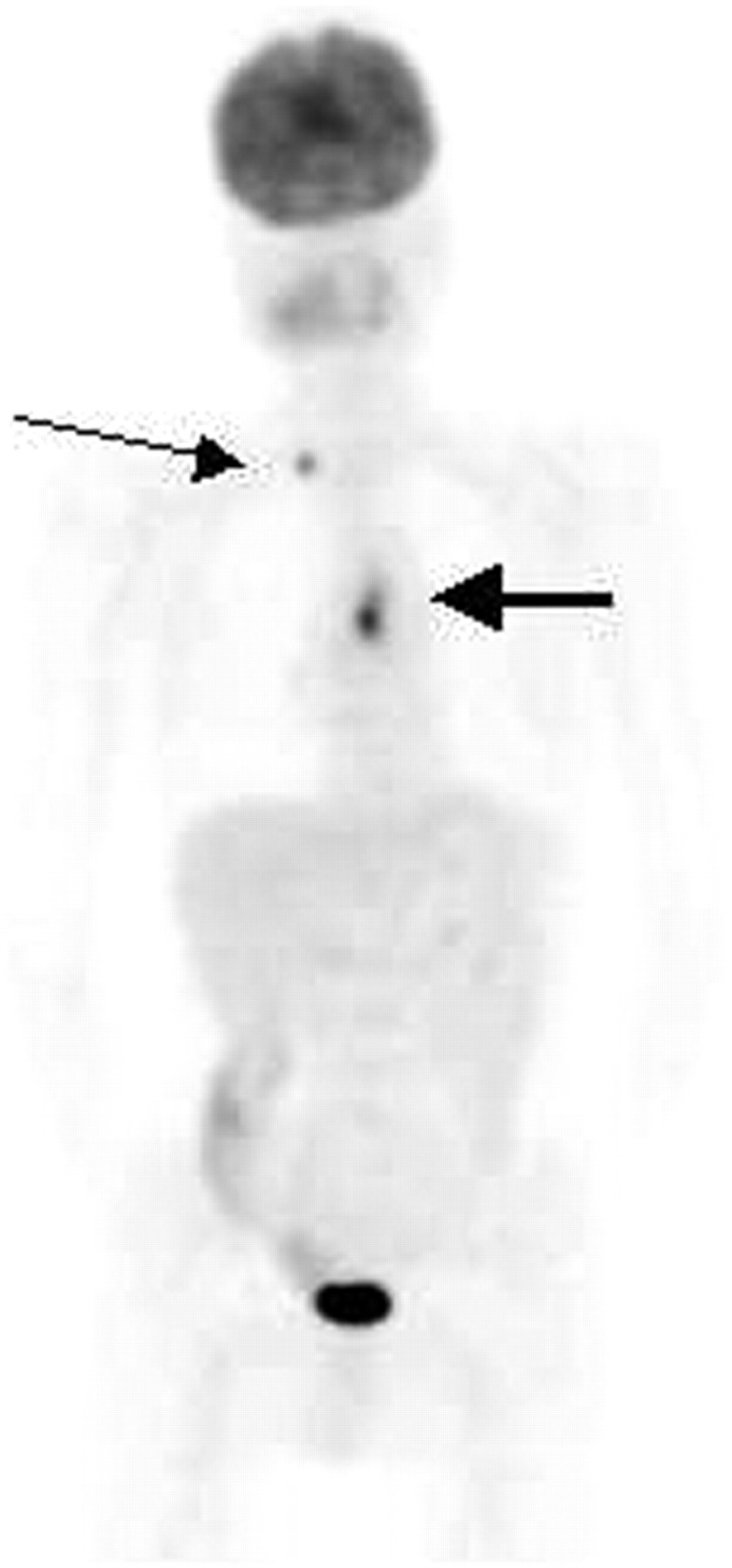
Detection of supraclavicular lymph node metastases with 18F-FDG PET leading to correct upstaging. Thick arrow indicates primary tumor; thin arrow indicates cervical node metastasis.
Distant Organ Metastasis
The gold standard for the presence of M1b disease was assessed in all 74 patients. In 10 patients (12%), pathologic biopsies, radiographic techniques, or clinical follow-up demonstrated the presence of organ metastases. CT identified M1b disease in 3 of the 10 patients with confirmed lesions, whereas PET correctly identified 7 M1b lesions (sensitivity, 30% vs. 70%). Peritoneal metastases were present in 5 patients, liver metastases in 5 patients, lung metastases in 3 patients, and a combination of different organ involvement in 3 patients. In 4 of the 5 patients with hepatic metastases, conventional staging methods missed these lesions, but 18F-FDG PET correctly upstaged the disease in 3 of these 4 patients. In 1 patient, neither PET nor CT/EUS was able to detect a solitary liver metastasis of 0.8 mm in size, which was detected during laparotomy. Both CT and PET correctly identified lung metastases (n = 3) but could not identify peritoneal carcinomatosis (n = 5) seen during laparotomy. However, 4 of these patients already had been upstaged correctly by PET, identifying distant nodal (celiac trunk or paraaortic) disease. On a lesion basis, conventional staging identified 4 (sensitivity, 33%) and PET identified 7 of the 12 lesions (sensitivity, 58%). CT demonstrated 12 false-positive lesions in 6 patients (8 hepatic lesions in 4 patients and 4 lung lesions in 2 patients). Echographically guided biopsy was performed unsuccessfully in 1 patient and all 4 lung lesions were negative during follow-up. With PET, a total of 20 hot spots in 7 patients were identified, warranting further diagnostic procedures or follow-up. Seven hot spots were confirmed to be malignant, (PPV, 35%; 7/20). Six other spots were negative, including 4 costal lesions in a patient with rheumatoid arthritis, one suspicious rectal hot spot caused by proctocolitis, and one liver lesion not seen during laparotomy or detected during follow-up. The character of 7 intrapulmonary hot spots in 3 patients could not be assessed because the patients died within the acquired follow-up period. In 2 patients, the cause of death was peritoneal disseminated disease. A second primary tumor was detected with 18F-FDG PET in 2 patients (3%). CT missed a non–small cell lung carcinoma with a distinct hot spot in the right upper pulmonary lobe on PET. The other was a carcinoma in the hepatic flexure confirmed by colonoscopy.
Relation of PET to Tumor and Patient Characteristics on Conventional Staging
We examined whether certain tumor or patient-related characteristics influenced the value of PET in determining the presence of distant metastases. The influence of histologic type (adenocarcinoma vs. squamous cell carcinoma), tumor localization (tubular esophagus vs. GEJ), tumor stages as identified by EUS and quality of CT, and referral from other (nontertiary) hospitals on the outcome of PET were studied. To determine the effect of CT imaging quality, the study group was divided into patients investigated by CT with a resolution of ≤5 mm and those staged with a resolution of >5 mm. Moreover, the effect of the acquisition type (multidetector vs. spiral CT) was noted. Finally, the group of patients with adequate EUS was compared with patients in whom EUS results were not available. The main endpoint was the number of patients in each group in which PET provided correct upstaging from M0 to M1 disease. None of the characteristics mentioned earlier had a significant influence, as shown in Table 2.
The results of PET were not related to the histologic type, although a fair comparison was difficult due to a relatively low number of squamous cell carcinomas. Tumor localization, acquisition and type of CT used, and referral of patients from other hospitals had no significant effect on the correct upstaging by PET. In addition, upstaging of PET occurred in the same frequency in the group in which EUS was part of conventional staging compared with the group in which no EUS was performed. However, when patients were divided according to tumor stage as identified by EUS, an interesting phenomenon was seen. All patients, correctly upstaged by PET from M0 to M1 disease, at least had an EUS-confirmed T3 tumor. None of the 11 EUS-staged T1 or T2 N0 tumors turned out to have M1 disease. In this subgroup of patients, PET was false-positive for N1 disease in 6 patients (55%) and false-positive for M1 disease in 1 patient, limiting the additional value of PET in these patients. In contrast, 8 of 41 patients (20%) with T3 or T4 tumors, as determined by EUS, were correctly upstaged as M1 disease with PET.
Overall Prognostic Value
Sensitivity to detect M1 disease defined by distant node or organ metastases was increased with PET (78% [21/27] vs. 37% [10/27], P = 0.012; Table 5). As a whole, 15 of the 74 patients (20%) were correctly upstaged with PET by identification of M1a metastases (n = 10), lymphatic M1b metastases (n = 2), hematogenic (liver) M1b metastasis (n = 1), and a combination of M1a/M1b disease (n = 2). However, with PET, surgery would have been avoided in only 2 of these patients by detecting supraclavicular node metastases. In 4 patients (5%), PET correctly performed downstaging from M1 to M0 disease. False upstaging and downstaging were obtained in 5 patients (7%) and 3 patients (4%), respectively.
Sensitivity, Specificity, PPV, NPV, and Accuracy in Different Staging Modalities for Overall Assessment of M1 Disease (Combination of Distant Node and Organ Metastases)
DISCUSSION
This study clearly shows the additional value of 18F-FDG PET in staging carcinoma of the esophagus and GEJ. Though performance of PET in assessing N1 disease is not better than that of current staging methods, there is a significant advantage in detection of M1 disease, avoiding unnecessary surgery. 18F-FDG PET detected 95% (70/74) of the primary esophageal tumors, which is comparable with percentages in previously reported studies (5–10). PET missed 5% of the primary tumors, but all missed lesions were pT1 adenocarcinomas of the GEJ that were <0.5 cm. False negativity in these small tumors is usually caused by limitations in the spatial resolution of PET (14).
18F-FDG PET does not add much in the detection of regional nodes. Currently available staging methods are of limited value to assess regional node involvement, with the highest reported sensitivity for EUS (70%–90%) (2). The direct vicinity of the primary tumor, obscuring 18F-FDG uptake, probably causes false-negative results in peritumoral N1 nodes. Moreover, small metastatic nodes could cause false negativity by limitations in the spatial resolution. Specificity of 71% (15/21) with PET in assessing regional metastases is comparable with that of other series. Anthracosilicosis in mediastinal nodes, multifocality of the primary tumor, and inhomogeneous uptake of the tracer may cause different hot spots, leading to false-positive results, as shown in 3 of 6 patients in this study. Combining CT, EUS, and PET leads to an increased sensitivity but the number of false-positive N1 nodes also increases, lowering the specificity as found in the literature (14–17).
To identify unsuspected M1 disease, 18F-FDG PET performed better than the combination of CT/EUS. The rate of M1 metastases only detected by 18F-FDG PET in conventionally staged tumors is 10%–20% (5–10,15–18). 18F-FDG PET upstaged the disease in about 20% (15/74) as M1 disease. The accuracy of 69% (51/74) for detecting M1 disease with CT/EUS increased to 86% (64/74) with 18F-FDG PET (Table 5). A combination of all 3 modalities increased the accuracy for detecting M1 disease up to 92% (68/74) as was the result of a more sensitive detection of both distant node and organ metastases. Some considerations must be mentioned about the upstaging role of 18F-FDG PET. First, the difference in detecting M1 disease between conventional staging and 18F-FDG PET is probably high due to a substantial percentage of patients referred to our hospital—a tertiary referral center—after CT was already performed. If CT in the referring center had indicated M1 disease, this patient would not have been referred to our hospital for surgical resection. On the other hand, this phenomenon—the central finding of correct upstaging M1 disease by 18F-FDG PET in a substantial percentage of patients compared with conventional staging—does not explain low sensitivity for detection of distant abdominal nodes (24%).
Second, in 13% of the patients (2/15) who were correctly upstaged by 18F-FDG PET, surgery could be avoided. Both patients had cytologically confirmed cervical node metastases. The other 13 patients needed a laparotomy to confirm distant nodal or liver metastases. This is related to the premise that suspicious hot spots in our study design must be confirmed by cytopathologic examination, avoiding the possibility of denying a curative resection or the risk of tumor progression during possible unnecessary induction treatment. Otherwise, all intraabdominally located M1a lesions demonstrated on PET in our series were confirmed during laparotomy (PPV, 100%). Performing surgery in this group would possibly postpone induction chemotherapy. Furthermore, EUS-guided cytologic biopsies of suspected celiac nodes are a promising technique currently used in this respect (19). A proportion of CT scans was not performed in our institute, limiting standardization of this procedure. The influence on the quality of the conventional staging in this study seems to be small because all CT scans were revised at the time of initial staging and would have been repeated if they were of unacceptable quality. Furthermore, all available CT scans were rescored without knowledge of the results of 18F-FDG PET or the gold standard without increasing sensitivity and accuracy in the assessment of N1 or M1 disease. Although EUS was not acquired in a proportion of patients, increasing the number of EUSs performed in our study would probably not have led to a higher detection of M1 disease because none of the M1a or M1b lesions identified by conventional staging had negative CT scans. Moreover, comparison of the accuracy for the assessment of M1 disease did not differ significantly between referred and nonreferred patients or between patients for whom EUS results were not available (Table 2). Therefore, the central finding of this study—namely, a correct upstaging by 18F-FDG PET in 20% of the patients (15/74)—merely depends on the metabolic reflection of the tumor rather than on the limitations of anatomic staging results of the conventional methods.
The incremental value of 18F-FDG PET will be higher in tumors with a high probability of distant metastatic disease. Eleven of 54 patients, in whom EUS was performed, were staged as T1/T2 N0 M0. In 5 of these 11 patients, PET displayed locoregional hot spots, but none of them was found in resection specimens, representing false upstaging of N1 disease by 18F-FDG PET. Therefore, the additional value of performing PET scans in these low-staged tumors may be questionable. Otherwise, all patients who were correctly upstaged to have M1 disease had T3 N0–N1 tumors, as identified by EUS. Therefore, these results support the arguments for a selective demand of 18F-FDG PET in high-staged esophageal tumors. This option becomes even more attractive at the background of the limited availability of PET scanners. A proposal for such a selective demand of PET based on the staging of these tumors with EUS is given in Figure 3. A well-designed cost-effectiveness study eventually should definitively answer this important question.

Diagnostic tree proposal for staging of patients with cancer of esophagus or GEJ.
Based on the results of this study, comparing the results of conventional staging methods (CT/EUS) with 18F-FDG PET, we recommend the routine addition of 18F-FDG PET in the preoperative staging of potentially resectable esophageal tumors. This approach may lead to a remarkable increase in the detection of distant node and organ metastases. This benefit seems to be even greater for locally advanced tumors, as being more often affected by M1 disease.
CONCLUSION
This study showed that 18F-FDG PET is sensitive and accurate in the preoperative staging of distant metastases in patients with cancer of the esophagus and GEJ and leads to upstaging, particularly in T3 and N1 tumors.
Footnotes
Received Oct. 16, 2003; revision accepted Jan. 13, 2004.
For correspondence or reprints contact: John Th.M. Plukker, MD, PhD, Department of Surgical Oncology, University Hospital of Groningen, 9700 RB Groningen, The Netherlands.
E-mail: j.th.plukker{at}chir.azg.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Performance of 18F-FDG PET and PET/CT for the Detection of Recurrent Esophageal Cancer After Treatment with Curative Intent: A Systematic Review and Meta-Analysis
- An update on the staging of oesophageal and gastric cancers
- 18F-FDG PET/CT Has a High Impact on Patient Management and Provides Powerful Prognostic Stratification in the Primary Staging of Esophageal Cancer: A Prospective Study with Mature Survival Data
- Diagnostic and Prognostic Value of 18F-FDG PET/CT for Patients with Suspected Recurrence from Squamous Cell Carcinoma of the Esophagus
- Comparison of 18F-FLT PET and 18F-FDG PET in Esophageal Cancer