


Abstract
The functional role of various angiographic grades for coronary collaterals remains controversial. The aim of this study was to assess the influence of the Rentrop angiographic grading of coronary collaterals on myocardial perfusion in patients with single-vessel chronic total occlusion (CTO) and no prior myocardial infarction (MI). Methods: The study included 56 patients with single-vessel CTO and no prior MI who underwent rest–stress myocardial perfusion SPECT and coronary angiography within 6 mo. All patients had angiographic evidence of coronary collaterals. Patients were divided according to the Rentrop classification: Group I had grade 1 or 2 (n = 25) and group II had grade 3 collaterals (n = 31). Results: Group I had a higher frequency of resting regional wall motion abnormalities on left ventriculography (52.6% vs. 19.2% [P = 0.019]). The mean perfusion scores of the overall population showed severe and extensive stress perfusion defects (summed stress score of 14.1 ± 7.1 and summed difference score of 12.9 ± 6.9) but minimal resting perfusion defects (summed rest score of 1.0 ± 2.7). No perfusion scores differed between the 2 groups. The perfusion findings suggested that chronic stunning rather than hibernation is the principal cause of regional wall motion abnormalities in these patients. Conclusion: In the setting of single-vessel CTO and no prior MI, coronary collaterals appear to protect against resting perfusion defects. Excellent angiographic collaterals may prevent resting regional wall motion abnormalities but do not appear to protect against stress-induced perfusion defects.
Despite decades of study, the functional role of the coronary collateral circulation remains controversial (1–3). Although myocardium supplied by well-developed collaterals may maintain normal resting perfusion, patients may still have myocardial ischemia, as manifested by anginal symptoms, ischemic electrocardiographic (ECG) changes, or abnormal myocardial perfusion studies (1,2). Discordance in the results of prior studies is due, in part, to inclusion of a nonuniform patient population, often with multivessel coronary artery disease, prior myocardial infarction (MI), various degrees of incomplete coronary occlusion, or a combination of these factors.
Because blood flow distal to a chronic total occlusion (CTO) would be entirely collateral dependent, Gregg and Patterson suggested that patients with single-vessel CTO in the absence of MI would be the optimal subset in which to study human coronary collaterals during stress (4). The aim of this study was to determine whether the grade of coronary collaterals relates to myocardial perfusion SPECT (MPS) and regional wall motion findings at rest or stress in patients with a single-vessel CTO and no prior MI.
MATERIALS AND METHODS
Study Population
Using the Cedars-Sinai database for 1991–2000, we identified 56 patients who underwent rest 201Tl–stress 99mTc-sestamibi dual-isotope MPS and within 6 mo of MPS had coronary angiography findings of single-vessel CTO with no coronary revascularization or MI between the studies. Additional exclusion criteria included a prior MI by history or ECG, previous bypass surgery, or angioplasty less than 1 y before either study. The mean difference between MPS and coronary angiography was 10.8 ± 33.1 d, with the time of angiography ranging from 165 d before the time of MPS to 144 d after. In 52 patients (92.9%), MPS preceded coronary angiography.
Coronary Angiography and Left Ventriculography
Coronary angiography was performed using the standard Judkins approach, and 2 observers who were unaware of the clinical and scintigraphic data analyzed the angiograms specifically for this study. Single-vessel CTO was defined as an estimated luminal narrowing of ≥99% in 1 of the 3 main coronary arteries or a major branch. Collaterals were graded by the degree of filling of the involved vessel beyond the CTO according to the Rentrop classification (5): grade 0 = no visible filling, grade 1 = side branch filling but without any dye reaching the epicardial segment, grade 2 = partial epicardial filling, and grade 3 = complete filling of the epicardial segment. In patients who underwent contrast ventriculography (n = 45), regional wall motion was visually analyzed (6). The left ventricular wall was divided into 9 segments: anterobasal, anterolateral, apical, diaphragmatic, posterobasal, basal septal, apical septal, posterolateral, and lateral. Segments in the territory of the occluded vessel showing hypokinesis, akinesis, or dyskinesis were considered to have regional wall motion abnormality. Patients were divided into 2 groups according to the presence of Rentrop grade 3 coronary collateral vessels. Group I consisted of 25 (44.6%) patients with Rentrop grades 1 or 2 and group II consisted of 31 (55.4%) patients with Rentrop grade 3 (excellent) collaterals. No patients had Rentrop grade 0 collaterals.
Rest–Stress MPS Protocol
All patients underwent rest 201Tl–stress 99mTc-sestamibi MPS, as previously described by our group (7). Initially, 201Tl (92.5–148.0 MBq) was injected intravenously at rest, with the dose varying by weight. Rest 201Tl SPECT was performed 10 min after tracer injection. Patients with resting perfusion defects (n = 5) underwent late redistribution 201Tl imaging 24 h after the stress study. Patients were instructed to discontinue taking β-blockers and calcium channel antagonists 48 h before, nitrates 6 h before, and caffeine-containing products 24 h before the MPS. Patients underwent either symptom-limited treadmill exercise using the Bruce protocol (n = 38, or 68%) or adenosine stress (n = 18, or 32%). For exercise stress, patients received an injection of 99mTc-sestamibi (740–1,295 MBq) at peak stress. Maximal exercise was continued for 1 min after injection, and exercise at a lower speed and grade was then continued for an additional 2 min. For adenosine stress, adenosine was infused intravenously at a dose of 140 μg/kg/min for 5 or 6 min. 99mTc-Sestamibi was injected at the end of the second or third minute of infusion, and SPECT was performed approximately 1 h later (8). With respect to ECG changes during both exercise and pharmacologic stress, horizontal or downsloping ST-segment depression of 1 mm or greater or upsloping of 1.5 mm or greater at 80 ms after the J point was considered an ischemic ECG response.
SPECT Acquisition Protocol
SPECT images were acquired and processed as previously described (7), with a circular or elliptic 180° acquisition for 64 projections at 25 s/projection for 99mTc or 35 s/projection for 201Tl using a multidetector γ-camera. During imaging, 2 energy windows were used for 201Tl, a 30% window centered on the 70-keV peak and a 20% window centered on the 167-keV peak. For 99mTc-sestamibi SPECT, a 15% window centered on the 140-keV peak was used. No attenuation correction or scatter correction was used. All images were subject to quality control measures, as previously described (7).
Image Analysis
Two observers unaware of the angiographic results assessed the MPS images. Semiquantitative visual scoring of the perfusion images was performed using a 20-segment model as previously described (7). Two experienced observers scored each segment by consensus, using a 5-point scoring system (0 = normal, 1 = equivocal, 2 = moderate, and 3 = severe reduction of radioisotope uptake; 4 = absence of detectable tracer uptake in a segment) (7). Summed stress score (SSS) and summed rest score (SRS) were calculated by adding the 20 segment scores of the stress and rest images, respectively. When patients underwent 201Tl late redistribution studies, the late redistribution score was substituted for the rest score. Summed difference score (SDS), a measure of stress-induced perfusion defect, was derived as the difference between stress and rest scores (9). As previously described, SSS < 4 was considered normal; SSS of 4–8, mildly abnormal; SSS of 9–13, moderately abnormal; and SSS > 13, severely abnormal (10,11). The number of nonreversible segments was defined from segments with stress–rest score combinations of 4–4, 4–3, 3–3, 3–2, or 2–2 (12). The number of reversible segments was defined from all other segments with a stress score ≥ 2 or with scores of 4–2 or 1–0.
Prescan Likelihood of Coronary Artery Disease
The prescan likelihood of coronary artery disease was calculated by Bayesian analysis of prescan patient data (13). For patients who underwent pharmacologic stress testing, history and resting ECG alone were considered, whereas for those who underwent exercise stress testing, the prescan likelihood of coronary artery disease included history and exercise test information.
Statistical Analysis
All continuous variables are expressed as mean ± SD. The mean differences between 2 groups for continuous variables were compared by the Student t test (2-tailed). One-way ANOVA was used to compare the means of continuous variables among the 3 coronary arteries. Categoric variables were compared by the χ2 statistic. A P value < 0.05 was considered significant.
RESULTS
Patient Characteristics
The mean age of the study population was 66.9 ± 10.5 y; 38 (67.9%) were male and 18 (32.1%) were female. Clinical characteristics of the 2 groups according to the presence or absence of grade 3 collaterals are shown in Table 1. There were no significant differences in any of the descriptors assessed except for hypertension, which was more prevalent in patients with grade 3 collaterals (group II) (P = 0.02).
Patient Demographics According to Collateral Group
Angiographic and Ventriculographic Results
Forty-eight patients (85.7%) had occlusion of 1 of the 3 main coronary arteries, and 8 patients (14.3%) had occlusion of a major branch (diagonal, obtuse marginal, or posterior descending artery). Coronary angiographic and ventriculographic results according to collateral group are shown in Table 2. The 2 groups did not differ in the proportion of patients having CTO of each major coronary artery. Regarding ventriculographic findings, among the 45 (80.4%) patients with left ventricular angiograms, normal regional wall motion was common (30/45, or 67%) and patients of group I had a higher frequency of resting regional wall motion abnormality (52.6% vs. 19.2%, P = 0.02).
Angiographic and Ventriculographic Results According to Collateral Group
MPS Results
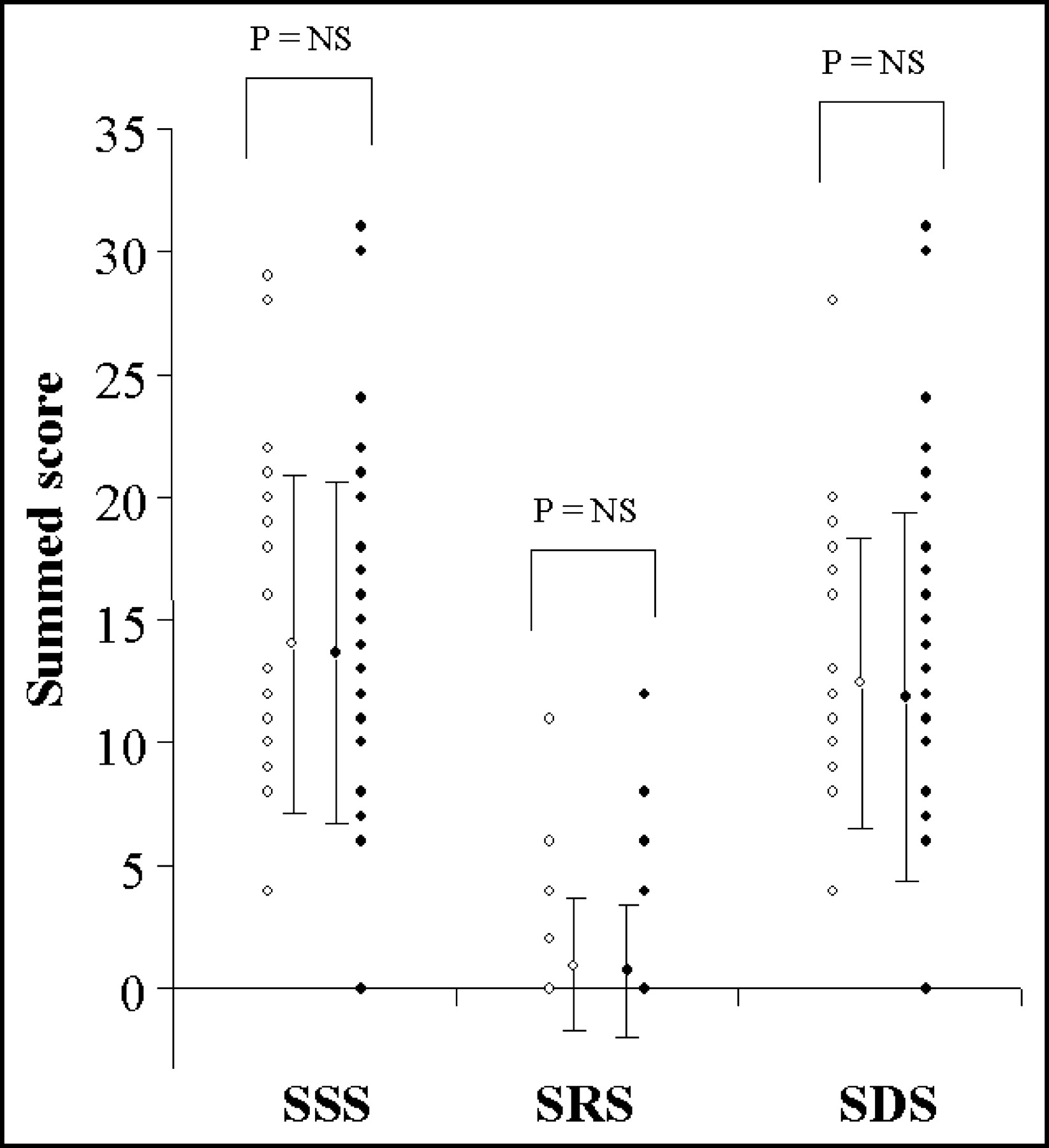
The mean overall stress perfusion scores for the population were very abnormal, with an SSS of 14.1 ± 7.1 and an SDS of 12.9 ± 6.9. However, the resting perfusion studies in these patients were nearly normal, with a mean SRS of 1.0 ± 2.7 and few nonreversible segments (mean, 0.43 ± 1.1). MPS results according to coronary collateral group are summarized in Tables 3 and 4, and individual perfusion scores are plotted in Figure 1. The 2 groups did not significantly differ in frequency of abnormal MPS (SSS ≥ 4); mean perfusion scores, including SSS, SRS, and SDS; reversible segments; or nonreversible segments. Even when comparing patients with proximal LAD occlusion, we found no significant difference in any of the perfusion scores between groups.

CTO MPS scores as a function of coronary collateral group. Group I patients (less than excellent collaterals) are shown by open symbols; group II patients (excellent collaterals), by closed symbols.
Myocardial Perfusion SPECT Results According to Collateral Group
Myocardial Perfusion SPECT Results According to Presence of Regional Wall Motion Abnormality on Left Ventricular Angiogram
DISCUSSION
In patients with a single-vessel CTO and no prior MI, our study investigated the relationship between the Rentrop angiographic grade of coronary collaterals, rest and stress MPS variables, and regional wall motion abnormality. Patients with single-vessel CTO had severe and extensive stress-induced myocardial perfusion defects regardless of the grade of angiographic coronary collaterals. The MPS defects were predominantly reversible, suggesting that coronary collaterals preserved myocardial viability in the regions subtended by a total coronary occlusion. Resting defects in the overall population were minimal; however, patients with resting wall motion abnormality had higher resting perfusion scores, consistent with a matched decrease in resting myocardial perfusion and function (myocardium hibernation). Interestingly, when patients with and without regional wall motion abnormality were subdivided by collateral group, there was no significant difference in any perfusion parameter, including rest perfusion scores, between patients in the 2 collateral groups.
Experimental Studies on Coronary Collateral Circulation
In a canine model of collateral development, although collateral vessel blood flow may be adequate to meet myocardial needs at rest (14), the collateral circulation is generally not sufficient to meet myocardial demands during exercise (15). In a canine model of a CTO with collaterals from a source vessel, even well-developed grade 3 collaterals were shown to distribute only a small fraction (<20%) of source artery flow to the collateral bed and, in the setting of an abrupt occlusion, were generally insufficient to provide normal flow to the region in the distribution of the CTO (16).
Coronary Collaterals and Myocardial Perfusion Scintigraphy
The results of previous studies assessing the relationship between myocardial perfusion scintigraphy and coronary collateral vessels remain inconclusive. With PET, several studies have suggested that coronary collaterals preserve resting myocardial flow but are inadequate to protect against reduced blood flow during hyperemic stress (17,18). In contrast, several studies with planar 201Tl scintigraphy suggested that coronary collaterals also prevent stress-induced ischemia (19–24). The reason for the discordance in these PET and planar 201Tl studies is unclear. In the only study we encountered reporting stress SPECT results, He et al. demonstrated that in patients with single-vessel total coronary artery occlusion without MI, stress-induced myocardial ischemia is almost always present, irrespective of the presence or absence of angiographic collaterals (2). They did not assess resting perfusion findings, because 201Tl stress/redistribution SPECT (without resting injection) was one of the many MPS protocols used.
Collateral Grade and Myocardial Perfusion
Using controlled coronary artery occlusion by an angioplasty balloon, Rentrop’s group initially described the classification of coronary collaterals in 1985 (5). Later, the same group demonstrated that grade 3 collaterals appear to be almost completely protective during transient, sudden, and total coronary occlusion (25). All patients with grade 0 or 1 collaterals had pain at the time of balloon inflation during coronary angioplasty, whereas only 36% of patients with grade 2 or 3 collaterals had pain during occlusion. The group further demonstrated a correlation between collateral grade and the percentage of hypocontractile myocardium as well as the sum of ST-segment elevation. Subsequent studies demonstrated a relationship between exercise-induced U-wave collaterals such that this exercise finding was associated with well-developed collaterals and less angina and ST elevation during subsequent balloon occlusion with angioplasty. The implications of these findings were that well-developed collaterals protect against MI at the time of acute coronary occlusion; however, the long-term implications of well-developed collaterals were not addressed by these studies.
Sand et al., using 99mTc-sestamibi injected during balloon occlusion of the left anterior descending coronary artery in 30 patients, showed that recruitable collaterals had a protective effect on resting MPS (26). Furthermore, they found that all 6 patients with no or mild perfusion defects on MPS during occlusion had Rentrop grade 3 collaterals. In contrast, our findings in the chronic setting demonstrated that resting flow is often preserved in patients with CTO and no history of prior MI, even with Rentrop grade 1 collaterals. The difference in these findings may be related to differences in perfusion through collaterals acutely and chronically.
The disparity between the angiographic grade of coronary collateral vessels and rest or stress myocardial perfusion may have at least 2 potential explanations: First, angiographic grading by current procedures is limited (27), since coronary angiography demonstrates only those epicardial collateral channels with a lumen diameter > 100 μm (28), giving no insight to the subendocardial and intramural intercoronary channels, which are the most numerous and probably most important (4). Such vessels can be as small as 20 μm in diameter (29,30). Second, the development and visualization of collateral vessels depend, at least in part, on the transanastomotic pressure between the collateralizing and the occluded vessel (31).
Collaterals and Resting Wall Motion Abnormality
Of the 45 patients in this study on whom left ventriculography was performed, 30 (67%) had no regional wall motion abnormalities. Of interest, resting perfusion abnormalities were minimal in these patients, whereas most had severe and extensive stress-induced perfusion defects. The near absence of resting perfusion defects would support the concept that resting wall motion abnormalities in patients with coronary artery disease without infarction may be caused more commonly by repetitive stunning than by true myocardial hibernation (17,32). Our findings do suggest that true hibernation, although less common, may play a role in some of these patients, since the resting perfusion findings, although minimal overall, were more abnormal in the patients with than in those without resting wall motion abnormality. The protective effect of collaterals on resting left ventricular function was demonstrated in a study by Werner et al. using intracoronary Doppler ultrasound during balloon angioplasty (33). In the setting of CTO, although epicardial collaterals were observed in only 28% of patients, collateral function calculated by collateral flow index and collateral resistance index was better in patients with normal regional function than in those with impaired regional function (33,34). Our data are consistent with these findings in that patients with higher-grade angiographic collaterals (group II) less frequently had resting regional wall motion abnormality than did patients with lower angiographic collateral grades.
Study Limitations
Although we excluded patients with a history or ECG evidence of MI, the possibility of an undocumented MI or a patient-recall bias could not be ruled out. Because most of our patients underwent coronary angiography after the myocardial perfusion study, a referral bias probably existed. Patients demonstrating ischemia might have preferentially been referred for catheterization, whereas people (not yet patients) or patients with excellent collateral function resulting in no or minimal ischemia might not have been referred for MPS or catheterization and, consequently, not have been included in this study. Only the Rentrop method of collateral assessment was evaluated; it is possible that the results of other angiographic methods of collateral assessment may have differed. The scintigraphic findings in the current work were not analyzed quantitatively but were interpreted by experienced observers using a standardized, semiquantitative approach to visual interpretation that we have developed and have documented to be highly reproducible (35). These visual results form the basis for quantitative analysis programs that have been shown to correlate strongly with the results of quantitative analysis (35,36). Although the semiquantitative system of analysis worked well, a quantitative method might have been preferable for this study. Regional wall motion abnormalities were assessed in only 45 of the 56 patients. Resting gated SPECT, which could have provided important insight into the relationships between perfusion and function, was performed on only a small proportion of the patient population and was not used in the analyses.
CONCLUSION
In the setting of single-vessel CTO and no prior MI, coronary collaterals appear to protect against resting perfusion defects. Excellent angiographic collaterals may prevent resting regional wall motion abnormalities but do not appear to protect against stress-induced perfusion defects.
Acknowledgments
This work was supported in part by a grant from Bristol-Myers Squibb Medical Imaging Inc., Billerica, Massachusetts, and a scholarship granted by the Egyptian Cultural and Educational Bureau, Washington, DC. This study was presented in part at the 49th annual scientific sessions of the American College of Cardiology, Orlando, Florida, 2001.
Footnotes
Received Nov. 25, 2003; revision accepted Dec. 15, 2003.
For correspondence or reprints contact: Daniel S. Berman, MD, Department of Imaging, Cedars-Sinai Medical Center, 8700 Beverly Blvd., Taper Room 1258, Los Angeles, CA 90048.
E-mail: bermand{at}cshs.org
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of collateralisation to a concomitant chronic total occlusion in patients with ST-elevation myocardial infarction: a subanalysis of the EXPLORE randomised controlled trial
- Long-Term Survival Benefit of Revascularization Compared With Medical Therapy in Patients With Coronary Chronic Total Occlusion and Well-Developed Collateral Circulation
- 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions
- 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions
- Effect of Progenitor Cells on Myocardial Perfusion and Metabolism in Patients After Recanalization of a Chronically Occluded Coronary Artery
- Percutaneous Recanalization of Chronically Occluded Coronary Arteries: A Consensus Document: Part I
- The Year in Cardiac Imaging