


Abstract
Disorders of the upper digestive tract have a high impact on modern society, in terms of both direct and indirect health care costs and of social burden. The most common presenting symptom is either dysphagia or dyspepsia. Discriminating specific diagnoses within this wide group of diseases requires sound clinical judgment and application of procedures to distinguish organic from nonorganic disease and to further characterize the functional or motility disturbance of nonorganic diseases. Non–radionuclide-based diagnostic techniques include both noninvasive tests (upper gastrointestinal barium series, ultrasonography, and breath test for gastric emptying) and invasive procedures (fiberoptic endoscopy, esophagogastroduodenoscopy, pharyngeal manometry, stationary esophageal manometry, 24-h pH monitoring, esophageal biliary reflux monitoring, multichannel intraluminal impedance, and electrogastrography). Some of these techniques are not well tolerated by patients or not widely available. Radionuclide transit/emptying scintigraphy provides a means of characterizing exquisite functional abnormalities with a set of low-cost procedures that are easy to perform and widely available, entail a low radiation burden, closely reflect the physiology of the tract under evaluation, are well tolerated and require minimum cooperation by patients, and provide quantitative data for better intersubject comparison and for monitoring response to therapy. Despite the relatively low degree of standardization both in the scintigraphic technique per se and in image processing, these methods have shown excellent diagnostic performance in several function or motility disorders of the upper digestive tract. Dynamic scintigraphy with a radioactive liquid or semisolid bolus provides important information on both the oropharyngeal and the esophageal phases of swallowing, thus representing a useful complement or even a valid alternative to conventional invasive tests (such as stationary esophageal manometry) for evaluating abnormalities of oropharyngoesophageal transit. Clinical applications of esophageal transit scintigraphy include disorders such as nutcracker esophagus, esophageal spasm, noncardiac chest pain of presumed esophageal origin, achalasia, esophageal involvement of scleroderma, and gastroesophageal reflux and monitoring of response to therapy (either medical or surgical treatment of disease—for example, organic disease such as esophageal cancer). Scintigraphy with a radiolabeled test meal represents the gold standard for evaluating gastric emptying, whereas more recent radionuclide methods include dynamic antral scintigraphy and gastric SPECT for assessing gastric accommodation. Clinical applications of gastric-emptying scintigraphy include, among others, evaluation of patients with dyspepsia and evaluation of gastric function in various systemic diseases affecting gastric emptying. The present review includes the proposal of clinical algorithms for evaluating patients with the main disorders of the upper digestive tract. These algorithms, originally derived from available literature, have been developed on the basis of a vast clinical experience in conjunction with the specialists more deeply involved in the care of patients with such disorders (medical and surgical gastroenterologists and nuclear medicine physicians). The role of radionuclide gastroesophageal motor studies is clearly identified in the various steps of patients’ management, from the initial diagnostic approach to functional characterization to postoperative follow-up or monitoring of medical therapy.
- upper digestive tract
- radionuclide transit studies
- quantitative parameters
- diagnosis and monitoring
- functional disorders
- motility disorders
- clinical algorithms
Disorders of the upper gastrointestinal tract are prevalent in all countries. These diseases reduce the quality of life and often require long-term medication for control of symptoms (1–3). In the late 1980s, about 12% of the U.S. population (approximately 34 million people) reported at least one chronic digestive disease. Diagnosis and treatment of these disorders caused 1.8 hospitalizations per 1,000 people (4). The estimated incidence of gastroesophageal reflux disease (GERD) is about 18,600,000 cases per year in the United States. For comparison, peptic ulcer disease has an incidence of 6,730,000 cases per year and Barrett’s esophagus has an incidence of 808,000. In an unselected population the overall incidence of GERD and dyspeptic symptoms is about 45% in the United States and 30% in Canada, with the associated deterioration in the quality of life (1).
In European countries, GERD and dyspeptic symptoms occur in about 30% of the population. There are marked regional differences in the incidence of these disorders, ranging from 16% in Belgium and Norway to 41% in France (3,5).
The global cost of upper gastrointestinal tract diseases is difficult to calculate because, in addition to the direct costs, there are the additional costs of reduced work performance, absence from work, premature retirement, and other factors. These costs are estimated to add about 30% to the direct costs (hospital stays, medical procedures, physician charges, rehabilitation and retraining procedures, and drugs) (6). In the United States alone such global costs easily reach tens of billions of dollars each year (2), with European countries following closely (3). The cost of drugs for disorders of the upper gastrointestinal tract is more than €1.5 billion in the United Kingdom and $6.5 billion in the United States (2,3). Substantial savings can occur by optimizing diagnosis and treatment. Optimal treatment requires accurate characterization of the underlying disorder. Radionuclide methods are well suited for evaluating this group of diseases.
Upper gastrointestinal disease often has symptoms of dysphagia (difficulty swallowing) and dyspepsia (pain or discomfort in the upper abdomen). These symptoms are frequently due to impairment of motor function. Radionuclide gastroesophageal motor studies are well suited for identifying and characterizing these disorders semiquantitatively and for monitoring the efficacy of therapy. Understanding the anatomy and physiology of the upper gastrointestinal tract helps in selecting the procedure most suitable for each patient and in interpreting the results.
ANATOMY
The adult esophagus is a hollow muscular canal that varies in length with patient height but averages about 25 cm, with a diameter of about 2.5 cm. It begins in the neck at the lower border of the cricoid cartilage, extends through the diaphragm, and ends at the cardia of the stomach. The esophagus is perfused by branches from the inferior thyroid artery, descending aorta, left gastric branch of the celiac artery, and inferior phrenic artery of the abdominal aorta. There is both superior and inferior lymphatic drainage. Muscular activity is under the control of the autonomic nervous system, with parasympathetic innervation through the vagus and sympathetic innervation through preganglionic fibers originating at T1–T10, mostly between T4 and T6 (Fig. 1). The stomach is a hollow muscular viscus about 30 cm long and 15 cm wide, with a capacity of about 1 L in the resting state to a maximum of about 5 L. The mucosa of the stomach has more than 35,000 gastric glands, producing mucus, hydrochloric acid, and digestive enzymes. Blood vessels to the stomach arise from the common hepatic, left gastric, and splenic arteries to form 2 vascular arcades, which perfuse the greater and lesser curvature of the stomach. Lymph drains from the stomach to the left and right gastric nodes and the subpyloric and omental nodes, which drain to the hepatic and celiac nodes. The stomach has both sympathetic and parasympathetic innervation, which controls both the secretory and the motor activity of the organ.
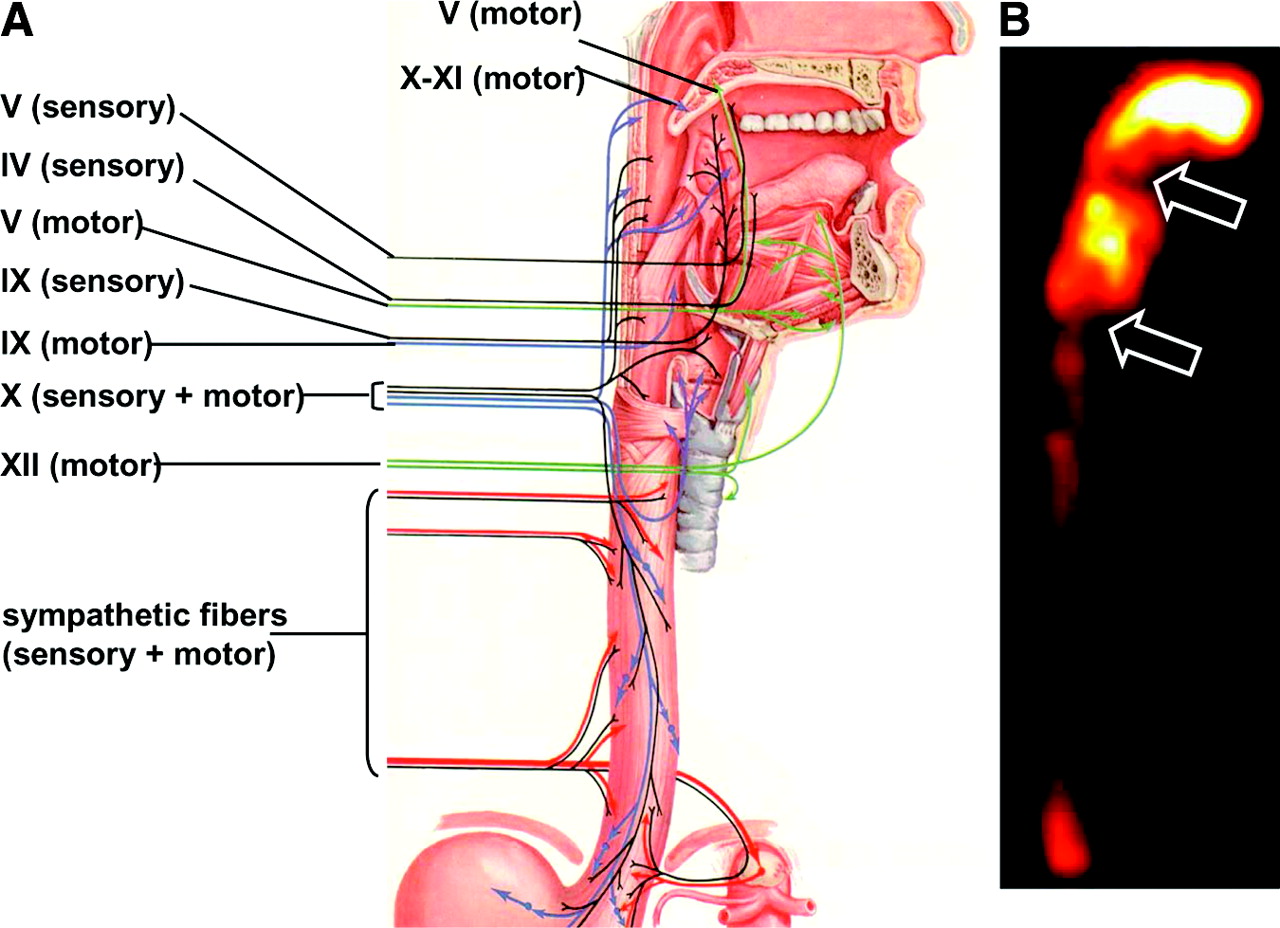
(A) Anatomic drawing shows the complex afferent and efferent neuroregulation of deglutition (sensory fibers in black, motor fibers in different colors) and cranial nerves participating in the system. (B) Summed image from dynamic recording of oropharyngoesophageal radionuclide transit study (liquid bolus) allows clear identification of the various anatomic regions. Upper arrow indicates posterior mouth sphincter, lower arrow indicates upper esophageal sphincter, and space between arrows is pharyngeal region. During scintigraphic acquisition, patient stood facing collimator surface for an anterior view of the chest, with head and neck tilted left. (Modified from (235).)
PATHOPHYSIOLOGY OF MOTOR FUNCTION
Oropharyngeal Motor Function
The normal esophagus propels a bolus of solid or liquid from the mouth to the stomach. Liquids require approximately 2 s to traverse the esophagus, whereas solids can take about 9 s. The process begins with swallowing. Of the 6 phases that constitute swallowing, only the first phase is totally voluntary: positioning of the bolus on the tongue’s central groove and propulsion of the bolus toward and through the faucial arches (oral phase) (7). The subsequent phases are involuntary and are initiated by elevation and retraction of soft palate, with closure of the nasopharynx associated with simultaneous opening of the posterior mouth sphincter (oropharyngeal phase). The next 2 steps (proximal and distal pharyngeal phases) take the bolus into the hypopharynx (8). The most important and delicate task of these 2 phases is avoiding passage of food through the larynx into the respiratory tree (9). Aspiration is avoided through a complex, multistep process involving a reflex mechanism consisting of sensitive afferences and articulated motor efferences (10). The pharyngoesophageal phase is marked by progression of the bolus through the striated cricopharyngeus muscle, or upper esophageal sphincter, whose function is to avoid reflux of the esophageal content back into the pharynx (11,12). Although the first phases of swallowing are concentrated in a relatively short space immediately posterior and inferior to the mouth, their physiologic coordination requires complex interaction of muscular and nervous structures. Coordinating this process requires participation of the IV, V, IX, X, and XII cranial nerves and of sympathetic fibers originating mostly at T4–T6 (Fig. 1). Oropharyngeal dysphagia can be caused by degenerative disorders of the central nervous system (Parkinson’s disease, multiple sclerosis, and supranuclear palsy), of the spinal motor neuron (amyotrophic lateral sclerosis), of the neuromuscular junction (myasthenia gravis), or of striated muscle per se (polymyositis and muscular dystrophy) (13,14).
Esophageal Motor Function
The last step of swallowing (the esophageal phase) involves the traveling of a much longer distance by the bolus yet involves a much simpler peristaltic mechanism aided by gravity. The primary peristaltic pump originating in the pharynx propagates through the inner (circular) and the outer (longitudinal) muscular layers of the esophagus at about 4 cm/s. Coordination of the primary peristaltic pump with postswallowing relaxation of the lower esophageal sphincter (LES) lets the bolus enter the stomach (15). Disorders of peristalsis can be caused by derangement of motor innervation provided by the vagus nerve for the striated muscle fibers, derangement of the sympathetic and parasympathetic innervation provided for the smooth muscle, and derangement of the myenteric plexus (Table 1) (16).
Classification of Gastroesophageal Motor Disorders
Functional esophageal disorders are a heterogeneous group of chronic disturbances often complicated by association with psychiatric or psychologic disorders, as determined on the basis of a lack of identifiable structural or metabolic damage (Table 2). After irritable bowel syndrome, esophageal disorders are the second most frequent functional gastrointestinal disorder and are usually not associated with GERD or other structural, metabolic, or motor disorders (17,18).
Classification of Functional Gastroesophageal Disorders
Achalasia is a primary esophageal motility disorder of unknown cause. The disease results in partial or absence of relaxation of the LES and loss of esophageal-body peristalsis. It is characterized by progressive neuronal degeneration in the myenteric plexus, with a paucity of ganglion cells, the presence of neural fibrosis, and some degree of chronic inflammation at histology. There is also a significant decrease in the synthesis of nitric oxide, a mediator of relaxation in the LES. Dysphagia and varying degrees of regurgitation, weight loss, and chest pain are the most common clinical presentation. Achalasia may present at any time, with the highest incidence occurring between 20 and 50 y of age. Most patients seen today in a surgical practice have had dilation or botulinum toxin injections before. Nevertheless, having undergone previous therapies should not be regarded as proof that a patient has achalasia. In fact, one can confuse the clinical manifestations of achalasia with those of other esophageal disorders; thus, patients must have, in addition to dysphagia and regurgitation, the radiologic and manometric findings consistent with achalasia.
GERD is common among the populations of industrialized countries (19). Heartburn, the most common symptom of gastroesophageal reflux, occurs daily in approximately 10% of the population and is the major reason for the consumption of antacids in our society. GERD can be overlooked for several reasons: First, the most common symptoms, heartburn and regurgitation, occur in only half of these patients; second, because of the natural history of the disease and the frequency of its spontaneous remission, many patients will not seek medical advice; and third, there is no diagnostic standard for GERD.
Symptoms of GERD are divided into 2 categories: esophageal, which includes typical esophageal reflux complaints (heartburn, regurgitation, and dysphagia) and noncardiac chest pain, and extraesophageal, which includes pulmonary (asthma and recurrent aspiration pneumonia), otolaryngologic (hoarseness, chronic dry cough, chronic sore throat, and globus sensation), and dyspeptic symptoms (upper abdominal pain, nausea, vomiting, and bloating).
The work-up of patients with gastroesophageal symptoms should include confirmation of the presence of pathologic gastroesophageal reflux and exclusion of other motility disorders or lesions of the esophagus and stomach, quantification of the severity of reflux, and clear definition of the anatomy of the esophagus and gastroesophageal junction.
Gastric Motility and Emptying
Gastric Motor Function.
Motor functions of the stomach result from a complex interaction of muscular and neural activity in physiologically distinct regions, integrated with feedback regulation from the small bowel (20). The stomach can be divided into 3 functional regions: the proximal stomach (cardia, fundus, and proximal body), the distal stomach (distal body and antrum), and the pylorus.
The proximal stomach regulates gastric emptying by accommodating and storing food and by regulating intragastric pressure and tonic propulsion of chyme into the distal stomach. Smooth muscles of the proximal stomach do not exhibit rhythmic fluctuations in their membrane potential but, rather, are in a state of continual partial contraction, or tone. This motor activity of the proximal stomach maintains a stable intragastric pressure even after consumption of a large meal; in fact, the stomach can accommodate up to 2 L of fluid with less than a 10–mm Hg increase in intragastric pressure.
This property is mediated by 2 neurally mediated reflexes: receptive relaxation (vagovagal reflex reducing gastric tone in response to swallowing) and gastric accommodation. The latter reflex is elicited in response to gastric distension and is mediated by stimulation of mechanoreceptors in the gastric wall.
In contrast to the proximal stomach, the distal stomach exhibits electrical and contractile activity characterized by rhythmic oscillation in the membrane potential, accompanied by phasic, rather than tonic, motor activity. This regular rhythmic depolarization, known as pacesetter potentials (21,22), originates in the interstitial cells of Cajal (network of specialized cells extending from the corpus to the distal antrum) and initiates gastric peristalsis. The gastric pacesetter potential (which propagates in both distal and circumferential directions but not proximally to the fundus) has a baseline frequency of 3 cycles per minute and is modulated by parasympathetic (vagal) and sympathetic innervation, in addition to the intrinsic enteric neurons organized as the myenteric and submucosal plexuses (23). Motor activity of the distal stomach results in mixing, grinding, and trituration of solid food (ingested food is propelled distally by antral contractions, only to be repelled back into the more proximal stomach) and also regulates gastric emptying. For equivalent volumes of ingested food, the amplitude of phasic contractions is more intense in response to particulate than to homogenized material. Additional neural and hormonal factors modulate postprandial gastric motility.
The pylorus is a specialized region of the stomach at the junction of the antrum with the duodenal bulb, which acts as a sieve, regulating outflow of intraluminal gastric content. Because of the thickness of the smooth muscle layers and the presence of highly redundant mucosa, the pylorus acts as a mechanical stricture preventing the passage of large particles.
Gastric Emptying.
Because the stomach handles solids and liquids differently, liquid gastric emptying and solid gastric emptying can be specifically described.
Inert liquids, such as water, empty exponentially; thus, the volume of fluid emptied into the duodenum in a given time is a constant fraction of the volume remaining in the stomach. The emptying rate is modified by volume, osmolality, pH, caloric density, and nutrient content of the liquid. Although interesting from the physiologic point of view, evaluation of liquid emptying per se is of little if any clinical significance (20,24).
After ingestion of a meal, solids are kept in the stomach to be ground and triturated into fine particles. During this phase, there is no emptying. This interval has been called the lag phase. In addition to being reduced into a finely dispersed suspension of particles, the solid material is converted into chyme because of extensive contact with gastric acid and peptic enzymes. When the solid particles are <1–2 mm in diameter, a linear emptying phase commences during which the chyme is slowly delivered to the duodenum (25–29). Physical and nutritional properties may modify the rate of delivery of solid food to the small bowel by modulating the duration of the initial lag phase. Larger particles prolong the lag phase, whereas evenly dispersed suspensions have a relatively short lag phase; however, after the initial lag phase a homogenized meal and a nonhomogenized meal empty at a similar rate (30). The emptying rate is also affected by the caloric content of the meal and its composition of total fats, triglycerides, and carbohydrates (26,27). Although the volume of liquid ingested with the solid food modifies the rate at which the solid food is delivered to the intestine, the liquid component is emptied more rapidly than the solid component, suggesting that the stomach can distinguish between the 2 phases when present simultaneously (31). The gastric-emptying rate can also be modified by additional factors such as age, sex, menstrual cycle, and time of day (32–36). Although variable, the lag phase of gastric emptying is prolonged in some disease states, such as diabetic gastroparesis (37), and is shortened after antrectomy and pyloroplasty or after administration of metoclopramide and domperidone (38).
Gastric neuromuscular disorders, such as visceral hypersensitivity, gastric dysrhythmias, gastric dysrelaxation, antral hypomotility, pylorospasm, and gastroparesis, can cause dysmotility-like dyspepsia characterized by various symptoms such as early satiety, fullness, abdominal discomfort, bloating, nausea, and vomiting (23,39). The other possible face of the dyspepsia syndrome is represented by ulcer-like symptoms, whose predominant feature is pain centered in the upper abdomen.
When considering a patient with either dysmotility-like dyspepsia or ulcer-like dyspepsia, one should keep in mind that dyspepsia can either be the expression of a well-defined organic condition (peptic ulcer, GERD, malignancy, hepatobiliary disease, or side-effects of drugs) or have no association with definite structural or biochemical disorders (functional dyspepsia). Therefore, functional dyspepsia should always be considered after other organic conditions have been excluded (40,41).
NON–NUCLEAR MEDICINE EVALUATIONS
Upper Gastrointestinal Series
Upper gastrointestinal radiography with barium contrast medium allows examination of the esophagus, stomach, and duodenum, whereas special protocols have been developed to evaluate the oropharyngeal phase of swallowing. This is the procedure most patients who complain of dysphagia still undergo before any other testing. On the other hand, current diagnostic protocols call for esophagogastroduodenoscopy as a first-line approach for patients who complain of heartburn or regurgitation, chest pain, or epigastric pain or have unexplained vomiting or severe indigestion. This leaves a more limited role than in the past for an upper gastrointestinal series for these symptoms. Barium radiography is now considered a second-line diagnostic test whenever endoscopy reveals no obvious abnormalities explaining these symptoms.
Different barium suspensions (solid, semisolid, or liquid) can be used to characterize the parameters of swallowing. Although capable of identifying the major categories of dysfunction in patients with pharyngoesophageal dysphagia (42), the examination cannot estimate muscle fatigue, measure pharyngeal contractile forces, or estimate the intrabolus pressure during swallowing (12).
The esophagogram should include upright double-contrast views with a high-density barium suspension to assess mucosal disease, and prone single-contrast views with a low-density barium suspension to assess distensibility and motility. Barium swallows allow a dynamic evaluation of esophageal motility and transit of the barium boluses from the mouth to the stomach through the entire esophagus. Cine- and videoradiography (possibly recorded as digital videofluorography) help in evaluating functional disorders of the pharyngoesophageal and the esophageal phases of swallowing. Particular attention is paid to evaluation of the gastroesophageal junction and hiatus through varying of the patient position (e.g., oblique, standing, and supine).
An upper gastrointestinal series should always include evaluation of the stomach and duodenum, even if symptoms suggest a primarily esophageal disorder.
Ultrasonography
The oral phase of swallowing can be evaluated by positioning the ultrasonography probe under the chin to the hyoid region, using transverse and longitudinal scans to visualize the tongue and mouth floor both at rest and during swallowing of a bolus (43,44). This procedure can be used to identify various abnormalities, such as inability to keep the bolus in the mouth, lack of backward propulsion of the bolus, and asymmetric contraction of the tongue.
Although a simple ultrasonography examination can give useful information on visceral wall thickness, a functional evaluation is needed for patients with upper gastrointestinal disorders to gain data on esophageal and gastric motility. As with other diagnostic ultrasonographic applications, the test is highly dependent on the operator’s skill; in addition, the test is relatively time consuming because it requires repeated and prolonged observations (45,46).
The proximal (cervical) tract of the esophagus and its distal tract (gastroesophageal junction) can be explored in children. Ultrasonography can detect gastroesophageal reflux in children up to 5 y of age with 100% sensitivity and 87.5% specificity (47).
Even though air in the gastrointestinal tract and a thick abdominal wall can interfere with visualization of the fundic and antral regions, ultrasonography can evaluate gastric volume and emptying and transpyloric flow (45,48). A high correlation has been found between gastric-emptying values evaluated by ultrasonographic procedures and those derived by radionuclide-based procedures (49). In addition, ultrasonography can measure gastric area and volume and detects gastric contraction and distension (50).
Functional ultrasonography of the stomach is indicated mainly for evaluation of patients with dysmotility-like dyspepsia (45), evaluation of both dyspeptic and nondyspeptic patients with chronic disease potentially causing delayed gastric emptying (e.g., diabetes mellitus, systemic sclerosis, and myotonic dystrophy) (51,52), monitoring of the effects of pharmacologic and nonpharmacologic agents potentially affecting gastrointestinal motility (53), and evaluation of newborns with suspected hypertrophic pyloric stenosis (54).
Breath Test for Gastric Emptying
The use of breath tests in gastroenterology has become increasingly popular since stable isotopes such as 13C were introduced. Mass spectrometers are required to measure the concentration of these nuclides in expired air. These instruments are now widely available (at relatively low cost) and easy to operate. This technologic evolution has caused the β-emitter 14C to largely be replaced by the mass isotope 13C. This change avoids the need for extensive isotope inventories and record keeping, eliminates radiation exposure for both patients and personnel, and allows gastroenterologists to perform these procedures in their own environment.
Combined with different food substrates, octanoic acid (solid meal) or acetate (liquid meal) labeled with 13C are used to assess gastric emptying. The underlying concept is that these compounds pass unabsorbed through the stomach to the duodenum, where they are quickly absorbed. After absorption in the duodenum, portal circulation transports the 13C-labeled substrate to the liver, where fast metabolic degradation produces 13CO2, which is excreted with exhaled air. Breath is therefore tested for enrichment with13CO2 at regular intervals for up to 6 h, thus deriving the basic parameters of 13CO2 appearance in the breath (beginning of gastric emptying) and time-related enrichment (a rising curve whose slope is related to the gastric-emptying rate) (55,56).
The test is safe and noninvasive, can be performed on children and during pregnancy, and can be repeated whenever necessary, as when monitoring the efficacy of therapy or assessing the effects of drugs on gastric emptying (56). Because the breath test is not an imaging technique, information is not provided about intragastric distribution of the different phases of the meal. Moreover, considering gastric emptying as the sole limiting step of the delivery of 13CO2 to the breath can be misleading (thus reducing the reliability of the test) in certain conditions such as malabsorption; in diseases of the pancreas, liver, or lungs; or in the presence of visceral hemodynamic changes (e.g., physical exercise) (46,56).
Fiberoptic Endoscopy
Small, dedicated fiberoptic endoscopes are available to directly visualize all mucosal surfaces of the nasopharynx, pharynx, and larynx. Nasoendoscopy is minimally invasive, repeatable, and easy to perform and allows bedside evaluation for nonambulatory patients. Although this technique can evaluate both the motor and the sensorial components of swallowing, it can examine only the pharyngeal phase, with the additional limitation of a swallowing blackout (57).
A recent variant of the technique uses endoscopic delivery of pulsated air on the laryngeal mucosa to estimate the adductional reflex contraction of vocal folds or the patient’s ability to discriminate increasing pressure (58).
Esophagogastroduodenoscopy
This is the procedure that most gastroenterologists and surgeons choose when evaluating patients with gastroesophageal disorders, as it permits direct visualization of the esophageal, gastric, and duodenal mucosa and permits tissue biopsies of suggestive lesions. Endoscopy is indicated for any patient complaining of dysphagia or dyspepsia, generally as a first-line diagnostic procedure. More rarely (depending on the choice of the general practitioner and local logistics), endoscopy is performed after an upper gastrointestinal series revealing no obvious abnormalities.
The gastroesophageal flap valve is easily seen during esophagogastroduodenoscopy, thus revealing esophagitis and abnormal hiatal and paraesophageal hernias. Esophageal diverticula can also be visualized during endoscopy. This invasive technique is not always well accepted by patients and requires a relatively long learning curve for the operator. A consensus has been reached on the grading of mucosal damage and esophagitis, thus minimizing interobserver variability and subjectivity in reporting results (59). However, about 55% of patients with typical GERD-related symptoms do not have gross esophagitis, although careful endoscopic examination may detect, in about 12% of patients with GERD, the presence of intestinal metaplasia (Barrett’s esophagus, a condition associated with a 40-fold increased probability of development of esophageal adenocarcinoma).
Pharyngeal Manometry
A transnasally positioned manometric probe permits estimation of the rate of upper esophageal sphincter relaxation and the strength of pharyngeal contraction while also measuring the duration of these 2 events (60). Manometry can be performed at the time of videofluoroscopy (manofluorography) for better positioning of the pressure sensor and for distinguishing between recordings of intrabolus pressure and recordings from within a closed lumen (8).
Pharyngeal manometry is more difficult to perform than the esophageal test because of the extreme longitudinal and radial asymmetry of intraluminal pressures recorded from within the pharynx during deglutition (61). Moreover, movements during the pharyngeal phase of swallowing frequently displace the pressure sensor, thus making the technique difficult to standardize (62).
Stationary Esophageal Manometry
Esophageal manometry is usually performed on patients with dysphagia in whom endoscopy or a barium swallow study has excluded obvious structural abnormalities. The dynamic pressure measurement is especially useful in the diagnosis of primary esophageal motility disorders such as achalasia, diffuse esophageal spasm, nutcracker esophagus, or hypertensive LES. It is also useful in the characterization of esophageal disorders secondary to systemic diseases such as scleroderma, dermatomyositis, and polymyositis.
Although esophageal manometry is rarely indicated in patients with typical GERD-like symptoms, it is crucial for correct placement of the probe for esophageal pH testing in patients with atypical symptoms or unresponsive to proper medical therapy and in patients being considered for antireflux surgery. Esophageal manometry may identify a defective LES, suggesting the diagnosis of GERD, and provides valuable information on peristaltic function (thus allowing selection of the most appropriate antireflux procedure).
Ambulatory pH Monitoring
A pH electrode at the end of a catheter is placed in the esophagus 5 cm above the upper limit of the LES for prolonged monitoring of esophageal pH. The pH electrode is attached to a battery-operated ambulatory device that can record data for up to 24–48 h. This device records pH over a circadian cycle to identify the frequency and duration of esophageal mucosa exposure to acid and the ability of the esophagus to clear gastric reflux and allows correlation of the intensity and duration of symptoms with reflux episodes.
Esophageal exposure to gastric juice is evaluated as 6 major components contributing to a combined score: the percentage of the total time, upright time, and supine time that esophageal pH drops below 4; the total number of reflux episodes per day; the number of episodes > 5 min; and the duration of the longest episode (63,64).
Biliary Reflux
The combination of bile and hydrochloric acid has a noxious effect on esophageal mucosa. An ambulatory bile-reflux monitor (Bilitec 2000; Medtronic) has been developed to detect the presence of bile reflux in the esophagus (65,66). Using bilirubin as a marker for bile, this spectrophotometric system records the frequency and duration of bile exposure in either the stomach or the esophagus over a 24-h period. Combined with 24-h pH testing, the bile-reflux detector gives a more complete profile of a patient’s reflux, thus identifying patients at greater risk for developing complications such as Barrett’s esophagus. Nevertheless, reflux alone of bile in the esophagus cannot be considered the main risk factor for such complications.
Reflux of duodenal content into the stomach, possibly causing alkaline gastritis and intestinal metaplasia in the gastric mucosa, occurs in up to 40%–50% of patients who undergo cholecystectomy (Fig. 2). This condition can also be secondary to gastric surgery that alters the function of the pylorus. As already emphasized, reflux of duodenal and gastric contents into the esophagus can play a role in the pathogenesis of Barrett’s esophagus.
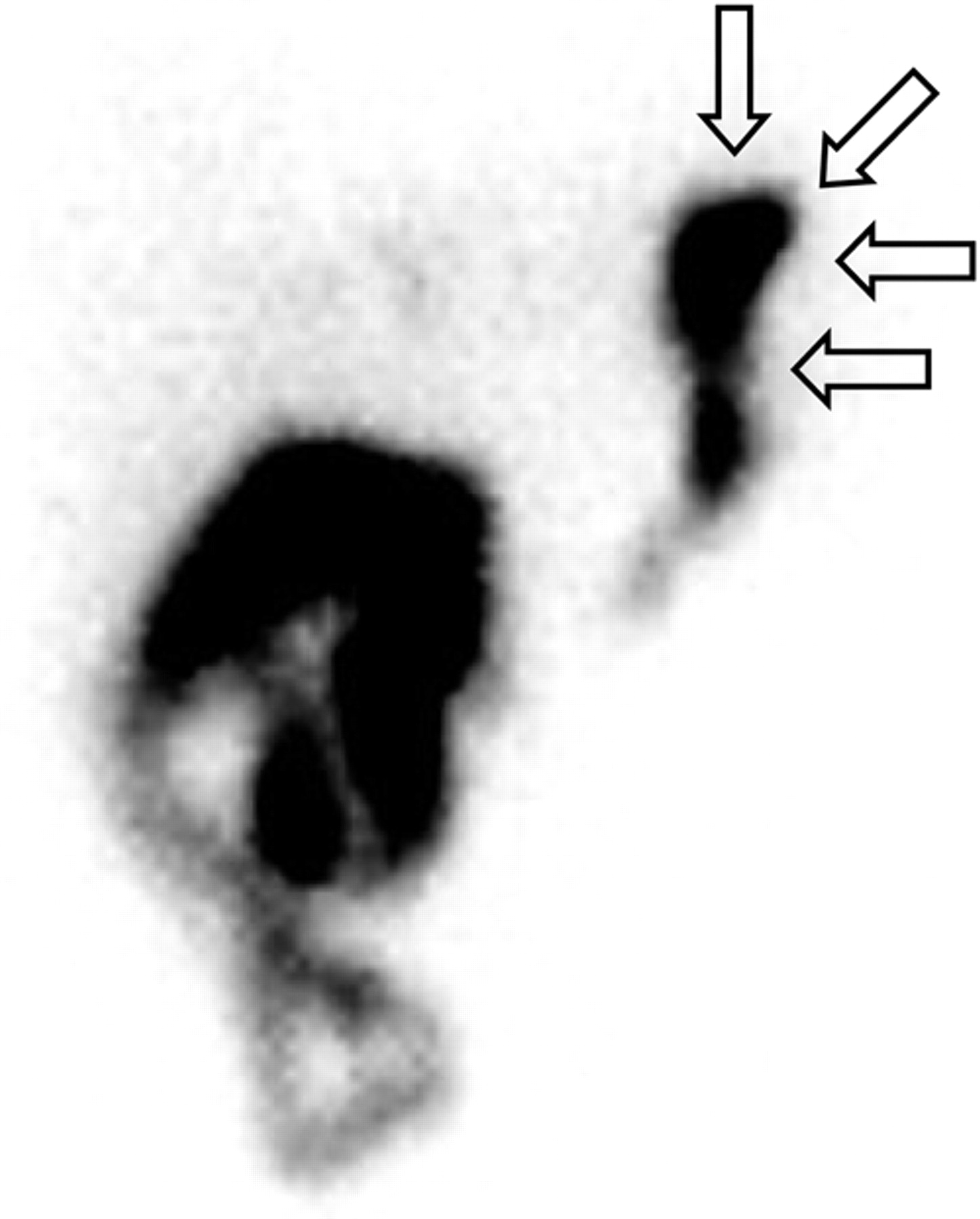
Delayed abdominal hepatobiliary scan (45 min after injection, when radioactivity has almost cleared from hepatocellular compartment) obtained with a 99mTc-iminodiacetic acid analog for a patient with persisting dyspepsia after endoscopic cholecystectomy. Reflux of radioactive bile from duodenum into stomach is obvious (arrows), possibly explaining persistence of symptoms.
Multichannel Intraluminal Impedance (MII)
In this new technique for evaluating esophageal function and gastroesophageal reflux, a change in resistance to alternating current between 2 metal electrodes is produced by the presence of a bolus inside the esophageal lumen (67,68). Combined MII and esophageal manometry provide simultaneous information on intraluminal pressure changes and bolus movement, whereas combined MII and pH monitoring allow detection of reflux episodes irrespective of their pH values (i.e., acid vs. nonacid reflux). Combined MII and pH testing shift the gastroesophageal reflux testing paradigm, in that reflux events are no longer detected solely by pH changes. In fact, reflux presence, distribution, and clearance are detected primarily by MII and are characterized simply as acid or nonacid on the basis of pH change and as liquid, gas, or mixed on the basis of MII.
On the other hand, combined MII and esophageal manometry identify those patients with abnormal esophageal motility on manometry who actually have a clinically important defect in esophageal function. In fact, whereas manometry is an indirect measure of esophageal function, impedance makes it possible to follow the bolus movement.
Impedance technology has great potential for identifying the relative roles of acid and nonacid reflux, such as in patients who continue to have reflux-related symptoms even though their acid is being successfully suppressed or controlled with traditional acid-suppressant therapy. This technique can also help in assessing patients with reflux-related respiratory problems and in understanding dysphagia and its manometric and clinical correlates.
Electrogastrography
By using mucosal, serosal, or cutaneous electrodes, this technique evaluates the fasting and postprandial myoelectrical activity generated by the gastric antrum (69). Cutaneous electrogastrography is most frequently used clinically through the positioning of 3 or 4 electrodes on the epigastrium (46). The normal gastric pacesetter potentials range from 2.5 to 3.75 cycles per minute (cpm). Either bradygastria (<2.5 cpm), tachygastria (3.75–10 cpm), or bradytachygastric arrhythmia (mixed pattern) is detectable (69). Such gastric dysrhythmias can be observed in dysmotilitylike dyspepsia, idiopathic gastroparesis, diabetes mellitus, nausea of pregnancy, and motion sickness and after drug intake or gastric surgery (69), whereas increased wave amplitude has been reported in gastroparesis due to mechanical obstruction (70). Electrogastrography has a complementary role in evaluating patients with dyspeptic symptoms, in predicting gastroparesis, and in assessing gastric motor function in patients with GERD or with chronic constipation or atypical upper-gastrointestinal symptoms (46).
ESOPHAGEAL TRANSIT SCINTIGRAPHY
Esophageal scintigraphy was first introduced by Kazem in 1972 (71). Esophageal scintigraphy performed with a large-field γ-camera views the entire esophagus. The images can quantitate rates of emptying and reflux in all segments simultaneously (72,73). Using esophageal manometry as the gold standard, sensitivities and specificities up to 95% and 96%, respectively, have been reported (74,75), whereas some investigators found esophageal scintigraphy to be more sensitive than esophageal manometry itself or contrast radiology (76,77). Such discrepant results are probably due to the application of different protocols for imaging and data analysis. Relevant differences include bolus consistency, volume and temperature, patient population, single or multiple swallows, display methods, quantitative parameters, and thresholds used in decision making (75).
Because esophageal scintigraphy is not standardized, we will describe various approaches at reaching an acceptable degree of standardization.
Scintigraphy Procedure
Patient Preparation.
Esophageal scintigraphy should be performed after a fast of at least 3 h but preferably overnight. The patient should rehearse the procedure with a practice swallow using unlabeled plain water. This approach helps educate patients about the procedure to encourage their enthusiastic participation.
Image Acquisition.
A large-field-of-view γ-camera fitted with a low-energy, general-purpose collimator is adequate. Because high temporal resolution is preferred for quantitative studies, a high-sensitivity collimator should be used whenever available. Dynamic images in either a 64 × 64 or 128 × 128 matrix must be acquired in a rapid sequence. Because many of the events occur in a short time, images should be acquired at 4–10 frames per second for 60 s. The data can be summed if necessary, but high temporal resolution is necessary to identify brief episodes of reflux or delays in transit through segments of the esophagus.
Although esophageal scintigraphy can be performed with the patient supine or upright, it is more “physiologic” to study patients who are seated and upright. Obviously, quantitative parameters derived from the study (transit time and retention indices) vary according to the position adopted (78–81). Although the upright position mimics the physiologic condition of swallowing and esophageal emptying, by eliminating the effects of gravity the supine position may allow easier demonstration of esophageal motility disorders (82).
Both the anterior and the posterior views have been used for esophageal scintigraphy. The ideal view should minimize tissue attenuation and keep it constant along the entire length of the esophagus. In a cross-section of the body, the esophagus is situated rather anteriorly at its most proximal portion, with a posterior-to-anterior depth ratio of 2.3; it moves posteriorly at its mid portion, where it lies behind the heart, and anteriorly again at its distal extreme. In the anterior view, tissue attenuation is initially relatively low but increases significantly after the middle third, especially because of interposition of the heart. In the posterior view, although tissue attenuation is more significant, it is more uniform along the whole esophageal length. This is especially advantageous because accurate monitoring is possible when the counting rate is relatively independent of distribution within the organ (83). On the other hand, anterior imaging is preferred when the oral and pharyngeal phases are being evaluated, because the mouth and pharynx can be brought closer to the detector surface. External markers on the cricoid cartilage may help improve anatomic localization of the pharynx. An optimum solution uses a dual-head γ-camera with the patient positioned to allow simultaneous recording of anterior and posterior views. The corresponding pixels in each view are combined to create a geometric mean image, which is used for analysis.
Radioactive Bolus.
Any radiopharmaceutical that is not absorbed by the gastrointestinal tract, including 99mTc-sulfur colloid, 99mTc-nanocolloid, and 99mTc-diethylenetriaminepentaacetic acid (DTPA), can be used to prepare a radioactive bolus for esophageal scintigraphy. A dose of at least 7–11 MBq (200–300 μCi) of the 99mTc-labeled agent is usually mixed with water or juice (to form a radioactive liquid bolus) or with a semisolid medium. Most esophageal scintigraphic studies have been performed using a liquid bolus, whereas few studies have used a semisolid bolus (75,84), probably because of the difficulty in reaching a consensus on the viscosity and type of semisolid bolus. In our experience, homogenized baby paste or “gelified water” (available for patients with swallowing difficulties, e.g., in the rehabilitation phase after pharyngolaryngeal surgery) is an optimal viscous semisolid meal, provided attention is paid to keep the bolus viscosity constant and to avoid possible fragmentation.
The pharyngeal ejection force is sufficient to propel the liquid bolus to the gastroesophageal junction, leaving minor work to be done by peristalsis. A more viscous, semisolid bolus is propelled only to the proximal half of the esophagus, thus requiring more intense peristalsis to complete transport over the distal half (85). Therefore, a semisolid bolus is more challenging for assessing esophageal transit, thus resulting in increased sensitivity of the test. When a liquid bolus was compared with a semisolid bolus (homogenized baby meal), the latter showed higher sensitivity at comparable levels of specificity, thus suggesting a preference for semisolid over liquid boluses (75).
Solid boluses consisting of radiolabeled gelatin capsules or chicken liver cubes have been proposed, but such boluses can remain in the esophagus for as long as 2 h despite repeated dry swallows, even in subjects with normal esophageal function. Esophageal scintigraphy performed with a solid gelatin bolus ingested with water demonstrated abnormalities in half the patients with dysphagia and normal esophageal manometry, barium radiology, and pH studies, thus resulting in high sensitivity for the test. The clinical significance of this finding, however, is uncertain (77,86–88).
The volume of the bolus also requires standardization; healthy individuals can easily ingest a liquid 20-mL bolus in a single swallow (89); failing to pass a liquid bolus smaller than 20 mL from the mouth to the esophagus in a single deglutition might reflect impaired oropharyngeal swallowing (90). Esophageal transit may vary substantially according to the bolus volume, as 10-mL boluses were shown to travel more quickly than 20-mL boluses in the upright but not in the supine position (91). In addition, the larger bolus increased the swallow interval required to reestablish normal peristaltic progression of a second bolus (92).
The Swallow (Single or Multiple Swallow, Dry or Wet Swallow).
There is intrasubject variability in repetitive swallows (76,93). Aberrant swallows (which can occur in healthy subjects) may hamper distinction of normal from abnormal findings, especially in borderline cases (79,85,94,95). Barium swallow studies have shown that up to 5 swallows are needed to maximize sensitivity for detecting abnormal swallows (96). Mughal et al. found poor sensitivity (44%) and low specificity (71%) for esophageal scintigraphy performed with a single swallow test, compared with manometry analyzing at least 10 swallows (74). In a similar manner, scintigraphy is expected to yield optimal results if performed with a corresponding number of swallows (84). Two approaches have been proposed to overcome this problem.
In the first approach, the patient is asked to first perform a wet (liquid bolus) swallow, followed 30 s later by a series of 40 dry swallows at 15- to 30-s intervals. Esophageal retention at 10 min is considered an indirect index of esophageal clearance (93). Klein demonstrated that an acquisition spanning only 4 swallows (1 wet and 3 subsequent dry swallows) over 75 s is enough to reliably estimate the esophageal residual fraction (79,97).
In the second approach, the patient is asked to perform 6 independent wet swallows at 30-s intervals; this procedure provides sufficient data to establish an accurate diagnosis of esophageal abnormality (84,98). A summed image of all 6 swallows is used to calculate both time parameters (mean time, mean transit time, and transit time) and retention parameters at particular time points (75). In this multiple-swallow approach, it is important to pay attention to the interval between swallows, because a second swallow in <4 s inhibits the peristaltic wave, and a second swallow between 3 and 8 s may arrest the swallow in the striated muscle. Regular peristaltic waves are elicited at swallow intervals > 10–15 s (92).
In adults, esophageal transit scintigraphy should be completed by acquiring a high-temporal-resolution dynamic sequence over 120 s, during which the patient is asked to perform 4–5 Valsalva maneuvers. In this manner, it is possible to detect the presence of gastroesophageal reflux because of the increased intraabdominal pressure.
Image Processing
Few studies have evaluated patients with oropharyngeal dysphagia with a radiolabeled swallow test; most of these studies concerned patients with neuromuscular dysphagia, and the analysis was based on the oral and pharyngeal transit times and their corresponding indices (99,100). Because of the high interobserver variability in the calculation of transit times (G. Mariani et al., unpublished data, 2003), we believe that simple retention indices obtained after single swallows are a reliable means of assessing oropharyngeal dysphagia.
Visual Analysis and Image Display.
Reviewing the recorded sequence in the cine mode depicts the dynamics of swallowing. This procedure helps to identify aberrant patterns, such as oral or pharyngeal retention, bolus fragmentation, premature swallows resulting in deglutition inhibition, gastroesophageal reflux, tracheal aspiration, and abnormal esophageal events.
The adynamic pattern is characterized by slow progression (or even stopping) of the bolus along the esophagus, but with a craniocaudal direction basically maintained. This pattern is observed in patients with achalasia or scleroderma.
The incoordinate oscillatory pattern is characterized by random disorganized movement up and down the esophagus, as occurs in patients with diffuse esophageal spasm or elderly patients or simply as a passive response to respiration, rather than an esophageal muscular activity (76,79,101). This visual pattern corresponds to multiple peaks of the time–activity curves in all esophageal segments as determined by quantitative analysis.
Svedberg developed an elegant method for presenting dynamic data in a single image with 1 temporal dimension and 1 spatial dimension (swallowing occurs in a craniocaudal direction without any lateral motion) (102). This condensed dynamic image displays the profiles of the swallowing event side by side on the y-axis, along with time on the x-axis. This method displays the whole deglutition event in a single image, and when multiple swallows are performed a summed, condensed image can be generated, thus providing the pattern that more precisely identifies the predominant dysfunction (75,84).
Quantitative Parameters.
The main goal of quantitative analysis is to quantify retention and measure the rate of esophageal transit. Most quantitative approaches use multiple-swallow techniques to overcome problems related to the intraindividual variability of a single wet swallow. Usually 3 regions of interest (ROIs) are drawn, encompassing the upper, middle, and lower thirds of the esophagus. The data can be summed for a total esophageal measurement. The gastric fundus should be identified and excluded from the lower third region, as oscillations linked to respiratory movements interfere with the analysis (Fig. 3).

Typical time–activity curves obtained for oropharyngoesophageal radionuclide transit study (10-mL liquid bolus, upright, anterior view) of healthy subject. Shown are curves for mouth (A), pharynx (B), and whole esophagus (C) and for upper third (D), middle third (E), and lower third (F) of esophagus. Summed image at center defines the 3 esophageal ROIs.
Based on 1 wet (15 mL of water labeled with 99mTc-sulfur colloid) and 3 successive dry swallows, Klein and Wald calculated the fourth-swallow residual activity fraction. A fraction > 19.8% in the posterior view (or 13.1% in the anterior view) is considered abnormal. They also proposed a mathematic 2-compartment model to calculate the mean transit time, by separating the time–activity curve of the first swallow into a rapid component (major fraction of the bolus that has traveled the esophagus) and a slow component (residual fraction of the bolus clearing with subsequent swallows). The mean transit time is calculated as the ratio of the area under the fast component to the maximum height. Although this index is elegant, it did not prove to be diagnostically meaningful (97).
An alternative approach is based on multiple independent swallows (6 swallows are adequate for a reliable scintigraphic study). The individual swallows of a given esophageal scintigraphy study are normalized to their corresponding starting points, arranged consecutively, and then condensed in a sum image. Curves are generated by plotting the counting-rate columns assembled in each image. The following indices have been suggested (75,84,98):
Transit time: lag time from the starting point until activity falls to ≤10% of peak activity;
Mean transit time: (∑cts)/ctsmax;
Mean time: (∑cts(t)x t)/∑cts (t);
Esophageal emptying (EE) at 10 s after Tmax as fraction of peak activity: EET max+10 s; and
Esophageal emptying at 12 s after swallow as fraction of peak activity: EE12 s.
Mean transit times and mean times do not reflect true values, since the esophageal time–activity curves never actually drop to zero. Calculation of esophageal emptying should take into account residual activity after each swallow; the following formula attempts to correct for this residual background activity (usually expressed as percentages): esophageal emptying = (ctsmax – cts(sec))/(ctsmax – ctsmra), where ctsmra is the mean residual activity calculated on the first 5 swallows. However, this procedure overcorrects for background, sometimes yielding emptying rates > 100%. Tatsch demonstrated a high discriminating capacity for EE12 s (95% sensitivity, 96% specificity), followed by mean time, by EET max+10 s, and lastly by transit time (similar specificities but lower sensitivity) (79,84).
Quantitative analysis of esophageal scintigraphy can also be performed with the time–activity curves obtained separately on the 3 ROIs: upper, middle, and lower third of the esophagus. In this case, one should keep in mind the delay in clearance at the distal third that is due to the time lag required for relaxation of the LES (76). This procedure can constitute a second-line approach reserved for patients in whom cine-mode visual analysis or condensed-dynamic-image analysis has detected abnormalities in the overall esophagus, so that the specific abnormal segments can be identified.
Regional-transit-time topography has recently been developed. The method, which is based on visualization of the esophageal bolus transit as profiles connecting pixels containing the same number of counts, produces a multicontour plot and calculates relative local transit times along the esophagus. The counting rate measured at a certain cross-section is inversely proportional to the velocity of flow and directly proportional to transit time. The relative local transit times so obtained concisely describe the local kinetics of bolus transit along the esophagus, with a longitudinal resolution of about 25% of the esophagus (103,104).
General Clinical Application
The wide range in sensitivity and specificity reported for esophageal scintigraphy can at least in part be attributed to the different disorders evaluated. The potential clinical role of esophageal scintigraphy (including the oropharyngeal phase of swallowing) in patient management is better appreciated in light of the pathophysiologic changes underlying esophageal motility disorders (Figs. 4 and 5).
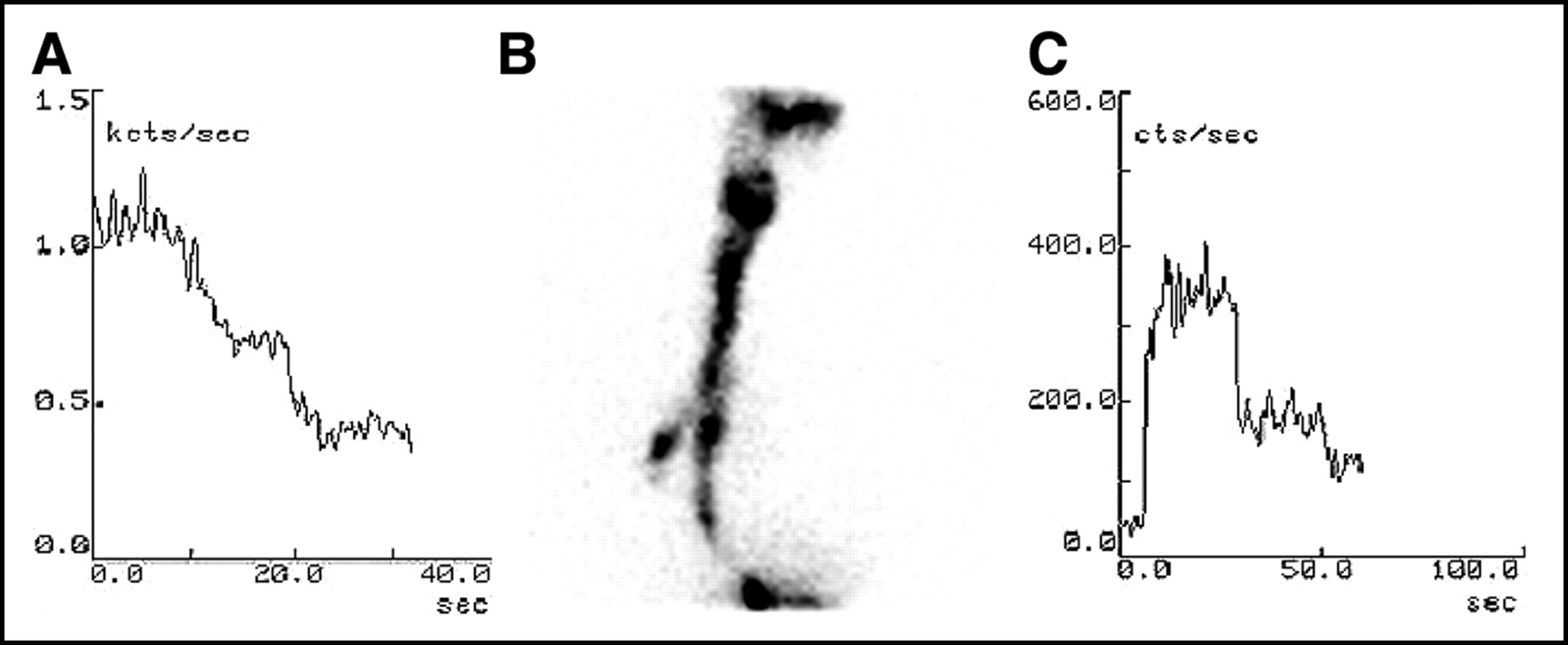
Examples of radionuclide swallow studies of patients with oropharyngeal dysphagia. (A) Time–activity curve for ROI drawn over oral region of patient with amyotrophic lateral sclerosis after patient swallowed liquid bolus (10 mL, upright, anterior view) shows significant retention and markedly delayed clearance of activity from mouth, with double swallow (piecemeal deglutition because entire bolus could not be swallowed at once). (B) Static image of patient with severe oropharyngeal dysphagia after total thyroidectomy (damage of upper left laryngeal nerve). Dynamic recording of the swallowing of a liquid bolus (10 mL, upright) was impossible because of wide movements due to coughing. Aspiration in trachea is obvious. (C) Semisolid bolus (10 mL, upright, anterior view) did not cause gross aspiration, thus permitting dynamic recording. Time–activity curve obtained for ROI drawn over pharyngeal region on completion of semisolid transit study shows markedly delayed, irregular, and incomplete clearance of radioactivity from pharynx.
Nutcracker Esophagus.
The term nutcracker esophagus was coined by Dalton et al. to describe the conditions under which patients with noncardiac chest pain or dysphagia exhibit peristaltic waves in the distal esophagus with mean amplitudes exceeding the normal values by more than 2 SDs (105). These high-amplitude waves may not interfere with esophageal clearance or strictly correlate with episodes of dysphagia or chest pain or may result in mild distal esophageal retention with reflux. Furthermore, symptoms may not respond to drugs that modulate the peristaltic wave pressure (106).
The clinical consequences of an isolated hypertensive LES remain unclear. Three groups of patients fall under the term isolated hypertensive LES: those with abnormally elevated resting LES, those with exaggerated contraction of LES after relaxation, and those with incomplete LES relaxation. Although the first 2 conditions can even be asymptomatic, incomplete LES relaxation usually interferes with esophageal emptying; this disorder is thus better termed atypical disorder of LES relaxation (with impaired esophageal clearance) rather than isolated hypertensive LES (105,107,108).
No definite diagnostic benefit of esophageal scintigraphy has been demonstrated in patients with normal peristalsis, even in the presence of nutcracker esophagus or isolated hypertensive LES (109,110). On the other hand, abnormal esophageal scintigraphic patterns, such as dysmotility or gastroesophageal reflux, were identified in 89% of patients with atypical chest pain, which in some cases was associated with nutcracker esophagus despite the fact that these patients did not complain of dysphagia (111).
Diffuse Esophageal Spasm.
Diffuse esophageal spasm is characterized by uncoordinated esophageal contractions that can interfere with esophageal clearance (Fig. 6). Different manometric criteria have been proposed for diagnosing this condition, including either the presence of spontaneous and repetitive contractions or the presence of high-amplitude or prolonged contractions. The key diagnostic criterion is the presence of simultaneous contractions induced by wet swallows. Besides the discrepancies in manometric criteria, diffuse esophageal spasm is an intermittent phenomenon that is evident manometrically in >10% (but ≪100%) of wet swallows (106,112). Therefore, in patients with this condition, esophageal scintigraphy should include multiple wet swallows, visual analysis of bolus dynamics (showing chaotic bolus movements), and definition of the time–activity curves (showing multiple peaks after a single swallow).
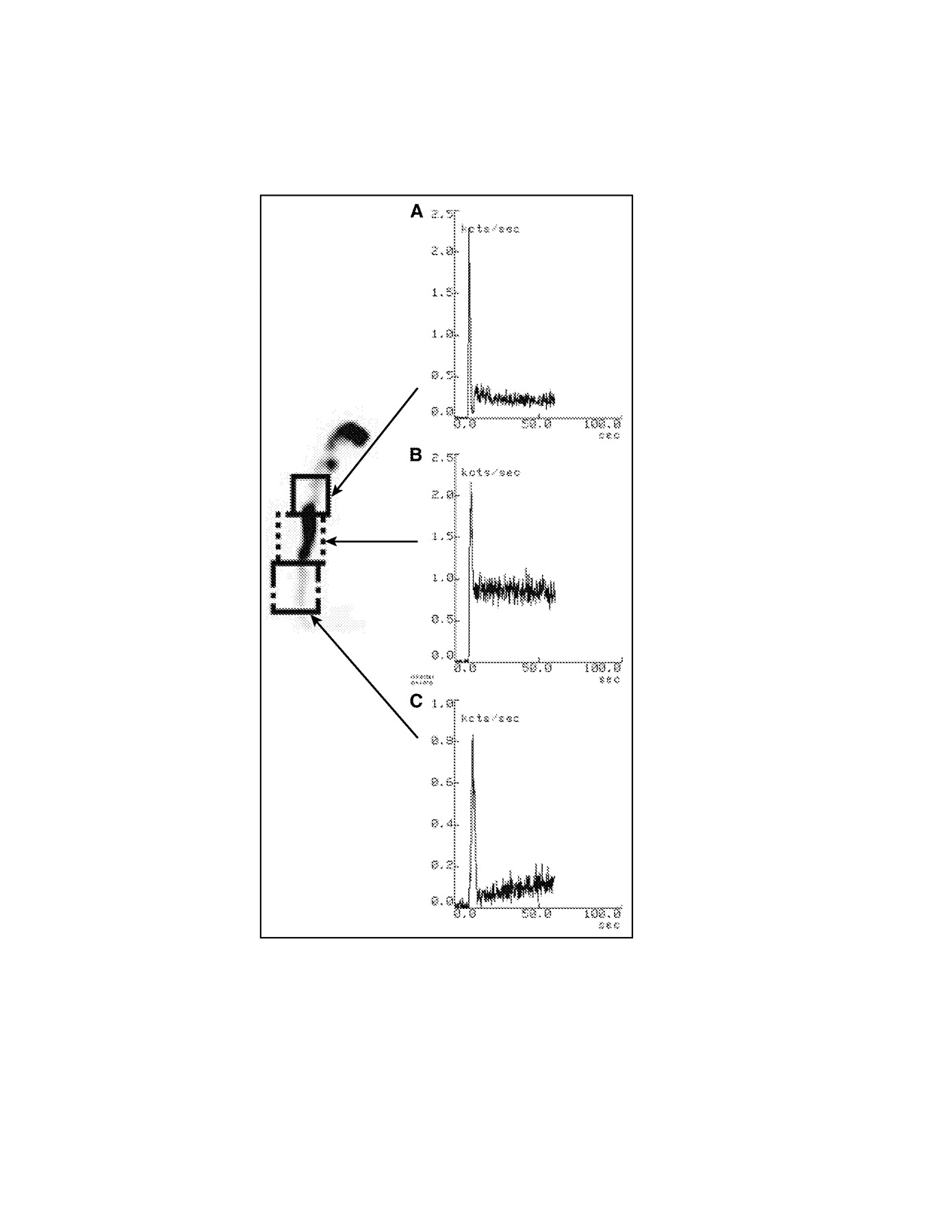
Radionuclide esophageal transit study (15-mL semisolid bolus, upright, anterior view) of patient with amyotrophic lateral sclerosis. Shown are time–activity curves for upper third (A), middle third (B), and lower third (C) of esophagus. Summed image at left defines the 3 esophageal ROIs. All 3 portions of the esophagus clear initially with a normal-appearing pattern, but there is marked retention of radioactivity, mainly in mid esophagus but also somewhat in proximal third, and slow subsequent passage of radioactive bolus to lower third. A similar scintigraphic pattern with delayed clearance of esophageal radioactivity is also seen in patients with achalasia or with scleroderma, but with retention in distal rather than middle portion of esophagus (Fig. 7).

Radionuclide esophageal transit study (10-mL liquid bolus, upright, anterior view) of patient with esophageal dysphagia. (A) One-second frames from dynamic recording show irregular movements of radioactive bolus up and down the esophagus. (B) Time–activity curve for ROI drawn over pharynx shows the normal efficiency of a single swallow without regurgitation. (C) Time–activity curve for ROI drawn over entire esophagus shows incoordinate clearance of radioactivity, the typical pattern for a patient with diffuse esophageal spasm. Review of the dynamic recording in cine mode excluded gastroesophageal reflux as an alternative cause of the irregular, multiple-peak pattern in the esophageal time–activity curve.
Achalasia.
Classic achalasia is caused by degeneration of neurons in the wall of the esophagus. These neurons are involved in the production of nitric oxide, which relaxes esophageal smooth muscle, therefore causing the basal LES pressure to rise (106,113–116). The result is impaired esophageal clearance and delayed transit times. Esophageal scintigraphy readily detects the delay in transit (Fig. 7), with a sensitivity close to 100% (74). Distal esophageal retention does not clear after the patient assumes an upright position or drinks a glass of water. Scintigraphic evaluation of esophageal clearance is widely accepted as the method of choice in the follow-up of patients with achalasia, for monitoring the efficacy of treatment (myotomy, pneumatic dilation, or botulinum toxin injections). To optimize sensitivity for this condition, the patient should be upright when studied and should swallow a bolus of unlabeled water after the radiolabeled swallow (117–122).

Radionuclide esophageal transit study (15-mL liquid bolus, supine, posterior view, 1 wet swallow followed 30 s later by 3 dry swallows at 15-s intervals) of a patient with achalasia. (A) Summed image of whole esophagus, with ROI. (B) Time–activity curve shows marked retention of radioactivity in the esophagus. Marked esophageal retention of radioactivity remained virtually unchanged after patient stood upright for some minutes. In contrast, esophageal scintigraphy of patients with scleroderma shows similar pattern of radioactivity retention, which, however, clears after they stand.
Scleroderma.
Fibrosis and vascular obliteration of the esophageal muscle and its innervation are the underlying causes of ineffective esophageal motility in patients with scleroderma. Esophageal scintigraphy can detect esophageal involvement in patients with asymptomatic disease, showing a typical pattern of retention of radioactivity in the lower esophagus, with clearing after the patient is upright or drinks a glass of water. As an indicator of dysmotility in both early and advanced disease, esophageal scintigraphy has a higher sensitivity than do manometry and barium swallows (123–127).
Table 3 compares the diagnostic performance of esophageal scintigraphy and videoesophagography (upper gastrointestinal series with barium swallows) in a variety of disorders of the esophagus. A general conclusion is that esophageal scintigraphy, which is easy to perform and yields quantitative parameters reflecting pathophysiologic processes, is especially suitable for serial studies to monitor the efficacy of medical or surgical treatment of various disorders (achalasia, gastroesophageal reflux, scleroderma, and hiatal hernia). Esophageal scintigraphy also plays an important role in the assessment of a patient’s subjective sensation of difficult swallowing, offering objective evidence of dysphagia and therefore stimulating further investigation (e.g., in psychiatric patients) (128), since no clinically significant motor disorder is likely to be missed (129).
Comparative Diagnostic Performance of Esophageal Scintigraphy vs. Videoesophagography in Patients with Dysphagia Caused by Various Esophageal Disorders
The reliability of transit scintigraphy for diagnosing esophageal cancer is too low to warrant its routine use for diagnosis (130,131). However, it is particularly useful for its ability to assess the effect of stricture and of dysmotility in a single test (73). Furthermore, transit scintigraphy has a considerable role after esophagectomy. Transit scintigraphy is ideal for assessing swallowing function and gastric emptying after replacement of the esophagus (e.g., with a portion of the stomach formed into a tube to reestablish a route between the pharynx and stomach) (132–136). In patients with inoperable esophageal cancer being treated only palliatively (such as through insertion of a stent to palliate dysphagia), an esophageal transit study can easily be performed to evaluate, noninvasively, restoration of near-normal patency (73).
Application to Pediatric GERD
Regurgitation and vomiting are common symptoms in infants with GERD, probably because of the limited capacity of the esophagus in this age group. In infants, it is difficult to discriminate pathologic from physiologic reflux. If the event is within physiologic levels, the infant thrives well and usually responds to simple measures such as nursing in an upright position or thickening of the food.
Most infants with severe reflux have symptoms by the age of 2 mo; the condition usually has a benign course, and about 60% of these babies are free of symptoms by the age of 18 mo. However, about 30% have persistent symptoms until approximately 4 y of age, 5% develop esophageal strictures, and another 5% die if they do not receive adequate treatment.
Clinical presentation of severe gastroesophageal reflux in children includes regurgitation or vomiting and failure to thrive. The spectrum of complications includes recurrent infections due to aspiration, asthma, apnea, cough, and stridor (137,138), along with the sequelae of esophagitis, including anemia, esophageal stricture, esophageal dysmotility (139), Sandifer’s syndrome, and even sudden infant death. Primary respiratory disorders may predispose to gastroesophageal reflux as a result of increased intraabdominal pressure caused by coughing. Contrary to common beliefs, crying does not exacerbate gastroesophageal reflux (140).
Most conventional tests for diagnosing gastroesophageal reflux in adults are not suitable in infants and children because of the radiation dose or because they require substantial cooperation from the patient (141). In particular, a barium upper-gastrointestinal series (with either intermittent imaging or cineradiography) uses a nonphysiologic test meal and requires provocative measures such as abdominal compression. Other diagnostic tests are more or less invasive, such as the acid infusion test (during which the patient is asked to communicate symptoms), intraluminal pH monitoring, esophageal manometry, upper digestive endoscopy, and tracheal aspiration (searching for lipid-laden macrophages to confirm aspiration of milk) (142).
The radionuclide method that has been adapted for use in infants and children (143) is performed at the time of scheduled feeding. 99mTc-Sulfur colloid (3.7–18.5 MBq [100–500 μCi]) mixed with milk or formula is used to label the liquid meal at a concentration of <1.85 MBq/mL (<50 μCi/mL). About half the regular meal is labeled, leaving the remainder unlabeled for completing the feeding study. If possible, the scintigraphic study includes the initial swallowing phase and esophageal transit. After the radiolabeled half of the meal has been given, the remaining, unlabeled, portion is given to wash radioactivity from the mouth, pharynx, and esophagus. The baby is then burped and placed supine for imaging of the chest and gastric area (reflux in infants is more likely to occur in the supine than in the prone position) (144). According to age and cooperation, the child can be positioned either lying on the imaging table or lying on the γ-camera head. A high-sensitivity collimator should be used to maximize radioactive counts, because the activity during an episode of reflux can be low or in a small volume.
Sequential images should be recorded continuously for about 5–10 s per image for at least 60 min, since about 25% of reflux episodes can be missed when limiting the acquisition to 30 min. Although dynamic acquisition at 20, 30, or even 60 s per frame (64 × 64 matrix) is usually adequate to identify gastroesophageal reflux, using shorter framing (e.g., 5 s per frame) can help in detecting brief reflux episodes and in evaluating clearance of reflux from the esophagus. At the end of dynamic acquisition, 5-min static images of the anterior and posterior lung fields are obtained, taking care to exclude the high gastric radioactivity. An additional procedure normally applied only to adults is to progressively increase abdominal pressure, as is done during a conventional barium radiography study. If aspiration is suspected, static imaging should be repeated at about 2 and 24 h.
For data analysis, ROIs are manually defined over the lower, middle, and upper esophagus and the oropharynx to generate time–activity curves, in which reflux episodes are characterized as sharp spikes. The dynamic acquisition should be reviewed in the cine mode to identify movements of the body, which can simulate reflux spikes in the time–activity curve.
Gastroesophageal reflux can be quantitated using different indices, which usually consider the volume of each episode, the frequency of the episodes, and the rate of reflux clearance from the esophagus. A simple approach is to express esophageal activity (either in selected frames from dynamic recording or in the static images) as a fraction of gastric activity (145). This approach clearly discriminates adult patients with gastroesophageal reflux from those without reflux (11.7% ± 1.8% vs. 2.7% ± 0.3%). When the mean value of esophageal activity was expressed as a fraction of initial gastric activity, patients with peptic esophagitis had significantly different values from those of controls (3.66% ± 0.81% vs. 0.66% ± 0.12%) (146). One can also calculate an overall reflux index based on the ratio of summed activities in each episode to gastric activity over the entire 60 min of the dynamic study (recorded at 20 s per frame) (147). If higher than 5%, this index denotes the presence of reflux.
The sensitivity of scintigraphy in detecting gastroesophageal reflux has been reported to be 75%–100%, depending on the protocol used (148). These values are consistently higher than those of conventional barium studies or manometry.
GASTRIC-EMPTYING SCINTIGRAPHY
Since its introduction by Griffith et al. in 1966 (149), gastric scintigraphy has evolved to include an evaluation of compartmental or antral motility, and more recently to SPECT to evaluate postprandial gastric accommodation.
As a physiologic, quantitative, noninvasive test, gastric-emptying scintigraphy is well suited for evaluating patients before and after medical or surgical treatment. This procedure is now widely considered the gold standard for evaluating gastric emptying.
Scintigraphy Procedure
Patients fast for at least 8 h before a gastric-emptying study. In addition, it is preferable to study women during the first 10 d of the menstrual cycle, to avoid possible hormonal effects on gastrointestinal motility. Any medication that potentially interferes with gastric motility (narcotic analgesics, anticholinergics, antidepressants, calcium channel blockers, gastric acid suppressants, aluminum-containing antacids, or somatostatin) is discontinued for an appropriate period (depending on specific pharmacokinetics), unless the scintigraphic test is performed specifically to assess the effect of such drugs on gastric motility. Tobacco and alcohol is also withheld for at least 24 h.
The first radiopharmaceutical described for gastric-emptying studies was chicken liver labeled by injecting sulfur colloid into the chicken. The liver was harvested, cooked, and administered to the patient. An advantage of this approach was the stability of the label. However, this procedure is not practical for routine use (150). A more convenient alternative is to mix 11–18 MBq (300–500 μCi) of 99mTc-sulfur colloid with eggs or a fat-free egg substitute (EggBeaters; ConAgra Foods, Inc.) to obtain a stable label for the solid phase (Table 4) (151). Besides the radiolabeled component, the test meal typically contains other unlabeled products because a caloric content of at least 200–300 kcal is needed for complete activation of digestive functions (152). In a multicenter study, a standardized, low-fat meal showed excellent reproducibility for gastric-emptying studies. The meal consisted of fat-free egg substitute (EggBeaters) served with 2 slices of bread, 30 g of strawberry jam, and 120 mL of water (150). Standardizing the content of the meal, the proportion of liquid and solid, the amount of fat, the number of calories, and the rate of consumption is important for establishing a reproducible response (153,154).
Stability of the Radiolabeled Solid In Vitro
111In-DTPA is usually used for liquid-phase studies, as it is chemically inert and does not bind to the solid phase of the meal, thus allowing simultaneous assessment of both solid and liquid emptying.
The radiolabeled meal is ingested within 10 min, under standardized environmental conditions (ambient noise, ambient light, and patient comfort). If any portion of the meal is not eaten, the uneaten amount is recorded.
Imaging can be performed while the patient is either standing, sitting, or supine, provided the position does not change during the study. Because movement of solids from the posteriorly located fundus to the more anteriorly located antrum results in a nonuniform attenuation of the gastric activity, anterior and posterior imaging with subsequent calculation of the geometric mean is suggested to correct for this attenuation nonuniformity; alternatively, a single left anterior oblique view can be used (155–159). Images are acquired in at least a 64 × 64 pixel matrix. Continuous data recording at a framing rate of 30–60 s per image for at least 90 min is generally recommended (160) (up to 2–3 h for larger-volume meals or meals with a higher calorie, fat, carbohydrate, or protein content). Alternatively, data recorded at discrete 15-min intervals (or even at 0, 60, 120, and 180 min after meal ingestion) have been shown to provide reliable gastric-emptying data. However, with this approach no information is available on the lag phase, and rapid gastric emptying (dumping) may not be fully characterized (32,161). Images recorded at 4 h may be necessary to characterize delayed gastric emptying in cases with borderline 2-h emptying (162).
The evaluation of indigestible solids (fibers or pellets) requires prolonged patient observation and provides information on the interdigestive period rather than postprandial motility (32).
Data Analysis and Quantitative Parameters
After the set of geometric mean images has been created, the full study is initially reviewed in cine mode to detect patient motion. After the cine review, it is helpful to add the images from the serial acquisition to define the borders of the stomach and the adjacent loops of bowel. ROIs are drawn around the gastric area, adjacent esophagus, duodenum, and jejunum. The curves are corrected for radioactive decay.
The percentage of gastric retention at a specific time point (usually 2, 3, or even 4 h) is calculated with respect to the immediate postingestion value at the zero time point. Because this parameter does not have a normal, gaussian-type distribution, the median and 90th or 95th percentile, rather than the mean and SD, are used to define normal values (32).
When continuous imaging is recorded, half-emptying time (T50) is determined as the time it takes to reach half the peak counts, whereas when static, discrete-interval images are acquired, the data points should first be analyzed by nonlinear least-squares fit. Because solid gastric emptying follows a sigmoidal rather than a simple exponential curve, at least 2 parameters are required for an optimal description. At least 2 computational procedures have proven capable of adequately describing the pattern of biphasic solid gastric emptying: the Elashoff power exponential function, y(t) = (e–kt)β (163), and a modified power exponential function, y(t) = (1 − [1 − ekt]β) (25), where y(t) is the gastric retained activity at time (t), k is the gastric-emptying rate, and β is the intercept on the y-axis back-extrapolated from the terminal portion of the curve.
When the Elashoff function is applied, T50 = (ln 21/β)/k, whereas when the modified power exponential function is applied, T50 = −ln ([1 − 0.5]1/β)/k.
The lag phase represents the time required for transfer of solid food from the fundus to the antrum and then for the antrum to grind it into small particles (suspended in the gastric fluid) that can begin to empty into the duodenum (164). Various methods have been proposed for evaluating this parameter. With continuous imaging, it is relatively easy to visually define the transition point in the gastric time–activity curve: the point of first appearance of duodenal activity or the time of maximal antral filling. When data are acquired as serial static images, the lag phase can arbitrarily be calculated as a given percentage of drop (5%–10%) from peak counts; however, this approach is highly dependent on the slope of the second phase (165). In mathematic terms, the lag time corresponds to the inflection point of the gastric time–activity curve, where the second derivative equals zero. When the Elashoff function is applied, lag time = ([β − 1]/β)1/β/k, whereas when the modified power exponential function is applied, lag time = β/k.
The lag phase calculated by the modified power-exponential function correlates poorly with the data derived by other methods, and the accuracy of such an estimate is greatly limited by the rate of temporal sampling. It has therefore been suggested that the lag phase calculated by this method possibly represents a more complex phenomenon than just emptying of solid food into the duodenum (163).
Dynamic Antral Scintigraphy
Although manometry is the most accurate method for assessing gastric motor function, this invasive procedure is not well accepted by patients and is not widely available (166). Real-time ultrasound evaluation of gastric motor function is often hampered by poor image quality because of echogenic food particles (167). Simultaneous scintigraphic evaluation of both gastric motility and gastric emptying optimizes the characterization of gastric function with minimal additional cost, time, and technical effort.
Movements of the stomach wall induce changes in the distribution of radioactive food within the stomach. Therefore, dynamic scintigraphy as performed for a gastric-emptying study can evaluate gastric motility as well. Because antral hypomotility (reduction of phasic contractions in the distal stomach) has been reported for a variety of dyspeptic syndromes, almost all studies have evaluated only antral motility (168–175). The most common procedure is to add a short, high-definition dynamic acquisition (1–2 s per frame for 4–5 min) at the end of a standard gastric-emptying study, performed either with dynamic imaging or with serial static imaging. Data analysis is performed after attenuation correction, to generate time–activity curves for ROIs defined on the proximal, middle, and distal antral regions. Further data processing includes elimination of artifacts due to patient movement or to translational movement of the stomach (performed by baseline restoration of raw data using a polynomial fit) and elimination of background noise (performed by an autocorrelation function). A refined Fourier transform is then performed on antral time–activity curves to determine the amplitude and frequency of antral contractions.
Consistent with manometric (176), real-time ultrasonographic, and electrogastrographic estimates (177), in several scintigraphic studies the frequency of antral contractions has been found to be about 3 per minute (127,167–173). This normal frequency does not seem to change significantly in patients with diabetes, gastritis, functional dyspepsia, progressive systemic sclerosis, or pyloric stenosis, either after administration of gastric acid suppressants or after gastric surgery. In contrast, the amplitude of antral contractions seems to discriminate various patient groups. In functional dyspepsia, paradoxically increased amplitude has been reported, possibly explained by predominantly inefficient (nonexpulsive) antral contractility or by pyloric dysmotility (170), whereas decreased amplitude has been observed in diabetic patients (168) and in patients who previously underwent Billroth type I or type II gastrectomy or truncal vagotomy (178).
Unfortunately, variability in the definition of the antral ROIs, as well as in the normalization and filtering steps, hampers the reproducibility of measurement of antral function. Two methods avoiding the autocorrelation function have therefore been proposed to improve reproducibility. Both involve a postsynchronization method using either a single distal antral ROI (179) or Fourier analysis of condensed images of the whole stomach (180).
Gastric SPECT
Dyspeptic patients frequently have defective gastric accommodation contributing to postprandial symptoms such as early satiety, distension, and nausea. This condition has been reported in functional dyspepsia, postfundoplication dyspepsia, postvagotomy gastric surgery, and neuropathic diabetic gastroparesis (181–186). Although proximal gastric accommodation can be measured by a barostatic balloon, and real-time ultrasonography can measure antral accommodation, neither of these 2 methods can evaluate whole-stomach accommodation. SPECT has been used to measure gastric accommodation in response to a meal, based on the well-known ability of both the parietal (oxyntic) and the nonparietal (mucous) gastric cells to take up and excrete 99mTc-pertechnetate (187).
The procedure is as follows: A 370–740 MBq (10–20 mCi) dose of 99mTc-pertechnetate is injected intravenously after an overnight fast. Dynamic tomographic acquisition is performed starting 10 min after injection, using a multiorbit mode; 6° images are acquired in a 128 × 128 matrix at 3 s per step (total acquisition time, about 180 s). After 2 initial orbits have been recorded as baseline, the patient drinks the test meal while supine, with the aid of a straw. Immediately afterward, 7 additional orbits are acquired over about 21 min to evaluate gastric accommodation to the meal challenge.
A semiautomated segmentation algorithm is used to reconstruct the stomach. Total gastric volume is measured during fasting, during the 3- to 12-min postprandial period, and during the 12- to 21-min postprandial period. The procedure has recently been simplified by acquiring 3 complete 360° orbits every 10 min (6° steps, 64 × 64 matrix, 10 s per step) (188). Intra- and interobserver coefficients of variation in estimating fasting and postprandial gastric volumes are 8%–9% and 12%–13%, respectively. The greatest postprandial volume increase was in the proximal stomach (about 2- to 4-fold), with no significant difference between early (3–12 min) and late (12–21 min) volume changes.
The method has recently been validated by a phantom study using a balloon filled with 99mTc-DTPA, and changes in gastric volume measured in response to a meal proved to be as accurate as those derived by the barostat balloon technique, with no effects of age (at least in adults) and body mass index on the fasting or postprandial gastric volume ratio (189). Gastric SPECT has also demonstrated impaired accommodation in patients with idiopathic nonulcer dyspepsia and in patients after fundoplication (187,190,191).
Clinical Application
Gastric scintigraphy (Fig. 8) is generally indicated in several clinical conditions when morphologic investigations fail to reveal the cause of dyspepsia, such as postprandial nausea, vomiting, upper abdominal discomfort, early satiety and bloating, suspected gastroparesis, poor diabetic control, and severe reflux esophagitis unresponsive to medical treatment (46,158).

Examples of gastric-emptying curves (corrected for physical radioisotopic decay) obtained by sequential imaging at discrete intervals after ingestion of radiolabeled solid meal. (A) Results for healthy volunteer (in our institution, T1/2 values of gastric time–activity curves for healthy subjects range from 110 to 120 min). Curve is characterized by distinct lag phase lasting about 20–30 min before emptying begins. (B) Results for patient with gastroesophageal reflux; this curve shows virtually no lag phase and shows markedly delayed gastric emptying, as observed in an average 40% of these patients (236,237). On the basis of this finding, the surgical treatment chosen was fundoplication and pyloroplasty, instead of isolated fundoplication, which would have induced postoperative symptoms (e.g., bloating) with no obvious lag phase. (C) Gastric-emptying curve obtained for same patient after surgical treatment demonstrates slightly accelerated gastric emptying (due to pyloroplasty), with reappearance of a discernible lag phase.
The pathophysiologic basis of functional dyspepsia has variously been ascribed to delayed gastric emptying of solids (192,193), failure of fundic relaxation (184), visceral hypersensitivity (40), and Helicobacter pylori infection (194,195). Although more than 40% of patients with functional dyspepsia have delayed solid gastric emptying, whether such an abnormality explains the clinical symptoms remains controversial (190,196–199). However, some correlation has been found between delayed gastric emptying and relevant postprandial fullness or severe vomiting and with being female (191), the total symptom score being higher in those patients with delayed gastric emptying (200). In diabetic patients, independent predictors of delayed gastric emptying included abdominal bloating, the female sex, and high blood glucose levels and body mass index (201).
Another controversial issue concerns the effect of prokinetic drugs, inducing accelerated gastric emptying, on symptom relief. Surprisingly few studies have evaluated whether baseline gastric emptying is a predictor of the efficacy of these agents or whether accelerated gastric emptying after therapy is a predictor of symptom improvement (202). Helicobacter pylori infection in patients with nonulcer dyspepsia is usually not associated with delayed gastric emptying (203–205), although both gastric emptying and symptom scores have been reported to improve after Helicobacter pylori eradication (206).
Delayed gastric emptying, most likely due to autonomic neuropathy (resulting in a prolonged lag phase (168)), has been identified in 27%–58% of diabetic patients; however, hyperglycemia further delays gastric emptying, and delayed gastric emptying itself may contribute to poor glycemic control (207). Delayed gastric emptying is also associated with various systemic syndromes (Parkinson’s disease, amyloidosis, myotonic dystrophy, polymyositis, HIV infection, or cytomegalovirus infection) and with local conditions such as vagotomy without pyloroplasty, and gastroesophageal reflux (208–215).
As expected, accelerated gastric emptying is found after pyloroplasty or after surgical treatment of reflux (216–219).
Another clinical application of gastric scintigraphy is postsurgical evaluation of the gastroesophageal junction. Achalasia is the esophageal disorder whose treatment has been most substantially affected by the development of minimally invasive surgery—that is, a laparoscopic approach to Heller’s myotomy (220)—widely reported to yield favorable results in up to 90% of these patients (221–224). Because the support structures of the antireflux mechanism, such as the phrenoesophageal ligament and the LES, are sacrificed during laparoscopic dissection of the esophagus and myotomy, an antireflux procedure is also required (225–227). Residual dysphagia can be linked to persistent esophageal narrowing due to incomplete myotomy. Esophageal transit scintigraphy is well suited as an addition to esophageal manometry and 24-h pH monitoring for follow-up and monitoring of this complication.
The efficacy of medical therapy in patients with GERD seems to wane with time, and for many patients the dose of proton pump inhibitors needs to be readjusted to control symptom relapse. However, surgical therapy for GERD has seen dramatic changes over the last decade, making it much more accessible and less invasive than in the past (228). The goal of effective antireflux surgery is to restore the competency of the cardia. Incompetence of the gastroesophageal junction has a multifactorial etiology, including such abnormalities as transient relaxation of the LES (relaxation not associated with a swallow), primary hypotension of the LES, gastric-emptying abnormalities, and absence of a flap valve. The presence of hiatal hernia exacerbates reflux by impairing esophageal emptying and LES function. An ideal operation, thus, is one that addresses each of these aspects. The most effective way (shown to yield favorable results in about 90% of patients) to permanently restore the competency of the cardia is to create some form of plication over the esophagus just proximal to the cardioesophageal junction, according to the following principles. First, the wrap must be constructed over the esophagus, just proximal to the gastroesophageal junction, and must be fixed to the esophagus to remain in that position permanently. Second, the wrap must be constructed without tension using the fundus of the stomach and leaving enough space to accommodate a 42- to 50-French bougie inside the esophagus. Third, a total wrap, such as the total fundoplication described by Nissen, should measure about 2 cm in length in its anterior aspect. Fourth, the wrapped portion of the esophagus must lie below the diaphragm without tension. Finally, the diaphragmatic hiatus must be gently closed around the esophagus, above the wrap.
Esophageal transit scintigraphy and, above all, gastric-emptying scintigraphy are well suited for following up patients who undergo fundoplication because of GERD (Fig. 8) (229).
PROPOSED ALGORITHMS
Scintigraphic evaluation of the upper digestive tract with a transit study is simple, safe, quick, physiologic, and well accepted by patients. By quantitatively or semiquantitatively measuring serial changes or response to therapy, this technique noninvasively provides clinically relevant information on various motility disorders and can modify clinical management of patients. Nevertheless, there is a certain reluctance to rely on this set of procedures, although with some variance between esophageal transit scintigraphy (perhaps because of the paucity of information available on its reproducibility) (230) and gastric-emptying studies (widely recognized as the gold standard for this physiologic parameter). Thus, we can agree that transit scintigraphy, especially esophageal transit scintigraphy, is generally underused despite its recognized clinical value (73).
Here, we propose diagnostic and clinical algorithms for evaluating patients with some selected functional or motility disorders of the upper digestive tract. Although originally derived from published literature, these algorithms have been modified for this review on the basis of wide clinical experience and a consensus developed during extensive discussions with specialists in nuclear medicine and in medical and surgical gastroenterology.
Figure 9 shows a flowchart of a possible diagnostic algorithm for patients presenting with dysphagia of either oropharyngeal or esophageal origin. The left side of the figure concerns oropharyngeal dysphagia, whose evaluation is usually quite straightforward. In these patients, clinical evaluation is usually initiated by the otolaryngology specialist and must include careful neurologic assessment. Evaluation of the swallowing function with a barium transit study is usually the first imaging procedure, usefully completed with a radionuclide esophageal transit study that provides a more physiologic, quantitative assessment to better characterize the underlying disorder. After a specific diagnosis has been established and the best treatment chosen, esophageal transit scintigraphy is especially useful for monitoring the disease and its response to treatment.
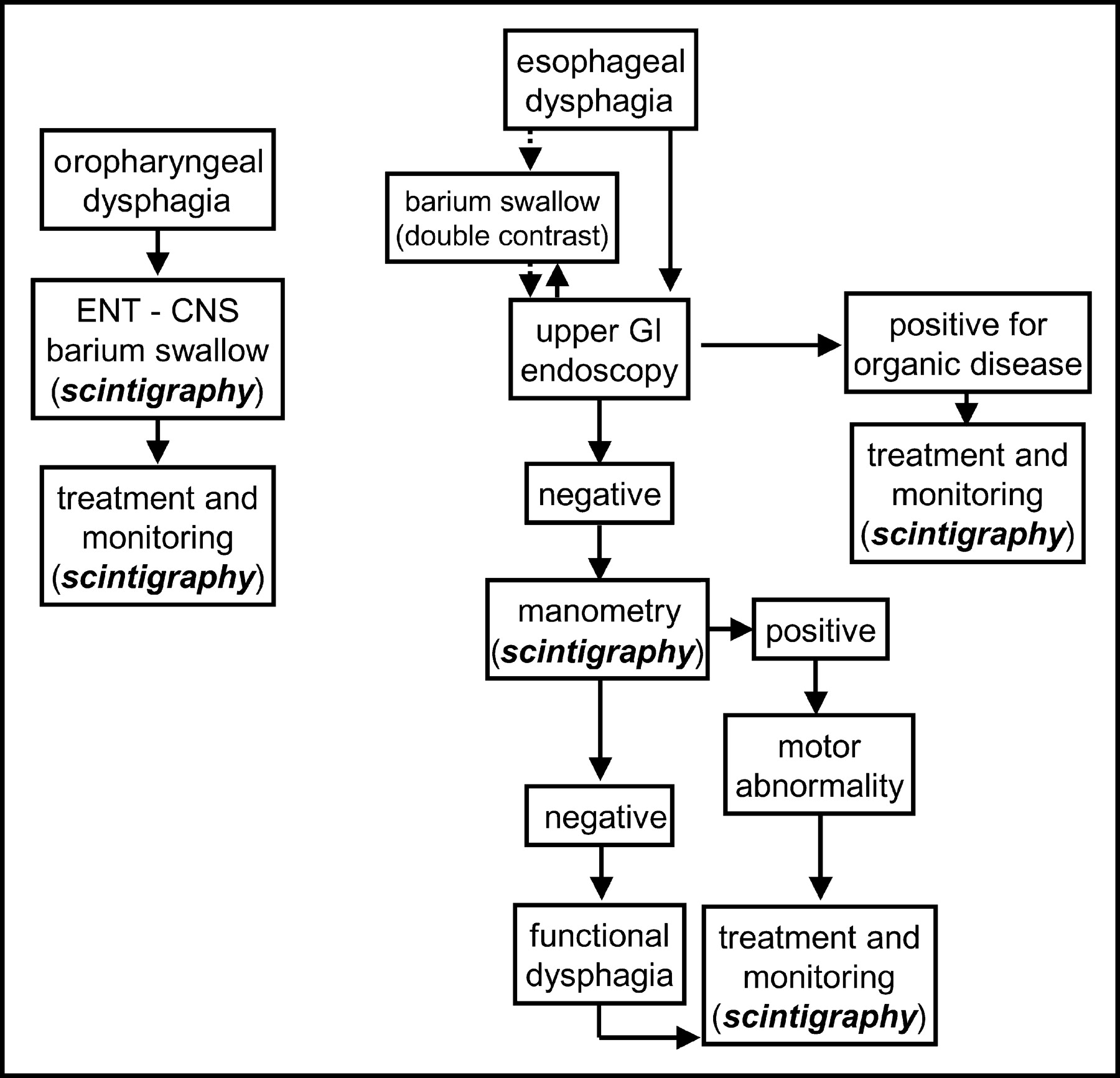
Proposed diagnostic–therapeutic algorithm for patients with dysphagia of either oropharyngeal or esophageal origin. Oropharyngeal dysphagia is defined as the occurrence of choking, coughing, and nasal regurgitation in association with the initiation of a swallow. Esophageal dysphagia is defined as a sensation of food stuck in the esophagus a few seconds after swallowing. Barium swallow for suspected oropharyngeal dysphagia is best performed as cineradiography. ENT - CNS = otolaryngologic and neurologic evaluation; GI = gastrointestinal.
The right side of Figure 9 concerns esophageal dysphagia. In these patients, whether upper gastrointestinal endoscopy (the most common occurrence, solid arrow) or a barium swallow (less frequent occurrence, dotted arrow) is performed first varies according to local logistics. When upper gastrointestinal endoscopy is performed first, a barium swallow study is generally performed anyway in a subsequent phase of the patient’s characterization. When upper gastrointestinal endoscopy reveals organic disease (e.g., esophageal stricture or tumor), treatment is usually surgical, with an ensuing certain role for transit esophageal scintigraphy as a simple, noninvasive test for assessing restoration of swallowing function. When endoscopy excludes organic disease, esophageal manometry is usually recognized as the gold standard for functional characterization of the swallowing disorder. Variously combined with the other nonradionuclide tests, transit esophageal scintigraphy is helpful for quantitative characterization of the functional disorder and especially for subsequent monitoring of the response to therapy (18).
As shown in Figure 10, the diagnostic work-up of patients with symptoms suggesting GERD (with the earlier, milder variant of nonerosive reflux disease) is particularly complex (231). In these patients, esophageal transit scintigraphy has a pivotal role in a relatively late phase of the clinical algorithm, as a means of stratifying patients for treatment or for full reevaluation after failure of medical therapy. In both instances, scintigraphy again provides useful information either for monitoring response to therapy (including surgical procedures) or for better characterizing the diagnosis.

Proposed diagnostic–therapeutic algorithm for patients with symptoms suggestive of GERD. Alarm symptoms are defined as pain, dysphagia, anemia, weight loss, fever, and hematemesis. Positive pH-metry is prolonged exposure of the esophagus to a pH of <4 for >5% of the total time. Negative pH-metry is exposure of the esophagus to a pH of <4 for <5% of the total time. A positive symptom index is ≥50% of the symptoms arising simultaneously with drops of esophageal pH to <4, even if extending over <5% of the total time; a negative symptom index is <50% of the same parameter. Full reevaluation is based on the entire set of diagnostic tests available, such as manometry, bilimetry, scintigraphy, upper gastrointestinal series, or multichannel impedance. GI = gastrointestinal; H2-blockers = histamine-2 receptor inhibiting/antagonist drugs; NERD = nonerosive reflux disease; PPI = proton pump inhibitors.
Esophageal transit scintigraphy has a pivotal role in determining whether patients with noncardiac chest pain have achalasia or other (spastic) motility disorders or have functional chest pain of presumed esophageal origin (Fig. 11) (229). These 2 classes of disease benefit from markedly different therapeutic approaches. Treatment of achalasia is based on administration of nitrates, endoscopic infiltration with botulinum toxin, endoscopic pneumatic dilation, or surgical (extramucosal) myotomy. Functional chest pain of presumed esophageal origin is treated with antidepressant drugs, psychotherapy, or behavioral therapy.

Proposed diagnostic–therapeutic algorithm for patients presenting with recurrent noncardiac chest pain. Positive pH-metry is prolonged exposure of the esophagus to a pH of <4 for >5% of the total time. Negative pH-metry is exposure of the esophagus to a pH of <4 for <5% of the total time. GI = gastrointestinal.
As shown in Fig. 12, the diagnostic and management approach to patients presenting with dyspeptic symptoms can also be quite complex (232,233). Gastric-emptying scintigraphy is important for diagnosing functional dyspepsia in patients with negative results on upper gastrointestinal endoscopy, either after failure of therapy for ulcer-like symptoms or in the presence of certain conditions increasing the risk for organic disease of the stomach.
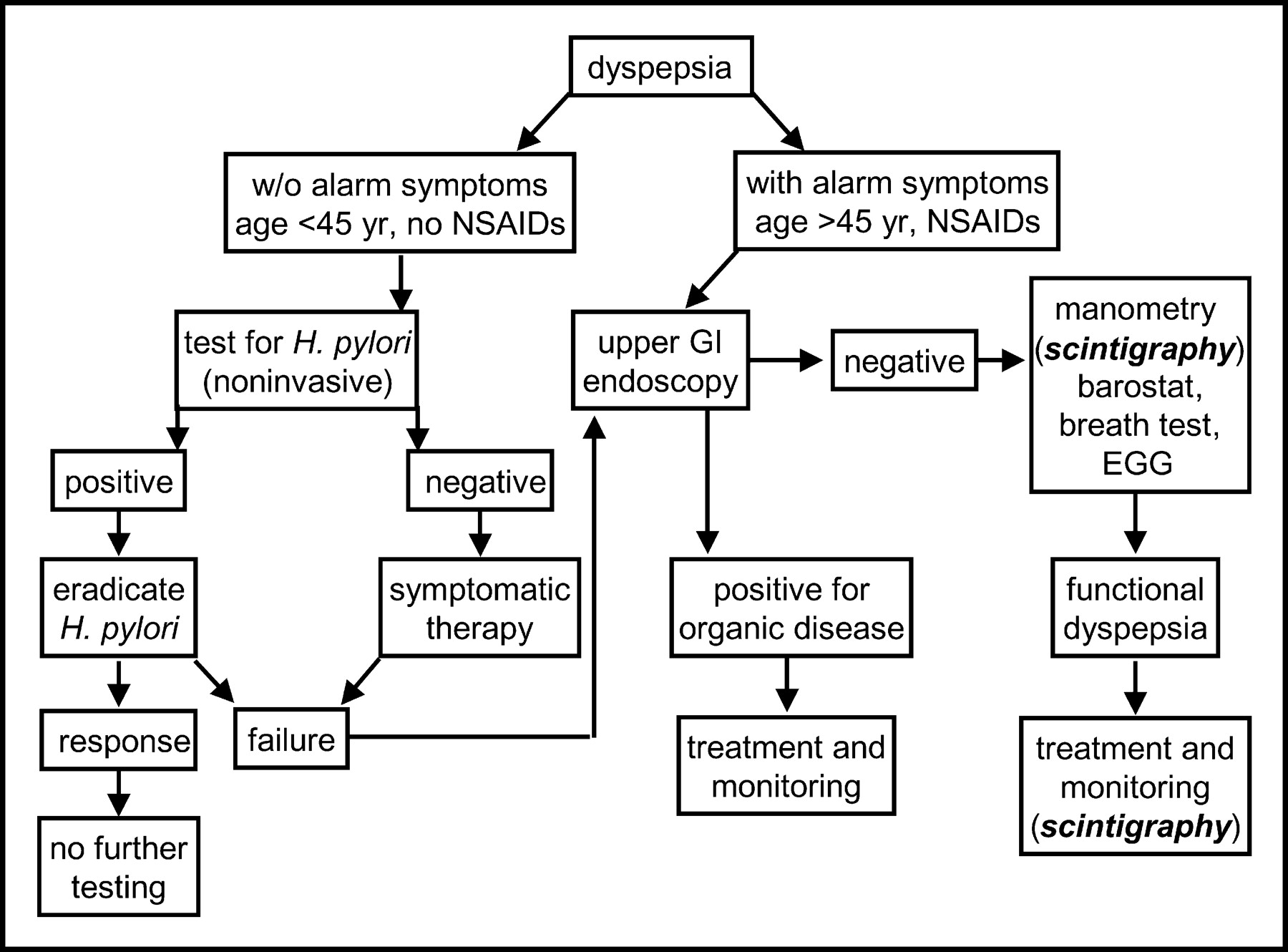
Proposed diagnostic–therapeutic algorithm for patients presenting with dyspeptic symptoms (epigastric pain or upper-abdominal discomfort). Alarm symptoms are defined as pain, dysphagia, anemia, weight loss, fever, and hematemesis. The breath test is a test for gastric emptying. Organic disease is defined as the presence of tumor or other gross anatomic abnormality. EGG = electrogastrogram; GI = gastrointestinal; NSAIDs = nonsteroidal antiinflammatory drugs.
Footnotes
Received Apr. 5, 2004; accepted Apr. 5, 2004.
For correspondence or reprints contact: Giuliano Mariani, MD, Regional Center of Nuclear Medicine, University of Pisa Medical School, Via Roma 67, I-56126 Pisa, Italy.
E-mail: g.mariani{at}med.unipi.it
*NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH JUNE 2005.
REFERENCES
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
In this issue





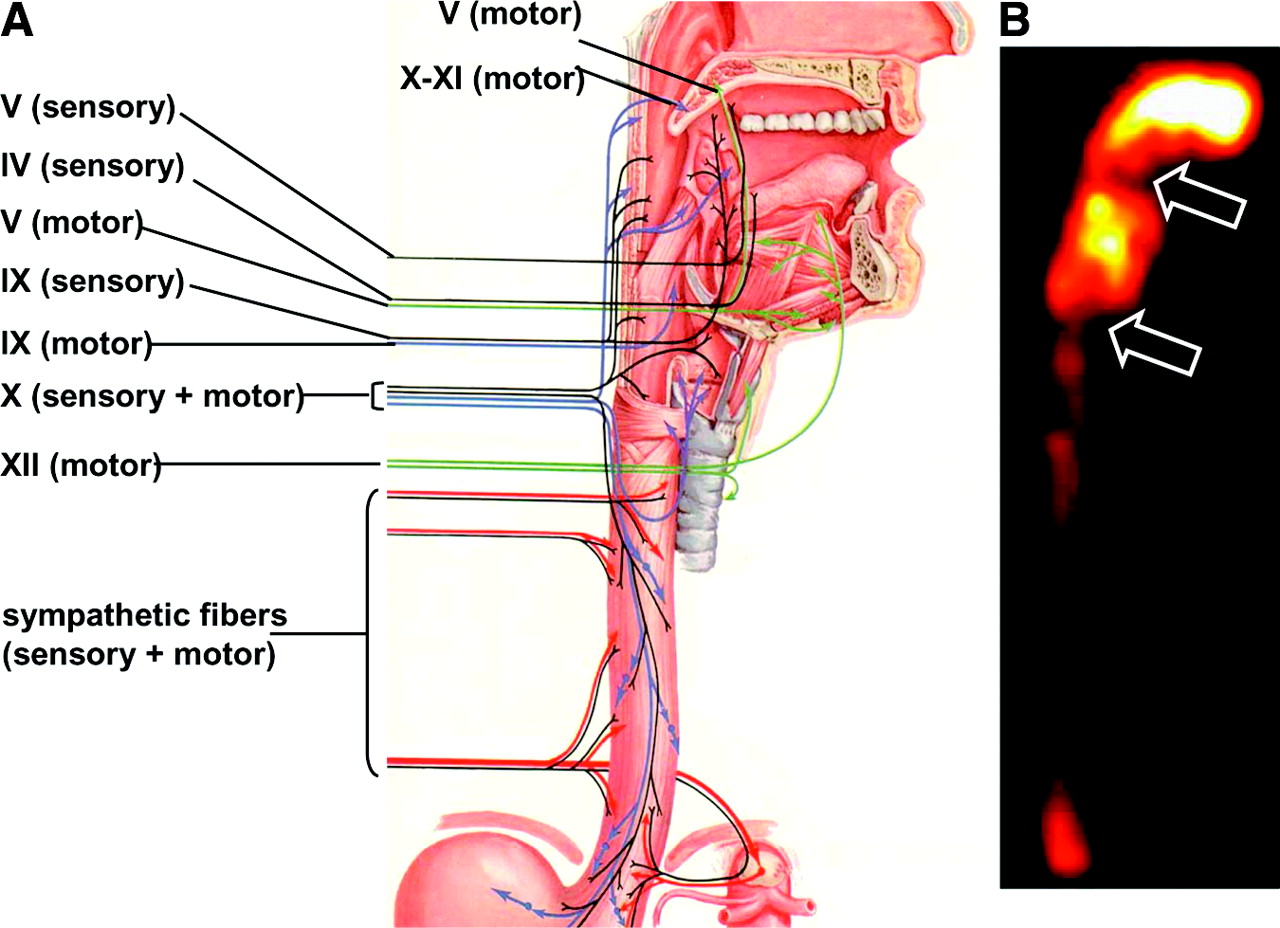{kind=link}
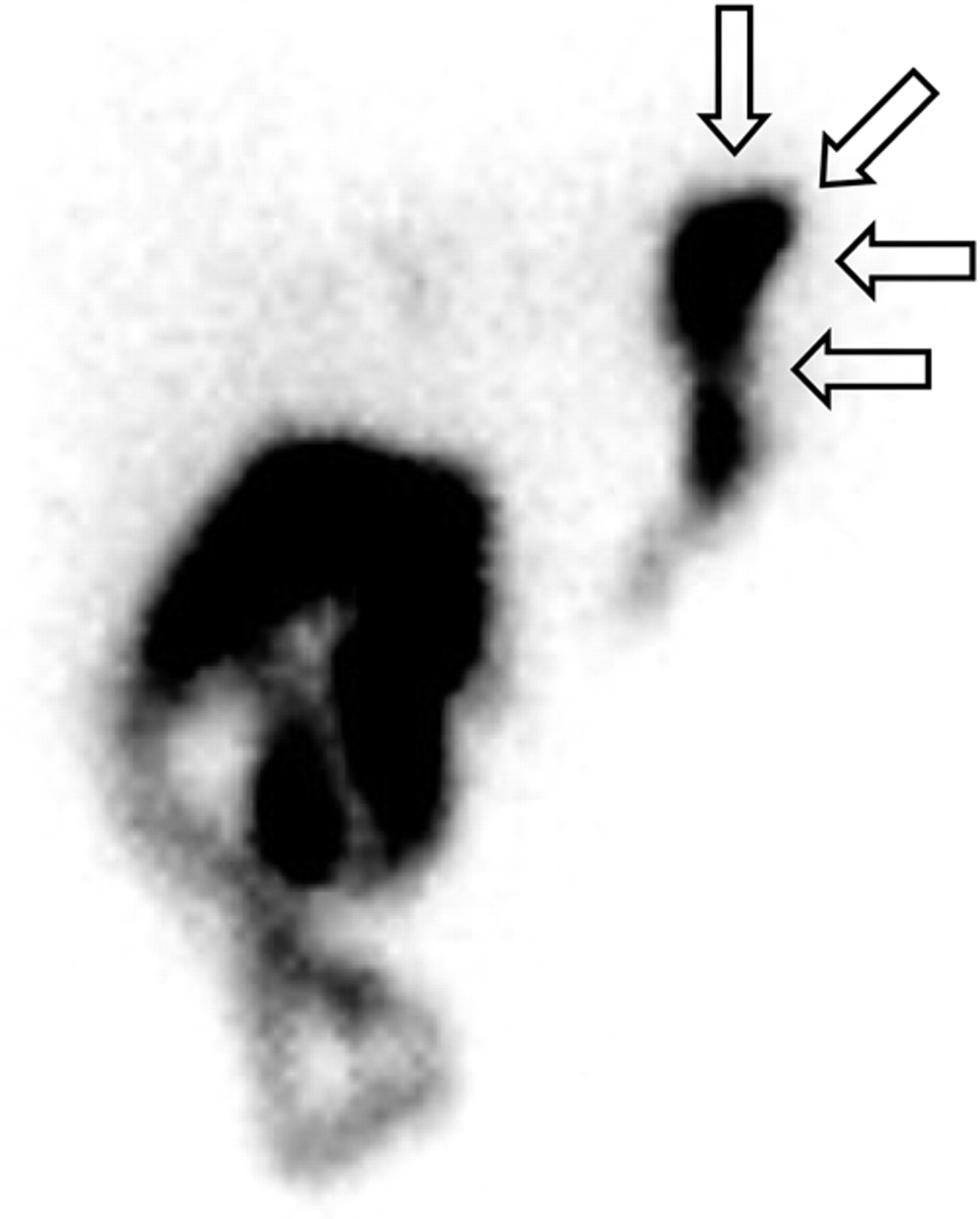{kind=link}
{kind=link}
{kind=link}
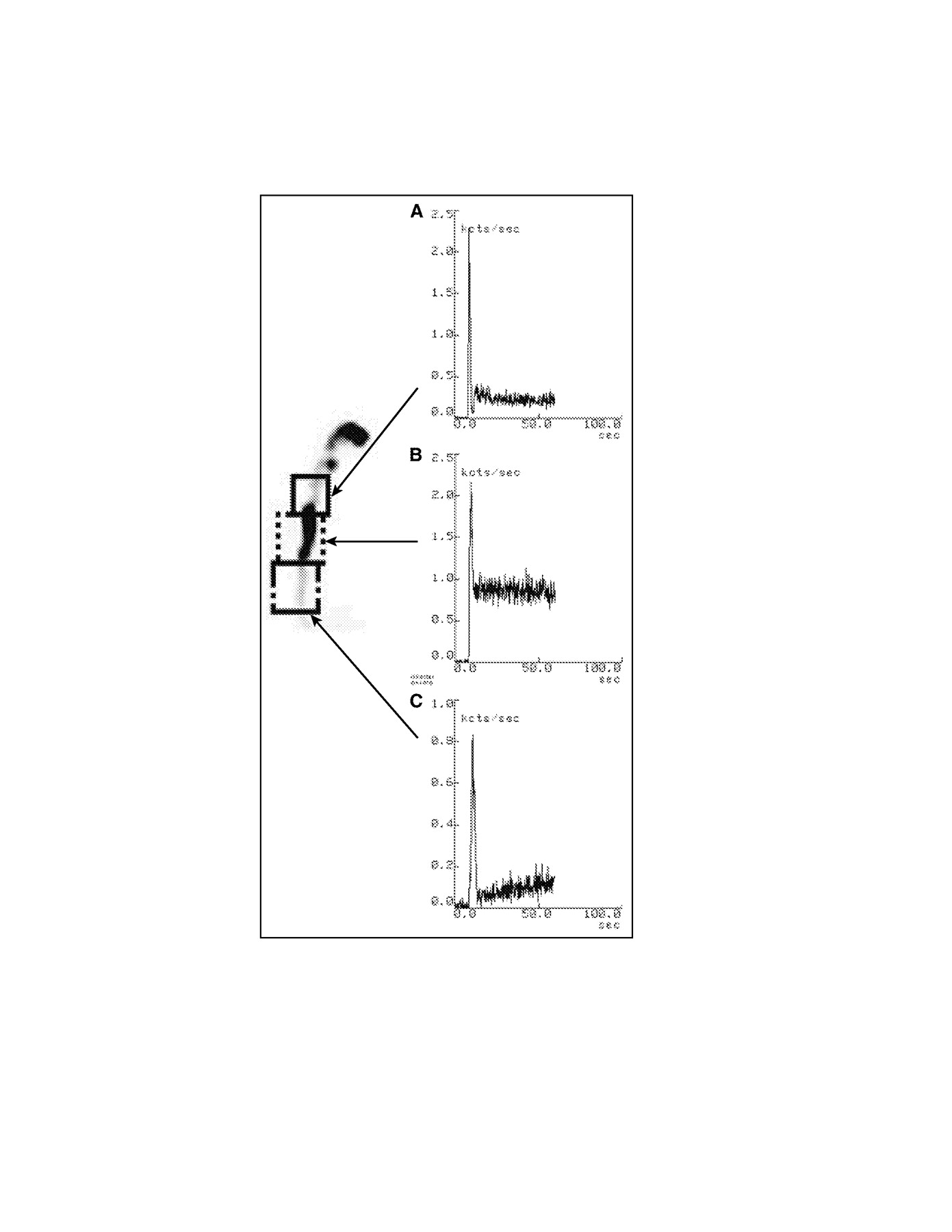{kind=link}
{kind=link}
{kind=link}
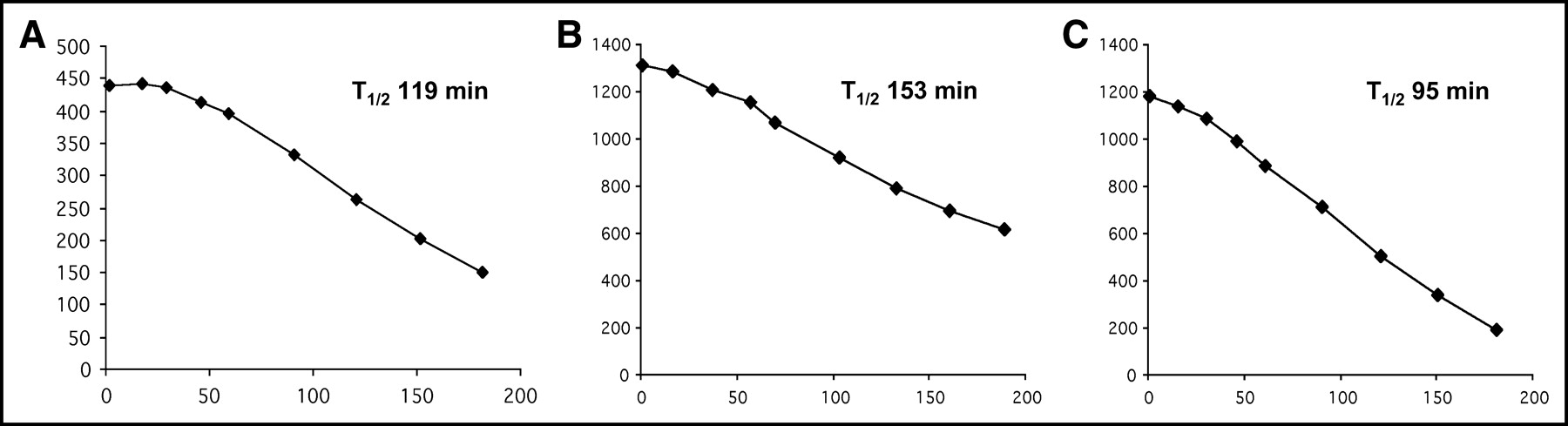{kind=link}
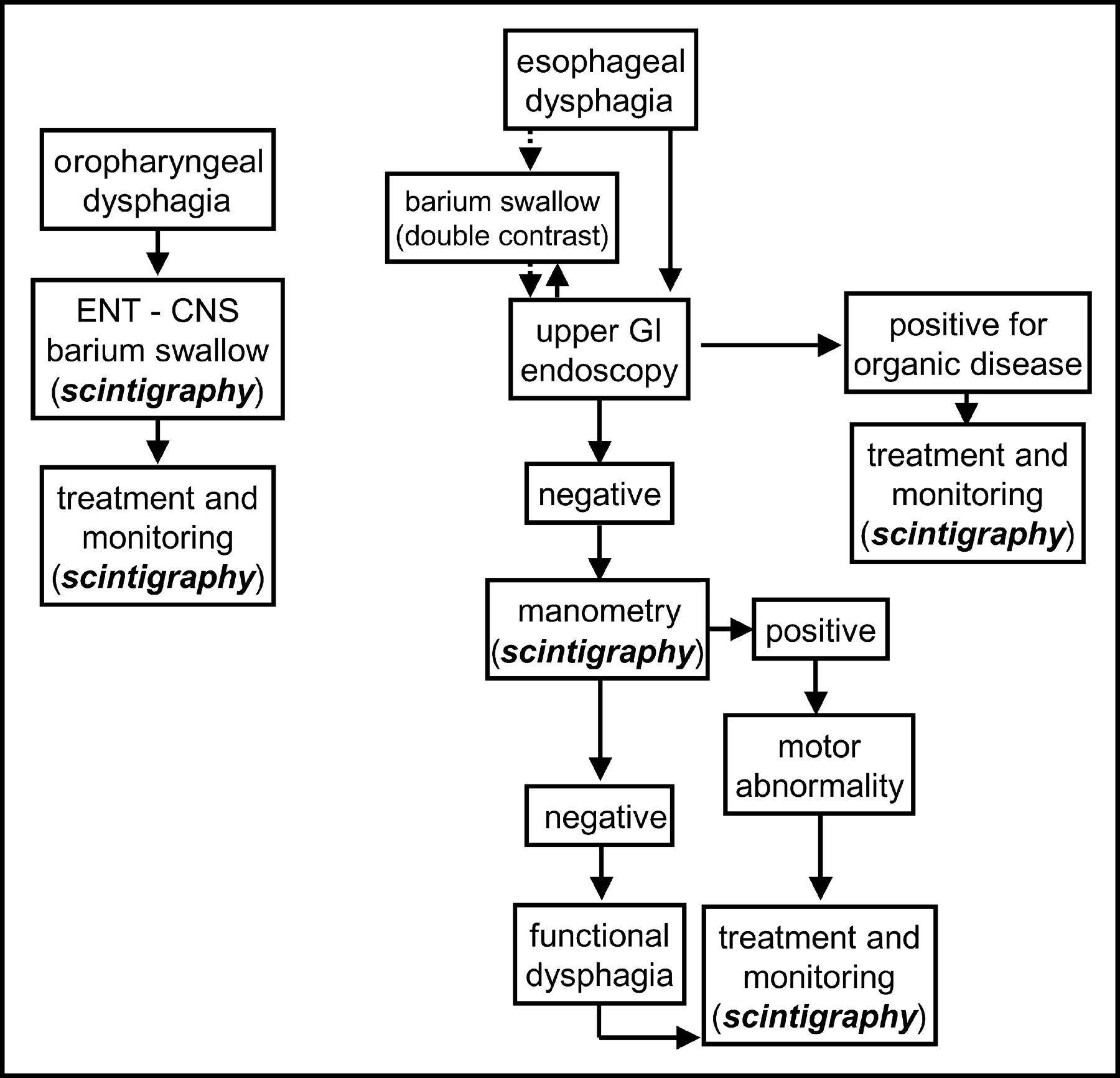{kind=link}
{kind=link}
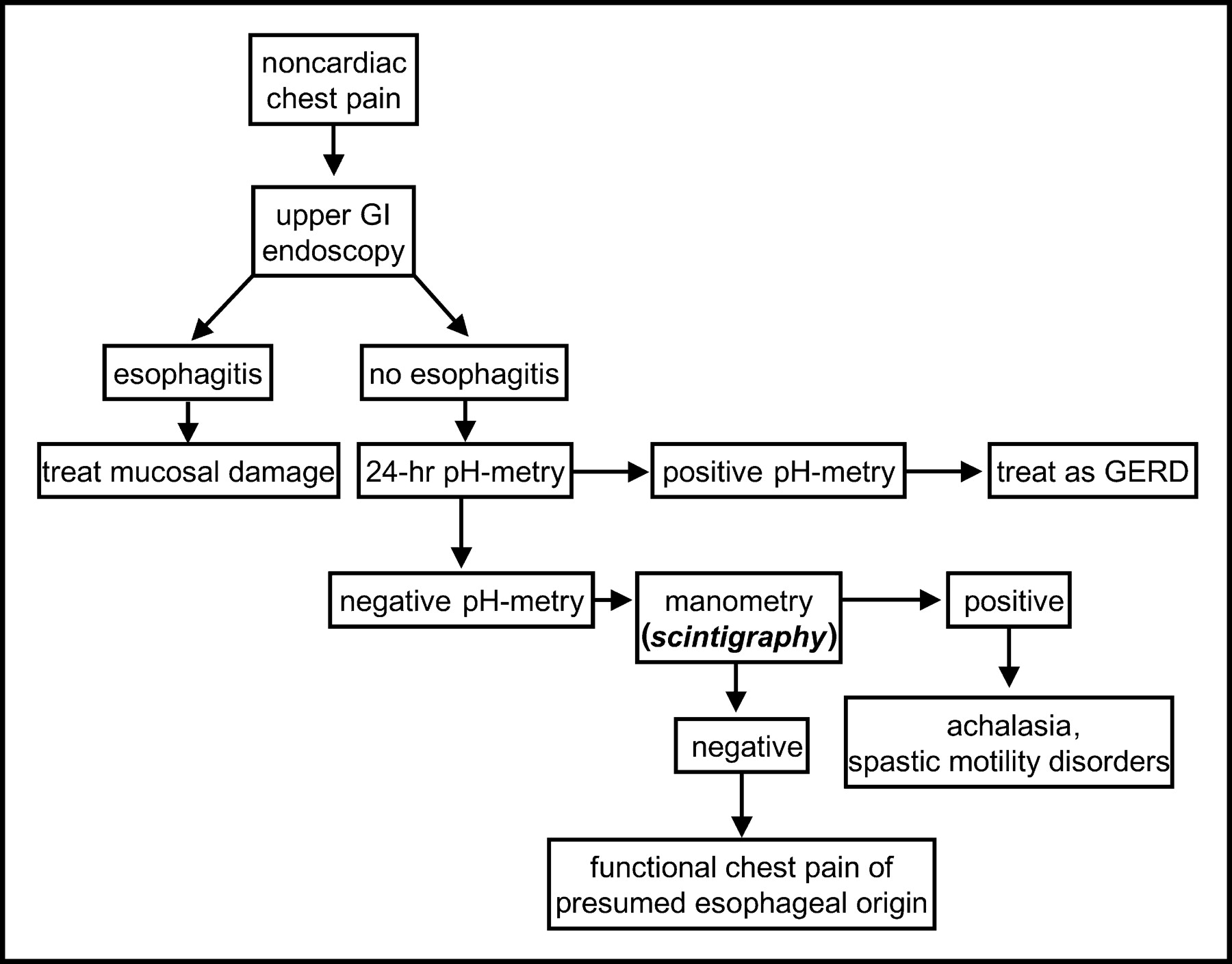{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Gastric Emptying Solid-Meal Content and Misinformation on Social Media Platforms
- Gastric Emptying Scintigraphy
- Compliance with Gastric-Emptying Scintigraphy Guidelines: An Analysis of the Intersocietal Accreditation Commission Database
- Comprehensive Radionuclide Esophagogastrointestinal Transit Study: Methodology, Reference Values, and Initial Clinical Experience
- Imaging of non-malignant disease of the oesophagus and stomach
- The Added Diagnostic Value of Liquid Gastric Emptying Compared with Solid Emptying Alone
- Oesophageal dilatation on high-resolution computed tomography scan of the lungs as a sign of scleroderma
- Radionuclide Evaluation of the Lower Gastrointestinal Tract
- Oesophageal dysmotility in systemic sclerosis: comparison of HRCT and scintigraphy