


Abstract
This was a study to evaluate the posterior cingulate sign in differential diagnosis between Alzheimer’s and frontotemporal disease. The impending availability of effective treatment for Alzheimer’s disease makes this differential diagnosis important. Methods: Images of 20 patients with clinically confirmed or autopsy-proven (10 patients) Alzheimer’s disease and 20 patients with clinically confirmed or autopsy-proven (7 patients) frontotemporal disease were compared with the consolidated images of 20 elderly healthy control subjects. The 99mTc-hexamethylpropyleneamine oxime SPECT data on brain blood flow from each patient were compared with the consolidated control image using statistical parametric mapping. Results: Sixteen of 20 patients with Alzheimer’s disease showed the posterior cingulate sign in the form of significant blood flow reductions; 1 of 20 patients with frontotemporal disease showed the posterior cingulate sign. That patient’s illness has evolved into Alzheimer’s disease. The remaining 19 patients were negative for the posterior cingulate sign. Conclusion: When present, the posterior cingulate sign indicates the presence of Alzheimer’s disease; it is apparently absent in frontotemporal disease, thus serving as a differential diagnostic sign. It was absent in 3 patients with proven tangle-predominant Alzheimer’s disease.
Alzheimer’s disease (AD) is the most common of the demential disorders, and it is increasingly prevalent in an aging population. However, recent publications have suggested the possibility of effective treatment (1–3). These developments indicate the need for differential diagnostic strategies to separate AD from the remainder of the demential diseases. An important observation was made by Minoshima et al. (4) in 1994 when they suggested that reduced tissue metabolism in the posterior cingulate cortex was a diagnostic sign of AD. We undertook a study to determine whether the posterior cingulate sign is useful in differential diagnosis between AD and the various frontotemporal diseases (FTDs).
MATERIALS AND METHODS
Twenty patients with clinically diagnosed or autopsy-proven (10 patients) AD; 20 patients with clinically confirmed or autopsy-proven (7 patients) with one of the FTD entities, and 20 elderly healthy volunteers underwent regional cerebral blood flow (RCBF) SPECT with 740 MBq 99mTc-hexamethylpropyleneamine oxime (Ceretec; Amersham Health), using a triple-head camera (PRISM 3000; Picker) with fanbeam collimation (6.5 mm in full width at half maximum). Fanbeam collimation correction was applied during acquisition; data were further processed for attenuation and postfiltration corrections (5,6).
Scan findings obtained from the 20 healthy volunteers were interpreted as normal. The scans were placed into Talairach space (7) and were then consolidated into a single reference image using statistical parametric mapping, as described by Friston et al. (8), with MEDx software (Sensor Systems). Scan data from the 20 AD patients and the 20 FTD patients were individually placed in Talairach space and individually compared with the reference image. A table was constructed for each patient showing z scores expressed in terms of P values; x, y, and z locations in mm; and Talairach atlas locations. Statistically significant data were then superimposed on standard MR images in transverse, coronal, and sagittal projections.
Experimental results were tabulated as follows: Table 1 shows the number of patients with AD and FTD in whom posterior cingulate RCBF reduction was identified. Also noted are the numbers of patients who had undergone autopsy. Table 2 shows the diagnostic performance of the posterior cingulate sign with respect to AD, together with 95% confidence intervals, which were calculated using a correction for continuity.
Identification of Posterior Cingulate Flow Deficits by SPECT and Statistical Parametric Mapping
Diagnostic Performance of Posterior Cingulate Sign with Respect to AD
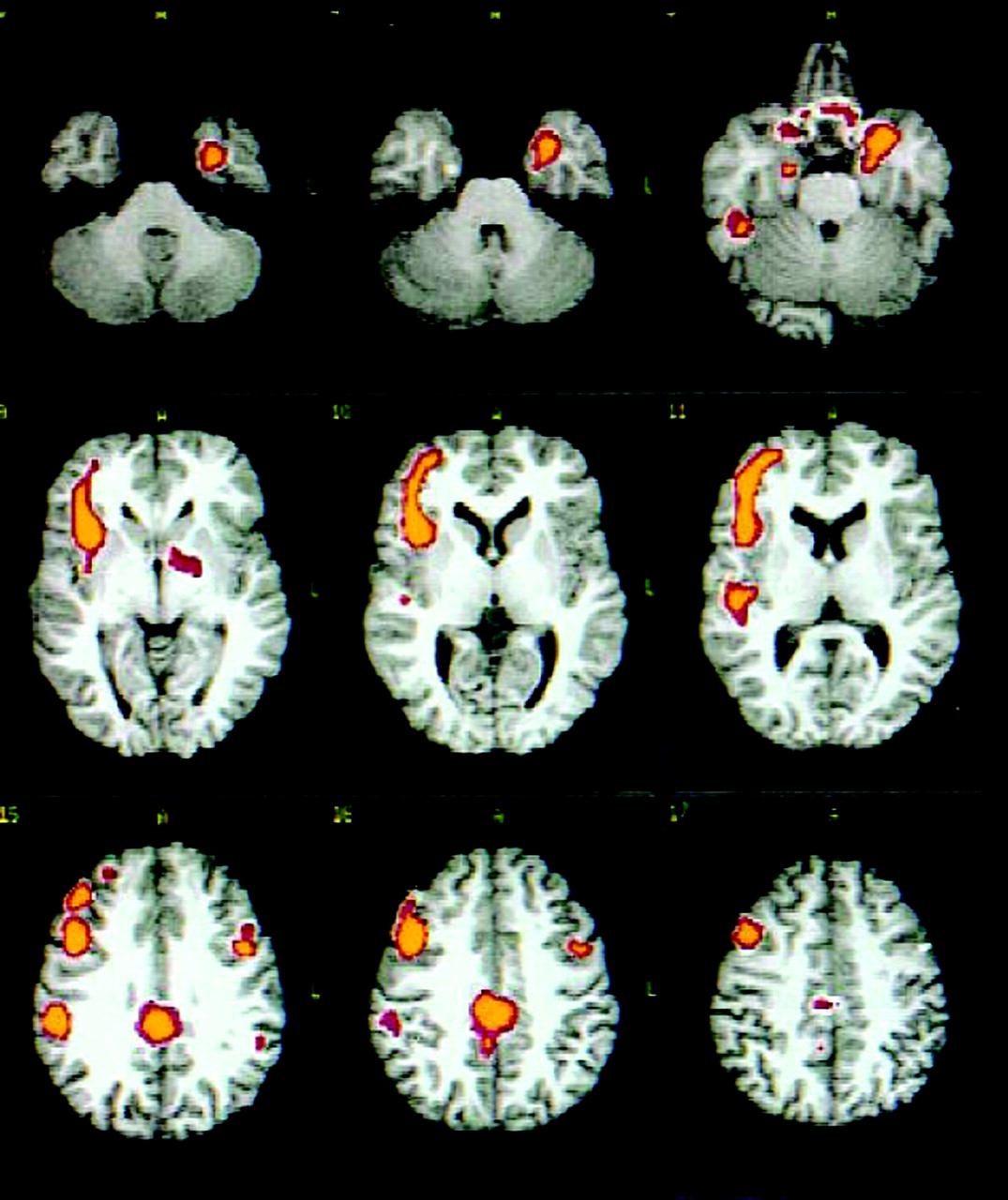
The appearance of the posterior cingulate sign (9–13) on RCBF SPECT scans is illustrated in Figure 1, which shows sets of contiguous transaxial and sagittal sections. The location of the posterior cingulate/retrosplenial area is indicated by arrows. Figure 2 is a set of transaxial sections from the study of a patient who was initially thought to have FTD and who now has a clinical diagnosis of probable AD. The use of the posterior cingulate sign in differential diagnosis is illustrated.

(A) Transaxial sections from a SPECT RCBF scan of a patient with autopsy-proven AD. Arrows indicate the posterior cingulate/retrosplenial cortex. Additional areas of reduced flow are seen bilaterally in the posterior parietal regions. (B) Midline and near-midline sagittal sections from the RCBF SPECT study of the same patient. Arrows indicate posterior cingulate and retrosplenial areas of reduced blood flow.
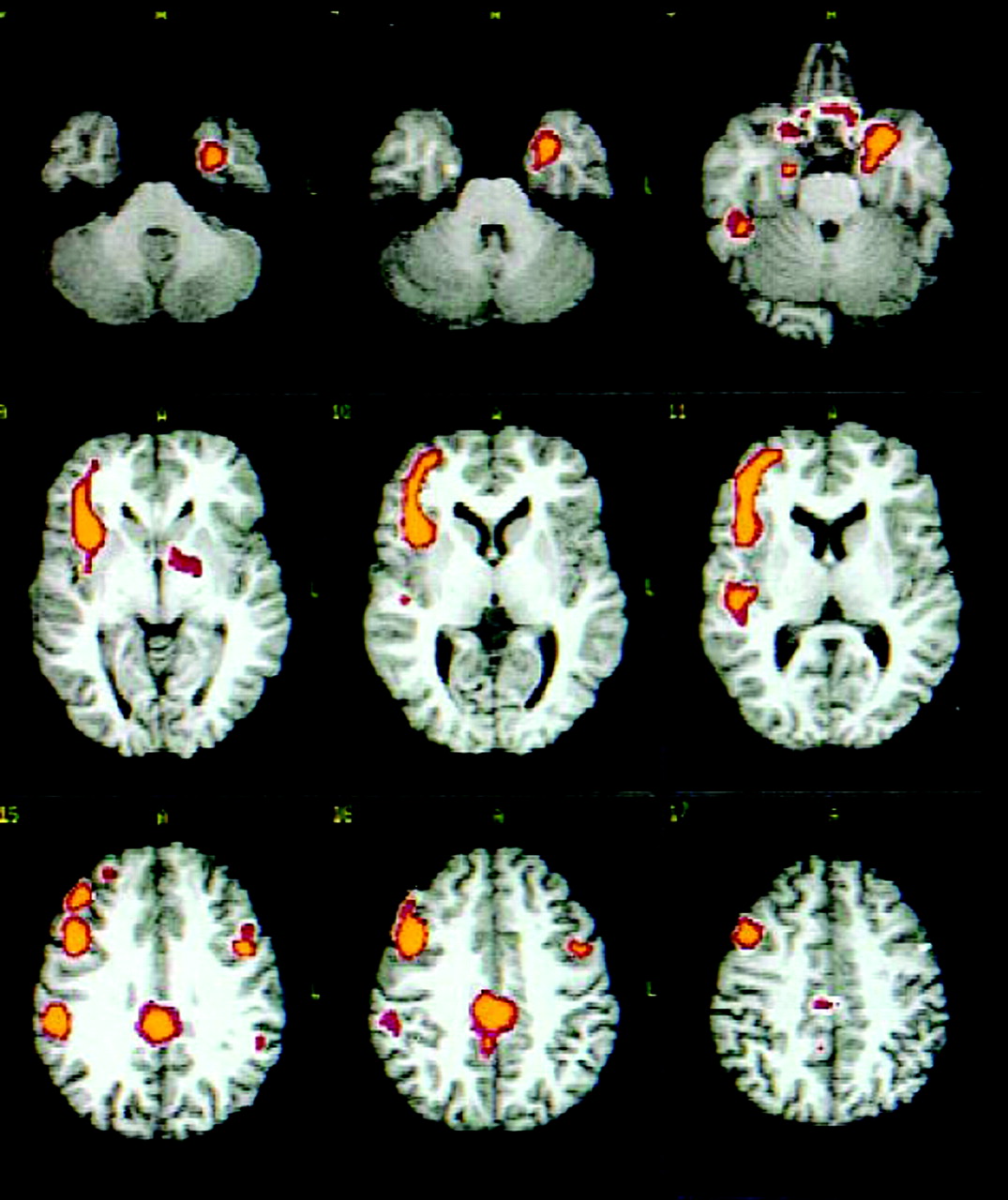
Selected transaxial sections from the RCBF SPECT study of a 67-y-old woman referred for imaging because of a diagnosis of possible frontotemporal dementia. The posterior cingulate sign is present in the posterior midline. With continuing evaluation of the patient, her diagnosis is now probable AD.
Autopsy specimens had been evaluated by commonly used standards including those of the National Institute on Aging-Reagan Institute, CERAD (Consortium to Establish a Registry for Alzheimer’s Disease), and the Braak-Braak Alzheimer Classification and several special stains including synaptophysin and α-synuclein. To date, no tissue samples have been taken from the posterior cingulate region.
RESULTS
RCBF deficits in the posterior cingulate are difficult to visualize on 99mTc-hexamethylpropyleneamine oxime scans, even with 5 projections and a variety of color scales. To improve identification of this potentially important diagnostic sign and estimate its relative statistical significance, we undertook the use of statistical parametric mapping, beginning with a small group of individuals who were thought to have AD and Lewy body disease. By comparing the group image of these patients with the group image of a matched group of elderly healthy controls (14), we showed the importance of the posterior cingulate sign in identifying AD in patients with AD and Lewy body disease. We then processed individual scan data against a reference image comprising the scan data of 20 elderly healthy volunteers.
Figure 1A shows the appearance of the posterior cingulate sign in transaxial sections of a patient with autopsy-confirmed early AD. In addition to the areas of significant involvement in the inferior left and posterior right frontal and temporal lobes, and in the inferior parietal regions bilaterally, a posterior midline localization representing the posterior cingulate region is seen. Figure 1B is a complete set of sagittal sections that show involvement not only of the posterior cingulate but also of the retrosplenial region, extending to the posterior cortical midline. These images represent the usual appearance of the positive posterior cingulate sign on RCBF SPECT scan data processed with statistical parametric mapping in the manner we have described.
As Table 1 indicates, we identified the posterior cingulate sign in 16 of 20 patients with clinical or autopsy-proven AD. The 4 patients in whom the posterior cingulate was not demonstrated had all undergone autopsy. It is interesting to note that 3 of these patients had tangle-predominant AD (15), whereas 1 patient had AD of moderate extent, even though the posterior cingulate sign was not apparent. Table 1 also shows that of individuals with clinical or autopsy evidence of the presence of an FTD (16), 19 showed no evidence of posterior cingulate flow deficits. However, the sign was present in 1 of the 20 patients; in Figure 2, transaxial views of this patient’s scan show the sign as an area of significantly reduced flow in the posterior midline. Further clinical follow-up of this patient made evident that she indeed had probable AD, confirming the positive posterior cingulate sign.
Table 2 shows the general performance of the posterior cingulate sign with respect to sensitivity, specificity, and positive and negative predictive values. Specificity and positive predictive values are encouraging for these small groups of patients. Of interest is the likelihood ratio of 16.00, which reflects the relative weight of the posterior cingulate positive sign in the differentiation of AD from FTD.
DISCUSSION
With the apparent advent of effective treatment for AD, differential diagnosis between AD and other entities such as the FTD group will be important. We have tested the posterior cingulate sign as a marker of AD in SPECT RCBF studies by comparing images of a group of 20 clinically diagnosed or autopsy-proven patients with AD and a group of 20 clinically diagnosed or autopsy-proven patients with FTD with a reference image of 20 elderly healthy volunteers using statistical parametric mapping. Interesting results have been obtained.
CONCLUSION
RCBF in the posterior cingulate/retrosplenial region is often significantly reduced in the presence of AD. However, the sign was not positive in the 3 cases of tangle-predominant AD in our series of 101 autopsied patients. Otherwise, the presence of the posterior cingulate sign helps to differentiate between AD and FTD.
Acknowledgments
This work was supported by grant 5 P30 AG0 12300 from the National Institutes of Health and from Amersham Health. The authors recognize Drs. Sandra Chapman, Anne Lipton, and Myron Weiner for significant clinical contributions and Drs. Eileen Bigio, Philip Boyer, and Charles L. White III for contributing to pathologic diagnoses by performing autopsies. The authors acknowledge the contributions of Dorothy Smith for illustrations and of Constance Wakefield, Carol Gibson, and RosaLina Harrison for manuscript preparation.
Footnotes
Received Sep. 30, 2003; revision accepted Dec. 12, 2003.
For correspondence or reprints contact: Frederick J. Bonte, MD, Nuclear Medicine Center, University of Texas Southwestern Medical Center, 5323 Harry Hines Blvd., Dallas, TX 75390-9061.
E-mail: Frederick.Bonte{at}UTSouthwestern.edu.





{kind=link}
{kind=link}