


Abstract
This trial was an initial assessment of the feasibility, in vivo targeting, and biokinetics of 16β-18F-fluoro-5α-dihydrotestosterone (18F-FDHT) PET in patients with metastatic prostate cancer to assess androgen receptor expression. Methods: Seven patients with progressive clinically metastatic prostate cancer underwent 18F-FDG and 18F-FDHT PET scans in addition to conventional imaging methods. Three patients had their studies repeated 1 mo later, 2 while on testosterone therapy, and the third after treatment with 17-allylamino-17-demethoxygeldanamycin (17-AAG). High-pressure liquid radiochromatography was used to separate 18F-FDHT from radiolabeled metabolites. Lesion-by-lesion comparisons between the 18F-FDHT, 18F-FDG, and conventional imaging methods were performed. Results: Metabolism of 18F-FDHT was rapid, with 80% conversion within 10 min to radiolabeled metabolites that circulated bound to plasma proteins. Tumor uptake was rapid and tumor retention was prolonged. Fifty-nine lesions were identified by conventional imaging methods. 18F-FDG PET was positive in 57 of 59 lesions (97%), with an average lesion maximum standardized uptake value (SUVmax) = 5.22. 18F-FDHT PET was positive in 46 of 59 lesions (78%), with the average positive lesion SUVmax = 5.28. Treatment with testosterone resulted in diminished 18F-FDHT uptake at the tumor site. Conclusion: 18F-FDHT localizes to tumor sites in patients with progressive clinically metastatic prostate cancer and may be a promising agent to analyze antigen receptors and their impact on the clinical management of prostate cancer.
Prostate cancer is the second most common cause of cancer-related deaths in the United States (1). Several aberrant pathways contribute to the development of the metastatic phenotype and the emergence of castration resistance, which eventually lead to death of the patient. Clinically, virtually all patients show elevations in prostate-specific antigen (PSA) and evidence of continued signaling through the androgen receptor (AR). Pathologic and molecular analyses show evidence of AR gene expression and increased protein mutation, all of which contribute to a change of function, and ligand-independent activation (2–7). To effectively study the biology of prostate cancer and to develop therapies that target the AR require methods of assessing AR expression and functionality. However, such analyses are difficult as the dominant site of metastases is bone, a difficult site to biopsy. Furthermore, the biology of the metastases can differ from the primary prostate cancer; therefore, tissue from the primary tumor does not necessarily inform as to the status of the bony disease.
We have been developing molecular imaging techniques for the assessment of these pathways in prostate cancer. Dihydrotestosterone (DHT) is the primary ligand of the AR. Recently, Washington University (St. Louis, MO) has developed a radiotracer form of DHT, for the purpose of imaging AR expression noninvasively in vivo, using PET (8,9). This radiotracer form, 16β-18F-fluoro-5α-dihydrotestosterone (18F-FDHT), was selected for clinical research evaluation after comparison in animals with related compounds. In this article, we report on the initial studies of molecular imaging using the AR as a target.
MATERIALS AND METHODS
Patients
Patients were selected prospectively under a protocol that required that patients were castrate with evidence of disease progression according to laboratory and clinical criteria. Eligibility criteria included progressive histologically documented prostate cancer despite castrate levels (<50 ng/dL) of testosterone, progression as defined by a ≥50% increase in PSA that was sustained for a minimum of 3 observations obtained at least 1 wk apart, the development of new lesions, or an increase in preexisting lesions on bone scintigraphy. Patients were required to have a Karnofsky performance status of >60%. All patients were required to sign informed consent before registration to the study. As this protocol was an imaging study; there were no restrictions on concomitant therapies. However, care was taken so that no medications that directly competed for the AR were initiated before the 18F-FDHT scans (except for posttherapy follow-up scans performed on 3 patients). Two of the patients were receiving chemotherapy regimens; 3 patients were on gonadotropin-releasing factor agonists while being prepared for therapies expected to alter AR expression or bioavailability (including treatment with the drug 17-allylamino-17-demethoxygeldanamycin [17-AAG] and high-dose testosterone); and the remaining 2 patients were on gonadotropin-releasing hormone agonist, goserelin (Zoladex) or leuprolide (Lupron) (Table 1), for the purposes of medical castration. The clinical trial was performed under the auspices of Memorial Sloan-Kettering Institutional Review Board, protocol IRB 97-007. 18F-FDHT was administered under the auspices of the Memorial Sloan-Kettering Radioactive Drug Radioactive Drug Research Committee.
Comparison of 18F-FDG and 18F-FDHT Uptake in Patients with Advanced, Progressing Prostate Cancer
All 7 patients underwent 18F-FDG PET, dynamic and whole-body 18F-FDHT PET, and a bone scan. All patients had their 18F-FDHT and 18F-FDG PET scans within 48 h, except patient 6, who had an interval of 8 d because of 18F-FDHT production problems.
The median age of the 7 patients was 66.5 y (range, 47–76 y), with a mean Karnofsky performance score of 85 (range, 80–90). The median baseline PSA was 69 ng/mL (range, 6.3−2,637 ng/mL), and the median testosterone concentration was 0 (range, 0–11 ng/dL). The median Gleason score was 7 (range, 7–10). Five of 7 patients had bone disease only, 1 patient had soft-tissue disease only, and 1 patient had both soft-tissue and bone disease.
Three of the patients were rescanned with 18F-FDHT, 2 after treatment with exogenous testosterone and one after treatment with 17-AAG, an ansamycin derivative intended to degrade the AR. The follow-up 18F-FDHT scan was performed 4–5 wk after the initial study. Two patients had pain and discomfort that precluded them lying in one position for a prolonged period. Therefore, dynamic scanning and kinetic analysis were not preformed on these patients.
Imaging Methodology
Before 18F-FDG PET scanning, the patient was required to fast for at least 6 h, and a serum glucose determination was checked just before injection of 370 MBq (10 mCi) 18F-FDG. All studies were performed with an Advance dedicated PET scanner (General Electric Medical Systems). This camera has a field of view of 55 cm in diameter and 15.2 cm in axial length. All scanning was performed in 2-dimensional (septa-in) mode. The transaxial resolution is 4.3-mm full width at half maximum (FWHM) at the center of the field of view, increasing to 7.3 mm at a radial distance of 20 cm. The average axial resolution decreases from 4.0-mm FWHM at the center to 6.6 mm at 20 cm (10). 18F-FDHT scans were performed at least 24 h after the 18F-FDG scan. No fasting was necessary. An index lesion was selected from the 18F-FDG scan, and the patient was positioned within the scanner so that the index lesion was approximately in the center of the field of view. A transmission scan was performed first before administration of the 18F-FDHT to verify correct positioning, and the patient was repositioned if necessary. The patient was injected through a central line and a 50-min dynamic emission scan was initiated. The dynamic scan was comprised of ten 1-min frames followed by eight 5-min frames. Upon completion of the dynamic scan, the patient was allowed to rest for 10 min and urinate if necessary. The patient was then repositioned on the couch, and a whole-body scan was performed from the bottom of the ear to the base of the pelvis. The emission scan was performed first (4 min per bed position) followed by the transmission scans of 3-min per bed position. All images were reconstructed by iterative reconstruction with segmented attenuation correction. The 18F-FDHT and 18F-FDG images were interpreted independently by one reader on a 5-point scale to categorize the confidence of detection of individual lesions. The studies were interpreted without knowledge of the bone scan, CT, or MRI findings. The scale was as follows: 1 = negative, 2 = probably negative, 3 = equivocal, 4 = probably positive, and 5 = definitely positive. The selection of a 5-point scale (rather than a 3-point scale) allowed the differentiation between clearly negative lesions (1) from probably negative (2), completely equivocal (3), highly suspicious (4), and definitely positive (5) lesions. This scale allowed a semiquantitative comparison of the confidence of the presence of tumor between 18F-FDHT and 18F-FDG. The comparative image reading of both tracers was performed using 2 triangulation display windows, which allowed transaxial, coronal, and sagittal slices of both image sets to be displayed alongside one another on a dual monitor. Lesions were delineated on the 18F-FDG image set using a region-of-interest (ROI) tool, which is then copied to the corresponding lesion on the 18F-FDHT image set. Only lesions that were scored 4 or 5 were considered positive for further analysis; therefore, the maximum standardized uptake value (SUVmax) is only reported for these lesions. SUVmax represents the maximum specific activity (Bq/g) of each tracer in the lesion divided by the injected activity (Bq) divided by the patient’s weight (g). This is a quantitative scalar magnitude that is independent of the PET window display settings.
Radiochemical Synthesis of 18F-FDHT
18F was produced on the Memorial Sloan-Kettering Cancer Center CS-15 Cyclotron from the H218O by the 18O(p,n)18F nuclear reaction. An aliquot of the target water containing approximately 7.4 GBq (200 mCi) 18F was added to nBu4NOH (2.3 μL) contained in a vacuum-sealed test tube. The target water was removed with 3 azeotropic distillations using 0.5–1 mL of CH3CN at an elevated temperature and a gentle stream of nitrogen. The dried activity was redissolved in tetrahydrofuran and transferred to a vacuum-sealed test tube containing 1–2 mg of triflate precursor, capped with a Teflon-lined stopper (DuPont), and placed in an oil bath at 55°C for 5 min. The mixture was subsequently cooled at −78°C. To the cold solution was added 0.150 mL of LiALH4 solution (1 mol/L in Et2O), mixed in a vortex, and allowed to react for 10 min before being quenched by the addition of 0.2 mL of acetone and 0.5 mL of 3N aqueous HCl. After a 10-min reaction period at 70°C, the contents were extracted with Et2O 3 times and subsequently dried over anhydrous MgSO4 and passed through a Na2SO4 drying column using ether. The ether was evaporated under vacuum and the residue was dissolved in 1 mL of high-pressure liquid chromatography (HPLC) solvent. The product was separated by normal-phase HPLC as previously described (11) with the no-carrier-added 18F-FDHT formulated in 0.9% Sodium Chloride for Injection USP and Alcohol USP. The inactive components consisted of 0.9% Sodium Chloride for Injection USP and Alcohol USP in a ratio of 90:10 with a total volume of 5 mL for formulation.
The total radiochemistry synthesis time was approximately 100 min, and the 18F-FDHT was produced in decay-corrected radiochemical yield approaching 30%.
Radiometabolite Analysis of 18F-FDHT
Four patients who underwent an 18F-FDHT scan had blood drawn for metabolite analysis. Up to a maximum of 17 serial blood samples were taken at the following collection times when possible: 0, 0.5, 1, 1.5, 2, 3, 4, 5, 7, 10, 15, 20, 30, 40, 50, 60, and 120 min after injection. Aliquots of blood were transferred in preweighed tubes and counted for activity. The remaining blood was centrifuged (5 min, 2,000g at room temperature), and aliquots of plasma were transferred into preweighed tubes and counted for activity in an LKB Wallac γ-counter (1282 Compugamma CS). The measured activities were corrected for decay, and data were expressed as SUV normalized to body weight.
To measure the fraction of free 18F-FDHT versus protein-bound 18F-FDHT, plasma samples were deproteinized by ultrafiltration. Therefore, 500 μL of plasma were transferred into prewashed filtration cartridges (Centricon YM-30; Millipore) and centrifuged according to the manufacturer’s instructions. The filtrate was removed, weighed, and counted immediately in an LKB Wallac γ-counter (1282 Compugamma CS). The obtained activity per gram of the free fraction was corrected for decay and expressed as the percentage of the activity per gram from the corresponding plasma sample.
Metabolite analysis was determined by HPLC. One-half milliliter of plasma was mixed with 0.7 mL of acetonitrile containing unlabeled FDHT (0.05 mg/mL) as reference compound. After centrifugation at 2,000g for 5 min, the protein-free supernatant (about 1.1 mL) was removed, concentrated under reduced pressure, and used directly for the chromatographic evaluation. The HPLC system consisted of 2 pumps (model 501; Waters), a reversed-phase C18 column (Beckman Ultrasphere; 5 mm, 250 × 4.6 mm) connected to an ultraviolet detector (model 486; Waters) operated at 254 nm followed by a radioisotope detector (Radiomatic 625TR, 500 μL cell; Packard) and a fraction collector (FRAC-100; Pharmacia). The column was eluted applying a gradient from 40% acetonitrile in 0.01 mol/L phosphoric acid up to 90% acetonitrile using a flow rate of 1 mL/min and a run length of 20 min for each sample. Under these conditions, 18F-FDHT elutes at 9 min. The data are expressed as the percentage of total activity in plasma. Fractions were collected and counted to calculate the recovery.
RESULTS
Imaging
A lesion-by-lesion comparison of the 59 individual lesions with regard to 18F-FDG and 18F-FDHT uptake was performed and a summary of all findings is summarized in Table 1. All of the bone lesions (detected by 18F-FDG) were positive on bone scan, and the remaining soft-tissue lesions were positive on CT (Table 2), with the exception of 2 prostate bed recurrences. Combining the findings of all 7 patients in this study, 10 soft-tissue lesions and 49 bone lesions were detected. The number of lesions per subject varied from 4 to 16. The majority of the mismatched lesions, 8 of 11, were clustered in patients 1 and 2. 18F-FDG was positive in 57 of 59 lesions (97%), with the average positive lesion SUVmax = 5.22. 18F-FDHT was positive in 46 of 59 lesions (78%), with the average positive lesion SUVmax = 5.28.
Results of Conventional Imaging Examinations in Patients with Advanced, Progressing Prostate Cancer
An example of a typical 18F-FDHT biodistribution (patient 6) is shown in Figure 1. The image is displayed in maximum-intensity-pixel (mip) format to allow full visualization of the biodistribution of the 18F-FDHT tracer. Of particular note is the presence of 18F-FDHT in the blood pool of the heart, great vessels, uptake in the vessels of the hand (of unknown cause) near the site of injection, concentration in the liver, and excretion of metabolite into the small and large intestine, especially excretion of the 18F-FDHT via the bile (prominent gallbladder and bile ducts). There is uptake evident in metastatic tumor sites in the skull, right upper humerus, right axillary region (probably in a rib), and in left scapula. More posterior lesions, in the ischium and T10, are not well seen in this imaging format.

18F-FDHT scan of patient 6 (Table 1) displayed in mip format to allow better visualization of the whole-body distribution of this tracer. There is uptake in the skull, right upper humerus, and upper thorax at 2 sites.
Figure 2 shows another 18F-FDHT PET image (Fig. 2A) alongside the 18F-FDG PET image (Fig. 2B) for patient 7. It illustrates the contrasting metabolism of the 2 tracers. As with patient 6, blood-pool activity is clearly apparent as is the gallbladder and biliary tree. In addition, there is uptake in numerous metastatic lesions in the cervical spine, left rib cage in 2 ribs, and left periaortic region. The large area of uptake in the pelvis could be confused with right iliac uptake, but the uptake is actually in an iliac loop, related to a urinary diversion, which the patient has undergone. There is uptake at the same sites on the 18F-FDG images, although quantitative differences are apparent, in terms of the intensity of uptake. For example, the cervical lesion, though clearly 18F-FDG positive, is less well seen than on the 18F-FDHT image.

18F-FDHT (A) and 18F-FDG (B) of patient 7 (Table 1) displayed in mip format.
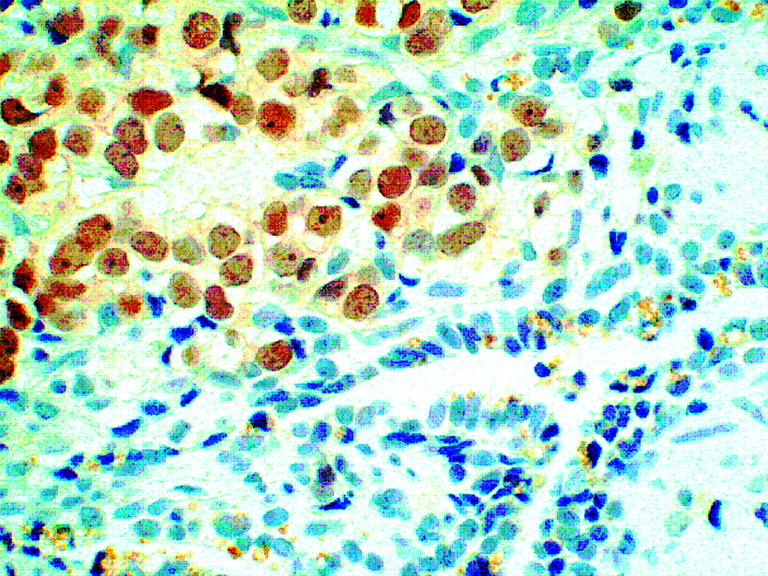
Patient 1 underwent biopsy of the prostate bed recurrence, 13 d after a positive 18F-FDHT study, at the site. The biopsy was positive for prostate cancer recurrence with a Gleason lesion score of 9/10. The histologic section (Fig. 3) shows clearcut AR expression or overexpression in the nuclei of the prostate cancer cells (brown stain) as they invade the blue-staining seminal vesicle cells. The brown stain reflects AR expression and illustrates the concept that AR staining in the nucleus is thought to represent active receptor.

Prostate tumor section from a biopsy sample obtained from patient 1 stained with hematoxylin–eosin and also showing positive for androgen by immunohistochemistry (brown stain).
Pharmacokinetics
Four patients had blood drawn over the 60 min after injection. Plasma was separated, and analysis of protein-bound radioactivity and the proportion of radioactivity and metabolites were determined, after extraction with alcohol. The results for these 4 patients are shown in Figures 4A–4D.
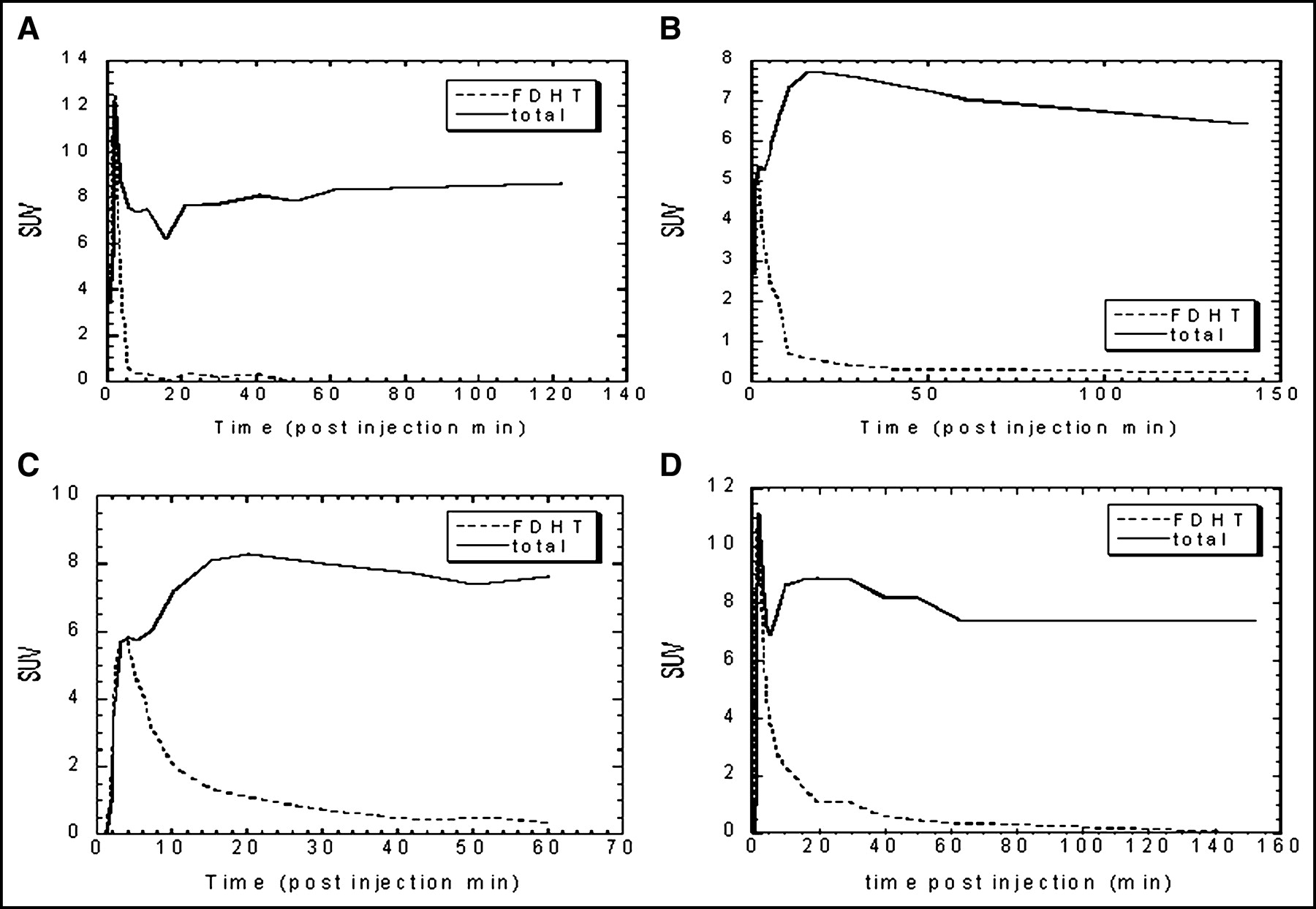
Fraction of 18F-FDHT vs. total 18F activity from blood samples of 4 patients (A–D), who had repeated blood samples drawn over the 60 min after injection.
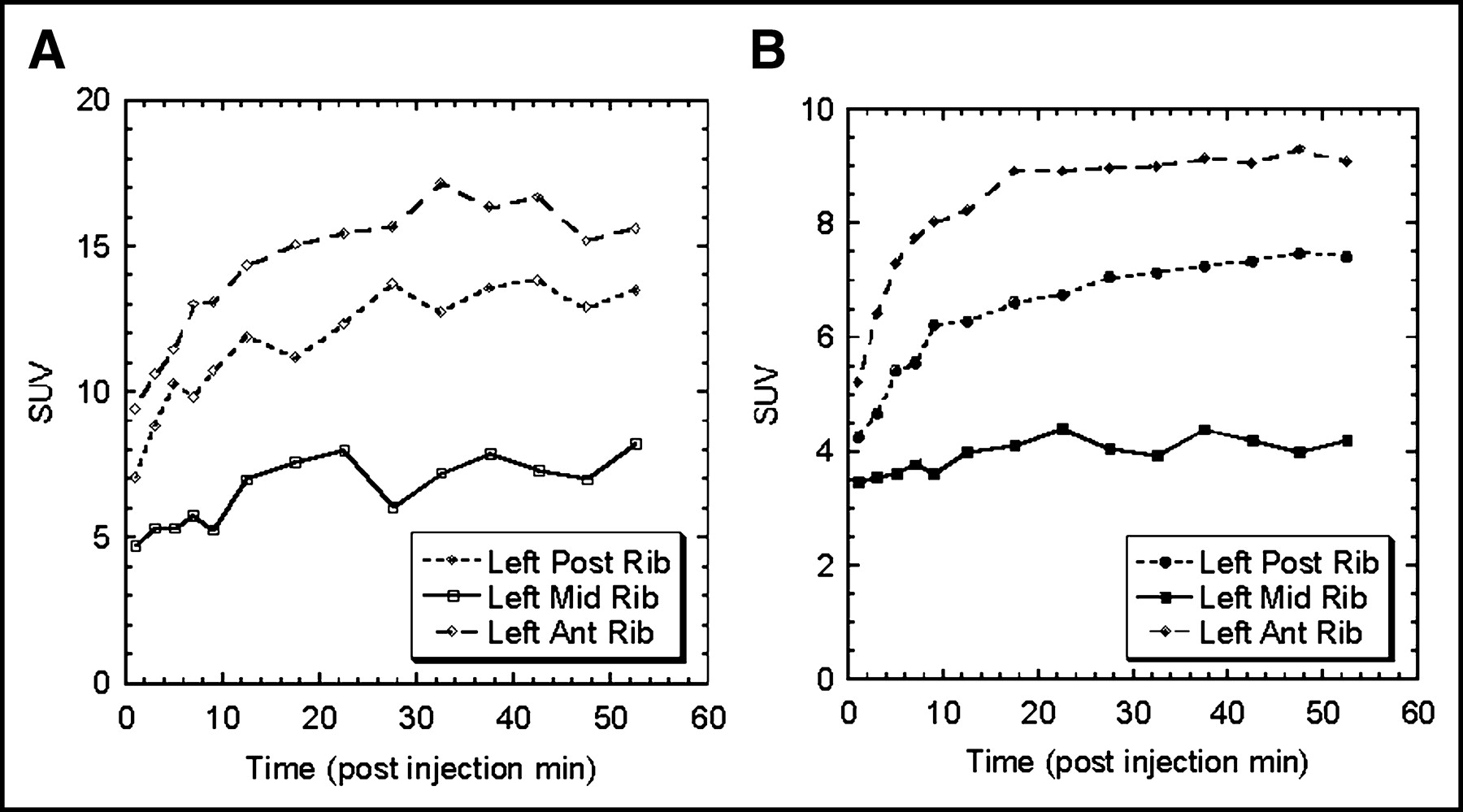
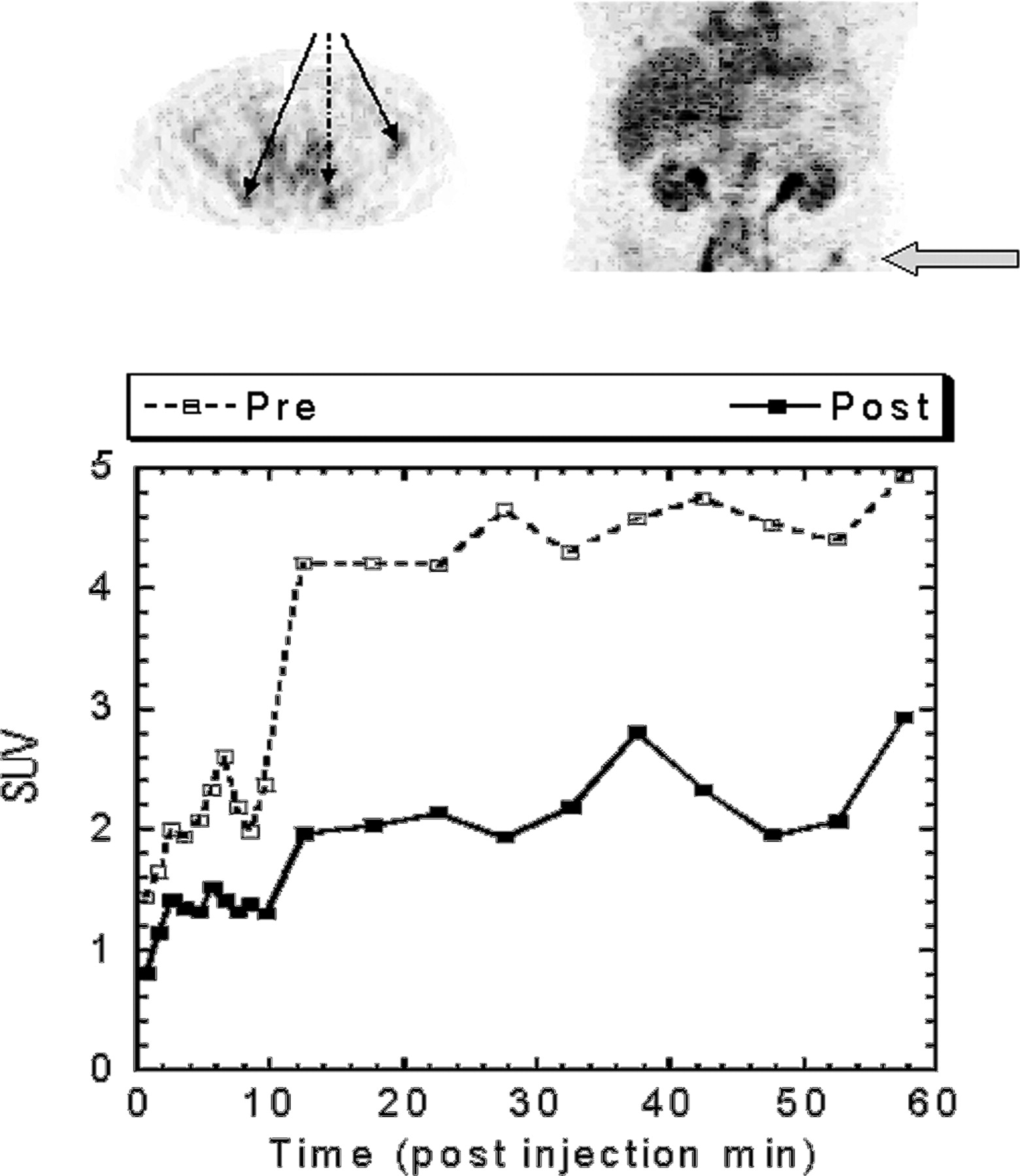
Two patients had complete tumor uptake curves in 3 lesions before and after therapy. One such case is shown in Figures 5A and 5B. Uptake was rapid, with 80% of the final uptake occurring within 10 min. There was a prolonged plateau thereafter, during which time there was retention throughout the interval of study, with little discernible increase or loss in this plateau phase.

18F-FDHT tumor uptake in each of 3 lesions of patient 7 obtained by ROI analysis from the dynamic PET data before (A) and after (B) therapy. Post = posterior; Mid = middle; Ant = anterior.
Blood clearance of 18F-FDHT was determined by serum analysis (Fig. 4). The free fraction of activity in plasma was <2% at all time points during the investigation for patients 5, 6 (first 18F-FDHT scan), and 7, indicating that 18F-FDHT as well as the metabolic products are highly bound to plasma proteins. The only exception was found in patient 6 for the second 18F-FDHT scan, where the free fraction was 95% and 30% for the 0.5- and 1-min plasma sample, respectively. This might be due to saturation of the peripheral DHT binding sides as a result of the testosterone treatment.
HPLC analysis of plasma samples shows a very fast metabolism of the radiotracer. The calculated in vivo half-lives were 4.2 min (patient 7), 3.5 min (patient 5), 5.8 min (patient 6, first administration), and 5.8 min (patient 6, second administration). The metabolic profile in all 4 subjects shows that the metabolites are more hydrophilic compared with those of 18F-FDHT. However, in the subject with the fastest metabolism, additional more lipophilic metabolites are seen. These more lipophilic metabolites account for 75% in the 5-min plasma sample and drop to 5% in the 30-min plasma sample. They are below the detection limit in all later plasma samples. Values for the recovery of the samples from HPLC were measured and were always >95%, indicating that no lipophilic metabolites were missed due to the selected elution conditions. Therefore, it must be assumed that the in vivo metabolism of 18F-FDHT can vary somewhat between subjects but is uniformly rapid.
Posttreatment Effects on Uptake
Three patients had follow-up scans after treatment. Two received exogenous testosterone (patients 3 and 6 in Table 1) and patient 1 received ansamycin (17-AAG). Both of these types of treatments would be expected to reduce the binding of 18F-FDHT to the AR. Testosterone treatment should increase the amount of DHT competing at the receptor site, and this should reduce uptake. 17-AAG should reduce the concentration of the AR itself, through its action on heat shock protein-90 (12).
A coronal and axial image shows the sites of the lesion in patient 3 (Fig. 6 top). The ROI analysis of these 3 lesions on the dynamic PET datasets is also shown in Figure 6 (bottom) for scans before and after therapy. In this patient, the DHT concentration increased from a baseline level of 3 ng/dL to a value of 62 ng/dL at the time of second study. In the posttreatment scan, the 18F-FDG scans showed no significant change, either in the number of lesions or the SUV level, before and after therapy. The average SUV1 = 4.56 (n = 16); the average SUV2 = 4.37 (n = 16). There was a major reduction in 18F-FDHT uptake in the 3 tumors for which time–activity curves were available, and the whole-body images showed a visual reduction in uptake in all 15 lesions that were initially positive with 18F-FDHT.
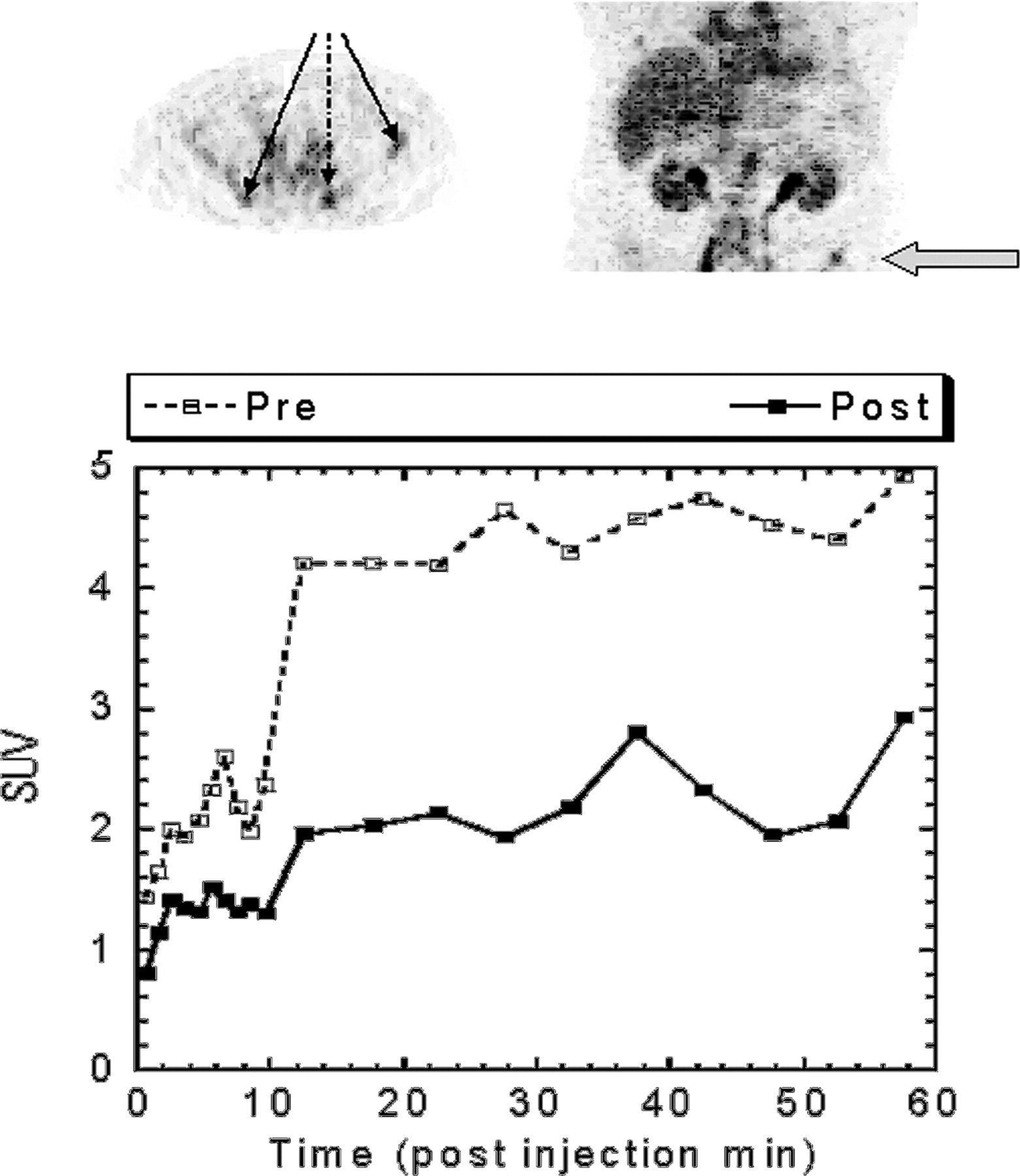
(Top) Coronal and transaxial image displays containing 3 tumor sites in the pelvis (left iliac crest, the left and right sacroiliac joints) on which ROIs were drawn. (Bottom) Time–activity curves before (dashed line) and after (solid line) treatment with testosterone. The ordinate values represent an average of all 3 lesion SUVs for clarity, although all 3 tumors showed significant suppression of 18F-FDHT uptake after treatment.
The second patient treated with testosterone had a documented elevation in serum DHT of 54 ng/dL, but this decreased to 2 ng/dL before the follow-up 18F-FDHT scan. The 18F-FDG scans showed no significant change from the pretherapy scan (average SUV of 4.05 [n = 5] before therapy vs. 4.06 [n = 5] after therapy). The follow-up 18F-FDHT study was essentially unchanged from the baseline, suggesting that it is the ambient concentration of hormone—not the prior history of treatment—that determines 18F-FDHT tracer localization.
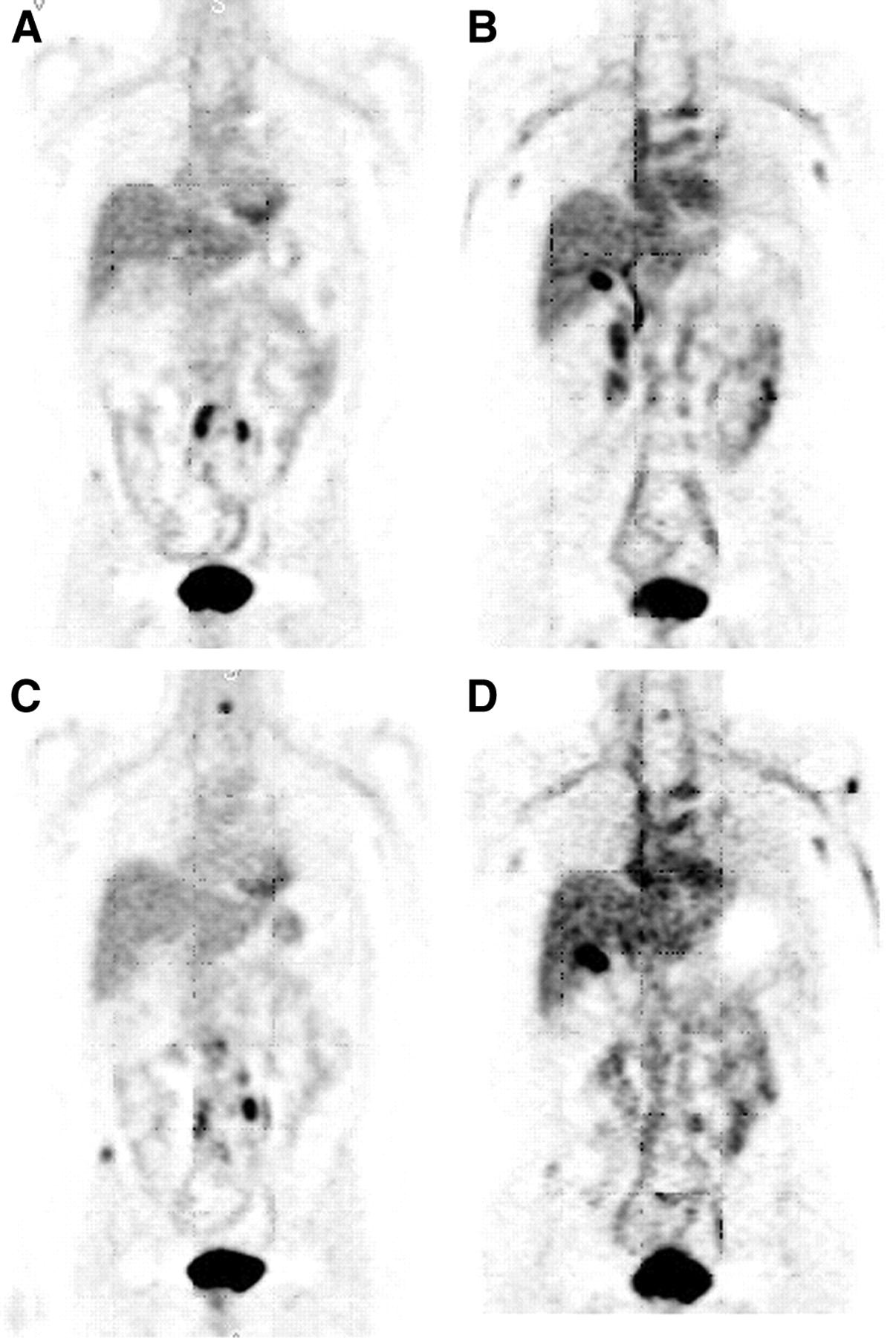
A third patient (patient 1) was treated with 17-AAG, and both 18F-FDG and 18F-FDHT scans were repeated after therapy. The 18F-FDG scans showed only a slight change (average SUV of 7.5 [n = 7] before therapy vs. 8.8 [n = 9] after therapy]). Two new lesions, one in the right iliac crest and another in the cervical spine, had avid 18F-FDHT and 18F-FDG uptake (Fig. 7).

18F-FDG and 18F-FDHT images of patient 1 before and after treatment with 17-AAG. (A and B) Corresponding coronal sections from the pretreatment 18F-FDG and 18F-FDHT scans. (C and D) Respective coronal slices after therapy. New lesions are seen on 18F-FDG and 18F-FDHT in the ilium, C3, and prostate bed. The site in the prostate bed was confirmed by biopsy.
The data from the 3 patients imaged with 18F-FDHT after therapy support the concept that there is competition between 18F-FDHT and DHT for the AR in the tumor sites and also that the uptake of 18F-FDHT in lesions does reflect posttreatment changes in the AR levels.
DISCUSSION
This study was performed to investigate the potential of a new radiotracer, 18F-FDHT, to characterize the biology in terms of the androgen levels of patients with prostate cancer. Direct tissue samples are not part of routine clinical practice for metastatic prostate cancer and are, in many cases, difficult or impossible to obtain. The patterns of spread of prostate cancers make it difficult to quantify tumor regression and progression in a reproducible way. Most patients with advanced disease have bone metastases, and the radionuclide bone scan is a sensitive means for detecting initial spread to bone (13), but this method does not visualize tumor directly and exhibits a significant lag when used to assess acute tumor response (14).
These difficulties with conventional single-photon nuclear techniques have resulted in the exploration of 18F-FDG PET (15) for the detection of metastatic prostate cancer, and there is emerging evidence that such approaches will be useful for monitoring treatment response in solid tumors as well (15–17). However, the role of 18F-FDG PET in prostate cancer is controversial, and the results are heavily influenced by the patient selection. At our center, a disease-states model is used to control patients for a discrete phase in the natural history of the disease (18,19). Our selected patient population has shown that lesions seen on bone scan only remain stable over time, whereas lesions seen on 18F-FDG PET progressed (20).
In this study, we applied similar stringent criteria for selecting patients eligible for the 18F-FDHT protocol. 18F-FDHT is a selective marker for ARs and, therefore, exhibits prostate cell specificity. In this way, it is a more direct measure of prostate metastases than the bone scan (or even 18F-FDG).
In the 7 patients studied, we identified 57 18F-FDG–avid lesions in bone and soft tissue that correlated with suspicious findings on bone scintigraphy, CT, or MRI. Seventy-nine percent of these 18F-FDG–avid lesions also took up 18F-FDHT. The purpose of this study was to identify a group of metabolically active tumor sites that could be assessed in terms of their ability to take up and retain 18F-FDHT. Correspondence between 18F-FDHT with 18F-FDG was found in 5 of 7 patients. Two of the patients accounted for the majority of mismatched lesions, which were 18F-FDG–positive, 18F-FDHT–negative lesions. The basis for this metabolic heterogeneity is unknown but is hypothesized to represent variability in AR status versus glucose metabolic rate. Such differences may underscore the biologic heterogeneity of prostate cancer that occurs during disease progression. Follow-up studies to further explore these relationships are being undertaken in the laboratory and the clinic. The results of properly controlled clinical trials show that there is continued AR signaling in the overwhelming majority of castrate patients and, therefore, that AR is a relevant therapeutic target.
In all subjects for whom adequate data were available, the metabolism of 18F-FDHT was rapid, with 80% conversion within 10 min to a radiolabeled metabolite that circulated bound to plasma proteins. Tumor uptake was also rapid (80% uptake at 10 min), suggesting that 18F-FDHT was the active radiopharmaceutical for targeting, and entered a plateau phase for the duration of the dynamic and subsequent whole-body scan, indicating tumor cell retention. Tumor SUV values for 18F-FDHT were in the same range as for the initial scans on all patients, suggesting that the rapid metabolic half-life did greatly affect individual lesion uptake. Instead, biologic features of the tumor, such as the AR, are the likely cause for the finding that some tumors had excellent uptake.
CONCLUSION
To our knowledge, this study is the first assessment of PET scanning to characterize castrate metastatic prostate lesions, in patients with progressive disease visible by conventional imaging methods, on the basis of the AR. We have shown that imaging prostate cancer by 18F-FDHT PET is feasible and that sites of uptake correspond with sites demonstrated by standard bone scintigraphy, soft-tissue imaging, and 18F-FDG PET. A major finding of this study was that, of the 59 lesions detected in 7 patients, the majority of metastatic lesions also demonstrated 18F-FDHT uptake. A second important observation was that, although many tissues in the body would be expected to exhibit AR expression, prostate cancer bound tracer with far greater affinity than normal tissue. This finding allows the identification of active disease, lending credence to the observation that the AR is overexpressed in androgen-independent metastatic disease.
The data from this initial study will be used to generate hypotheses for further testing. Questions raised by our findings include the following: What is the correlation between 18F-FDG avidity, 18F-FDHT avidity, and treatment response of individual lesions? What is the relationship between lesions seen by standard imaging studies and 18F-FDHT uptake. What is the relationship between 18F-FDHT uptake and AR expression as assessed by immunohistochemistry. A separate clinical trial in which 18F-FDHT is being compared with 18F-FDG PET and with pathologic assessments of the AR is now underway.
Acknowledgments
The authors thank Dr. Victor Reuter, of the Pathology Department, Memorial Sloan-Kettering Cancer Center, for providing the immunohistology shown in Figure 3. Also, special thanks go to John Katzenellenbogen from the University of Illinois, Urbana, for his continued intellectual input and support of this study. The authors also thank Rebecca Gonzalez and Elaina Chu for assisting in the gathering of scan- and patient-related data. This research was supported in part by the Norman Hascoe Fund, the Laurent and Alberta Gerschel Foundation, and National Cancer Institute grant P50 CA 86438.
Footnotes
Received June 20, 2003; revision accepted Oct. 29, 2003.
For correspondence or reprints contact: Steven M. Larson, MD, Department of Nuclear Medicine (SC212), Memorial Sloan-Kettering Cancer Center, 1275 York Ave., New York, NY 10021.
E-mail: larsons{at}mskcc.org
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Report on the PET/CT Image-Based Radiation Dosimetry of [18F]FDHT in Women, a Validated Imaging Agent with New Applications for Evaluation of Androgen Receptor Status in Women with Metastatic Breast Cancer
- Report on the PET/CT Image-Based Radiation Dosimetry of [18F]FDHT in Women, a Validated Imaging Agent with New Applications for Evaluation of Androgen Receptor Status in Women with Metastatic Breast Cancer
- Consecutive Prostate-Specific Membrane Antigen (PSMA) and Antigen Receptor (AR) PET Imaging Shows Positive Correlation with AR and PSMA Protein Expression in Primary Hormone-Naive Prostate Cancer
- Synthesis and Evaluation of 18F-Enzalutamide, a New Radioligand for PET Imaging of Androgen Receptors: A Comparison with 16{beta}-18F-Fluoro-5{alpha}-Dihydrotestosterone
- Multimodality Imaging of Prostate Cancer
- Assessment of Simplified Methods for Quantification of 18F-FDHT Uptake in Patients with Metastatic Castration-Resistant Prostate Cancer
- Loss of dihydrotestosterone-inactivation activity promotes prostate cancer castration resistance detectable by functional imaging
- Reproducibility and Repeatability of Semiquantitative 18F-Fluorodihydrotestosterone Uptake Metrics in Castration-Resistant Prostate Cancer Metastases: A Prospective Multicenter Study
- Specific 18F-FDHT Accumulation in Human Prostate Cancer Xenograft Murine Models Is Facilitated by Prebinding to Sex Hormone-Binding Globulin
- Androgen and Estrogen Receptor Imaging in Metastatic Breast Cancer Patients as a Surrogate for Tissue Biopsies
- Evaluation of Castration-Resistant Prostate Cancer with Androgen Receptor-Axis Imaging
- A Phase I/II Study for Analytic Validation of 89Zr-J591 ImmunoPET as a Molecular Imaging Agent for Metastatic Prostate Cancer
- Phase I Study of ARN-509, a Novel Antiandrogen, in the Treatment of Castration-Resistant Prostate Cancer
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- Unmet Needs in the Prediction and Detection of Metastases in Prostate Cancer
- Measuring Oncogenic Signaling Pathways in Cancer with PET: An Emerging Paradigm from Studies in Castration-Resistant Prostate Cancer
- Practical Approach for Comparative Analysis of Multilesion Molecular Imaging Using a Semiautomated Program for PET/CT
- Noninvasive measurement of androgen receptor signaling with a positron-emitting radiopharmaceutical that targets prostate-specific membrane antigen
- In Vivo Imaging of Intraprostatic-Specific Gene Transcription by PET
- Androgen stimulates glycolysis for de novo lipid synthesis by increasing the activities of hexokinase 2 and 6-phosphofructo-2-kinase/fructose-2,6-bisphosphatase 2 in prostate cancer cells
- Pharmacokinetic Assessment of the Uptake of 16{beta}-18F-Fluoro-5{alpha}-Dihydrotestosterone (FDHT) in Prostate Tumors as Measured by PET
- Development of a Second-Generation Antiandrogen for Treatment of Advanced Prostate Cancer
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Molecular Imaging In Tumor Treatment Response
- Imaging Surrogates of Tumor Response to Therapy: Anatomic and Functional Biomarkers
- Novel Tracers and Their Development for the Imaging of Metastatic Prostate Cancer
- Tumor Receptor Imaging
- 7{alpha}-18F-Fluoromethyl-Dihydrotestosterone and 7{alpha}-18F-Fluoromethyl-Nortestosterone: Ligands to Determine the Role of Sex Hormone-Binding Globulin for Steroidal Radiopharmaceuticals
- N-[N-[(S)-1,3-Dicarboxypropyl]Carbamoyl]-4-[18F]Fluorobenzyl-L-Cysteine, [18F]DCFBC: A New Imaging Probe for Prostate Cancer
- Tumor-Specific Positron Emission Tomography Imaging in Patients: [18F] Fluorodeoxyglucose and Beyond
- Initial Experience with the Radiotracer Anti-1-Amino-3-18F-Fluorocyclobutane-1-Carboxylic Acid with PET/CT in Prostate Carcinoma
- Positron Emission Tomography As an Imaging Biomarker
- The Progress and Promise of Molecular Imaging Probes in Oncologic Drug Development
- Biology of Progressive, Castration-Resistant Prostate Cancer: Directed Therapies Targeting the Androgen-Receptor Signaling Axis
- Radiolabeled Small-Molecule Ligands for Prostate-Specific Membrane Antigen: In vivo Imaging in Experimental Models of Prostate Cancer
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- PET-Based Radiation Dosimetry in Man of 18F-Fluorodihydrotestosterone, a New Radiotracer for Imaging Prostate Cancer
- PET Imaging of GRP Receptor Expression in Prostate Cancer