


Abstract
The purpose of the study was to assess the role of 18F-FDG PET/CT in the assessment of secondary malignant involvement of the spinal column. Methods: In 51 patients, 242 lesions at the spinal region detected on 18F-FDG PET/CT were interpreted separately on PET, CT, and fused PET/CT images, including differentiation between benign and malignant lesions and the level in the vertebral column. CT evaluation also included the type of bony lesion (osteolytic, osteoblastic, or mixed) and accompanying soft-tissue abnormalities; for example, epidural masses and tumor involvement of the neural foramina. Results: Of the 242 lesions detected on PET/CT, PET alone identified 220 lesions and CT alone identified 159; 217 (90%) were malignant and 25 benign. 18F-FDG PET alone detected significantly more malignant lesions than did CT alone (96% vs. 68%, respectively, P < 0.001). The specificity was 56% for both PET alone and CT alone. PET alone was incorrect in determining the level of abnormality within the vertebral column in 33 (15%) lesions and in determining the part of the vertebra involved in 40 (18%) lesions. In 17 (33%) patients, either epidural extension of tumor (n = 7 lesions), neural foramen involvement of tumor (n = 7 lesions), or a combination of both (n = 11 lesions) was detected. On a patient-based analysis, the sensitivity of PET and of PET/CT for the detection of spinal metastasis was 98% and 74%, respectively (P < 0.01). Conclusion: 18F-FDG PET/CT has better specificity for detection of malignant involvement of the spine than does 18F-FDG PET. It allows for precise localization of lesions and identifies accompanying soft-tissue involvement, which is of potential neurologic significance.
The vertebral column is the region of the skeleton most frequently affected by metastatic disease. The tumors that most commonly metastasize to the vertebrae are carcinoma of the breast in women and carcinoma of the lung and prostate in men; however, metastasis is also frequently seen in patients with lymphoma and multiple myeloma (1,2).
Vertebral metastases may invade the epidural space by direct extension from adjacent bone, by extension through the intervertebral foramina, or by hematogenous dissemination. Involvement of the epidural space may result in compression of the spinal cord or cauda equina or in radiculopathy because of compression of nerve roots (1). However, occasionally the involvement may be asymptomatic (3,4). Multilevel involvement of the epidural space may also be seen (5). Early diagnosis and treatment before the development of permanent neurologic and functional deficits is essential for a favorable prognosis (6). Radiation remains the primary treatment for metastatic spinal tumor; however, the use of a combined-treatment approach including radiotherapy, chemotherapy, and surgery may be appropriate in selected patients.
MRI of the spine is the method of choice to assess marrow involvement or epidural extension of tumor (7–10). The most commonly used screening test for the assessment of bone metastases is 99mTc-methylene diphosphonate bone scintigraphy, which is obviously not capable of detecting accompanying soft-tissue abnormalities. 18F-FDG PET has been reported to be more sensitive than bone scintigraphy in patients with lung cancer and lymphoma and was shown to detect early bone marrow involvement before cortical changes could be seen by bone scintigraphy (11,12). With the increased use of whole-body 18F-FDG PET for staging and follow-up of malignant diseases, it is not uncommon to encounter vertebral metastases. The aim of this study was to assess the added value of CT in PET/CT studies in lesion detection and localization of vertebral lesions. Special attention was given to detection of compression of the spinal cord, cauda equina, or nerve roots on PET/CT images.
MATERIALS AND METHODS
Patient Population
A retrospective review of 18F-FDG PET/CT reports from studies performed over a 1-y period yielded 51 patients with malignant involvement of the spinal column: 27 female and 24 male (mean age, 62 y; age range, 25–83 y). Primary sites of malignancy were lung cancer (n = 20), lymphoma (n = 12), breast cancer (n = 7), colon cancer (n = 4), melanoma (n = 2), metastatic adenocarcinoma of unknown primary (n = 2), nasopharyngeal cancer (n = 1), carcinoma of the cervix (n = 1), chondrosarcoma (n = 1), and Ewing’s sarcoma (n = 1).
PET/CT Scanning
Patients were asked to fast for at least 4 h before undergoing the examination. All patients had glucose levels below 150 mg/dL. The patients received an intravenous injection of 370–666 MBq (10–18 mCi) of 18F-FDG. Data were acquired 60–120 min after injection using an integrated in-line PET/CT system (Discovery LS; GE Medical Systems).
Data acquisition was as follows: CT scanning was performed first, from the head to the pelvic floor, with 140 kV, 80 mA, a tube rotation time of 0.5 s, a pitch of 6, and a 5-mm section thickness, which matched the PET section thickness. Immediately after CT scanning, a PET emission scan was obtained that covered the identical transverse field of view. The acquisition time was 5 min per table position. PET image datasets were reconstructed iteratively using CT data for attenuation correction, and coregistered images were displayed on a workstation (eNTEGRA; ELGEMS).
Data Acquisition, Analysis, and Statistics
The PET/CT data were separated into PET and CT image sets. Two specialists, a radiologist and a nuclear medicine physician, performed a masked and independent interpretation of the CT and PET images. In a separate session afterward, the readers interpreted the fused PET/CT images. PET/CT image interpretation was considered the gold standard.
Both PET and CT images were assessed using a standardized form. The lesions assessed were either associated with increased 18F-FDG uptake or suggestive of malignancy on CT. PET images were assessed for 18F-FDG avidity of the primary tumor or metastases. On PET, spinal lesions suspected of being tumor sites were recorded. The level of the vertebra in the vertebral column and the part of the vertebra involved (body, posterior elements, or both) were recorded as well. On the basis of these data and the intensity of 18F-FDG uptake, scintigraphic lesions were scored on a 3-point scale for likelihood of malignancy (1 = likely benign, 2 = perhaps malignant, and 3 = likely malignant). Lesions localized at the facet joints, at the end plates, beyond the vertebral body, and at the posterior aspect of the spinous process were considered benign, whereas lesions localized at the posterior part of the body or at the pedicles were considered malignant (13).
On CT, malignant lesions were suggested by the presence of lytic, sclerotic, or mixed lytic-sclerotic changes; intramedullary changes; or bone lesions with accompanying adjacent soft-tissue abnormality and were scored on the same 3-point scale for likelihood of malignancy. Paravertebral soft-tissue masses, including epidural masses, or masses involving neural foramina were recorded. If epidural involvement was suggested, the observer classified compression of the spinal cord or cauda equina on a 3-point scale for percentage stenosis of the spinal canal (1 = mild [<25%], 2 = moderate [25%–50%], and 3 = severe [>50%]).
On PET/CT, all parameters inspected on PET and CT images alone were reassessed. Concordant lesions on PET and CT (i.e., a suspected metastatic lesion in the same location on both modalities) were classified as malignant. Lesions were classified as benign if PET/CT found that the location of the increased 18F-FDG uptake corresponded with that of a benign-appearing CT lesion, such as a hot osteophyte, degenerative facet joint changes, or physiologic 18F-FDG uptake in paraspinal muscles. Discordant lesions (i.e., lesions suspected of representing a metastatic deposit on only 1 modality) were considered malignant if 1 of 2 conditions was met. The first was if a score 3 lesion was identified on PET and, although CT findings were negative, extensive metastatic disease was identified in other skeletal locations. The second was if a small CT lesion was scored 3 and PET findings were considered false negative because of the small size of the lesion.
Lesions were considered equivocal if classified as possibly malignant (score of 2) on one modality and benign on the other. Discordant lesions and equivocal lesions were correlated with other imaging modalities and clinical follow-up for final diagnosis, and if the latter could not be established, those lesions were excluded from the result analysis. Correlative imaging or histologic proof was obtained for cases in which epidural or neural foramen involvement was suggested on 18F-FDG PET/CT.
The sensitivity and specificity of 18F-FDG PET and CT for differentiation of malignant from benign bone lesions were assessed on both lesion-based and patient-based analyses and compared using the McNemar test. P < 0.05 was considered statistically significant.
RESULTS
Lesion Detection
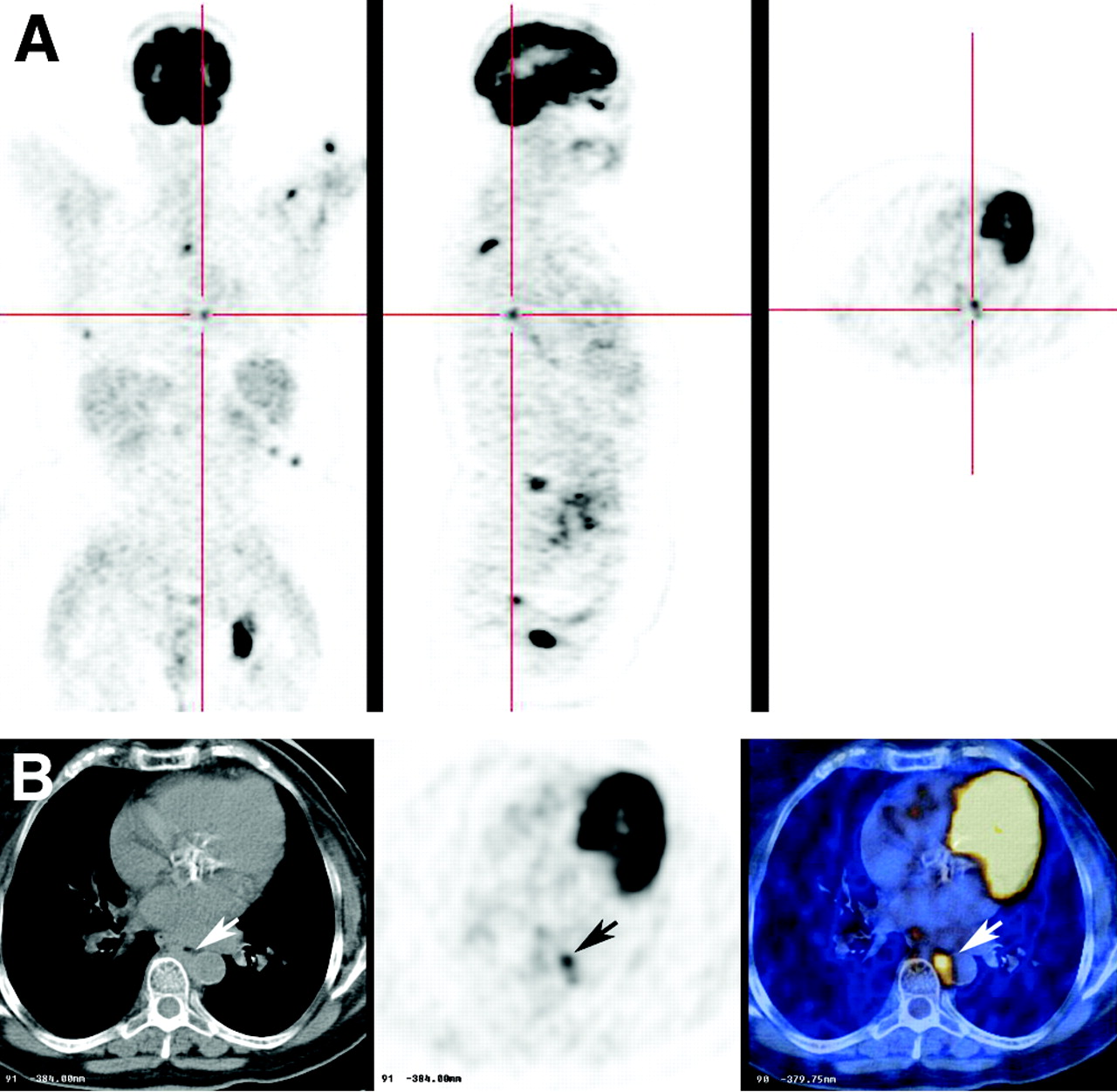
Overall, 51 patients with 253 lesions were assessed on PET/CT. Twenty-six patients had concordant lesions on PET and CT. In 25 patients, discordant or equivocal lesions were identified. For 14 of them, metastatic disease was confirmed by bone scintigraphy (n = 6) or MRI (n = 5) or by progression seen on follow-up PET/CT (n = 3). These 25 patients with discordant lesions had lung cancer (n = 13), lymphoma (n = 3), breast cancer (n = 3), melanoma (n = 3), colon cancer (n = 1), nasopharyngeal cancer (n = 1), or adenocarcinoma of unknown primary (n = 1). In an additional 10 patients with false-negative CT findings and intense focal uptake of 18F-FDG, additional skeletal metastases were seen. It is assumed that these cases represent extensive marrow involvement, which may precede the cortical bony changes detected by CT (Fig. 1).

Multiple bone marrow metastases seen only on PET and not on CT in a 52-y-old man with lung cancer. CT, PET, and PET/CT images are shown from left to right.
Of 253 lesions, a final diagnosis was not established for 11 and they were excluded from the result analysis. The remaining 242 lesions, with an average of 4.92 lesions per patient (mean, 2; range, 1–25), composed the study database. Of those lesions, 163 involved exclusively bone, 25 involved exclusively soft tissue, and 54 involved both bone and soft tissue.
Final analysis showed that 217 of 242 lesions assessed were tumor deposits in the spinal column. Table 1 compares the separate assessment of lesions by PET and CT. PET identified a significantly greater number of malignant lesions than did CT (209 [96%] lesions, compared with 148 [68%] lesions, respectively [P < 0.001, χ2 value = 51.25, 95% confidence interval of the difference = 0.354–0.208]). The specificity of PET and CT was 56% for each modality (P = not significant, χ2 value = 0.05).
Lesion-Based Analysis for Separate PET and CT Readings
Of the 110 true-positive bone lesions detected on CT, 55 (50%) were osteolytic, 21 (19%) were osteoblastic, and 34 (31%) were mixed. The sensitivity of PET in detecting osteoblastic metastasis was 88%, compared with 100% for osteolytic metastasis and 100% for mixed metastasis. Compression of the vertebral body was identified in 6 of the 110 (5%) metastases identified on CT (Fig. 2).

Vertebral body compression in a 63-y-old woman with multiple osteoblastic bone metastases. CT, PET, and PET/CT images are shown from left to right. (A) Sagittal images show vertebral body compression of T11 (arrows). (B) Axial CT images show posterior displacement of bony fragment into spinal canal (arrow).
Patient-Based Analysis
Of the 51 patients assessed, 2 patients were omitted from patient-based analysis. Both had solitary vertebral lesions that were equivocal on PET and PET/CT and were treated on the basis of extraskeletal proven metastases. Table 2 summarizes the results of the study on a patient-based analysis of the remaining 49 patients. On patient-based analysis, the sensitivity of PET and CT were 98% and 74%, respectively (P < 0.01, χ2 value = 7.7, 95% confidence interval of the difference = 0.08–0.39); and the specificity of PET and CT alone was 50% for either modality (P = not significant). When interpretations of PET and PET/CT were compared for the presence of spinal metastases on a patient-based analysis, only 1 patient had evidence of a metastasis in the occipital condyle on PET/CT, and that finding was overlooked on the PET-alone interpretation.
Patient-Based Analysis for Separate PET and CT Readings
Location
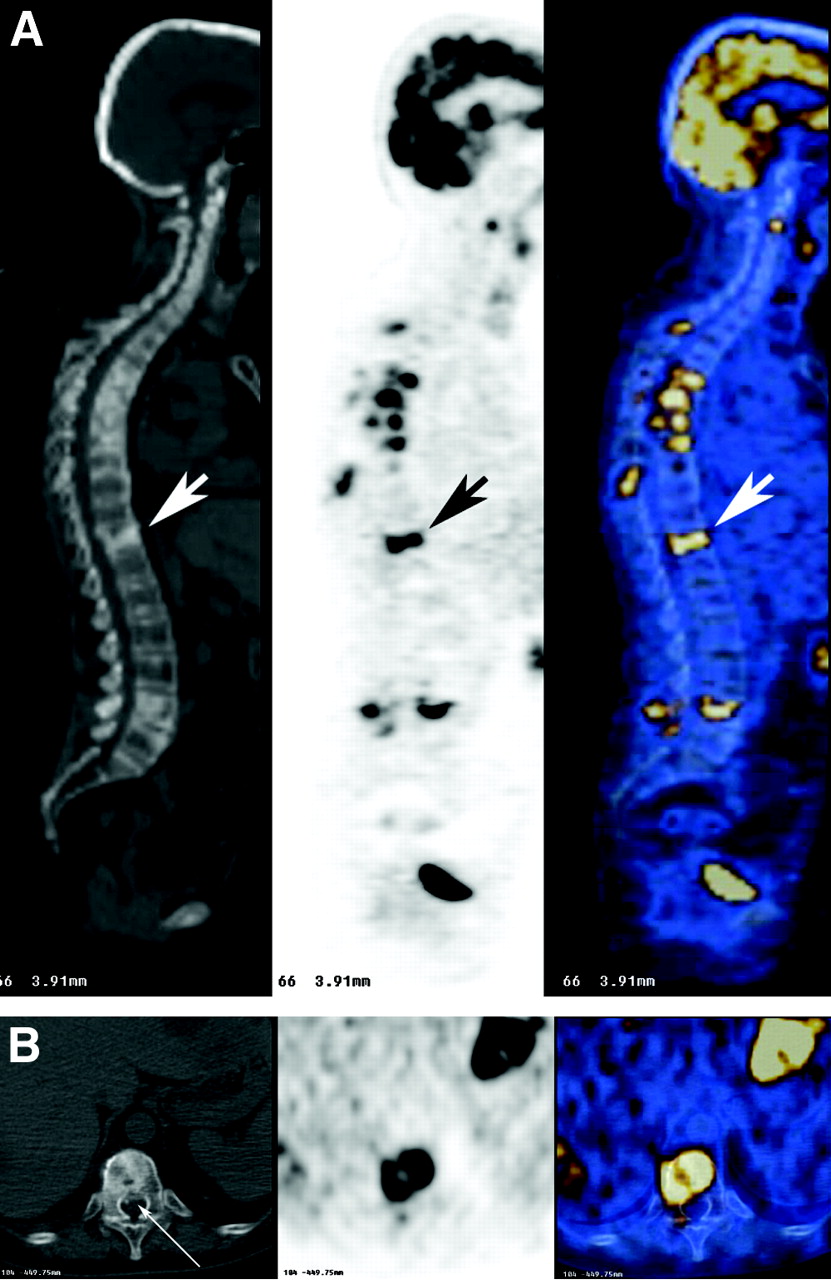
PET alone was incorrect in determining the level of metastases in 33 (15%) of 220 lesions (20 lesions involving bone only and 13 lesions involving soft tissue as well). The accuracy level was 1 level below or above the level suggested on PET interpretation (Fig. 3). Incorrect localization of abnormality within the vertebra by PET alone as compared with PET/CT was found for 40 (18%) of all vertebral lesions detected by PET. Most errors on PET (93%) were between posterior portions of the vertebral body and posterior elements. In 1 case, PET alone interpreted a vertebral metastasis, which was found on PET/CT to represent a metastatic lymph node without adjacent bone involvement (Fig. 4).

Difficulty in determining the level of vertebral metastasis on PET alone in a 77-y-old woman with lung cancer and severe scoliosis. CT, PET, and PET/CT images are shown from left to right. Sagittal PET/CT images show metastatic lesion in a mid- to lower-thoracic vertebra (arrows). The precise level of abnormality is impossible to determine on PET alone because of scoliosis and poor delineation of vertebral column.
Incorrect localization of a lesion on PET alone in a 68-y-old woman with lymphoma. (A) From left to right, axial, coronal, and sagittal PET images suggest abnormal uptake of 18F-FDG in the left aspect of a thoracic vertebra. (B) CT, PET, and PET/CT images are shown from left to right. Axial PET/CT image shows abnormality to be in a posterior mediastinal lymph node and not in a vertebra (arrows).
Soft-Tissue Abnormalities at the Spinal Region
Seventy-nine (36%) of the 217 tumoral lesions in 17 (33%) of the 51 study patients had either soft-tissue masses in the spinal column or vertebral metastases with an accompanying soft-tissue abnormality. Of those, 25 lesions were either epidural extension of tumor (n = 7) (Fig. 5), neural foramen involvement of tumor (n = 7) (Fig. 6), or a combination of both (n = 11) (Fig. 7). Of the 18 epidural lesions, 8 had mild compression, 9 had moderate compression, and 1 had severe compression of the spinal cord or cauda equine. Among the 17 patients with an accompanying soft-tissue abnormality in the spinal vicinity, the primary tumors were lung cancer (n = 5), lymphoma (n = 5), colon cancer (n = 2), adenocarcinoma of unknown primary (n = 2), cervical cancer (n = 1), breast cancer (n = 1), and chondrosarcoma (n = 1).

Epidural extension of tumor on PET/CT in a 50-y-old woman with carcinoma of the colon. CT, PET, and PET/CT images are shown from left to right. (A) Axial PET/CT images show a lytic metastasis involving the posterior aspect of the vertebral body and right posterior elements of T11, with a soft-tissue mass (arrows). Compression of spinal cord (arrowhead) is seen on CT image. (B) Sagittal images better delineate the extent of the epidural mass (arrows).

Involvement of neural foramen on PET/CT in a 53-y-old man with lung cancer. CT, PET, and PET/CT images are shown from left to right. PET/CT images show metastatic deposit in sacrum, involving the left S1 neural foramen (arrows). The right nerve root appears normal on CT (arrowhead).

Tumor mass extending through intervertebral foramina to involve epidural space in a 51-y-old woman with lymphoma. CT, PET, and PET/CT images are shown from left to right. (A) PET/CT images demonstrate invasion of paravertebral soft-tissue mass through right intervertebral foramina in mid-thoracic spine (arrowheads). (B) Axial images show clear extension of paraspinal mass (arrows) into epidural space (arrowhead). Moderate compression of spinal cord to the left is detected on the CT image.
Epidural or neural foramen involvement was validated by MRI (n = 9), contrast-enhanced thin-section full-dose CT (n = 2), biopsy (n = 2), or resolution or progression of findings seen on follow-up PET/CT (n = 3). In 1 patient, correlative imaging or biopsy was not obtained; however, the patient underwent radiation therapy on the basis of PET/CT data and symptomatology.
DISCUSSION
Bone scintigraphy is the most common screening test for suspected bone metastases because of its high sensitivity, availability, low cost, and ability to scan the entire skeleton. MRI is considered the most sensitive method for detection of bone marrow metastases and epidural masses (6,14). Unlike CT, which detects bony abnormalities, particularly cortical destruction, MRI can detect early bone marrow deposits (14,15). Another disadvantage of CT is that cortical destruction may be difficult to detect when osteoporosis or degenerative changes occur (16). 18F-FDG PET can detect increased glucose metabolism of neoplastic cells nested in the bone marrow, making it a sensitive method for assessment of bone and bone marrow metastases. In the current study, 18F-FDG PET alone detected approximately 30% more malignant lesions than did CT alone and, overall, almost 20% more extravertebral skeletal metastases than did CT alone. These findings are concordant with previous reports showing 18F-FDG PET to be more accurate than bone scintigraphy or CT in the detection of skeletal metastases (17,18). As previously reported, 18F-FDG PET is more sensitive for detection of osteolytic metastasis than of osteoblastic metastasis; however, our results indicate that it is a relatively sensitive modality even for the latter type of bone metastasis (19).
The sensitivity of PET alone is high (96% on a lesion-based analysis and 98% on a patient-based analysis). In fact, in only 1 patient of our series were PET-alone findings considered negative for metastatic disease of the spinal column and PET/CT findings considered positive. However, the relatively low specificity of PET and CT in this study (56% for each modality on a lesion-based analysis and 50% on a patient-based analysis) was markedly improved when the two were combined. PET/CT improved the specificity of PET interpretation alone by showing degenerative changes on CT in locations corresponding to areas of increased 18F-FDG uptake and by showing that areas of increased uptake suspected of being vertebral were actually physiologic muscular uptake.
Precise localization of abnormality is important in planning local therapy, such as radiation therapy, in which the radiation field encompasses the involved segment plus 1 or 2 levels above and below it (6). Using 18F-FDG as the radiopharmaceutical, PET defines the skeleton less well than do bone-seeking agents or bone windows on CT. As shown in the current study, this fact may cause uncertainty about the precision with which bony abnormalities have been localized. Fifteen percent of the lesions were incorrectly localized on PET alone, as judged by the vertebral level determined by PET/CT. In addition, in 18% of lesions, incorrect localization within the vertebra was found using PET, as judged by the location determined using PET/CT. 18F-FDG uptake may also be detected in benign changes, and exact localization of the part of the vertebra involved (body, pedicle and lamina, or facet joints) is essential for differentiation between benign and malignant lesions (13,20).
As indicated by the results of the current study, the CT in PET/CT also adds value in the diagnosis of clinically significant pathologies, which may cause pain or neurologic deficit. Metastatic lesions in the spinal column may be asymptomatic or may cause pain. Pathologic vertebral compression fractures are often accompanied by mechanical pain because of instability (21). Detection of these fractures is important because these patients do not respond to steroid therapy and require narcotics or an external orthosis for palliation (6). Recently, 18F-FDG PET was shown able to differentiate between osteoporotic and malignant vertebral compression fractures in patients with 18F-FDG-avid tumors (22). In the current study, 18F-FDG PET/CT enabled detection of pathologic compression fractures in more than 5% of lesions assessed. CT may also aid in determining the presence of spinal cord compression due to bony elements (Fig. 2). Surgical intervention may be indicated in these cases (21,23). A major contribution of CT in 18F-FDG PET/CT studies is its ability to detect and localize soft-tissue components of tumor involving the vertebral column, specifically epidural space invasion, or neural foramen involvement. These lesions are neurologically significant, as they may be associated with spinal cord or cauda equina compression or with radiculopathy. Early detection and treatment of these lesions, before major neurologic deficits occur, is of clinical importance (24,25). In more than 10% of lesions, in one third of the study subjects, 18F-FDG PET/CT detected soft-tissue tumor involving the spine.
The retrospective nature of the study, heterogeneous patient population, and lack of histologic proof for most lesions were limitations. However, obtaining multiple bone biopsies for tissue verification would have been ethically unacceptable. It should be borne in mind that when tumor detection by a new imaging modality is assessed, some suspected tumor sites cannot be characterized histologically, and when the results of different imaging modalities are compared, the more sensitive technique will provide its own standard of criteria (26).
CONCLUSION
18F-FDG PET/CT performed on patients with malignant involvement of the spinal column has better specificity than does 18F-FDG PET alone. PET/CT enables precise localization of lesion level in the vertebral column and—essential for optimal treatment planning—identification of potentially neurologically significant soft-tissue abnormalities.
Footnotes
Received Sep. 7, 2003; revision accepted Oct. 20, 2003.
For correspondence or reprints contact: Ur Metser, MD, Department of Nuclear Medicine, Tel-Aviv Sourasky Medical Center, 6 Weizman St., Tel-Aviv, 64239 Israel.
E-mail: umetser{at}tasmc.health.gov.il
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- [18F]FDG-PET Evaluation of Spinal Pathology in Patients in Oncology: Pearls and Pitfalls for the Neuroradiologist
- Prognostic Value of 18F-FDG PET in Monosegmental Stenosis and Myelopathy of the Cervical Spinal Cord
- Paraneoplastic isolated myelopathy: Clinical course and neuroimaging clues
- Assessment of Patient Exposure to X-Radiation from SPECT/CT Scanners
- Fusion of Metabolic Function and Morphology: Sequential [18F]Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography Studies Yield New Insights Into the Natural History of Bone Metastases in Breast Cancer
- Increased 18F-FDG Uptake in Degenerative Disease of the Spine: Characterization with 18F-FDG PET/CT
- Imaging of Malignant Bone Involvement by Morphologic, Scintigraphic, and Hybrid Modalities